
Abstract
Background
Surgical robots have innovated the microsurgical field by providing advantages that improve surgical performance. These robots have been adopted by certain specialties more than others. This study discusses the potential advantages of robotics in plastic and reconstructive surgery.
Method
This study is a literature review of articles investigating “robotic microsurgery in plastic and reconstructive surgery” using the PubMed database and the Cochrane Library.
Result
A total of nineteen relevant articles were found and 5 articles performed a direct comparison between the robotic and manual approaches. Longer operating times were reported in the robotic groups featuring higher learning curves. Reported advantages to robotic use included higher accuracy, precision and flexibility, elimination of tremor and improvement of ergonomic factors.
Conclusion
While the results provide an outlook into the outcome of robotic platforms in this field, current research is limited and further studies are required to provide a fundamental analysis.
Introduction
In 2000, the first robotic surgical platform was approved by the Food and Drug Administration (FDA) of the United States of America (USA), namely the da Vinci Surgical Robot No. 1 (Intuitive Surgical Inc.™, Sunnyvale, California, USA). 1 Throughout the years, different generations of the da Vinci robot were manufactured as well as other surgical platforms. 2 The clinical application of surgical robots has spread throughout surgical specialties and the reason for this progression is due to the proposed advantages. These advantages include enhanced surgical manipulation and flexibility, enhanced surgical precision through tremor filtration, providing 3D imaging and a reduction in surgical ergonomic factors as opposed to what is found in endoscopic surgery. In comparison to these advantages, conventional endoscopic surgery provides flat 2D vision, limited degree of freedom in surgical manipulation and decreased flexibility. 3 Ergonomic factors such as musculoskeletal pain perceived by surgeons is reported as less frequent in comparison to conventional or laparoscopic surgery. 4
Due to the proposed advantages, robotic surgical platforms have gained widespread clinical use in different surgical specialties. 2 However, specialties such as Ophthalmology and Plastic and Reconstructive surgery are yet to experience a similar increase in the role of robotic-assisted surgery.2,5 Plastic and Reconstructive surgeons commonly perform surgical procedures involving delicate and preferably minimally invasive techniques. Therefore, the previously discussed potential of robotic platforms could play an important role in Plastic and Reconstructive surgery. These advantages were supported by the studies of “pioneers” in the field of robotic reconstructive surgery.6,7 Despite the proposed benefits, robotic-assisted platforms do not play a vital role in Plastic and Reconstructive surgery yet.
The objective of this review is to describe the role of robotic microsurgery in Plastic and Reconstructive surgery and evaluate the outcomes. This analysis will describe the extent of current applications of robotic-assisted surgery in this field and highlight barriers to overcome for future applications.
Methodology
The methodology follows and incorporates the PRISMA checklist as appropriate for the purpose of a literature review.
PICO Table and Search Terms.
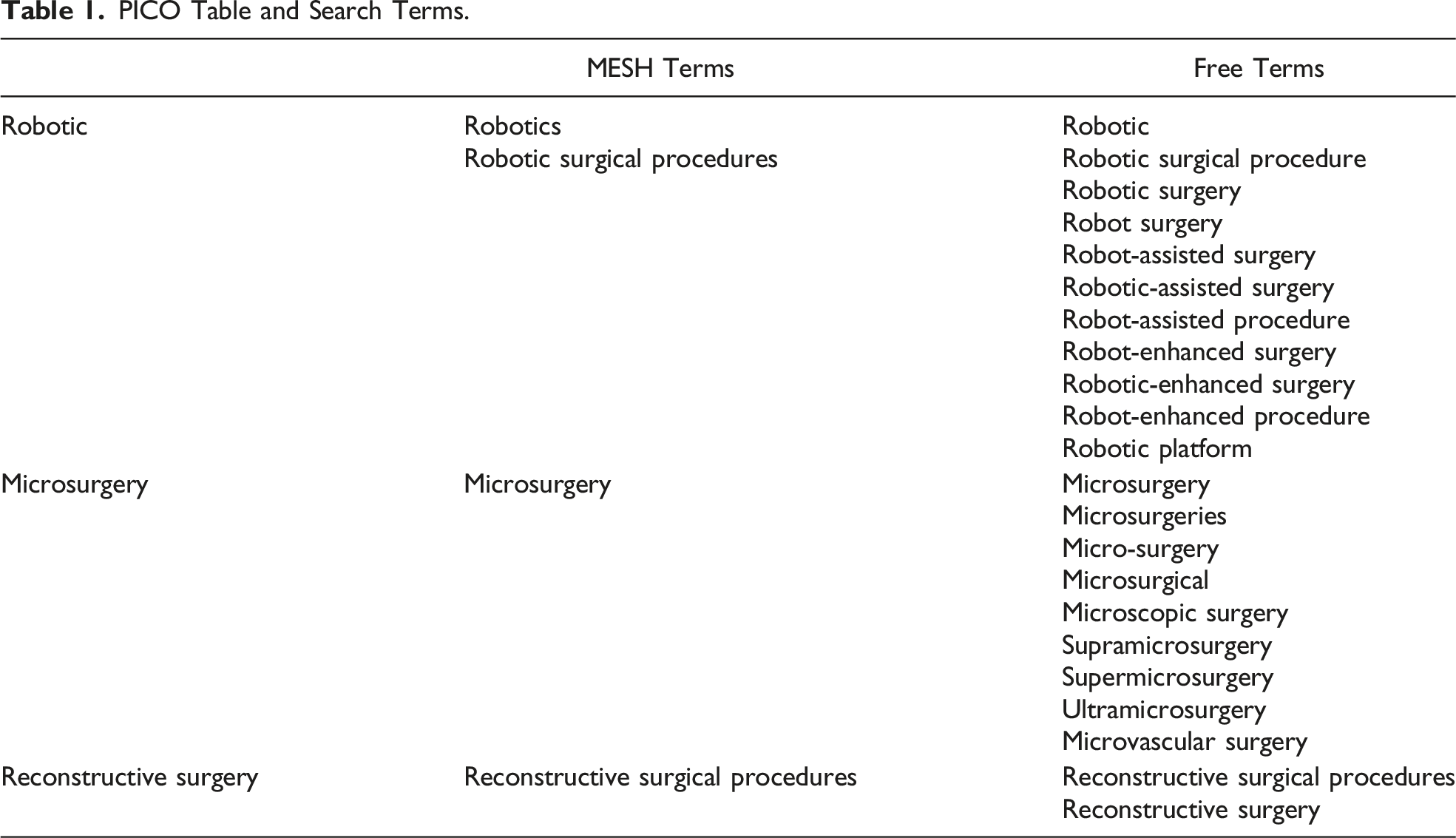
The goal of the search is to include feasibility studies, randomized control trials, cadaveric studies, animal and human studies, case studies, case series and cohort studies. Literature and systematic reviews were excluded. Studies concerning other surgical specialties not relating to reconstructive surgery were excluded. Only full-text English articles directly related to robotic microsurgery in the setting of reconstructive surgery were included. Due to the narrow field of this topic, no further limits have been placed on the search.
The abstracts were analyzed by 2 independent reviewers (H.G and R.M.S) based on relevance to the objective of this review. The resulting articles were grouped in Word for the purpose of visual display and providing rationale for choice of exclusion and inclusion. The articles were further assessed by screening the full-text undergoing a second round inclusion and exclusion to further accommodate the objective of this study. Both rounds of inclusion and exclusion were performed by the same reviewers (H.G and R.M.S).
The final result of the search containing articles with outcomes relevant to the research question of this study were downloaded into EndNote by 1 reviewer (H.G). All data and outcomes of the articles were extracted and collected into Excel and grouped into quantitative and qualitative outcomes. The relevant outcomes include total surgical and/or anastomosis time and presence of post-operative outcomes. All results compatible to the sought outcome were included. Any unclear information regarding the data was not included in the results.
No process of obtaining or confirming data from any study investigators was required. Reporting bias, effect measure and certainty assessment were not directly performed in this review. No methods to explore possible causes of heterogeneity nor sensitivity analysis for robustness of the results were performed in this review.
The respective statistical analyses were described with specific comments on statistical significance and possible outcome limitations.
Results
Figure 1 demonstrates the process of article inclusion and exclusion in the form of a flow diagram. The search yielded 19 articles that were divided into 2 groups by the type of outcome, qualitative or quantitative. Qualitative articles were studies that did not present any numerical variables but instead described their results. Quantitative articles included numerical variables and outcomes such as total surgical time, length of hospital or ICU stay and frequency of post-operative complications. These articles were further divided into 2 subgroups. The first subgroup contains studies which performed a direct comparison between robotic microsurgery and traditional manual surgery, while the second subgroup is a collection of quantitative studies that did not perform such a comparison. Flowchart diagram for the process of inclusion and exclusion of articles.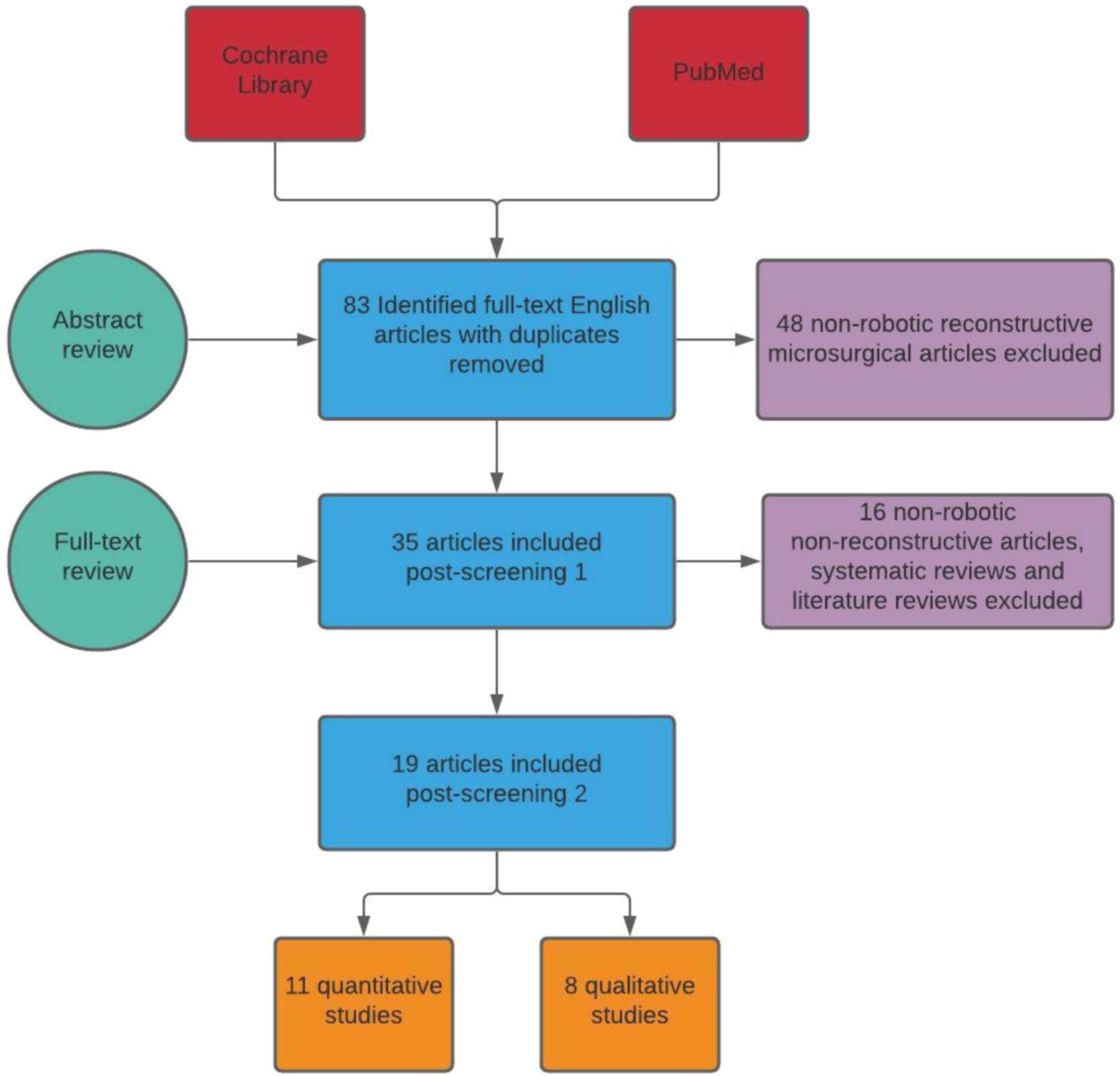
Quantitative Outcomes (Comparison Subgroup)
Quantitative Studies Featuring Comparison Between Robotic and Manual Surgeries.
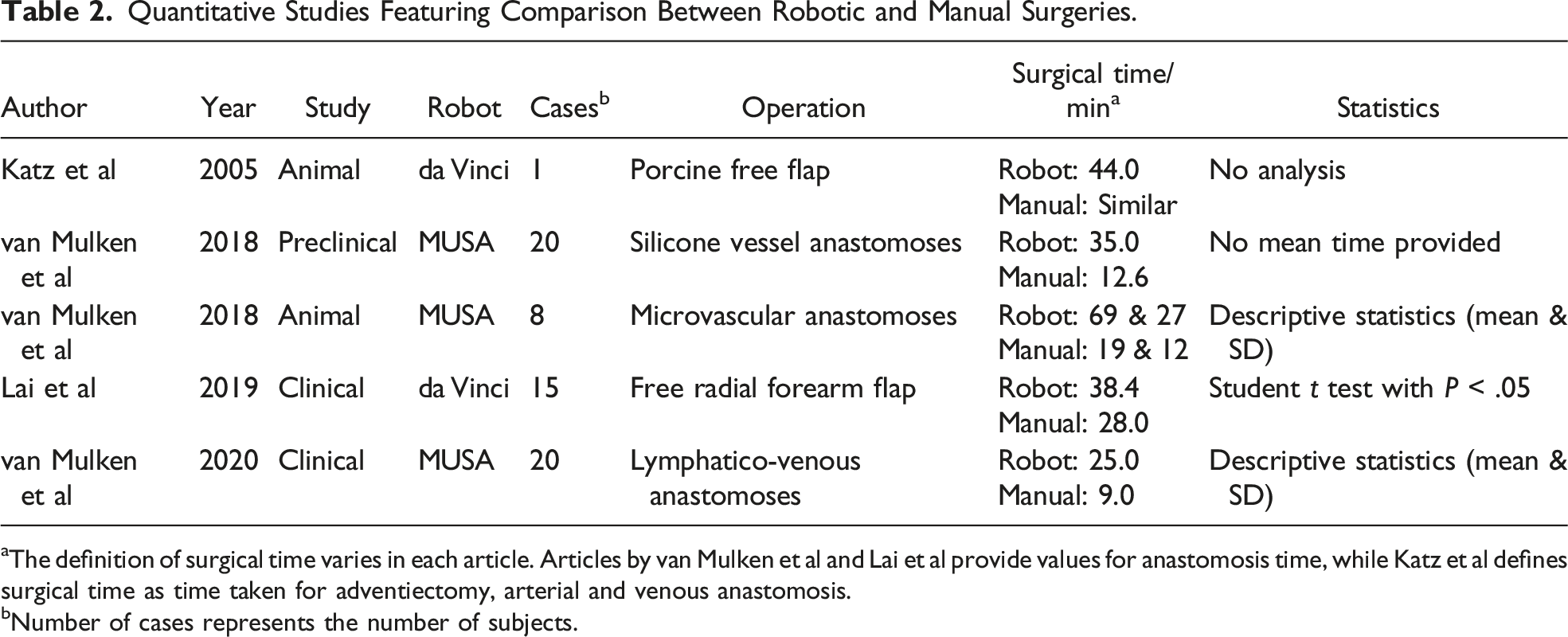
aThe definition of surgical time varies in each article. Articles by van Mulken et al and Lai et al provide values for anastomosis time, while Katz et al defines surgical time as time taken for adventiectomy, arterial and venous anastomosis.
bNumber of cases represents the number of subjects.
The overall outcome of the articles suggests a higher surgical time taken in the robotic approach in comparison to the manual approach, except for the study performed by Katz et al. 8 This study performed free flap surgery on 1 porcine model with the da Vinci robot used for the micro-anastomosis step. One leg was used for the robotic approach and another leg for the manual approach. The surgical time of the manual approach as similar to the robotic approach which took 44 min. Patency was achieved in both cases and no post-operative complications occurred.
Lai et al published a different free flap study utilizing the da Vinci robot for performing the microvascular anastomoses. 9 They performed a free radial forearm flap reconstruction in 15 patients suffering from oropharyngeal cancer undergoing resection. Flap harvesting was performed manually in all cases. The robot was used in 17 anastomoses (2 arterial and 15 venous) and was compared to 26 manual anastomoses (13 arterial and 13 venous) where there was complete patency and flap survival. The average difference in anastomosis time between the 2 approaches was 10 minutes with the robot taking 38.4 ± 10.4 min and manual surgery taking 28.0 ± 7.7 min. A student t test was performed in this study and it showed significant statistical difference in the operating time between the 2 approaches. There were no significant post-operative complications other than 1 hematoma occurring in the robotic group.
Similar results have been reported in 3 pilot studies by van Mulken et al using the MUSA robot (University of Technology, Eindhoven, The Netherlands) for microvascular anastomosis. All 3 studies reported the surgical time parameter of the anastomosis comparing the robotic approach to the manual approach. In the preclinical study, anastomoses were performed on 10 silicone vessels using the MUSA robot and 10 silicone vessels by the manual approach. 10 No mean time was provided, however, the surgical time in the final sessions were 35.0 for robot and 12.6 for the manual approach. No statistical analysis was performed to identify the significance in difference, yet there is clinical significance. An animal study by van Mulken et al included 3 microvascular anastomoses that were performed in the abdominal aortas (AA) and 4 femoral arteries (FA) of rats, while only 1 manual approach was performed in both groups as a comparison. 11 The mean surgical time for the robotic approach of the AA surgeries was 69.0 min (53-87 min) while manual was 19.0 min. The time difference for the FA group was significantly smaller, where the robot took only 27.0 min (26-29 min) in comparison to 12.0 min taken by the manual approach. All anastomoses were patent except for 1 FA in the robotic group. In the randomized clinical pilot study by van Mulken et al, lymphatico-venous anastomoses (LVA) were performed on 20 patients. 12 Eight patients underwent the robotic approach while 12 patients had the LVA performed manually. Complete patency was achieved in all anastomoses and there were no post-operative complications other than a suspected erysipelas infection in the robotic group which was treated with oral antibiotics. The mean surgical time taken by the robot was 115 min in comparison to the manual surgeries which took 81 min, showing a clinically significant difference. The mean anastomosis time taken by the robot was 25 min (16-33 min) in comparison to 9 min (4-33 min) in the manual surgeries. Both differences in mean duration and time range were statistically significant (P < .001).
Quantitative Outcomes (Non-Comparison Subgroup)
Quantitative Studies Without a Comparison Between Robotic vs Manual.
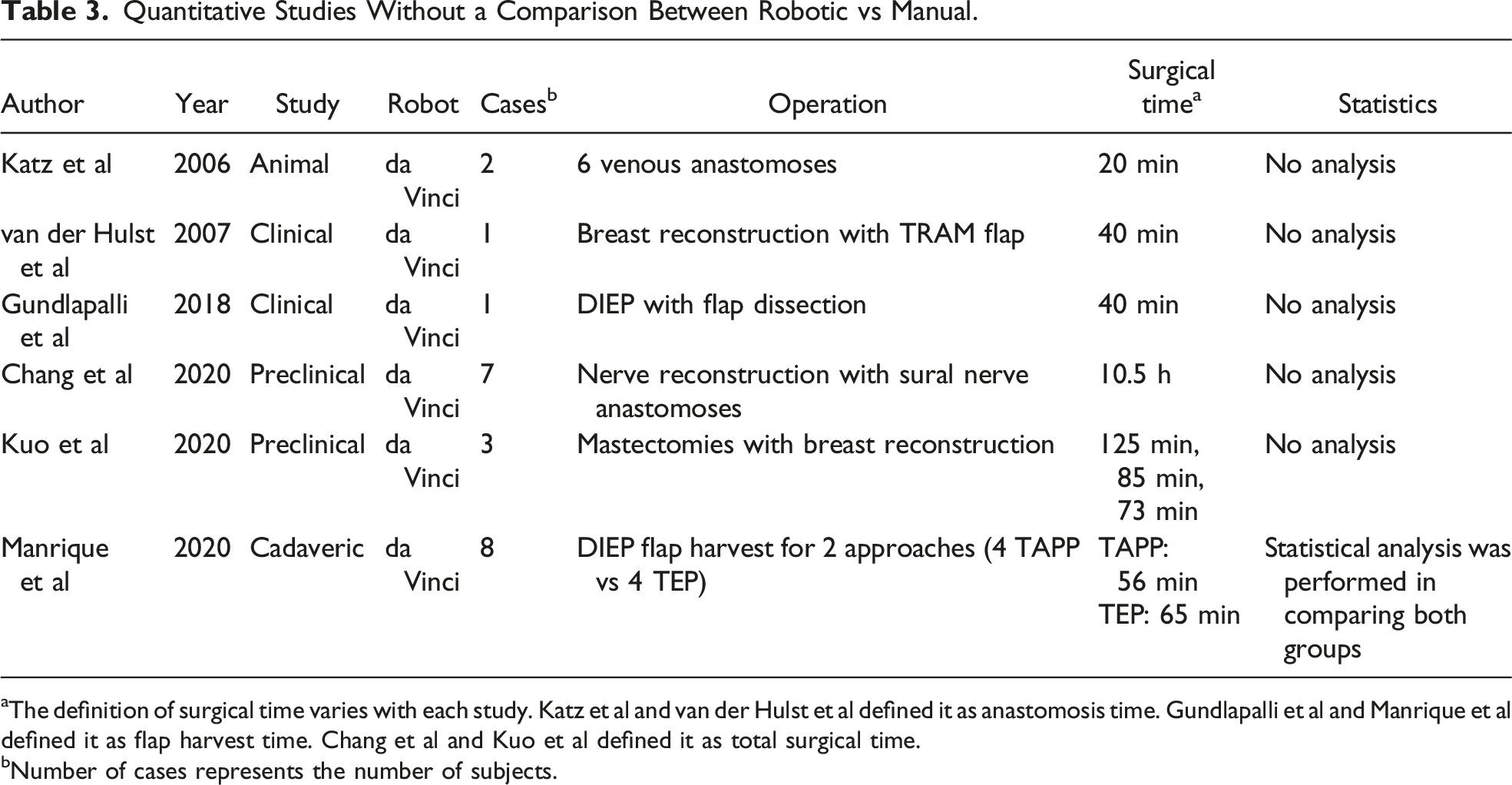
aThe definition of surgical time varies with each study. Katz et al and van der Hulst et al defined it as anastomosis time. Gundlapalli et al and Manrique et al defined it as flap harvest time. Chang et al and Kuo et al defined it as total surgical time.
bNumber of cases represents the number of subjects.
In the animal study by Katz et al, 6 anastomoses were performed in canine tarsal and superficial femoral veins robotically. 13 Patency was achieved completely. The anastomoses time decreased significantly between the first 2 anastomoses and the remaining 4, progressing from 67 and 70 min to 35, 21, 25 and 20 min respectively. There is no comparison to test statistical significance, however, the decrease in time is clinically significant.
Van der Hulst et al produced a case report using the da Vinci robot to perform arterial anastomosis in a patient undergoing breast reconstruction with a muscle sparing free transverse rectus abdominus muscle flap (TRAM-flap). 14 The anastomosis time was 40 min and while no direct comparison was performed, the article reports that the average time taken for such an anastomosis would take approximately 15 min to complete manually. While Gundlapalli et al also published a case report of a single patient undergoing a deep inferior epigastric perforator flap (DIEP) reconstructive surgery, the da Vinci robot was used in dissecting the intraabdominal flap instead of the microvascular anastomosis. 15 The time taken for flap dissection was 40 min and was also reported as similar to the average time taken if dissection was performed manually. There was successful patency and no post-operative complications.
Each of the remaining articles approached the study of robotic microsurgery uniquely. Chang et al published a feasibility study on 7 sural nerve reconstructions focusing on robotic-assisted micro-neural anastomoses. 16 There were no comparisons mentioned and average total surgical time taken was reported as 10.5 h without describing the difference in duration between the 7 surgeries. Median length of post-operative stay was reported as 4 days and only 1 patient developed a post-operative complication which was not directly linked to the use of the robot. This study does not perform statistical analysis on the outcome, however, symptom improvement was reported as 70% compared to the pre-operative period which was considered successful by the authors. Kuo et al performed robotic mastectomies on 3 patients with breast reconstruction. 17 The robot was used to perform the mastectomies and not the micro-anastomoses. The total surgical time decreased from 125 min in the first surgery to 85 min in the second surgery and finally 75 min in the final surgery. Despite the lack of statistical analysis, this outcome shows that there is a clinically significant difference between the surgeries. No post-operative complications occurred. The final article by Manrique et al was a unique cadaveric study aimed at comparing the difference between 2 robotic-assisted approaches to DIEP flap harvesting, the transabdominal pre-peritoneal (TAPP) and totally extraperitoneal (TEP) approaches. 18 Focus was on comparing the performance of these approaches rather than commenting on the clinical outcome of the use of the robot in this study. Statistical significance was shown in the different operating times between the 2 approaches. The TAPP approach took 56 min in comparison to the TEP approach which took 65 min.
Qualitative Outcomes
Qualitative Studies.
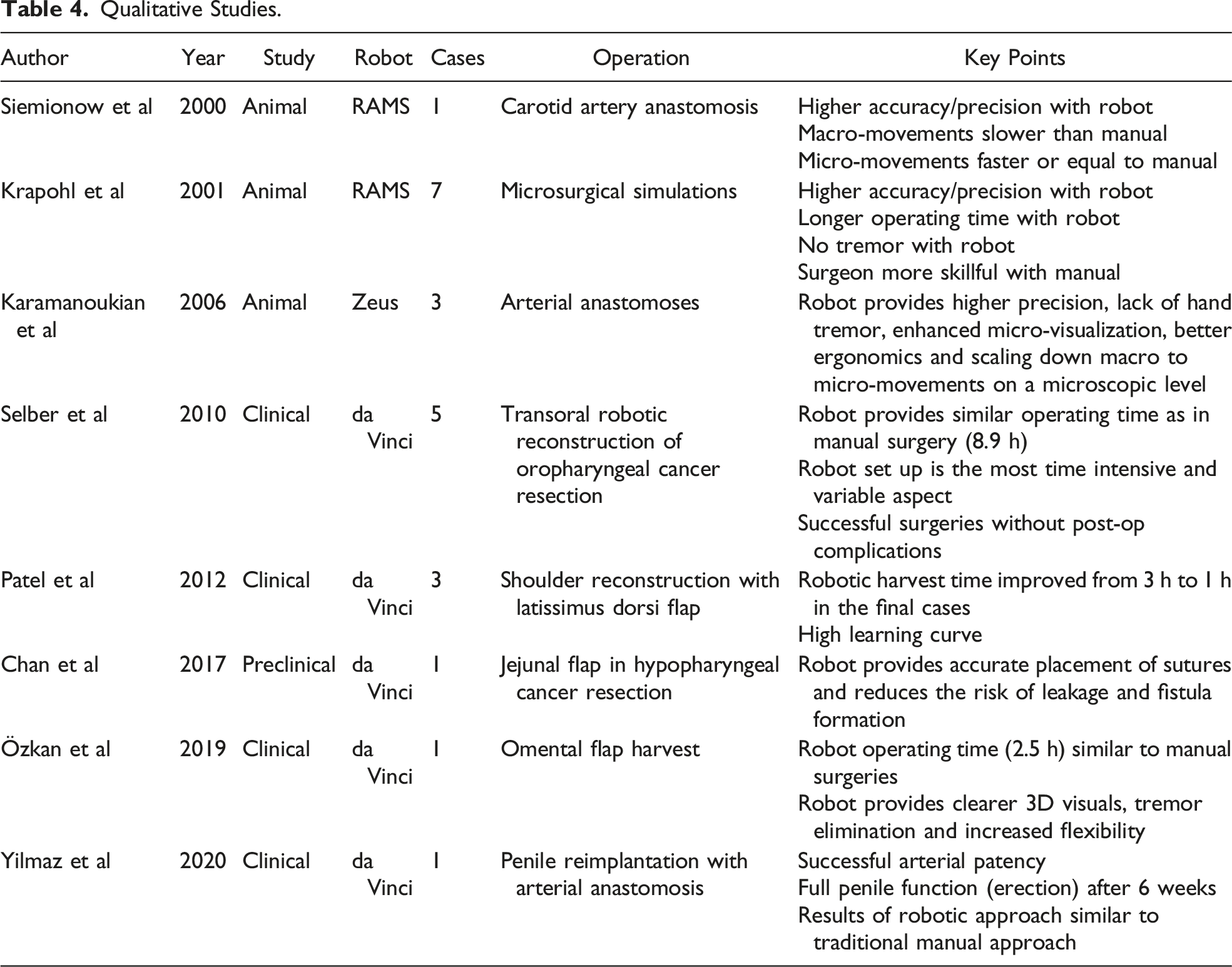
The most recent case report by Yilmaz et al claims that this was the first robotic-assisted penile transplantation report published. 26 The report describes a patient indicated for a penile amputation and consequently underwent transplantation. Full patency and penile function were achieved, and the article describes the overall results as very similar to the traditional manual microsurgical technique of penile transplantation, thus highlighting the feasibility of this robotic approach. However, the time needed to perform this operation was not mentioned.
Discussion
Robotic surgical platforms have gained widespread clinical use in different surgical specialties, e.g., Urology, Gynecology and Neurosurgery. Radical prostatectomies are more commonly performed with robotic assistance in the US and 95% of US graduating Gynecology fellows are trained to use the da Vinci robot. 2 The number and quality of studies investigating the feasibility and clinical performance of these robots are also higher in comparison to what has been produced in Plastic and Reconstructive surgery within the past 2 decades. Not only is the applicability of robotics in reconstructive surgery low, but the quality of research performed in this field is comparatively lower as evident by the number of samples and cases found in this review.
Despite a specific search, this current literature review yielded only 19 relevant articles with the majority being preclinical studies and single case reports. Only 3 clinical studies included 5 or more cases to provide a more valid foundation for their respective results and yet the number of cases is also low. Moreover, only 5 of the nineteen articles performed a direct comparison between robotic-assisted surgery and manual surgery. The comparison performed provides a stronger foundation to base published results on and to bridge further larger studies. However, the majority of these studies were still very recent containing comparatively smaller sample sizes with respect to the previously mentioned examples and were heterogeneous. Out of the 5 articles only 1 performed statistical analysis in order to discover if the difference in outcome was statistically significant or otherwise. This lack of homogeneity, small number of high quality studies and with limited statistical analysis creates difficulty in providing a complete overall judgement on the performance of robotic-assisted platforms in reconstructive surgery. Despite the proposed advantages, it is difficult to produce statistically and scientifically profound proof on their current performance based on the results of this review.
Certain common outcomes can be extracted from this data that would agree with the proposed advantages of using robotic platforms. A commonly found theme in this study was the presence of high and rapid learning curves. In almost all studies, operating time was found to be longer than the manual surgical counterparts. Yet in articles that performed a series of surgeries, it was found that the operative time decreased along the consecutive surgeries. This was highlighted in both studies by van Mulken et al concerning silicone vessel anastomoses and anastomoses of lymphatic vessels.11,12 The final operating times of the robotic surgeries were still higher than the manual surgeries, however, it was suggested that if further surgeries were performed such a significant time difference would no longer be observed.
Another common finding of this review was the confirmed advantages offered by the robotic platforms, such as increased precision, accuracy, flexibility in (micro) movement, tremor elimination and improvement of ergonomic factors.
A commonly described potential disadvantage was the lack of tactile feedback, which is also commonly experienced during manual microsurgery. According to different studies, this would not be an issue for experienced surgeons.8,9,13 Furthermore, the enhanced 3D visuals provided by the robots compensate for this lack.27,28 Additional disadvantages such as cost and restricted workflow were highlighted by Tan et al. 2 The cost of purchase, maintenance, training and providing suitable micro-instruments is high requiring a significant amount of funding which can limit widespread applicability. The operative processing of these robots is not guaranteed and a possible breakdown prior to or midway through surgeries can occur. This forces surgeons to switch between the robotic and manual approach halfway through surgeries which is more time-consuming.
Limitations of this study include the limited of amount of available research regarding robotic microsurgery in Plastic and Reconstructive surgery and the heterogeneity in the results of the reviewed articles which hinders the ability to perform a statistical analysis. Furthermore, this review aimed to study the effect of robotic microsurgery as a direct comparison to the traditional approach. However, due to the lack of such articles it is difficult to provide a solid conclusion on the topic.
Conclusion
This literature review provides an overview of the overall performance of robotic microsurgery in Plastic and Reconstructive surgery. The number of articles is limited and the reported outcomes lack sufficient comparison of robot-assisted operations to conventional manual techniques in addition to a lack of statistical analyses performed. This literature review reflects the potential benefits of using robots in Plastic and Reconstructive surgery but does not provide sufficient data to confirm these benefits. Further larger clinical studies with more extensive statistical analyses that compare robot-assisted operations to conventional microsurgery are needed in this field.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.