
Abstract
Objective. Motor imagery (MI) is widely used to improve technical skills in sports and has been proven to be effective in neurorehabilitation and surgical education. This review aims to identify the key characteristics of MI protocols for implementation into surgical curricula. Design. This study is a systematic review and meta-analysis. PubMed, MEDLINE, Embase and PsycINFO databases were systematically searched. The primary outcome was the impact of MI training on measured outcomes, and secondary outcomes were study population, MI intervention characteristics, study primary outcome measure and subject rating of MI ability (systematic review registration: PROSPERO CRD42019121895). Results. 456 records were screened, 60 full texts randomising 2251 participants were reviewed and 39 studies were included in meta-analysis. MI was associated with improved outcome in 35/60 studies, and pooled analysis also showed improved outcome on all studies with a standardised mean difference of .39 (95% CI: .12, .67, P = .005). In studies where MI groups showed improved outcomes, the median duration of training was 24 days (mode 42 days), and the median duration of each individual MI session was 30 minutes (range <1 minute-120 minutes). Conclusions. MI training protocols for use in surgical education could have the following characteristics: MI training delivered in parallel to existing surgical training, in a flexible format; inclusion of a brief period of relaxation, followed by several sets of repetitions of MI and a refocusing period. This is a step towards the development of a surgical MI training programme, as a low-cost, low-risk tool to enhance practical skills.
Introduction
Surgical education has been increasingly reliant on training methods which involve simulation, ranging from simple bench models to virtual reality simulation and box trainers. 1 Motor imagery (MI) can be described as a form of simulation; it consists of imagining oneself performing a voluntary movement, without physically moving. 2 It has also been called mental practice (MP), mental training and mental imagery.
Motor imagery has been proven to be effective at improving technical skills in various fields,3-6 and structured training programmes which incorporate this concept are reported in the literature. In sports psychology, MI has been integrated in several models such as the PETTLEP model 7 which delivers a format of training applicable to different sports. In the field of neurorehabilitation, Braun’s review 8 identified the elements which correlate with effective training outcomes.
Several studies have successfully shown that this method can also be adapted to surgical training9-11: Immenroth et al 11 used MI for training in laparoscopy cholecystectomy via one-on-one mental training sessions, where trainees memorised the operation primer and visualised their inner perception of the operation based on this. Louridas et al 12 developed and tested a script based on MI to perform laparoscopic jejunojejunostomy, using visual and kinaesthetic (tactile) cues. Despite encouraging results, these studies allow limited application for MI training outside of the specific surgical procedures they were designed for.
The aforementioned areas of neurorehabilitation, sport psychology and training in specific surgical procedures use common principles of MI to achieve motor improvement. Current understanding of the neurological mechanism of MI is dominated in the literature by Jeannerod’s central motor theory.7,13-16 It underpins the hypothesis that a degree of functional equivalence exists between MI, and motor preparation and execution, and that they share common neural substrate.7,13,14 Empirical evidence supporting the functional equivalence concept can be seen at different levels of control, namely central (in the frontal and parietal lobes 17 ), peripheral (via increased heart rate and respiratory rate 18 ) and behavioural (via mental chronometry18-20). This mechanism is applied to any motor development using MI, regardless of the type of skill being targeted. Based on this understanding, a cross-disciplinary use of MI protocols can be explored in order to identify important elements of MI training.
Protocols incorporating MI in medical education are not readily available in the literature, 10 and there has so far been no rigorous approach regarding the evaluation of the format in which MI training should be incorporated into surgical education programmes.
The aim of this review and meta-analysis is to identify the components necessary to a training protocol for surgical education which uses MI. This will be done by gathering evidence from fields which have successfully used this method for decades. 21 The primary outcome will be the effectiveness of a protocol using MI training, measured through different outcome measures due to the diversity of studies included. The secondary outcomes will be protocol components.
This review will be structured according to the PRISMA checklist for systematic reviews and meta-analyses.
Methods
Protocol and Registration
The review has been registered on PROSPERO (registration number: CRD42019121895).
Eligibility Criteria
In order to limit this review to evidence of the highest standard of quality, only randomised controlled trials (RCTs) of the use of MI in any discipline were used. Inclusion criteria were as follows: RCTs published up until December 2018; studies in English, French and Spanish only; studies of MI training programmes which measured an objective outcome for a specific voluntary skill; studies which included a protocol based on imagining a movement. Exclusion criteria were as follows: studies which were not RCTs; studies in which MI training was combined with simulation training; studies in which MI training was done in conjunction with functional magnetic resonance imaging (fMRI), electroencephalograms (EEG), electromyography (EMG), transcutaneous electric nerve stimulation (TENS), electroacupuncture or hypnosis. However, studies using fMRI, EEG or EMG only as part of pre- and post-intervention evaluation, and not during the intervention period (as may be the case in bio-neurofeedback), were included, providing they met the other eligibility criteria.
Search Strategy and Study Selection
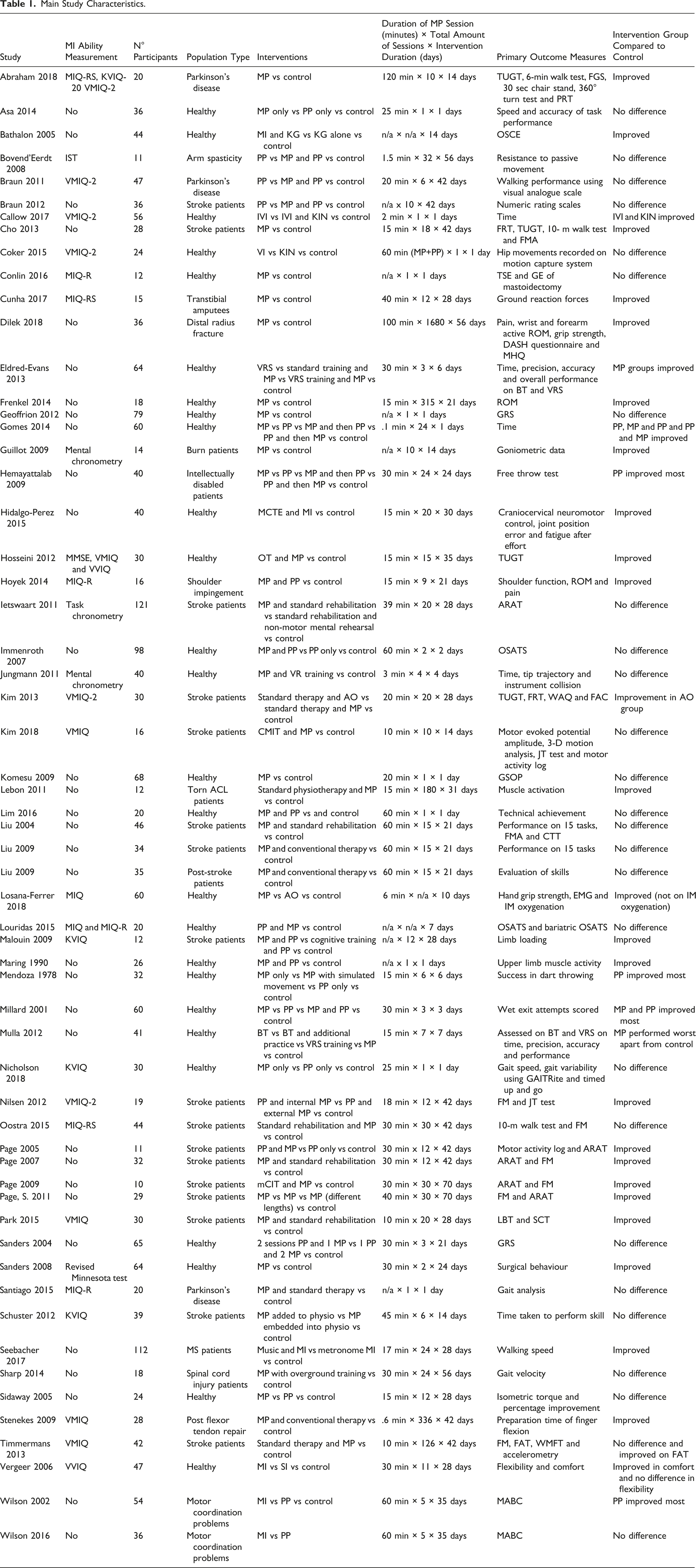
Main Study Characteristics.
Protocol Components for MI Training.

Data collection and Synthesis
Data were extracted by one author using a data extraction form. The primary outcome was the efficacy of the MI training intervention, measured according to the primary outcome measure as defined by study authors. The secondary outcomes were protocol characteristics. The following items were extracted: primary outcome measure, study population, MI intervention group characteristics, control group characteristics, study primary outcome measure and rating of MI ability. The mean and standard deviation of the primary outcome measure for each study were converted to a standardised mean difference. Where post-intervention scores and follow-up scores were reported, the results of the outcome measured post-intervention only were used. Where there were several MI groups with varying length of MI practice and no data on the results of all MI groups combined, the most effective length of practice only was kept. When studies compared different types of MP, they were excluded. Where SDs were not available, they were estimated using IQR/1.35 22 , and if the IQR was not available, they were estimated based on the SDs from other studies included in the meta-analysis. The primary outcome measure used was the primary outcome stated as such by authors. Where this was not reported, the outcome measure used was the most complete measure of progress as described by the study authors, or if this was not available an outcome which reported a single measurement. Where performance was measured in different simulators (e.g. box trainer and virtual reality simulation (VRS)), the simulator which had not been used in training was used.
Meta-analysis
Data were input into Review Manager in order to conduct meta-analysis if it satisfied the following criteria: The mean and standard deviation of the primary outcome measure were available, or could be estimated according to the methods described previously, and the study compared one group performing MI alone and one group performing MI and physical practice. Subgroup analysis was conducted based on length of training, inclusion of a relaxation component to the protocol and selection of participants based on MI ability.
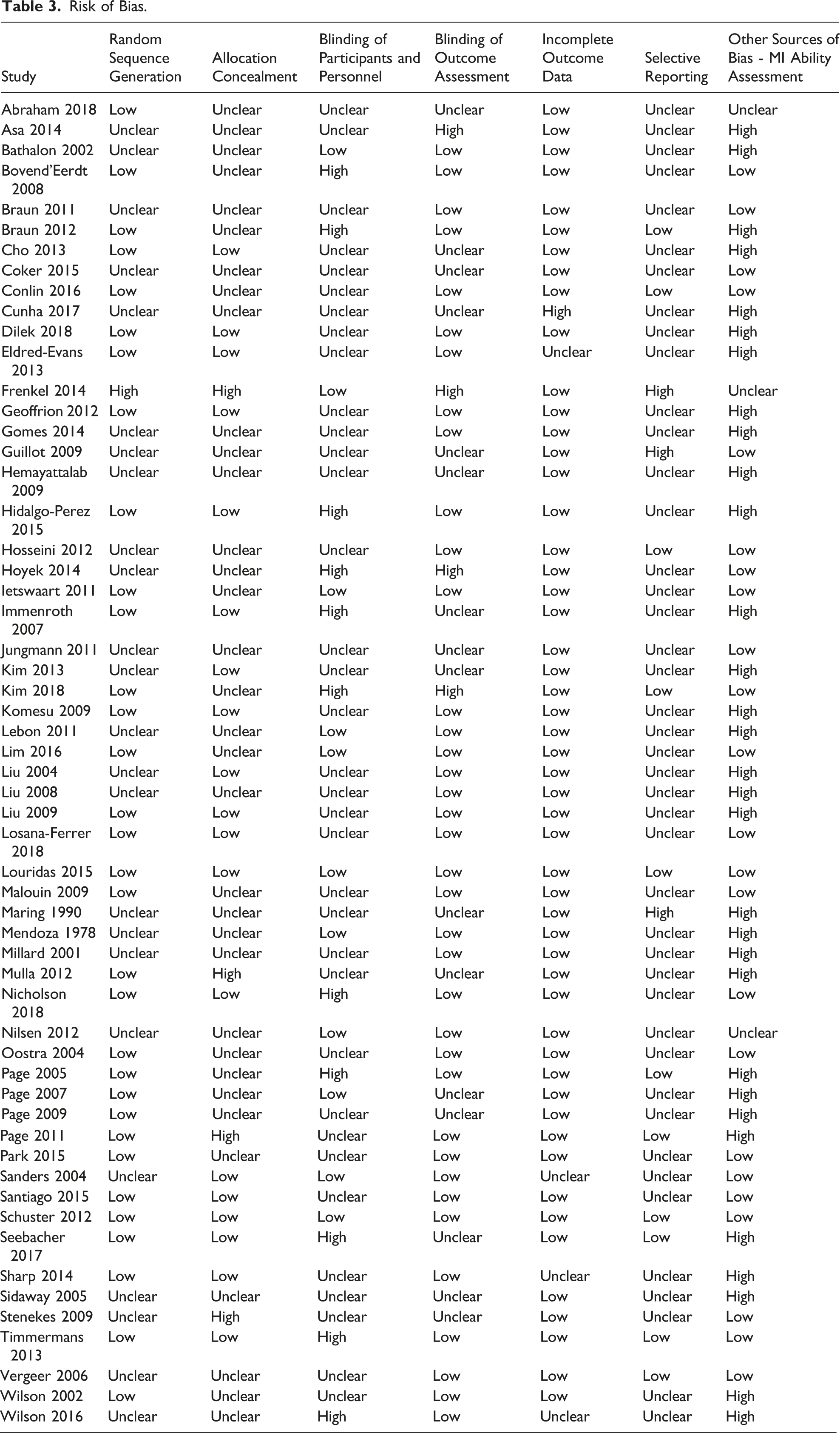
Risk of Bias
Risk of bias was assessed using the Cochrane risk of bias tool. 23
Results
General Study Characteristics
Overall, 60 RCTs were identified with a total of 2251 participants. A flow diagram of the studies’ selection process is illustrated in Figure 1. Studies were published between 1978 and 2018. Study sample sizes ranged from 10 to 112, and median was 34.5. Participants were healthy in 27 studies, had previously had a stroke in 20 studies or in 13 studies had a range of conditions including Parkinson’s disease, multiple sclerosis, arm spasticity or amputation. 6 studies only had surgical residents or trainees as participants, and 12 had healthy students. PRISMA flow diagram.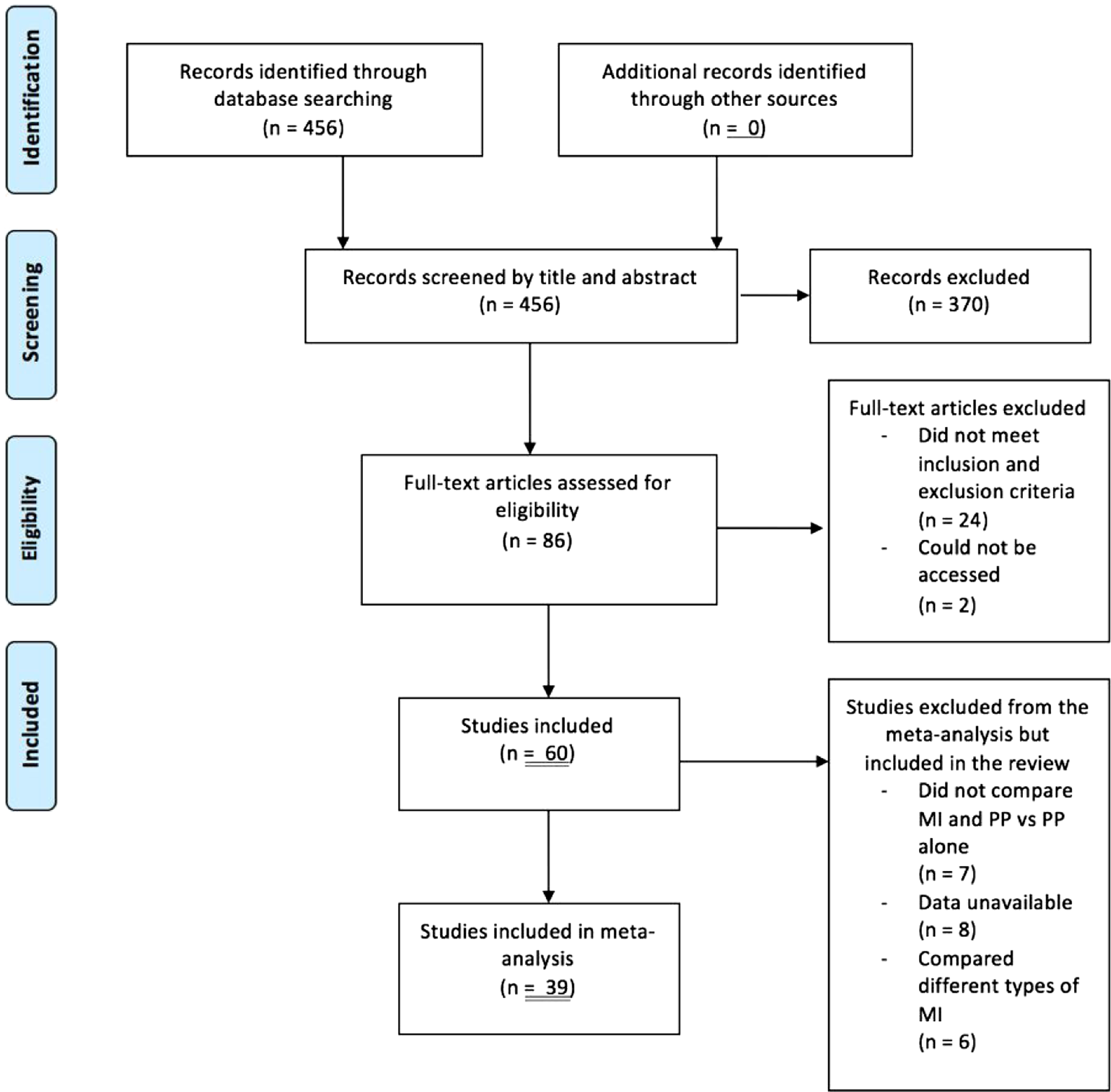
Primary Outcome Measures
The primary outcome was the overall effectiveness of a protocol using MI; several outcome measures were used due to the diversity of studies included. In the 12 studies11,12,24-33 which had medical students or trainees as their population, the primary outcome measures were the Objective Standard Assessment of Technical Skills (OSATS), variations of a Global Rating Scale, independent measures of time taken, precision and accuracy in completion of task or a purpose-built checklist. The remaining studies used task-specific measures such as the Fugl-Meyer assessment for stroke50,56,61 or broader measures of function such as using a goniometer for range of motion40-43.
Outcomes
25 (42%) studies found that the intervention group using MI did not perform better than the control group.6,11,24,26-31,34-49
In 35 studies (58%), the intervention group performed better than the control group.3,12,25,32,33,50-79 In 29/35 studies (83%), the intervention group which did MP and standard physical practice (rehabilitation, physiotherapy and surgical training) performed better than the control group which did only standard physical practice.3,12,25,32,33,50-70,76,78,79 There was no trend found between these study results and the use of MI ability assessment, the outcome measures used or the length of interventions.
A summary of all data extracted is presented in Tables 1 and 2.
Secondary Outcomes: Intervention Duration and Number of Motor Imagery Sessions
The median duration of each individual MI session was 27.5 minutes (range <1 minute-120 minutes).
In studies where the intervention group performed better than control, the median was 30 minutes (range <1 minute-120 minutes). The median number of MI sessions completed was 11 (range 1-1680); and 13 (range 1-1680) in studies where the intervention group performed better than control. The median duration of intervention across all studies was 22.4 days (mode 1, range 1-70), and in studies where the intervention group performed better than control, it was 24 days (mode 42, range 1-70).
Secondary Outcomes: Intervention Content
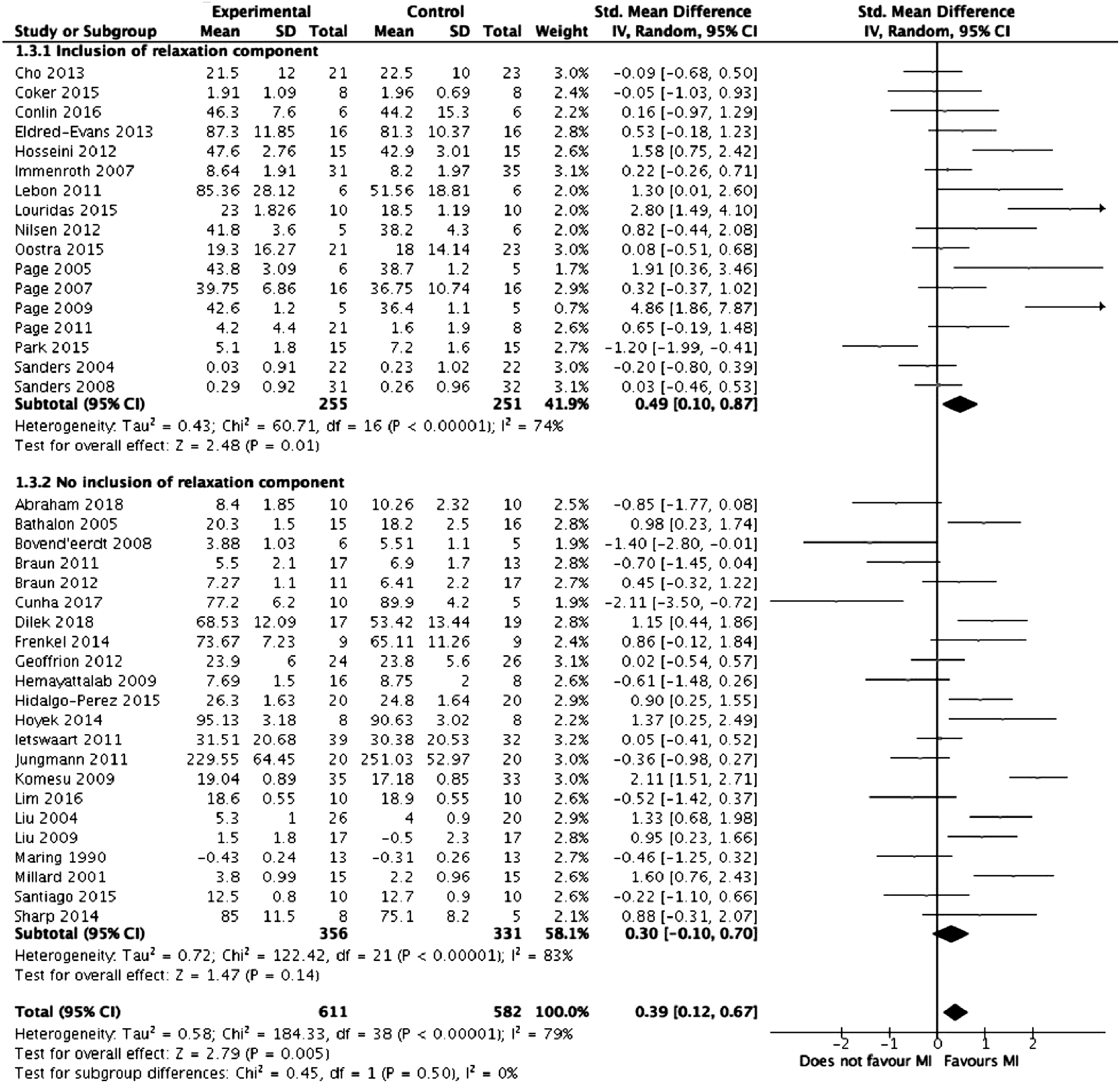
In 22 studies,11,12,24,25,27,29,32,41,42,44,47,48,50,51,53,58,59,61,65,66,69,77 the MI sessions began with a brief period of relaxation lasting <5 minutes. Out of these, 13 of them found the intervention group performed better than control.12,25,32,50,51,53,58,59,61,65,66,69,77 In 7 studies, there was explicit mention of the use of sensory cues for visualisation, giving an indication of the specificity of the instructions given to participants.3,31,39,51,59,65,69 The level of detail to which the protocols were reported was not consistent across the studies reviewed. In 13 studies, the MI sessions included several repetitions of MI with periods of rest in between.40,42,43,51,53,55,57,58,60-62,68,75 Out of these, 10 found the intervention performed better than control.51,53,55,57,58,60-62,68,75 7 studies mention a refocusing period at the end of the MI session.42,51,59,61,65,69
Secondary Outcomes: Motor Imagery Ability Assessment
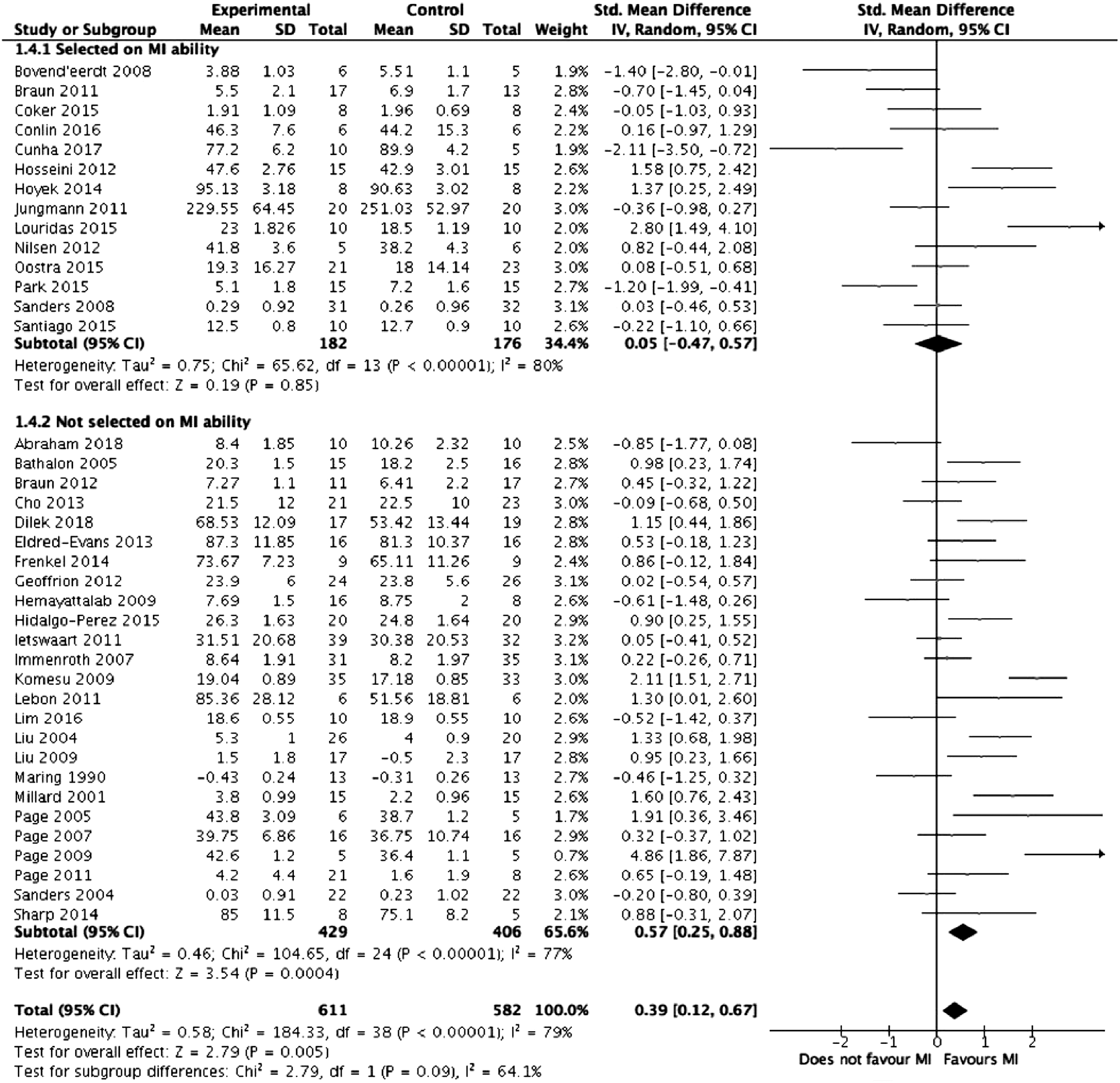
Certain studies measured participant ability to conduct MI, as MI ability differs in a healthy population, 80 and can be measured using validated imagery questionnaires, such as the Mental Imagery Questionnaire (MIQ), the Mental Imagery Questionnaire Revised, Second Edition (MIQ-RS) or the Vividness of Mental Imagery Questionnaire (VMIQ). 81 In patients who have a neurological impairment, the Kinaesthetic and Visual Imagery Questionnaire (KVIQ) 82 can be used, as can mental chronometry, which has been shown to correlate with MI ability in healthy and non-healthy patients. 23 studies (38%) used the MIQ, MIQ-RS, VMIQ, VMIQ-2, VVIQ, mental chronometry, KVIQ or time-dependent motor imagery (TDMI) to select participants based on MI ability.6,12,24,34,38,40-43,45,47,48,53,55,57,60-62,64,66,68,72,79 Out of these, 12 (52%) reported better outcomes in the intervention group compared to control.12,53,55,57,60-62,64,66,68,72,79
Meta-analysis
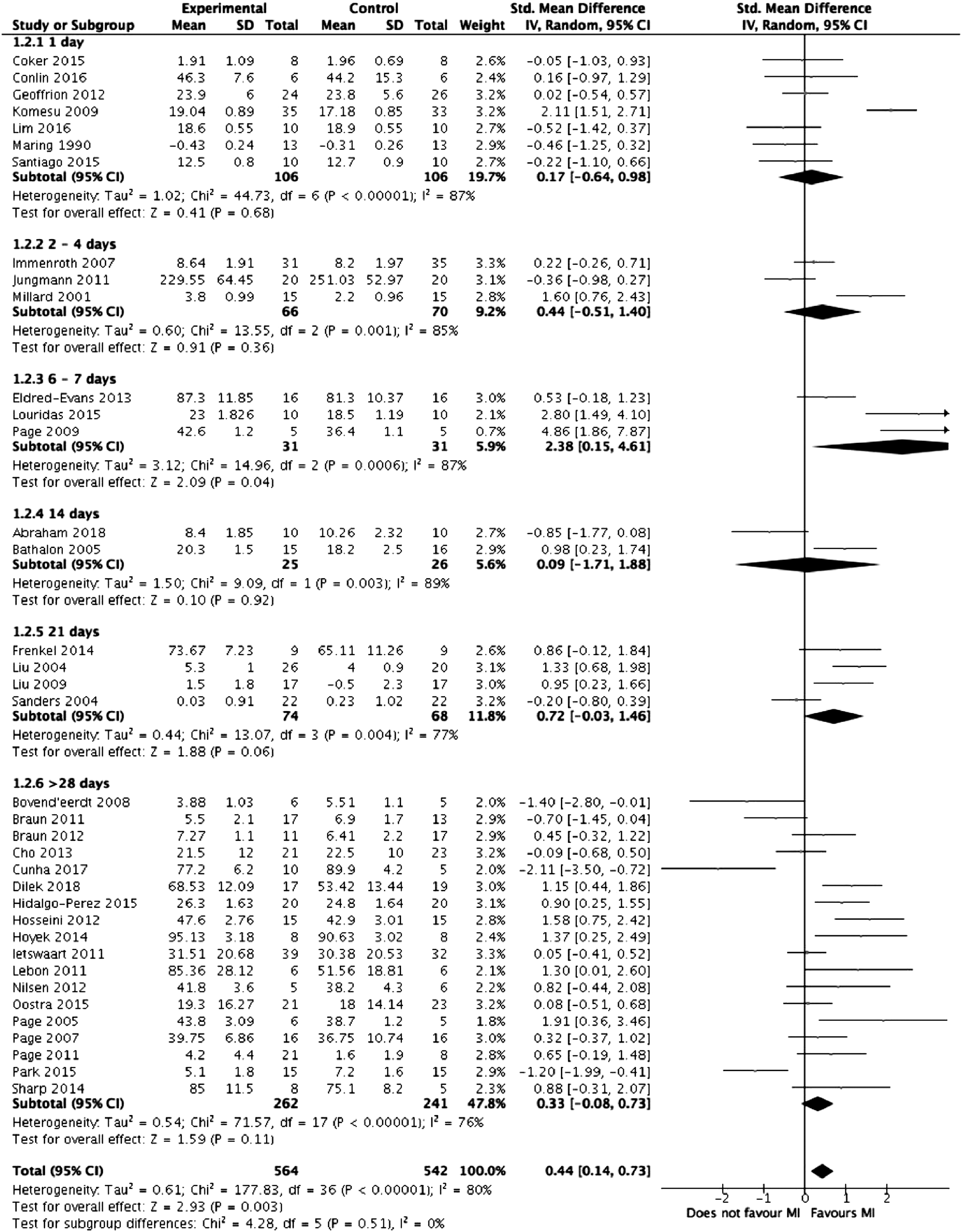
Meta-analysis was performed on the 39 studies eligible for inclusion. Figure 2 summarises the results of the meta-analysis. Overall, mental imagery was associated with improved outcomes (z = 2.79, P = .005) but with high heterogeneity between the studies (I2 = 79%, P < .00001). Figures 3-5, respectively, detail the results of subgroup analyses based on length of training, relaxation and selection of participants based on MI ability. Forest plot comparing mental training interventions to control. Forest plot comparing mental training interventions of 1 day, 2-4 days, 6-7 days, 14 days, 21 days and >28 days duration. Forest plot comparing mental training interventions with a relaxation component to mental training interventions with no relaxation component. Forest plot comparing studies where participants were selected based on mental training ability to studies where participants were not.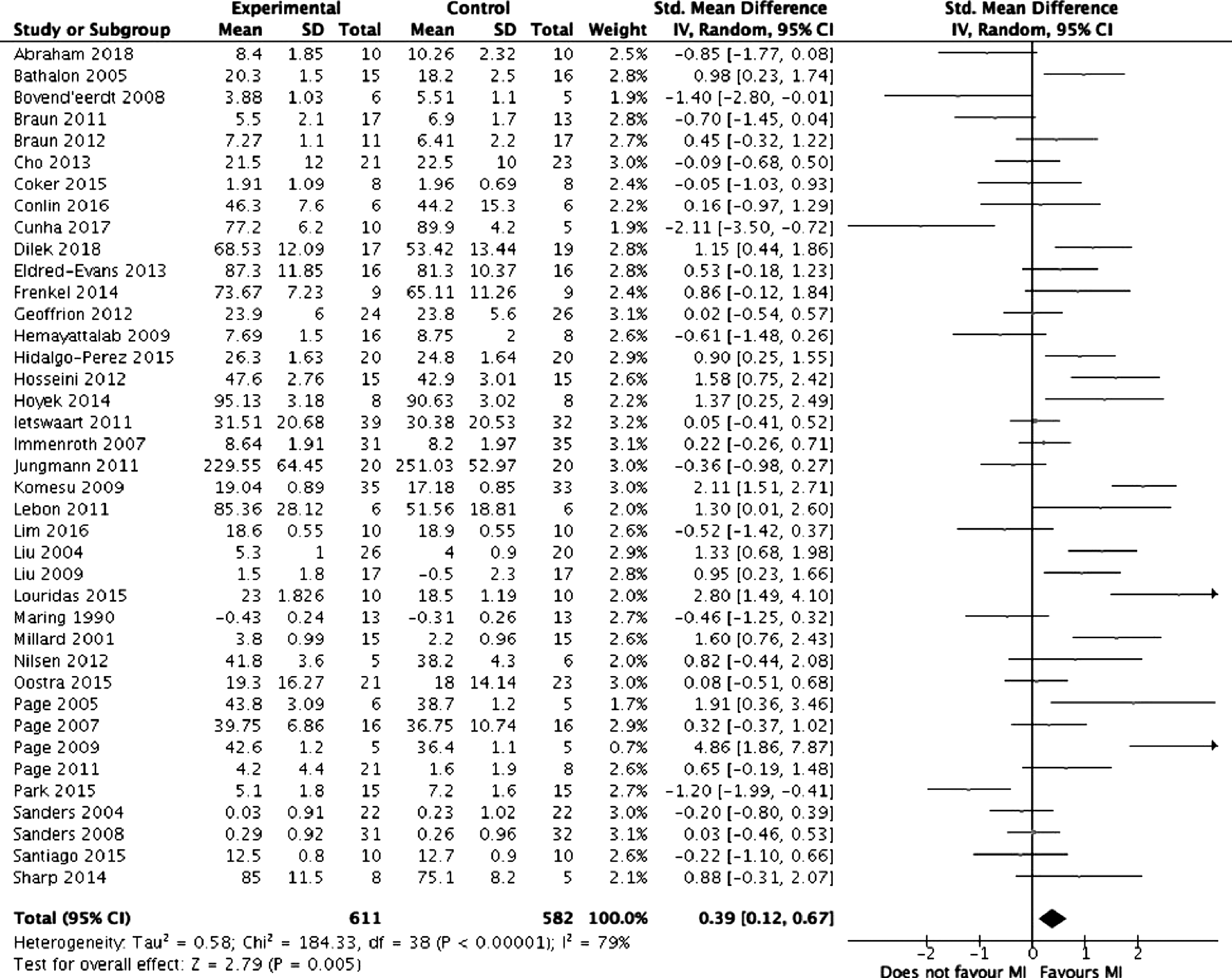
Risk of Bias Assessment
Risk of Bias.
Discussion
This review assessed only RCTs evaluating the effectiveness of various MI protocols across the fields of sports, neurorehabilitation, education and medical education. The aim was to extract the components of a successful MI protocol. The authors hypothesised these components might be universal to MI training applied to several different indications, hence the inclusion of a heterogeneous sample of studies. In addition, MI programmes for surgical training remain novel, with few studies having specifically evaluating its effectiveness on surgeons. Broadening the search across several disciplines allowed protocol components never included in surgical training programmes to be considered.
Performing MI in addition to standard rehabilitation or training led to improvements in the majority of trials (83%).This is consistent with the concept that MI is a valuable tool when added to existing training. Based on current understanding of the neurological processes of MI, it can be speculated that protocols which demonstrate improvement in non-surgical fields can be extrapolated to surgical training, due to the fact all are focussed on motor skill learning. This could be particularly true for healthy populations improving on a specific skill - such as athletes. Surgical trainees and athletes have in common a healthy physical baseline and the goal of improving a specific motor skill. However, the authors acknowledge the methodological limitation of assuming similarities between populations. Overall, there were very few studies which specifically tested MI skills in surgical residents; this is a novel method of training in this field which must be tested further. This method could be used to improve a range of motor skills, ranging from generic surgical skills to patient-specific skills. Motor imagery-based training could be a supplement to standard surgical training.10,31
Studies where the intervention group performed better than control on outcomes had a median duration of intervention of 30 minutes, with a median of 15 MI sessions completed in 26 days. This is equivalent to performing MI more than once every 2 days. An online surgical training course, where trainees conducted a short amount of imagery, regularly and at their convenience, would fit these requirements. Indeed, there were 712,27,30,52,55,60,74 studies in which subjects were instructed to perform MI independently at home and record their progress. In the study by Louridas et al, 12 surgical trainees were given 7 days to perform MI at home and had follow-up calls and feedback. Only 2 of these 7 studies, by Jungmann et al 30 and Mulla et al, 27 did not see an improvement in the intervention group compared to control. They were also the only 2/7 studies which used medical students as their population. This means a MI training protocol for surgical education could be in a format which allowed subjects to access training in their own time.
Regarding the content of MI interventions, the level of detail provided across the studies review varied widely, making direct comparisons of protocols and associated outcomes difficult. However, the following elements could be incorporated into the structure of MI protocols in the interest of standardising their format and enabling direct comparison of outcomes in future research: a period of relaxation <5 minutes long prior to starting MI proper; detailed instructions involving specific sensory cues, a predetermined number of sets of repetitions of MI to be performed in each session and a refocusing period to close the MI session.
Given that there was no association between MI ability and technical performance (when compared to control), this indicates that baseline MI ability may not be an important factor for a MI training programme.
Given the heterogeneity of study outcomes measured and the variability of populations studied, no extrapolation can be made of the primary outcome most suitable for measuring the effectiveness of an MI training protocol. Relevant to surgical education MI training, a variety of primary outcome measures were used amongst the medical student and resident populations. These were variations of a pre-established checklist and objective measurements such as time and accuracy.
In 9 of the studies24,27,29,30,34-36,39,40 where the intervention group performed worse or equivalent to the control group, subjects were students or healthy participants for whom the benefit of the study was not obvious: they did not have an intrinsic motivation to perform well on the outcomes measured such as increased function of a limb following a stroke or improved surgical technique. This may indicate that for MI interventions to be successful, participants need to be self-motivated, and in the context of surgical education, surgeons should only undergo MI training if they see potential benefit in it. However, this is difficult to establish in the heterogeneous group of studies reviewed here and would benefit from further research focussed on surgical trainees’ motivation to use MI with their performance after training. Guillot’s article did explore the relationship between intrinsic motivation and MI in the opposite direction and suggests that MI does enhance intrinsic motivation. 16
A number of limitations to these results need to be considered. The majority of the studies were intrinsically biased as the subjects who received the intervention could not be blinded. Another limitation is the heterogeneity of studies included in this review. Studies included represented many applications of MI training, which may limit the generalisability of findings. Only 12 studies focussed on the application of MI training directly to surgical trainees or medical students. Further research is required to demonstrate that the findings from this review can be translated to surgical education. Furthermore, variations in study methodologies limited pooled analysis.
Following this review, more research focussing on the implementation of MI training protocols in surgical education is needed, in addition to the acceptability of such training measures among trainees and surgeons. The results of this review may aid in constructing a purpose-built MI training programme to evaluate its efficacy on surgical trainees specifically.
Conclusions
This comprehensive systematic review and meta-analysis has identified several characteristics linked to successful MI training in sports or neurorehabilitation that can be used to construct MI training protocols for use in surgical education. It must be highlighted that this review and analysis included a wide range of studies in different fields. However, certain components found to be linked to successful programmes could be extrapolated to surgical training, based on current understanding of neurological processes of MI. A successful MI training programme could be delivered in parallel to existing surgical training, in a flexible format allowing surgeons to undertake several MI sessions in a self-directed manner. A single MI session conducted by a senior surgeon could include a brief period of relaxation, followed by several sets of repetitions of MI, and a refocusing period. Providing guidance on the construction of effective MI training protocols will allow replicability of trials investigating the best way to deliver MI training. This is a step towards the development of a surgical MI training programme, as a low-cost, low-risk tool to enhance practical skills. Further research will be required to evaluate the use of MI in a purpose-built surgical training programme.
Footnotes
Author Contributions
Study concept and design: Mary S. L. Goble and Nicholas Riason
Acquisition of data: Mary S. L. Goble and Ayah Mekhaimar
Analysis and interpretation: Mary S. L. Goble, Nicholas Riason, and Kamran Ahmed
Study supervision: Nicholas Riason, Kamran Ahmed, and Prokar Dasgupta
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant awarded from the Royal College of Surgeons. The funders had no involvement in the study design, the collection, analysis and interpretation of data; in the writing of the report and in the decision to submit the paper for publication.
Appendix A
Detailed Search Strategy
PubMed
((‘Motor imagery’) OR (‘mental imagery’) OR (‘mental practice’) OR (‘mental training’)) AND ((‘randomised controlled study’) OR (‘randomised controlled trial’))
265 results
Ovid (PsycINFO, Embase and MEDLINE)
((Motor imagery) OR (mental imagery) OR (mental practice) OR (mental training)) NOT (computerised OR computer)
Filter: Randomised controlled trial
191 results
Appendix B. List of Abbreviations Used in Tables 1 and 2.
ACL
Anterior cruciate ligament
AMIT
Advanced Mechanical Technology Inc
BT
Box training
CMIT
Constraint-induced movement therapy
EMG
Electromyography
FAT
Frenchay arm test
FM
Fugl-Meyer assessment test
GRS
Global Rating Scale
IST
Intelligence Structure Test
IVI
Internal visual imagery
KG
Kinesiology
KIN
Kinaesthetic imagery
KVIQ-20
Kinaesthetic and visual imagery questionnaire 20
LBT
Line bisection test
MABC
Movement Assessment Battery for children
MCTE
Motor control therapeutic exercise
MI
Mental imagery, motor imagery
MIQ-RS
Motor Imagery Questionnaire-Revised
MMSE
Mini-mental state examination
MP
Mental practice
n/a
Not available
OSATS
Objective Standard Assessment of Technical Skills
OT
Occupational therapy
PP
Physical practice
SCT
Star cancellation test
SI
Stretching imagery
TDMI
Time-dependent motor imagery
VMIQ-2
Vividness of Movement Imagery Questionnaire 2
VR
Virtual reality
VRS
Virtual reality simulation