
Abstract
Background: The transition from surgical residency to independent practice is a challenging period that has not been well studied. Methods: An email invitation to complete a 55-item survey and the Maslach Burnout Inventory–Human Services Survey (MBI-HSS) was sent to early career general surgeons across Canada. The chi-square test or Fisher’s exact test was used to compare demographic and survey characteristics with burnout. Multivariable logistic regression was performed. Results: Of the 586 surgeons contacted, 88 responded (15%); 51/88 surgeons (58.0%) were classified as burnt out according to the MBI-HSS. Most surgeons (68.2%) were not confident in their abilities to handle the business aspect of practice. The majority (60.2%) believed that a transition to independent practice program would be beneficial to recent surgical graduates. Conclusions: Our data showed high prevalence of burnout among recently graduated general surgeons across Canada. Further, respondents were not confident in their managerial and administrative skills required to run a successful independent practice.
Introduction
Within North America, medical trainees must successfully complete a residency program and in some cases, pursue fellowship training before they can start practicing as an attending staff in independent practice. 1 This transition from trainee to staff physician may be stressful and overwhelming.2,3 Within a short period of time, staff physicians are faced with multiple challenges such as adapting to a new setting with new colleagues, taking on the role of primary clinical decision maker, and managing non-clinical tasks such as teaching, research, financial planning, and their personal lives. The issues affecting recent graduates during this stressful transition period have been sparsely covered in the literature, and none of the published studies resulted in an empirically founded conceptual framework.4-10 The American College of Surgeons has recognized this and focused efforts toward creating transition to practice programs to better equip residents for a smoother transition. 11
Recent studies also highlight the growing problem of burnout in medical practitioners. 12 Within general surgery, rates of burnout are significant and may manifest with symptoms of depersonalization, emotional exhaustion, and reduced personal accomplishment. 13 Physician burnout is a serious area of concern as it has been correlated with low morale, personal dysfunction, insomnia, physical exhaustion, personal problems, poor performance, and deterioration in quality of medical care.14,15 In addition, both depression and burnout have been associated with major medical errors. 16 Of note, studies have demonstrated that burnout develops as early as medical school and continues throughout residency.15,17
Considering the potential increase in stress during the transition from residency or fellowship training to independent practice, we hypothesize that this subset of surgeons may have particularly greater prevalence of burnout. 13 Furthermore, most residency training programs focus on competencies and skills development in the residency curriculum. This leaves little or no teaching on the other aspects of career management including the administrative and business responsibilities of medical practice. The aims of this research were twofold. First, we sought to assess issues affecting new graduates of general surgery programs within Canada, particularly their perception of their ability to manage an independent practice. Second, we assessed the prevalence of burnout among this subset of general surgeons.
Methods
After obtaining institutional research ethics board review, a study invite was sent out via email to early career general surgeons across Canada asking them to complete a cross-sectional survey accessible through a provided URL from www.fluidsurvey.com. The names and contact information of surgeons were obtained from the database of surgical graduates participating in the annual General Surgery Review Course in Toronto, ON. This included surgeons who had graduated between 2007 and 2012 from a general surgery residency program in Canada. The survey was composed of 55 questions covering demographic factors, issues regarding independent practice, surgeons’ perception of their roles, responsibilities, and training preparation. We also included the validated Maslach Burnout Inventory–Human Services Survey (MBI-HSS). 18 Three iterations of the invitation emails were sent with 2-week intervals in between each. The completion and submission of the survey indicated implied consent for the data to be used in the study.
The demographic characteristics section of the survey was constructed by referring to several papers assessing burnout in healthcare providers,19-22 especially Soler et al, Balch et al, Napolitano et al, and Friedell et al. The MBI-HSS is the most widely used measure of burnout for healthcare professionals. It has been extensively tested for its reliability and validity since its creation in the early 1980s. Consequently, the MBI-HSS has become the gold-standard tool for burnout assessment and was selected for this study based on its strong psychometric properties. The MBI-HSS is a 22-item self-report questionnaire that measures three dimensions of the burnout syndrome: emotional exhaustion (EE), depersonalization (DP), and reduced personal accomplishment (PA). The response for each question is a 7-item Likert scale ranging from 0 (never) to 6 (everyday). For each dimension, the total score is calculated by summation of its questions and then classified into “low,” “moderate,” and “high” categories based on the cutoff scores outlined in the MBI-HSS interpretation guidelines. There is considerable heterogeneity in how studies define burnout syndrome. 23 For this study, we classified participants with high EE (score ≥27) or high DP (score ≥13) as having burnout.
We described demographic, survey, and burnout characteristics for all participants. Categorical variables were described as numbers and percentages. The chi-square test, or Fisher’s exact test as appropriate, was used to compare demographic and survey characteristics with burnout. Missing responses for question components related to EE or DP were assigned a score of 3. A sensitivity analysis was conducted assessing the impact of missing response score assignment on classification of burnout.
Multivariable logistic regression of the association of demographic and survey characteristics with burnout was performed utilizing the screening variable selection method. First, we selected covariates with a P-value of .25 or less on bivariate analysis, with burnout as the outcome variable. Second, we selected variables with the highest chi-square value, for the greatest number of variables allowed by the convention of one independent variable for every 10 events (or non-events, whichever is smaller). Third, we constructed a full model and verified model assumptions. P-values less than .05 were considered statistically significant. All statistical analyses were performed with SAS Studio 3.6 (SAS Institute, Carty, NC).
Results
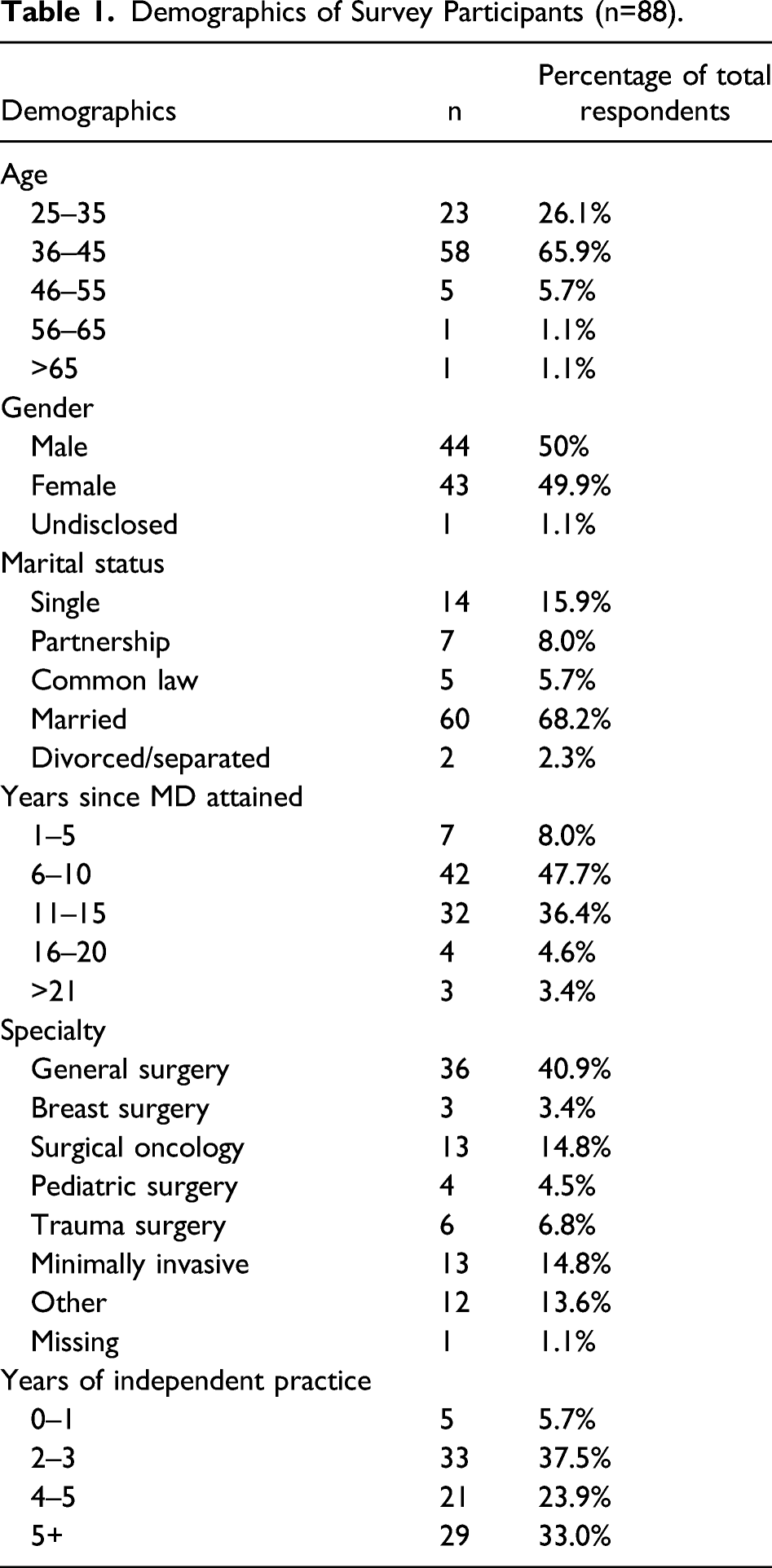
Demographics
Demographics of Survey Participants (n=88).
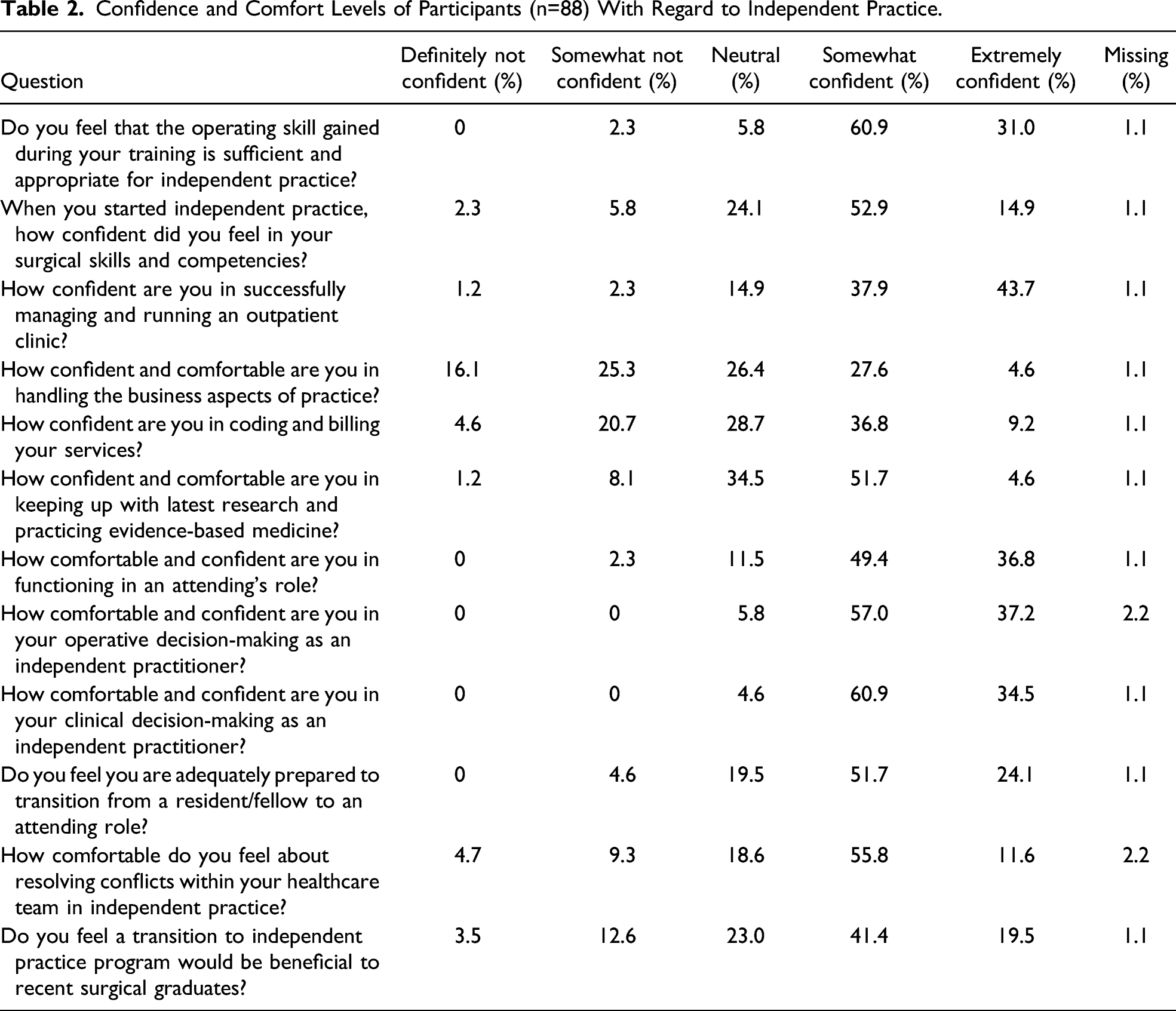
Confidence and Comfort in Independent Practice
Confidence and Comfort Levels of Participants (n=88) With Regard to Independent Practice.
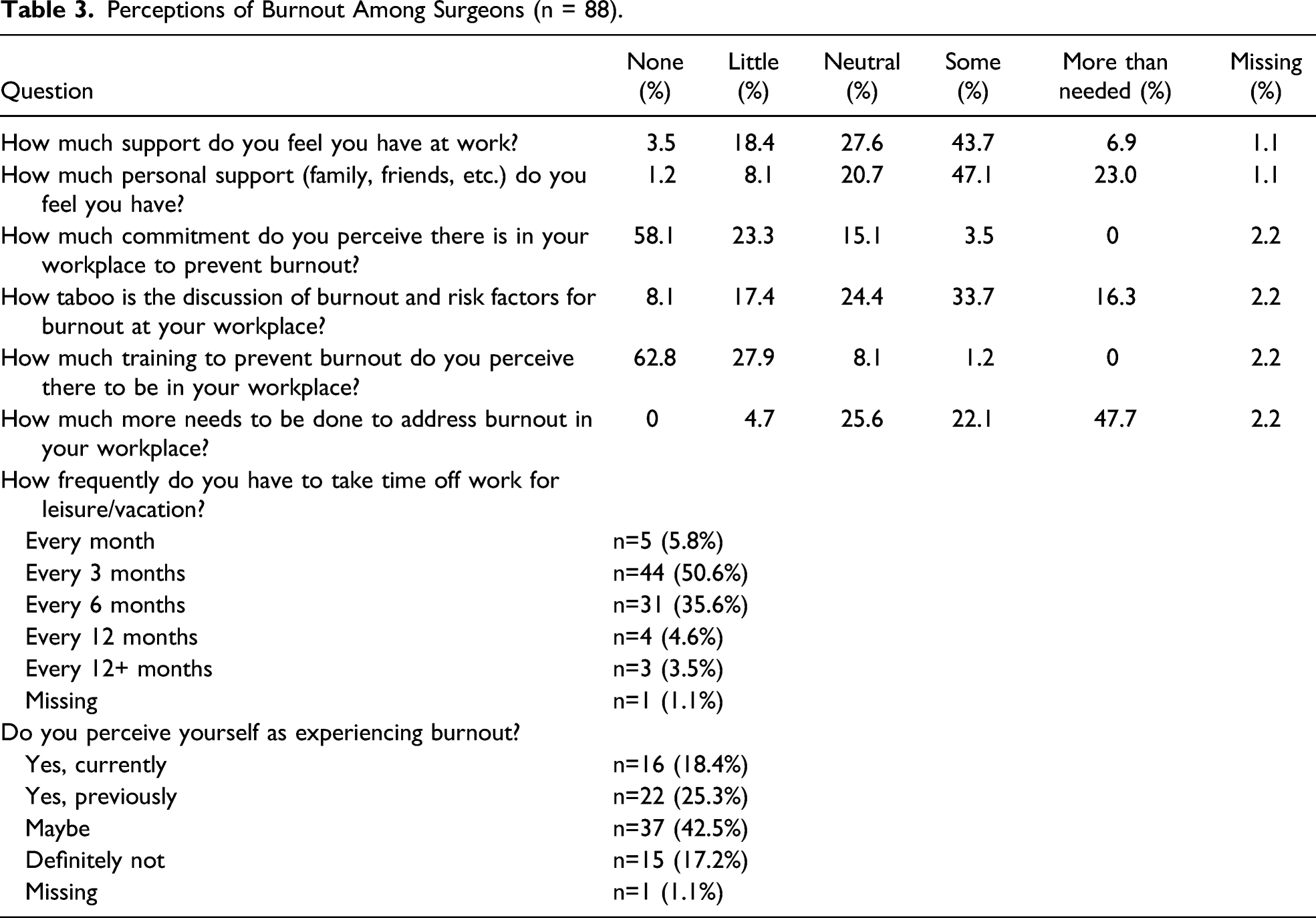
Perceptions of Burnout
Perceptions of Burnout Among Surgeons (n = 88).
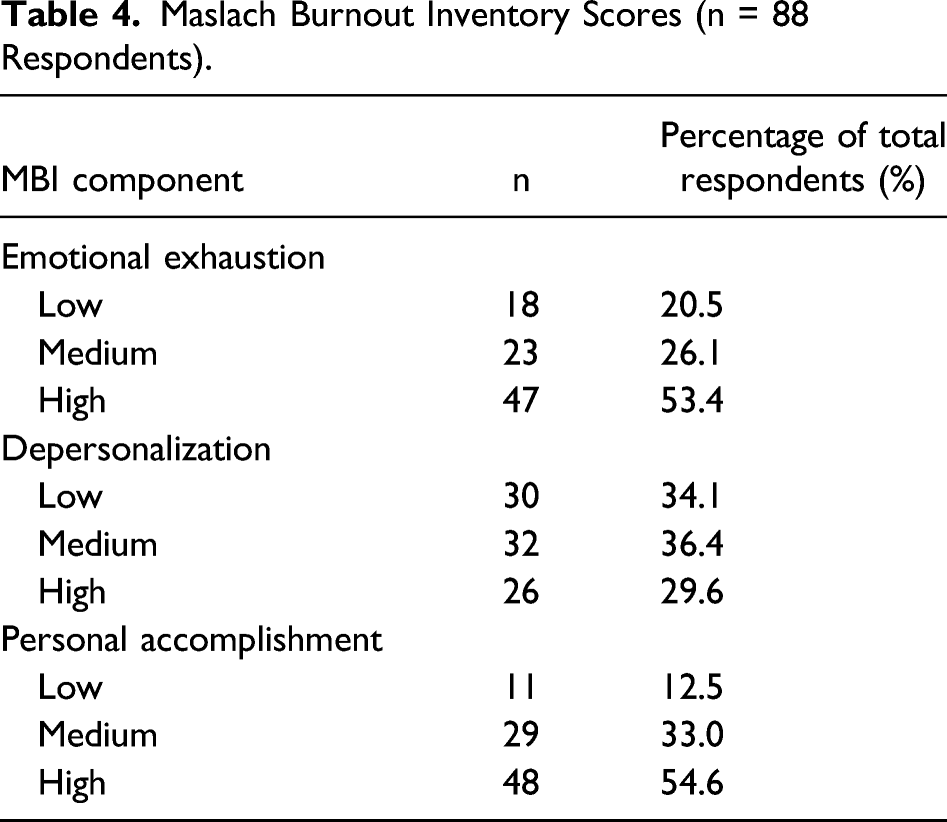
Maslach Burnout Inventory Scores
Maslach Burnout Inventory Scores (n = 88 Respondents).
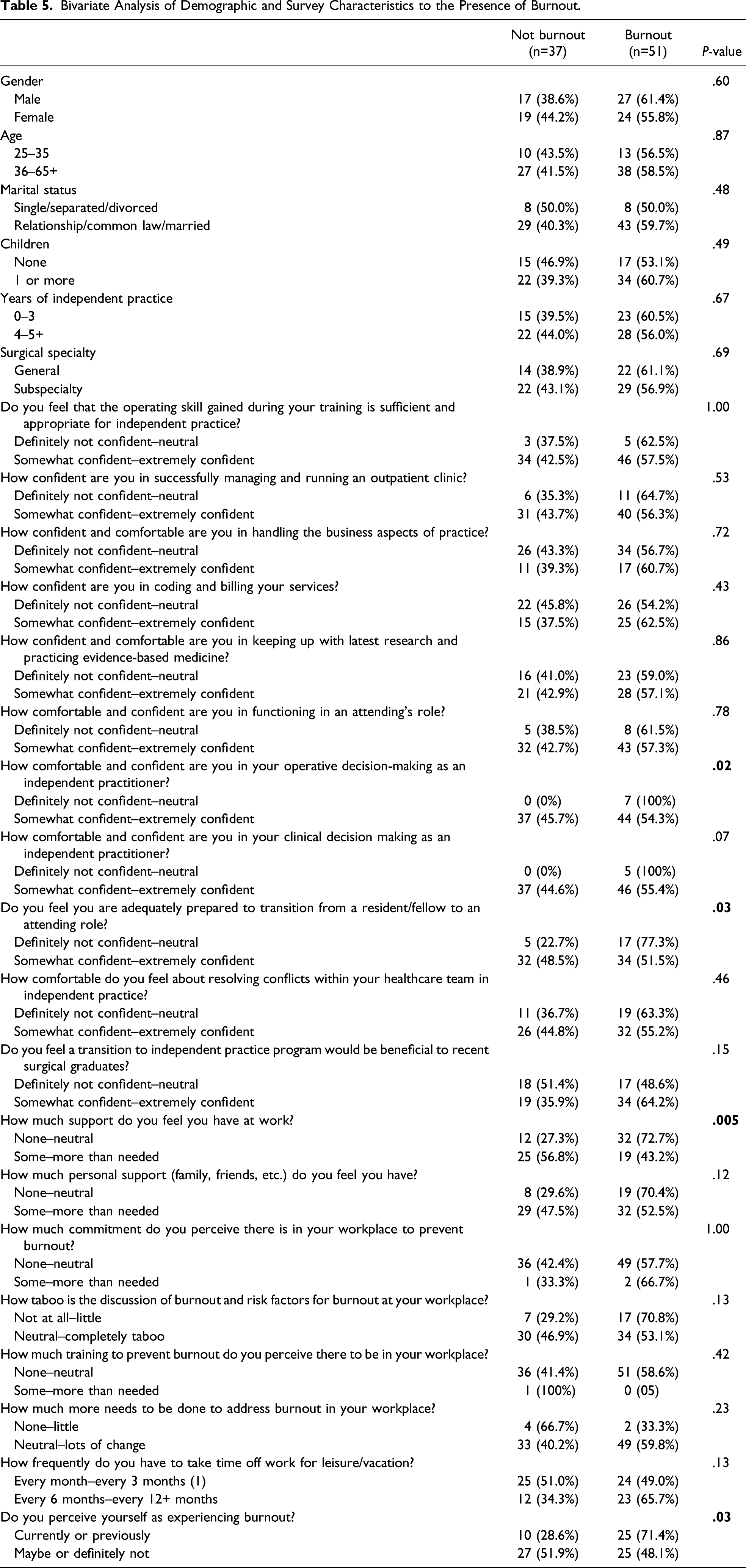
Bivariate Analysis of Demographic and Survey Characteristics to the Presence of Burnout.
Association of Demographics and Survey Characteristics With Burnout
There was no difference in burnout by gender, age, marital status, having children, years of independent practice, or by general surgical sub-specialty (Table 5). Factors associated with burnout included lack of confidence in operative decision-making as an independent practitioner (P=.02), lack of confidence in preparation to transition from a resident/fellow to an attending role (P=.03), lack of support at work (P=.005), and self-perception of currently or previously experiencing burnout (P=.03). Of the 35/87 surgeons (40.2%) from our study who perceived themselves as being burnt out, 25 surgeons (71.5%) met the criteria for burnout based on the MBI. Contrarily, of the 52/87 surgeons who were either unsure or not confident about experiencing burnout, 25 surgeons (48%) met burnout criteria.
Multivariable Logistic Regression Analysis of the Association Between Survey Characteristics and Burnout.
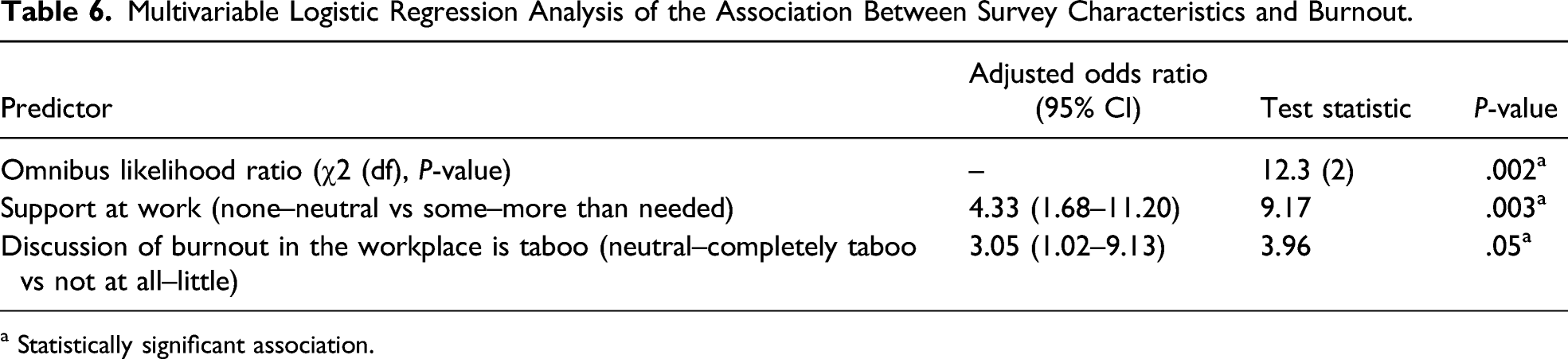
a Statistically significant association.
Discussion
Over half of the surgeons from our study were classified with burnout based on their responses to the MBI-HSS, although many did not identify or recognize this. This is in line with findings by Bucholz et al 24 from a national survey of 4136 American general surgery residents. Although, our data did not highlight any sex-based differences in burnout rates, likely due to a small sample size, a higher prevalence amongst female surgeons has been clearly demonstrated by various authors.13,25-27 Furthermore, in the national survey of American general surgery residents conducted by Elmore et al, those who voluntarily left their training programs cited the lack of a mechanism to discuss their personal and professional concerns without fear of reprisal as a contributing factor for burnout and their decision to change careers. Our data corroborate the aforementioned finding and warrant further implementation of institutional interventions to raise awareness as well as prevent and address burnout in the workplace setting.12,28
Our study also found that early career general surgeons did not receive sufficient training in easing their transition to independent practice. Of note, De Montbrun et al 29 showed that experiences during this transitional period are crucial in the growth and professional development of recently trained attending staff. Strikingly, while the majority of surgeons in our study felt confident with their technical skills and ability to operate in an attending’s role, only a minority was confident in their ability to successfully manage and run an outpatient clinic independently. Similar to our findings, Klingensmith et al 30 have demonstrated a strong desire and need from general surgery residents in the United States for training on surgical practice administration such as coding and reimbursement, patient billing, and taxes. Hashimoto et al 31 have also pointed toward lack of increased resident autonomy as being one of the factors hindering a smooth transition to independent practice.
This study represents the largest study on burnout among general surgeons at the start of their surgical careers. Although much focus has been placed on facilitating the transitions in other training periods (eg, from medical school to residency), no study to our knowledge has focused on the later end of the surgical training and early career period. Similar to a surgical boot camp for medical students entering surgery training, perhaps residency and fellowship programs may address their final year trainees to ensure they are adequately equipped to transition into independent practice. The American College of Surgeons has recognized this and focused efforts toward creating transition to practice programs to better equip residents for a smoother transition.11,32 However, long-term outcomes and utility of such curricula need to be further assessed.33,34 Wakeam et al has also suggested a practice-sharing model for surgeons early in their career. 35 In this model, senior surgeons close to their retirement may mentor and train the incoming new graduate for a few years, which may help alleviate some of their stress.
A limitation of our study is the relatively small sample size of 88 surgeons across Canada. This may call into question the study’s external validity and generalizability of our findings. Although the sample size is smaller than desired, we did have a diverse population representative of many training programs. Furthermore, our study included both general surgeons as well as subspecialty surgeons practicing in both community and academic settings. Although our survey data illustrate the various types of subspecialty vs general surgeons, we do not know the distribution of the participants based on the type of practice setting (community or academic). This variable may have provided further context to our findings as these practice settings may certainly yield different issues and potential stressors for participants. A final limitation of the study, as with any survey study, is that the value of the collected data solely depends on how accurately and truthfully the participants responded to questions in the survey. In general, survey studies assume the data collected to be legitimate and reflective of the participants’ true beliefs; however, this might not always be the case. Larger studies focusing on the aforementioned drawbacks are warranted.
Our findings provide some insight into the factors contributing to burnout amongst the recently graduated general surgeon population. Since burnout adversely effects physician–patient interactions and is associated with higher economic costs (as a result of higher absenteeism, job turnover, and quality control issues), the goal in preventing or mitigating burnout is to improve not only physicians’ quality of life but also patient care.36,37 Future directions for research include focusing on at risk populations to identify measures necessary to reduce burnout and ease the transition of surgical graduates to independent practices.
Conclusion
Our data showed high prevalence of burnout amongst recently graduated general surgeons across Canada. During the transition phase to independent practice, although most surgeons felt satisfied with their surgical skills, they were not confident in their managerial and administrative skills required to run a successful independent practice. Addressing these issues in surgical training programs may be beneficial for future surgeons.
Footnotes
Author contributions
Study concept and Design: Dr. Mohammed Firdouse, Dr. Tulin Cil, Dr. Jaime Escallon, Dr. Sandra de Montbrun
Acquisition of Data: Dr. Mohammed Firdouse, Caitlin Chrystoja
Analysis and Interpretation: Dr. Mohammed Firdouse, Caitlin Chrystoja, Dr.Tulin Cil
Study Supervision: Dr. Tulin Cil, Dr. Jaime Escallon, Dr. Sandra de Montbrun
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The primary author (MF) received funding as a part of the Comprehensive Research Experience for Medical Students (CREMS) program at the University of Toronto, ON, Canada.