
Abstract
Background & Aims. Postoperative weight loss is common following hepato-pancreato-biliary (HPB) surgical resections; however, the extent of weight loss and the association with poor outcomes have not been well described. We assessed the average percentage of weight loss and risk factors associated with sustained postoperative weight loss. Materials and Methods. We enrolled patients undergoing major HPB surgical resections from 2011–2016 at a single institution. We evaluated percent change in weight postoperatively, incidence of complications, and nutritional clinical markers at 1, 3, and 6 months postoperatively compared to preoperative baseline. We used multiple logistic regression to evaluate factors associated with significant weight loss (>10% from baseline) at 3 months from surgery. Results. Among 262 patients undergoing HPB surgery, liver surgery patients lost 2.5% of baseline weight at 3 months postoperatively but regained baseline weight by 6 months. Pancreatic surgery patients lost 7.7% at 3 months and were unable to recover their baseline weights at 6 months. Forty-three (16%) patients had major postoperative complications including abdominal abscess (5.3%) and anastomotic leak (3.8%). Patients who experienced major postoperative complications had a greater percentage weight loss at 3 months compared to those without major complications: median 11% (interquartile range (IQR): 7%–15%) vs 4% (IQR: 0%–8%), P < .001. In the multivariable analysis, major postoperative complications were associated with significant weight loss at 3 months (OR 3.39, 95% CI 1.38–8.33). Conclusions. Due to the association of weight loss and major postoperative complications, patients who experience significant weight loss (>10% from baseline) may benefit from nutritional assessment for dietary intervention.
Introduction
Many patients undergoing hepato-pancreato-biliary (HPB) surgical resections suffer from cancer cachexia. 1 Cachexia is defined as anorexia and malnutrition due to changes in gastrointestinal function. It is exacerbated by loss of muscle and adipose tissue due to increased metabolism. 2 The mechanism of cachexia is poorly understood but may be attributable to a negative protein balance from reduced oral intake, alteration of host energy metabolism due to production of pro-inflammatory cytokines, and acute-phase reactions that result in protein degradation.3,4 Preoperative factors such as body mass index (BMI) and cachexia have been identified as potential risk factors for postoperative complications.5-7 Patients with either low or high body fat and those with tumor cachexia may be at higher risk of postoperative complications and mortality.2,8-10
Many of the factors that contribute to preoperative weight loss can contribute to sustained cachexia postoperatively. For instance, patients undergoing pancreatectomies are at an increased risk of both preoperative and postoperative weight loss. 1 Diabetes mellitus and exocrine insufficiency are common comorbidities among patients with pancreatic malignancy, which can lead to malnutrition and vitamin deficiency. 11 It is thought that over 50% of patients with pancreatic malignancy lose over 5 kg of body weight prior to surgery. 12 Small studies have also suggested that these patients continue to have difficulty regaining weight following surgery, with an average weight loss of 6.8 kg at 3 months after surgery. 13 This weight loss is thought to be due to insufficient calorie intake associated with fat avoidance, exocrine insufficiency, or cancer recurrence. 13 After pancreatectomy, the percentage of patients suffering from exocrine insufficiency increase to 80%, which contributes to further muscle wasting.14,15
Weight loss after hepatectomy is poorly described in the current literature, with a small number of studies examining weight loss as a secondary outcome in these patients. One retrospective chart review involving 21 patients found a 4.7% weight loss among patients undergoing open hepatectomy compared to a 2.8% weight loss among patients undergoing minimally invasive hepatectomy. 16 Preoperative weight loss and decreased preoperative albumin <35 g/L have been proposed as risk factors for postoperative intra-abdominal infections; 17 however, the association between postoperative weight loss and postoperative complications is not well described.
Although there is convincing evidence that preoperative weight loss and cachexia might be associated with worse postoperative outcomes, the association between postoperative weight loss and postoperative complications is less clear. A better understanding on the magnitude of weight loss after HPB surgical resections would support early interventions for nutritional support among patients who experience major postoperative complications. Therefore, we have endeavored to quantify the magnitude of weight loss at 3 months following HPB surgical resections. Furthermore, we wanted to examine the association between markers of cachexia, including weight change and clinical biomarkers, and its association with postoperative complications.
Materials and Methods
Patient Population
The sampling set for this retrospective cohort study was patients ≥18 years of age who underwent hepatectomy or pancreaticoduodenectomy at a high-volume tertiary care center from 2011 to 2016. Multivisceral resections were included. Data collected included demographics (age and sex), type of surgery (pancreaticoduodenectomy, hepatectomy, or other biliary procedures), indication for surgery, preoperative and postoperative weight, height, body mass index (BMI), length of hospital stay, and postoperative complications within 90 days. Patients without weights at 3 months were excluded and, by extension, patients who experienced mortality within 3 months were excluded from the analysis. Patients with both 3 months and 6 months weights were identified for further analysis. Data were extracted by trained personnel using a standard protocol and data abstraction form. Data were abstracted from the following sources: (1) patient’s electronic charts, (2) surgeon’s and anesthesiologist’s notes, and (3) oncology center follow-up records. Postoperative complications were categorized as minor and major according to Clavien–Dindo classifications. 18 Pancreaticoduodenectomies were performed open either with a classic or pylorus preserving technique. We elected to include both tehcniques to capture the full scope of pancreatic procedures at our institution. Hepatectomies were performed either open or laparoscopic depending on surgeon’s preference. All patients received preoperative antibiotics (cefazolin) and venous thromboembolism prophylaxis with unfractionated heparin prior to surgery and with low molecular weight heparin following surgery but not following hospital discharge. The study was approved by the regional ethics review board.
Patient comorbidities were classified using the Charlson comorbidity index. 19 The administration of chemotherapy was classified as neoadjuvant chemotherapy, which refers to administration of chemotherapy up to 6 months prior to surgery. “Adjuvant chemotherapy” refers to the administration of chemotherapy within 6 months from surgery. Baseline clinical and nutritional markers, such as white blood cell count (WBC) and hemoglobin, were collected within a month, and albumin was collected within 3 months prior to surgery date. Malignant pathology was defined according to the surgical pathology report. For those patients with malignant pathology report, a negative resection margin was defined as a margin >1 mm. 20
Weight and Body Composition and Patient Follow-Up
Weight was recorded preoperatively (i.e., baseline weight) as well as postoperatively at 1 month (±2 weeks) and at 3 and 6 months (±4 weeks) from index surgery. We defined clinically relevant postoperative weight loss as greater than 10% change in baseline weight, based on the definition of cachexia described by the SCRINIO criteria.2,12 We chose a criteria based on weight lost rather than BMI to ensure that the data are easy to interpret and apply clinically. Postoperative clinical and nutritional markers, including albumin, hemoglobin, and WBC, were measured during the same time period.
Statistical Analysis
Continuous variables are expressed as median and interquartile range (IQR) and categorical variables as counts and proportions. Since weight data were expected to follow a non-normal distribution and to have unequal variance of values across the participants, a non-parametric (distribution free) 1-way ANOVA Kruskal–Wallis test was performed to analyze the percent change in patient weight. Proportions were compared using the chi-square analysis. Univariable and multivariable analyses were performed using logistic regression to evaluate risk factors (age, preoperative weight loss, postoperative complications, type of surgery, and comorbidities) associated with clinically relevant postoperative weight loss (weight loss >10% compared to baseline) at 3 months after surgery. Missing data were assumed to be missing at random. All analyses were conducted by using R 3.5.1 (The R Foundation, Vienna, Austria). 21 This study was performed in accordance to the STROCSS criteria. 22
Results
Patient Demographics
Patient Demographics.
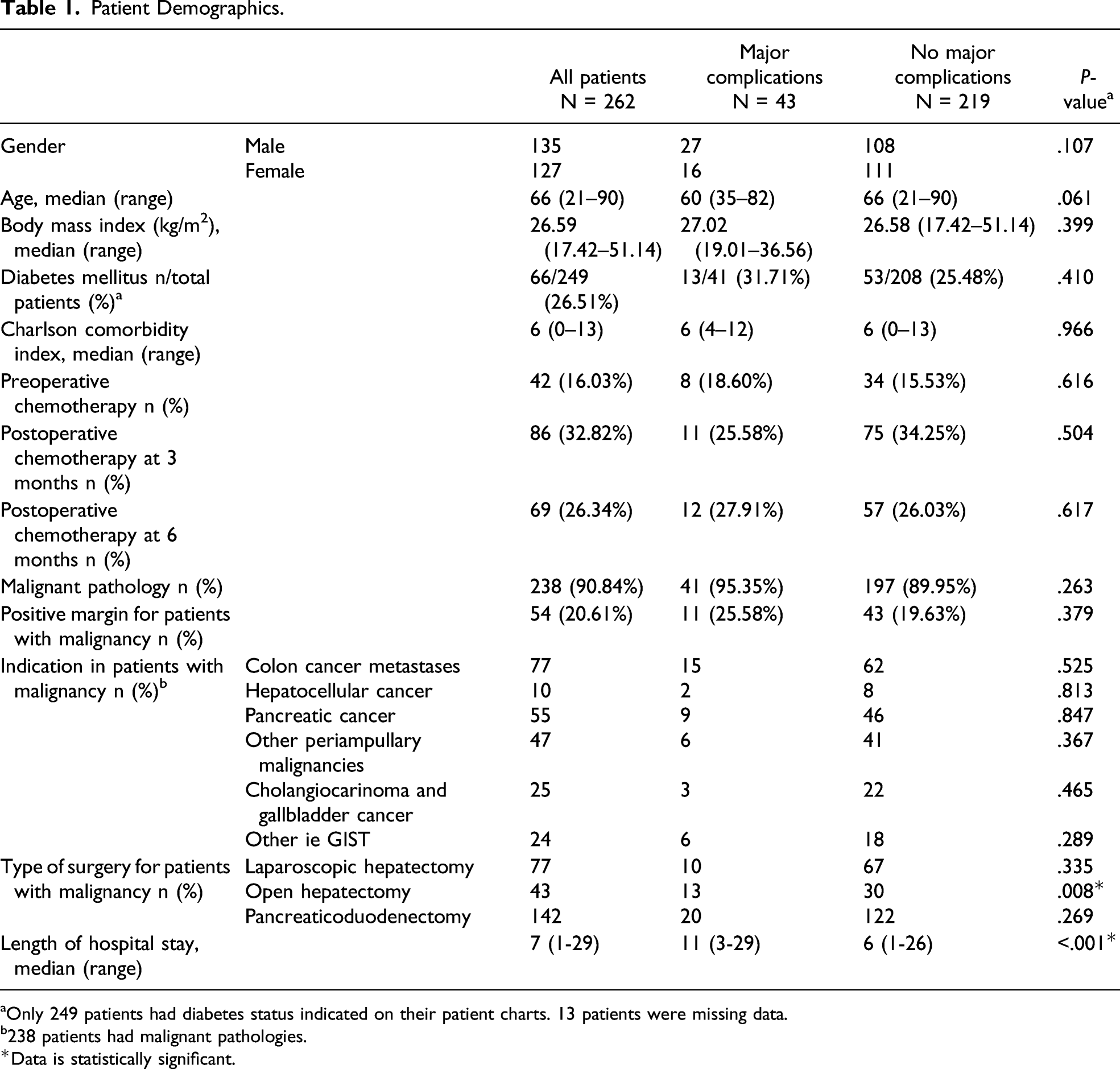
aOnly 249 patients had diabetes status indicated on their patient charts. 13 patients were missing data.
b238 patients had malignant pathologies.*Data is statistically significant.
Postoperative Weight
The median weight at baseline was 76 kg and at 3 months was 71 kg (P < .001). At 6 months, weight was 72 kg (P < .001). Patients who experienced major postoperative complications had a greater percentage weight loss at 3 months compared to those without major complications: median 11% (IQR: 7%–15%) vs 4% (IQR: 0%–8%), P < .001.
Patients were stratified into 4 groups, including pancreatic surgery with malignant pathology (N = 131), pancreatic surgery with benign pathology (N = 11), liver surgery with malignant pathology (N = 107), and liver surgery with benign pathology (N = 13). Figure 1 depicts the percentage change in weight from baseline in these 4 subgroups. Patients undergoing pancreatic surgery experienced a median 7.7% weight loss from baseline and were unable to recover baseline weights at 6 months follow-up. Patients undergoing liver resection had a median weight loss of 3.7% of their baseline weight at 1 month. By 6 months, the median weight was greater than the median baseline weight. Percentage change in weight from baseline, stratified into 4 groups: pancreatic surgery with malignant pathology, pancreatic surgery with benign pathology, liver surgery with malignant pathology, and liver surgery with benign pathology.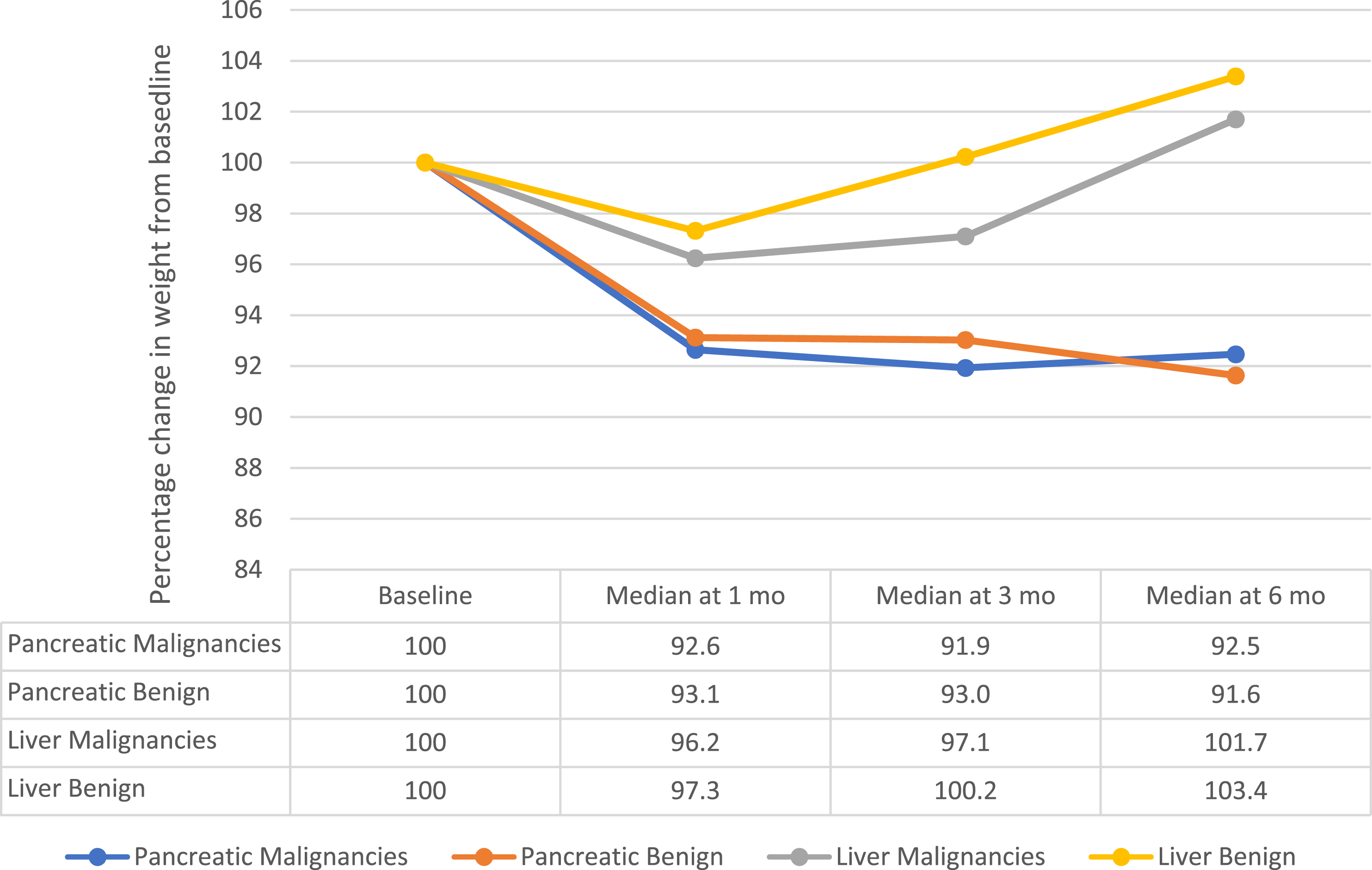
To evaluate potential causes of sustained weight loss in pancreatic patients, we further performed analysis of the weight trajectories for patients who experienced a major complication vs those who did not experience a major complication (Figure 2). Patients with a major complication had, on average, a greater percentage weight loss at all time points, but this difference was not statistically significant. Percentage weight loss from baseline in patients who underwent pancreatic surgery. Patients are stratified to those who experienced a major postoperative complication and those who did not experience a major postoperative complication after undergoing pancreatic surgery.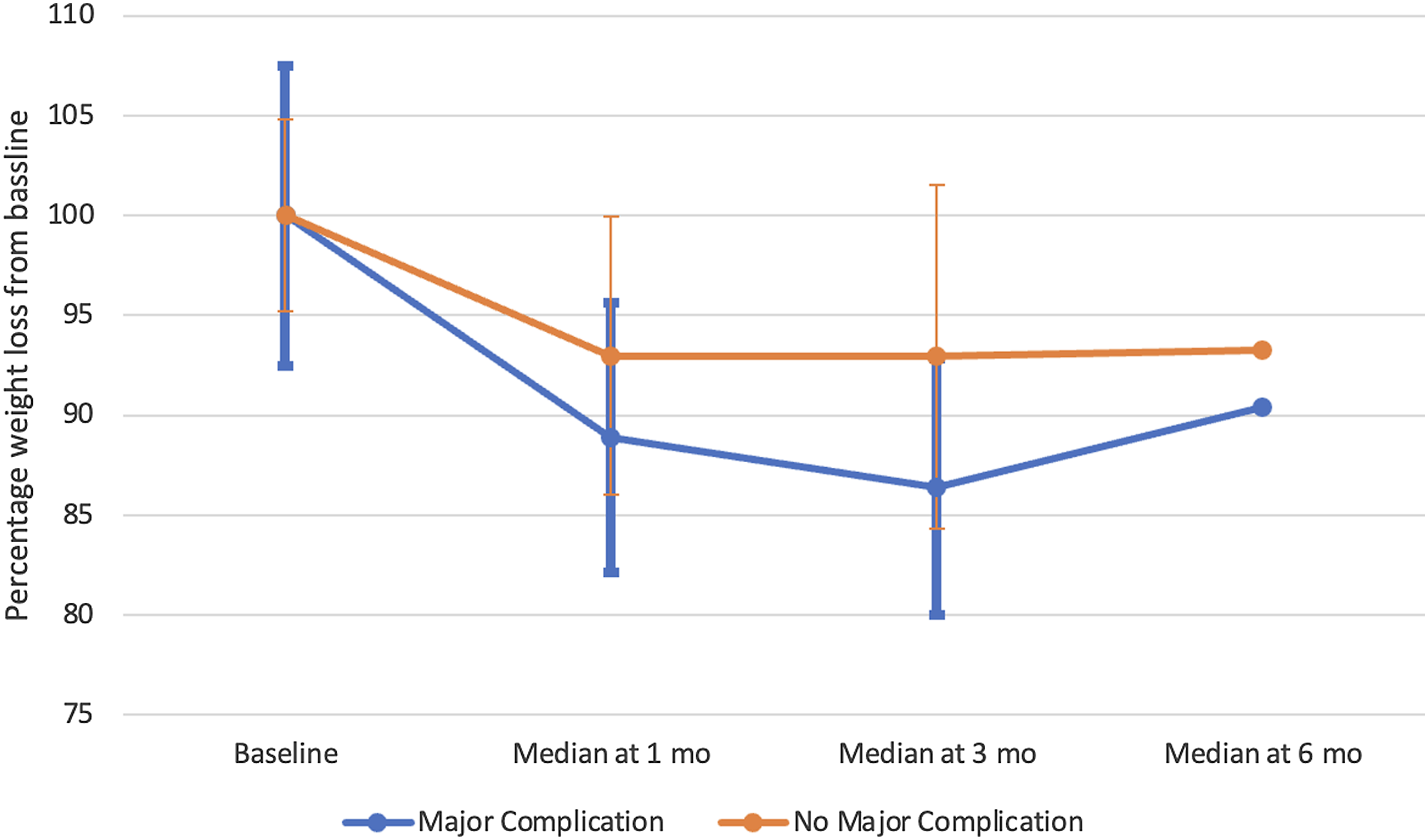
Using multivariable analysis, we found several statistically significant factors associated with >10% weight loss at 3 months from surgery. These include major and minor postoperative complications within 90 days after surgery, malignant pathology, and pancreatectomy. Factors that did not significantly impact patient weight included BMI, age, sex, neoadjuvant and adjuvant chemotherapy, and length of hospital stay (Table 3).
Prevalence of Weight Loss and Postoperative Complications
Postoperative Complications at 3 Months in Clinically Relevant Postoperative Weight Loss and those Without Clinically Relevant Weight Loss.
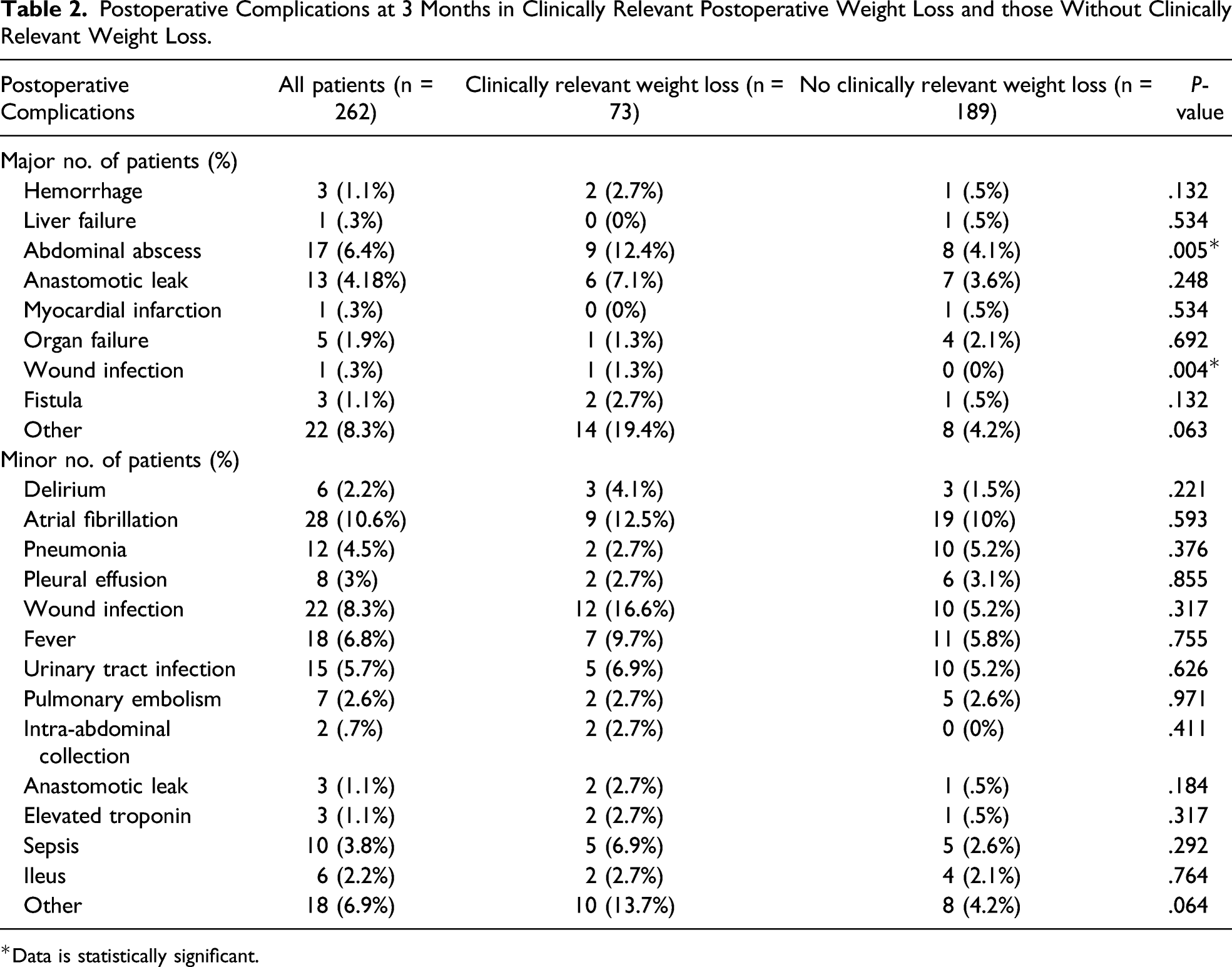
*Data is statistically significant.
Clinical and Nutritional Markers
Multivariable Analysis of Risk Factors Associated with Cachexia at 3 Months from Surgery.
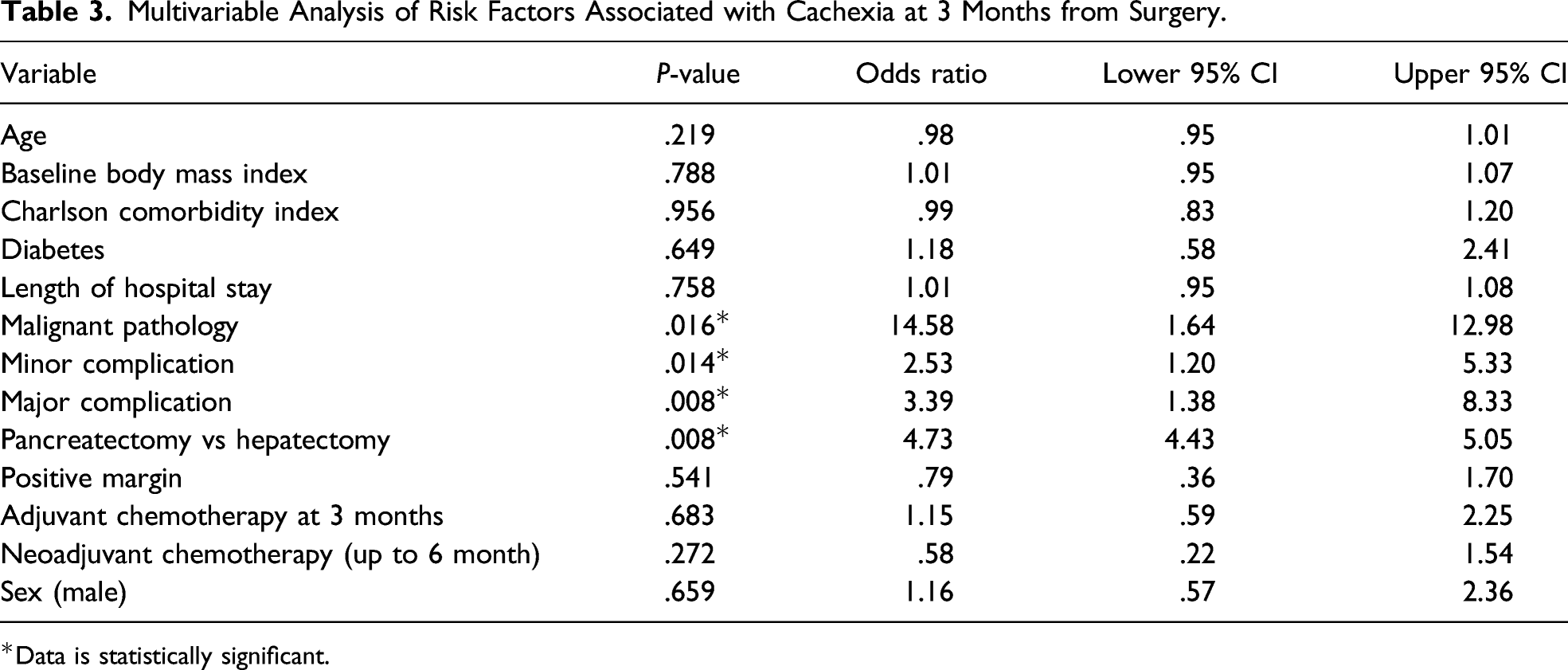
*Data is statistically significant.
Discussion
In our study, we found that among patients undergoing HPB surgical resections, those undergoing pancreatic surgery experienced significant and sustained weight loss, while patients undergoing hepatic surgery were able to recover their weight at 6 months. Patients who had clinically relevant weight loss experienced a substantially higher rate of postoperative complications compared to patients who did not have clinically relevant weight loss. Patients who experienced major postoperative complications had significantly lower levels of albumin and hemoglobin at 3 months from surgery.
Based on the previous work of Bachmann et al., 2 who examined 227 patients with confirmed ductal carcinoma and documented weight course of patients prior to surgery, at the time of surgery and at 6 and 12 months. Bachmann demonstrated that by 6 months after surgery, patients lost approximately 12–14% of their baseline weight. Our comparative patient subcohort had a weight loss of 7.5%. Furthermore, the study suggests that patients begin to recover weight by 12 months after the course of the operation. In our study, we did not observe weight recovery for the first 6 months after the operation. Our findings are consistent with previous studies on postoperative weight loss following HPB surgeries.
Cancer cachexia is well described in the literature as a product of muscle loss and insulin resistance resulting from inadequate nutrient intake (due to malabsorption, obstruction, or treatment side effects) and increased energy expenditure. 23 ACS-NSQIP data show that pancreatectomy has higher mortality index than hepatectomies. 24 It might be intuitive that patients experiencing postoperative complications should have higher percent weight loss compared to patients who do not experience complications. While these complications have not been directly linked to weight loss in the setting of pancreatectomies and hepatectomies, they can impair digestion and appetite, contributing to weight loss. Our data suggest a correlation between more weight loss postoperatively and higher incidence of postoperative complications.
The fact that patients undergoing pancreaticoduodenectomy have a higher risk of clinically relevant weight loss compared to patients undergoing hepatectomies is not surprising. Patients with pancreatic cancer are notably susceptible to perioperative weight loss secondary to preoperative biliary obstruction and postoperative exocrine insufficiency. 1 Pancreaticoduodenectomy is commonly considered a longer and more invasive procedure than hepatectomy, placing a larger metabolic demand on the body during the healing process. However, this common assumption needs further validation in the literature with long-term follow-up on postoperative weight changes until our study.
Some limitations of our study include missing weight data due to attrition. Of the 262 patients included in the primary outcome, only 161 patients had both three- and 6-month weight data. Potential reasons for missing this information may include patients being transferred to a local center for oncology follow-up and physician preference to record patient weight during follow-up visits. Very rarely, in-patients with severe complications or patients who died within 90 days after the index of operation would not have had a follow-up appointment to document their weight change; therefore, we considered these data to be missing at random for purposes of statistical analyses. In addition, we encountered missing information in albumin values both preoperatively and at the 1- and 3-month postoperative follow-up. However, albumin is considered an imperfect nutritional marker, 25 and more accurate biomarkers are needed to assess nutritional status in these patients. Importantly, we focused on clinical definition of cachexia without using radiological definition since not all patients underwent radiological evaluation ad 3 and 6 months from surgery.
Our study has a number of strengths. Notably, it is one of the first studies examining the relationship between postoperative weight loss and postoperative complications. We developed a systematic and rigorous protocol to extract patient data through electronic health records, patient information, and follow-up information from our cancer center. We also used validated scales to categorize the patient’s comorbidities and postoperative complications.
A key area of future study is to examine whether there is a need for postoperative nutrition supplementation to help patients recover their weight. Our study suggests that postoperative weight loss is associated with higher rate of postoperative complication; therefore, early intervention with nutritional supplementation and/or pancreatic enzymes on patients who experience clinically relevant weight loss may prevent complications and improve outcomes. We hope to use the experience and findings from this retrospective study to inform the design of randomized controlled studies aimed at decreasing postoperative complications by identifying the group of patients that are most likely to benefit from nutritional interventions in the postoperative period.
Footnotes
Author Contributions
All authors provided substantial contributions to the conception and design of the work, drafting the work and revising it critically for important intellectual content, and gave final approval of the version to be published. The authors agree to be accountable for all aspects of the work.
Study concept and design: Pablo E. Serrano, Betty H. Zhang, Leyo Ruo, Marko Simunovic, and Maria I. Pinto-Sanchez
Acquisition of data: Betty H. Zhang, Sanaa Ghazi Faisal, Leyo Ruo, Marko Simunovic, and Pablo E. Serrano
Analysis and interpretation: Betty H. Zhang, Sanaa Ghazi Faisal, and Pablo E. Serrano
Study supervision: Pablo E. Serrano
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.