
Abstract
Background. During the COVID-19 pandemic the question arises if laparoscopy, as an aerosol forming procedure, poses a potential risk for viral transmission of SARS-CoV-2 to healthcare workers. Methods. A literature search was conducted using PubMed, Embase and MEDLINE. Articles reporting information regarding COVID-19 or other relevant viruses and laparoscopy, surgical smoke, aerosols and viral transmission were included. Results. Although aerosols produced during laparoscopy do not originate from the respiratory tract, the main transmission route of SARS-CoV-2, research did show SARS-CoV-2 to be present in other body fluids. The transmission risk via this route is however considered very low. As previous research showed potential viral transmission during laparoscopy for viruses that spread through contaminated body fluids, there might be a potential risk of SARS-CoV-2 transmission during laparoscopy, albeit considered very small. Conclusion. Due to the small risk compared to widely known benefits of laparoscopy, there is no reason to replace laparoscopy by laparotomy due to COVID-19 infection. To avoid the potential small risk of viral transmission, additional safety measures are advised.
Introduction
The COVID-19 pandemic currently raises many questions regarding safe health care and protection of health care workers. It is suggested that elective surgery of COVID-19 positive patients should be postponed if medically justified. 1 However, emergency indications, for example, appendicitis or ectopic pregnancy, still occur. Laparoscopy is preferred for these indications as it has shorter hospital stay, quicker recovery, and fewer complications. The risk of viral transmission during laparoscopy is unclear especially as this procedure forms aerosols. In line, many surgeons are hesitant to perform this surgical procedure, especially since some medical associations recommend this procedure not to be first choice anymore. 2 Microbiologists on the other hand assume that SARS-CoV-2 viral transmission only occurs by droplet aerosol formation via the respiratory tract. 3 The question arises if laparoscopy is still advisable for COVID-19 positive patients and what additional safety measurements should be taken. The aim of this review is to discuss the potential risk of laparoscopy in COVID-19 positive patients and provide useful safety measurements.
Materials and Methods
A literature search was set up in collaboration with a clinical librarian, and original articles were identified through PubMed, Embase, and MEDLINE until October 2020. The search strategies are presented in Supplementary Material A and contain keywords for COVID-19 and other relevant viruses, laparoscopy, aerosol, surgical smoke, and viral transmission. Additional literature was found using relevant references. Due to limited evidence for COVID-19, literature regarding other viruses (SARS, MERS, hepatitis B, HIV, and HPV) was also considered relevant for inclusion. All study types were eligible for inclusion. Studies were only excluded when they were not addressing relevant information regarding laparoscopy, viral transmission, and protective measurements during surgery for viral transmission or when more recent research was available. Additional to the search strategy, international guidelines or statements regarding laparoscopy and COVID-19 and (inter)national guidelines regarding COVID-19 and other relevant viruses were included. This review was composed as basis for a national COVID-19 and laparoscopy guideline. As COVID-19 is a new disease and new data become available every day, conclusions might change in the future.
Results
Study Selection
1223 titles and abstracts were screened for relevance. 108 studies were obtained in full text and assessed for inclusion, and 26 articles were considered eligible (Figure 1 Flow diagram literature search.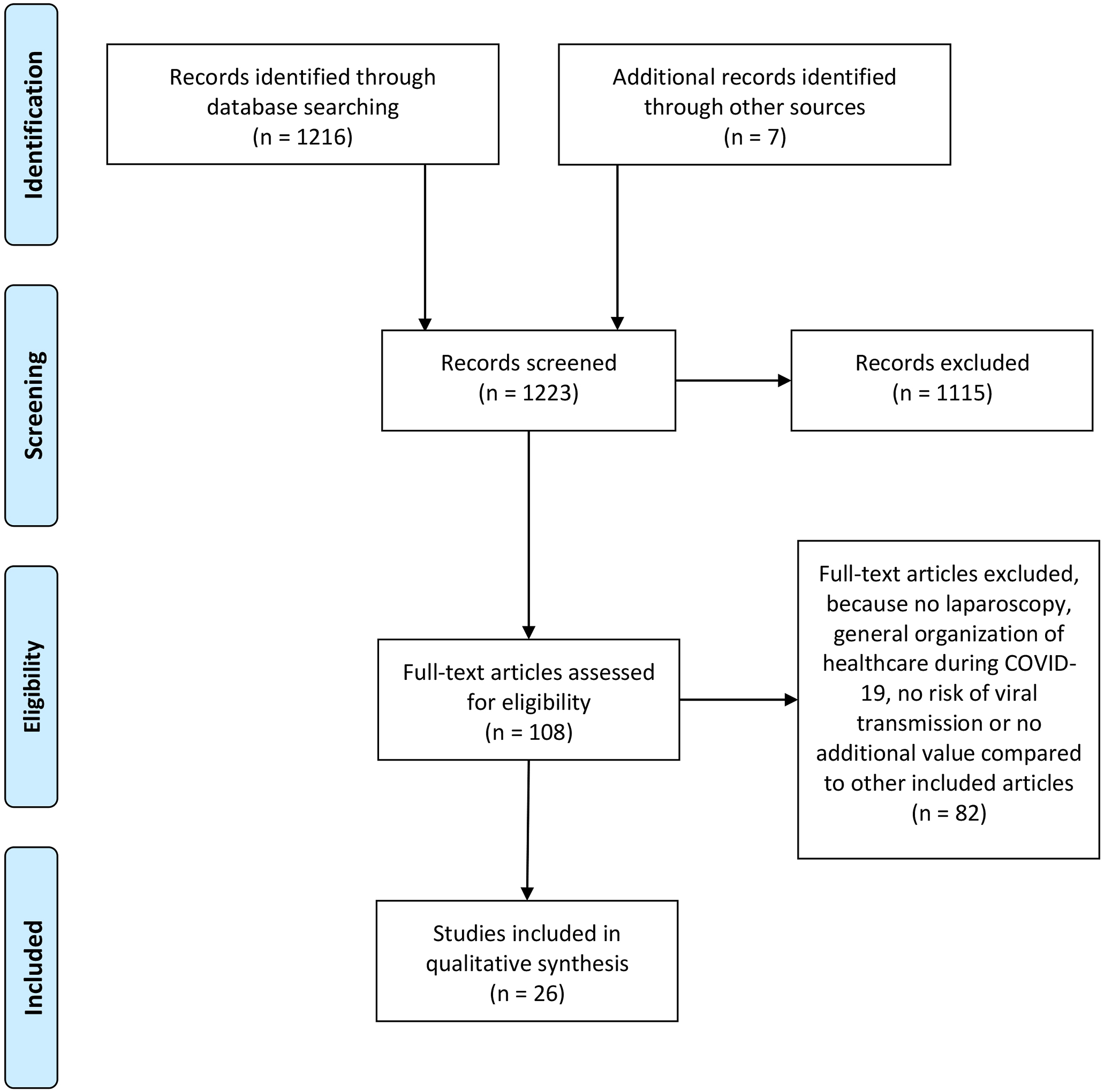
Viral Transmission of SARS-CoV-2 and Other Viruses
COVID-19 is caused by the RNA virus SARS-CoV-2, sized .06–.14 µm, and transmitted by close contact, droplets, and aerosols during aerosol-forming procedures.3,4 Until now, airborne transmission has not been proven. 3 Aerosol-forming procedures are described by the WHO as endotracheal intubation, noninvasive ventilation, tracheostomy, cardiopulmonary resuscitation, manual ventilation prior to intubation, bronchoscopy, tracheostomy procedures, and suctioning.4,5 SARS-CoV-2 viral RNA has also been detected in feces, whole blood, serum, saliva, and urine, 6 although detection of viral RNA is not equivalent to contagiousness. Viral RNA is found only in a small amount of blood samples, but in a larger amount of feces samples. Despite high RNA levels, live virus is only found in very few feces samples.7,8 Recent case series show various reports regarding viral RNA in peritoneal fluid, but until now, no living virus is detected.9-11 Therefore, the risk of viral transmission through other body fluids is expected to be low. MERS-CoV and SARS are other coronaviruses and also mostly transmitted via droplets12-14; hence, transmission is comparable to SARS-CoV-2. As Hepatitis B, HIV, and HPV are mostly transmitted through contaminated body fluids,15-17 transmission is less comparable to SARS-CoV-2. However, as viral transmission of SARS-CoV-2 has not yet been excluded via other body fluids, the risk of transmission during laparoscopy of all these viruses should be considered relevant.
Viral Transmission During Laparoscopy
During laparoscopic surgery, an artificial pneumoperitoneum is created in which aerosols are produced, which can spread to health care workers during the surgery. Therefore, laparoscopy could be considered as an aerosol-forming procedure. As these aerosols do not originate from the respiratory tract, the risk of viral transmission is presumably much smaller than aforementioned aerosol-forming procedures. At this point, no data on viral spread during surgery are available for SARS-CoV-2. Previous research showed evidence of potential viral spread of other viruses during surgery. As pneumoperitoneum contains cells and cellular debris, it is a potential carrier for viruses as Hepatitis B and HIV.18,19 Desufflation of this pneumoperitoneum can cause contamination of the environment with blood and body fluids. 20 Additionally, electrosurgery and ultrasonic surgery used during surgery create surgical smoke with particles sized .07–6.5 µm. 21 Research showed that surgical smoke can contain viral particles of HIV, hepatitis B, and HPV. The actual risk of transmission through surgical smoke to health care workers is uncertain but seems to be small.21-26 The risk of SARS-CoV-2 presence in surgical smoke is presumably smaller as this virus is only present in small amounts and nonactive form in blood. Viral RNA is found to a greater extent in feces, and there might be a very small risk of viable viruses,6-8 which might be of importance for surgery involving the bowel. The risk of viral transmission is however yet unclear and presumably small. Considering this combined information, it is important to minimize the CO2 dispersion into the operating room. There is no consensus about the difference in risk of surgical smoke between laparoscopy and laparotomy. Most research describes the aerosols to be more concentrated due to pneumoperitoneum in laparoscopy. Also, pneumoperitoneum may be released uncontrolled.2,21,27,28 On the contrary, surgical smoke can be suctioned less precise during laparotomy, 22 and the abdominal wall might work as a barrier. 29 In conclusion, there is a potential small risk of SARS-CoV-2 transmission through laparoscopy, and therefore, safety measures are advised.
Laparoscopy or Laparotomy
Elective surgery should not be performed in COVID-19 positive or suspected patients if it is medically justified to postpone this surgery. Postoperative pulmonary complications occur in half of patients with perioperative SARS-CoV-2, with high mortality. 30 Also, there is a risk of viral transmission to other patients and health care workers during surgery and hospital stay. However, emergency surgery or necessary oncological surgery should always be considered, also in COVID-19 positive or suspected patients.
The included articles do not state a clear preference for laparoscopy or laparotomy.1,2,28 Laparoscopy may expose health care workers to a small increased risk of infection; however, this potential risk can be reduced by sufficient protective measurement. Mainly in the postoperative recovery period, a laparotomy has more negative cardiac and pulmonary side effects than laparoscopy, and patients have a longer recovery period and length of stay. For a COVID-19 patient with potential pulmonary complaints, this especially is not desirable. In addition, efforts should be made to minimize hospital stay due to large demands on hospitals and to reduce nosocomial transmission. 31 On the contrary, a COVID-19 patient with many pulmonary complaints may experience worsening due to the use of pneumoperitoneum and Trendelenburg position during laparoscopy. These considerations should be made preoperatively.
From these data, it can be advised that the choice to perform a laparoscopy or laparotomy should not depend on COVID-19 status. Due to a limitation of conclusive evidence and the expected very low risk of transmission, COVID-19 is not a contraindication for laparoscopy. The surgical route should be based on surgical indication, clinical status, and experience of the surgeon.
Safety Measures
Prevention of Pneumoperitoneum Dispersion
Pneumoperitoneum dispersion should be avoided as much as possible to prevent aerosols from entering the operating room.27,28 It is advised to close trocars at introduction and close Veress needles during removal. Also, the use of trocars with intra-abdominal seal might prevent aerosol dispersion. Surgical smoke and pneumoperitoneum should be evacuated,1,2,21,23,27,28 especially before the end of surgery or before converting to open surgery, and a filtration device could be of additional value.1,2,21-23,28 It is suggested to evacuate pneumoperitoneum and smoke through a closed system to prevent aerosol dispersion. Afterward, trocars should be removed with caution to prevent herniation as sight might be impaired after desufflation.
Various filtration devices are available, with HEPA (high-efficiency particulate arrestance) filters and ULPA (ultralow particulate arrestance) filters widely used in laparoscopy. High-efficiency particulate arrestance filters eliminate 99.97% of particles larger than .3 µm,32,33 and ULPA filters have a minimum 99.999% efficiency rating for removing particles larger than .1 µm29,32,33 and some even up to .01 µm.29,34 However, virus filtration is based on particle size in HEPA and ULPA filters,1,23 and to date, the efficacy of filters on virus filtration has not been tested in peer-reviewed clinical studies. 35 Therefore, it is advised to use a filter additionally to a closed suction system, and not advised to let CO2 directly enter the OR through the filter.
In 2-way pneumoperitoneum insufflators, CO2 recirculates through the system during surgery via a filter and additionally releases CO2 into the OR to maintain a stable pressure and eliminate smoke. Systems use different modes and filters, and therefore, warrantee is needed when using these systems. In some modes, CO2 might not be filtered before entering the OR room.33,36 Although no data are available, on theoretical grounds, there might be a small chance the inside of the system gets contaminated as the filter is unable to guarantee 100% elimination. Inherently, on these grounds, the system could pose a small risk of cross contamination. It is recommended for users of these insufflators to contact the manufacturer to ensure the possibility of safe use for both patients and health care workers. Individual considerations must be made regarding potential benefits and risks.
Another consideration regarding pneumoperitoneum is intra-abdominal pressure. Zheng et al and SAGES advised to keep intraperitoneal pressure at the lowest possible levels without compromising the surgical field to reduce the risk of transmission.1,27 Theoretically, with less high intraperitoneal pressure, the aerosols will leave the abdominal space with less force upon uncontrolled dispersion of pneumoperitoneum. This is however based on little evidence. It is recommended that surgery should preferably be performed with the lowest intraperitoneal pressure possible in order to reduce the chance of aerosols escaping, without compromising the surgical field. Although as inexperience with a low pressure might lead to complications, surgeons should not deviate from their normal practice due to COVID-19.
Operating Technique
Electrosurgery and ultrasonic surgery are widely used in laparoscopy and cause smoke development. Prolonged use in one location and high voltage result in additional smoke development.1,27 As ultrasonic surgery creates low-temperature vaporization, cellular debris in surgical smoke may remain infectious, but evidence is lacking.21,24,27 However, the risk of viral presence in the abdominal cavity and transmission through pneumoperitoneum is considered very small. Hence, both techniques are considered safe to use as potential negative effects due to inexperience of the technique do not outweigh the very small reduction of viral transmission. During surgery, Trendelenburg position may negatively affect lung function and cardiac circulation, which can cause problems for COVID-19 patients. 27 It is advised to keep the duration of Trendelenburg position as short as possible if this is surgically justified.
Disinfection of Materials and Waste Disposal
Devices used on infection-suspected or proven patients should be assumed contaminated.1,27,37 In Dutch hospitals, all devices are considered contaminated, and no separate labeling is necessary. Otherwise, labeling is recommended. Waste must be treated as contagious and disposed according to hospital protocols.27,38 During surgery, instruments should be kept clean as possible of blood and other body fluids. 27
Surgical Team
Any contact with a COVID-19 patient provides a potential risk of infection. To minimize this risk, a minimum number of staff members should be present in the operating room.2,38,39 As intubation and extubation is marked as a high-risk aerosol-forming procedure, 4 the number of staff that is present during this event must be minimized,2,39 preferably only the anesthesiologist and nurse anesthetist. Health care workers present during this procedure should use personal protective equipment (PPE) and conform local protocols for high-risk aerosol-forming procedures. The remaining surgical team members should enter the operating room after intubation.
PPE
In accordance with national and local guidelines, protective measures must be taken for every contact with a COVID-19 positive or suspected patient. Several options are discussed in the literature with regard to additional measures for laparoscopy. The use of shoe covers is maintained in some protocols37,38; however, this is considered not necessary when operating clogs are used which are cleaned after surgery.
The use of N95/FFP2 masks can reduce the risk of viral transmission to health care workers, although small particles (<.1 µm) may not be filtered by these masks.21,23 International centers and guidelines differ regarding the use of a positive pressure mask, personal HEPA filter, FFP2, or FFP3 mask.2,37-39 The WHO recommends an FFP2/N95 mask for aerosol-forming procedures (involving aerosols originating from the respiratory tract) or FFP1 masks if the first is not available. IIR surgical mouth nose masks are recommended for all other moments of contact. 5 As mentioned before, the spread of the SARS-CoV-2 virus via laparoscopy has not (yet) been proven, and the risk is considered very small as aerosols do not originate from the respiratory tract. From these data, it is currently recommended to use at least an IIR mask during laparoscopy. In this context, it is important that the surgical team is not present during the intubation and extubation of the patient. Protective clothing is advised to consist at least a water-repellent apron, an IIR mask, tightly fitting goggles or a face shield,4,37,38,40 and gloves. One guideline 2 recommends the use of double gloves. However, this is not considered as clear added value in laparoscopy and therefore not advised.
Operating Room
It is recommended to create a dedicated operating room for COVID-19 positive or suspected patients to reduce the risk of transmission between patients.1,27,37-39 Door movements must be limited to prevent transmission to rooms outside the operating room (OR). 41 Some published protocols advised a negative pressure in the OR to prevent viral transmission to rooms outside the initial operating room due to positive pressure.1,38,39 In daily practice, a negative pressure OR will be difficult to achieve in many centers. This preventive measure is considered not specifically applicable to laparoscopic surgery. Therefore, no suggestions regarding positive or negative pressure in the OR are made. To eliminate the possible viral particles in the air, it is recommended to ensure a waiting time between surgeries after a COVID-19 positive or suspected patient. In included studies, this time varied from 30 (99% effectiveness) 39 to 60 minutes (dilution to .0000002%). 37 In Dutch class 1 operating rooms, air is changed at least 20 times an hour and additionally filtered using the HEPA filter, a maximum of 20 minutes is allowed to create a dilution of 1:100.41 It is recommended to take into account the time required to remove aerosols from the air, 41 formulated in national or local protocols.
Conclusion
Due to the pandemic outbreak of COVID-19, there is a need for guidance for health care workers to prevent viral transmission during laparoscopic surgery. There is currently little evidence from literature how to precisely deal with this problem. Since laparoscopy is an aerosol-forming procedure, there is a potential small risk of viral transmission. However, this risk is considered very small. Laparoscopy should not be replaced by laparotomy due to COVID-19 if there is no other clinical indication. This review describes practical safety measurements to minimize this small risk of viral transmission during laparoscopy.
Supplemental Material
sj-pdf-1-sri-10.1177_15533506211003527 – Supplemental Material for Potential Risk and Safety Measures in Laparoscopy in COVID-19 Positive Patients
Supplemental Material, sj-pdf-1-sri-10.1177_15533506211003527 for Potential Risk and Safety Measures in Laparoscopy in COVID-19 Positive Patients by Fokkedien HMP Tummers, Werner A Draaisma, Ahmet Demirkiran, Tammo A Brouwer, Brunolf W Lagerveld, Esther S van Schrojenstein Lantman, Klaartje Spijkers, Sjors FPJ Coppus, Frank Willem Jansen in Surgical Innovation
Footnotes
Acknowledgments
The authors would like to thank the Dutch microbiology COVID-19 expert group for their contributions.
Author Contributions
Study concept and design: Fokkedien HMP Tummers and Frank Willem Jansen Acquisition of data: Fokkedien HMP Tummers
Analysis and interpretation: Fokkedien HMP Tummers, Werner A Draaisma, Ahmet Demirkiran, Tammo A Brouwer, Brunolf W Lagerveld, Esther S van Schrojenstein Lantman, Klaartje Spijkers, Sjors FPJ Coppus, and Frank Willem Jansen Study supervision: Frank Willem Jansen
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.