
Abstract

Dear Editors:
Laparoscopic surgery has advantages over open surgery for several abdominal conditions due to improved short-term outcomes. 1 Performing laparoscopic surgery in many low and middle-income country (LMIC) settings is restricted by the lack of general anaesthesia (GA) and carbon dioxide (CO2) insufflation. Gasless laparoscopic surgery employs the use of a mechanical anterior abdominal wall lift device to create internal space within the abdomen. This negates the need for GA and CO2 which may help increase adoption of laparoscopic surgery in LMIC settings. 2
The safety and efficacy of gasless techniques appear to be non-inferior when compared to conventional laparoscopic surgery for many gastrointestinal and gynaecological conditions. 3 However, concerns from surgeons before adopting this technique are operative field of view and safety concerns including damage to the abdominal wall during the lift. 3 Many lift devices produce a tenting effect, creating an angular cavity that can restrict view. 3 Monitoring to ensure a ‘safe’ force is applied is also essential, as lifting the abdominal wall carries the potential for trauma if too much force is applied. 4 Our aim was to develop methods that may be used in future clinical studies aimed at mitigating these concerns by assessing field of view and force exerted on tissues during gasless lift procedures.
Firstly, we developed a novel mechanical force sensor and integrated this into a lift device. The sensor indicated the magnitude and estimated ‘safety’ of the vertical load applied to the wall during lifting. Using a frugal design approach, we developed a ‘spring-balance’ system which provides a robust low-cost mechanism that can be readily manufactured and maintained in LMICs (Figure 1). The gauge consists of a spring housed within 2 concentric tubes, combined with a calibrated colour scale on the outside of the inner tube to inform the user of the load being applied. The sensor was calibrated to display Green (Force = 0-130N), Yellow (Force = 130-150N), and Red (Force = 150-170N). These values align with literature values for acceptable force ranges exerted during conventional laparoscopic surgery.
5
The sensor can be readily integrated into a low-cost lift system and would be ideal during training to provide the user with objective visual feedback on loading. 3D scanning technology and a novel mechanical force sensor can be used to evaluate field of view and safe lift forces during gasless laparoscopic experiments.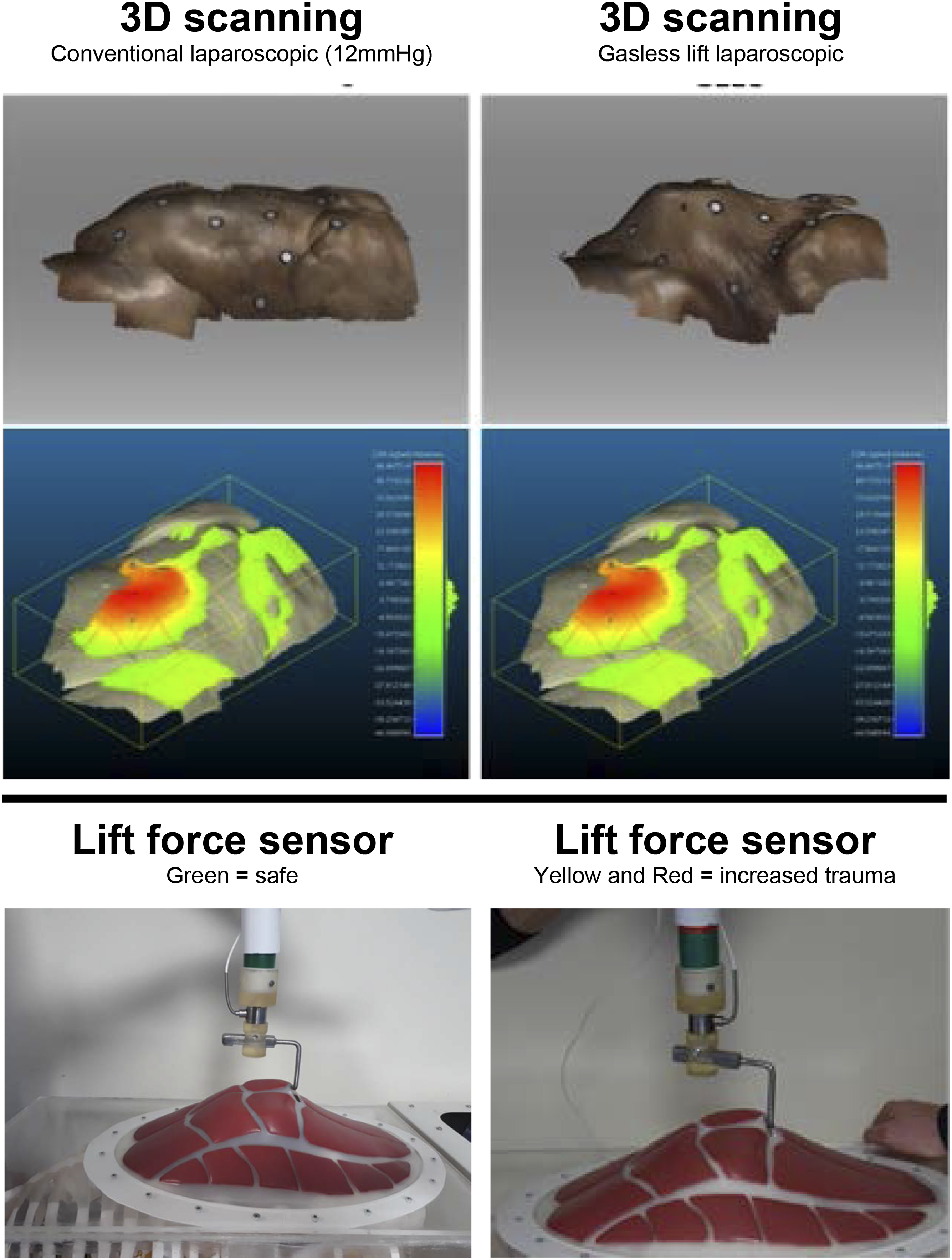
Secondly, we conducted an experiment using a single human cadaver. The purpose of this was to assess the field of view via 3 dimensional (3D) abdominal wall surface scanning and volumetric analysis. Intra-abdominal volume created via the techniques was used as the proxy for field of view. Paper reference markers were sutured to the abdominal surface to aid registration during the surface scanning that was carried out using a commercially available 3D laser scanner (Artec Space Spider, Artec 3D). The associated scans were processed using a bespoke software package (Artec Studio 12, Artec 3D) and the resultant surfaces of the cadaveric abdominal wall were analysed to obtain cross-sectional data using an open source 3D mesh analysis software (CloudCompare). The headroom profile and abdominal wall shape created by conventional laparoscopic surgery at 12 mmHg and gasless lift were compared (Figure 1). While some ‘tenting’ effects are apparent, similar volumes were achieved by gasless techniques as compared to insufflation. Further validation as to the impact of field of view in clinical studies is required.
Our results demonstrate the use of the 3D surface scanning technology and the novel mechanical force sensor are suitable methods to evaluate field of view and force applied to the abdominal wall. These methods have relevance to support further evaluation of gasless surgery techniques in clinical trials with living patients.
Dissemination Declaration
The results will be disseminated on social media platforms and reports back to funders.
Author Contributions
William S. Bolton, Peter R. Culmer, Jesudian Gnanaraj and David G. Jayne conceptualised the study. William S. Bolton, Noel K. Aruparayil, Joshua R. Burke and William R. Kitchen arranged the cadaveric assessments. Manish Chauhan, Kevin J. N. Gnanaraj, Alice M. Benton, and Sophie E. Hutchinson led the development of the mechanical force sensor and conducted volumetric analysis. William S. Bolton prepared the first draft of the manuscript which was subsequently edited by all authors. David G. Jayne is the study guarantor.
Study concept and design: William S. Bolton, Peter R. Culmer, Jesudian Gnanaraj, and David G. Jayne
Acquisition of data: William S. Bolton, Noel K. Aruparayil, Joshua R. Burke, and William R. Kitchen
Analysis and interpretation: Manish Chauhan, Kevin J. N. Gnanaraj, Alice M. Benton, and Sophie E. Hutchinson
Study supervision: David G. Jayne and Peter R. Culmer
Footnotes
Acknowledgments
The authors would like to acknowledge the staff at the Division of Anatomy, University of Leeds School of Medicine, for their support in this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Translate MedTech and the National Institute for Health Research (NIHR) (16/137/44) using UK aid from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care.