
Abstract
Introduction. Laparoscopic treatment of deep endometriosis (DE) is associated with intra- and post-operative morbidity. New technological developments, such as haptic feedback in laparoscopic instruments, could reduce the rate of complications. The aim of this study was to assess the room for improvement and potential cost-effectiveness of haptic feedback instruments in laparoscopic surgery. Methods. To assess the potential value of haptic feedback, a decision analytical model was constructed. Complications that could be related to the absence of haptic feedback were included in the model. Costs of complications were based on the additional length of hospital stay, operating time, outpatient visits, reinterventions, and/or conversions to laparotomy. The target population consists of women who are treated for DE in the Netherlands. A headroom analysis was performed to estimate the maximum value of haptic feedback in case it would be able to prevent all selected intra- and post-operative complications. Results. A total of 9.7 intraoperative and 47.0 post-operative complications are expected in the cohort of 636 patients annually treated for DE in the Netherlands. Together, these complications cause an additional length of hospital stay of 432.1 days, 10.2 additional outpatient visits, 73.9 reinterventions, and 4.2 conversions. Most consequences are related to post-operative complications. The total additional annual costs due to complications were €436 623, amounting to €687 additional costs per patient. Discussion. This study demonstrated that the potential value for improvement in DE laparoscopic surgery by using haptic feedback instruments is considerable, mostly caused by the potential prevention of major post-operative complications.
Introduction
Endometriosis is a benign disorder defined as the presence of endometrial-like tissue outside the uterus which induces an inflammatory response. This response is accompanied by adhesions, fibrosis, angiogenesis, neuronal infiltration, and anatomical distortion, resulting in pelvic pain, pelvic organ dysfunction, and infertility. It affects 5-10% of women of reproductive age. 1 In women with endometriosis, the prevalence of involvement of the gastrointestinal tract is 8-12%. The prevalence of involvement of the urinary tract is lesser and amounts 1-5.5%.2-4 Surgical treatment can be used as first-line therapy in patients with (imminent) organ dysfunction or initiated after failed medical therapies including nonsteroidal anti-inflammatory drugs and hormonal treatments. The majority of these surgical procedures are performed laparoscopically in the Netherlands; the remainder is performed by laparotomy or robot-assisted surgery. 5
Surgical treatment of deep endometriosis (DE) involving the bowel or urinary tract can be challenging due to the extensive inflammation and fibrosis destroying normal anatomy. The normal embryological planes present in normal tissue are no longer visible in severe endometriosis. Therefore, endometriosis surgery is associated with a risk of major complications.6,7 For treatment of DE of the urinary tract, intraoperative accidental injuries of the ureters and bleeding are reported. Major post-operative complications include anastomotic leakage, ureteral fistulae, and vesicovaginal fistulae. Conversions or re-interventions are prevalent in 3-6.7% and 3.9% of cases, respectively. 8 Treatment of DE of the bowel is associated with iatrogenic damage, bleeding, bowel perforation, and intraoperative anastomotic leakage. Post-operative complications include anastomotic leakage, late bowel perforation, intra-abdominal infection, and rectovaginal fistulae. 9 Intraoperative complications lead to significantly increased post-operative morbidity.
Laparoscopic surgery has 3 general limitations: reduced hand–eye coordination, reduced depth perception, and reduced haptic feedback. 10 Reduced haptic feedback leads to grasping and tearing of tissue with excessive force. 11 Which in turn causes tissue damage and more complications. Henceforth, force reflecting operative instruments (FROIs) have been developed to increase haptic feedback during laparoscopic surgery.
Haptic feedback is the human physiological process of touch. Haptic perception incorporates tactile and kinaesthetic perception. Tactile perception is based on pressure receptors in our skin of our fingers and hand, which detect pressure, vibration, and texture. Our kinaesthetic perception is based on receptors in our muscles, tendons, and joints. They detect position, movement, and force applied. 12
This very sensitive input and output of nerve signals are a continuously ongoing motion loop with hardly noticeable delay. Although this cycle is automatic and independently controlled, the surgeon can adjust this cycle by increasing or decreasing on purpose the position and power of the applied muscles. Overall, the effect on tissue manipulation and movement and the position of instruments is based on visual control of the kinaesthetic part of the process of feeling the haptic process.
This physiological process of feeling touch has been copied in haptic feedback graspers for use in laparoscopic surgery. The nerve endings have been replaced by the tip of the glass fibres at the end of the graspers. The small nerve sensors have been replaced by fibre Bragg gratings of 2 to 4 mm. The shift of light frequencies, on the level of nanometres, caused by stretching or compressing these gratings, is transported through the long glass fibre to the control unit. In the unit, the special gator measures the information and translates this into a signal to a control board. The output of an electrical signal is modulated to control the actuator in the hand piece of the surgeon and creates the resistance felt on the grasper tip to the gripper on the fingers of the surgeon.11,13,14
So, the two-way physiological system in the human is copied in this FROI instrument to create real haptic feedback without any delay, as the frequency is 6000 per second. The modulation of the feeling on purpose can be done by changing the gain or pre-settings.
The introduction of a new technology in surgery is related with complications and poor outcome. 15 The introduction of new technology in surgery may also be influenced by industry’s financial incentives, physician’s drive to remain competitive, and the lure of new technology. 16 SAGES has created guidelines for the introduction process of new technology and techniques. 17 They have recommended that health technology assessment (HTA) is the currently best accepted method for the analysis of optimisation of health outcomes and related costs and should be the initial step for introduction of a new technology. 18 In this article, we have performed a HTA by the use of a decision analytic model comparing the current standard technology, conventional laparoscopic surgery, to the new technology haptic feedback in laparoscopic surgery for DE of the bowel and urinary tract. The aim of this study was to estimate the potential value of the use of haptic surgery during laparoscopic DE surgery involving the bowel and/or urinary tract by using a decision analytic model.
Methods
Model
To assess the potential value of haptic feedback during laparoscopy for DE, a decision analytical model was constructed. The model was used to synthesise various sources of evidence in order to estimate expected differences in costs and effects for the 2 strategies under comparison: the current standard of care, in which minimally invasive surgery without haptic feedback is performed, and the strategy with haptic feedback added to laparoscopic instruments. Therefore, complications were included in the model that could be related to the absence of haptic feedback.
Population
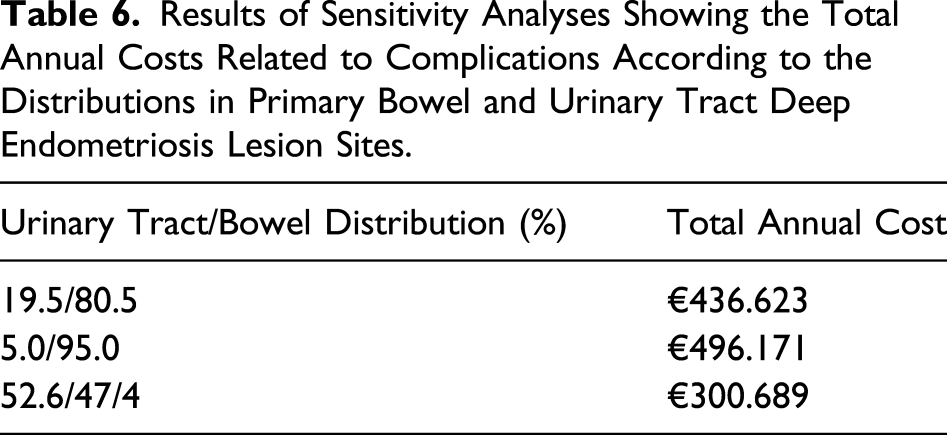
No approval by the institutional medical ethics review board was required. The target population of the model consists of patients with DE in the Netherlands, who received a surgical procedure for removal of a primary bowel or urinary tract DE lesion. The starting population in the model is an annual number of 636 patients registered at the Dutch Endometriosis Foundation who have undergone surgery to remove DE lesions in the Netherlands. 5 Large variation exists regarding the exact distribution between primary lesions (primary bowel lesions or primary urinary tract lesions). Therefore, we made an assumption of this distribution based on the prevalence of urinary tract DE (19.5%) found in a study with 221 patients with DE. 19 We assumed that the remainder of patients (80.5%) had a primary bowel DE lesion.
Selection of Complications Through an Expert Panel Using a Delphi Procedure
There was no clinical evidence on which intraoperative and post-operative complications might be prevented by the use of haptic feedback in laparoscopic surgery. Therefore, an expert panel (consisting of gynaecologists and surgeons) made a selection of intraoperative and post-operative complications (due to undetected intraoperative injury) which can potentially be reduced by the advantages of having haptic feedback in laparoscopic surgery (Supplementary Material S1). Consensus was achieved according to the Delphi method. 20 Their selection was supported by several preclinical studies and veterinary studies.11-14,21 The following intraoperative complications were included in the model: bowel injury, haemorrhage, and ureteral injury. Furthermore, the following post-operative complications were included in the model: late bowel perforation, vesicovaginal fistula, ureteral fistula, rectovaginal fistula, and anastomotic leakage.
Model Structure
A decision tree was developed to simulate the chain of events in the target population within both strategies. For both strategies, the structure of the model was similar.
A complete overview of the decision tree is shown in Figure 1. First of all, a division was made between laparoscopic procedures performed for primary bowel DE lesions and for primary urinary tract lesions. Secondly, a division was made between either having intraoperative or post-operative complications. Thirdly, the intraoperative and post-operative complications were divided in the specific complications and subsequent clinical consequences per complication. Decision tree comparing laparoscopic instruments with and without haptic feedback graspers.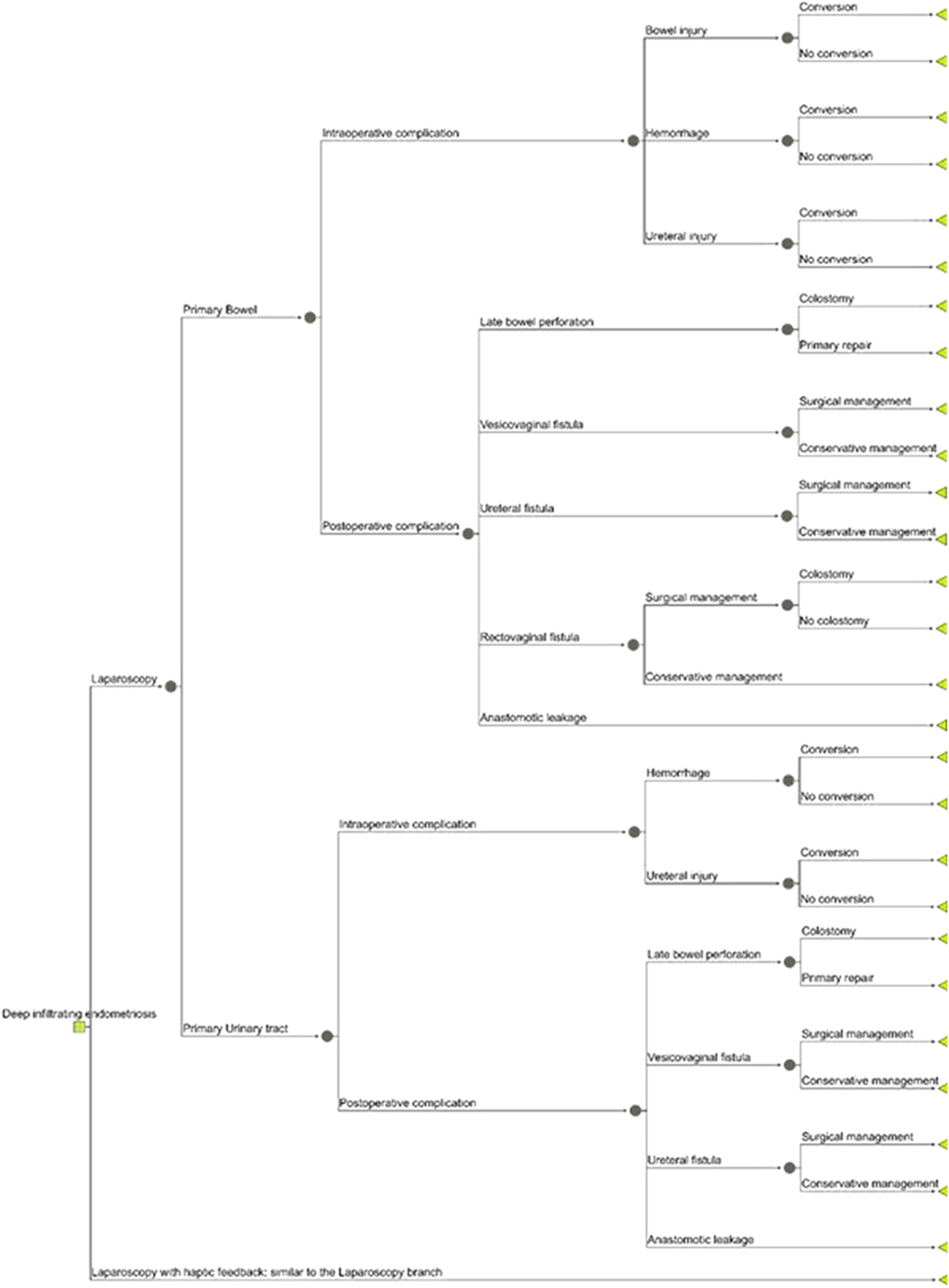
Model Input
Transition Probabilities Used in the Model.
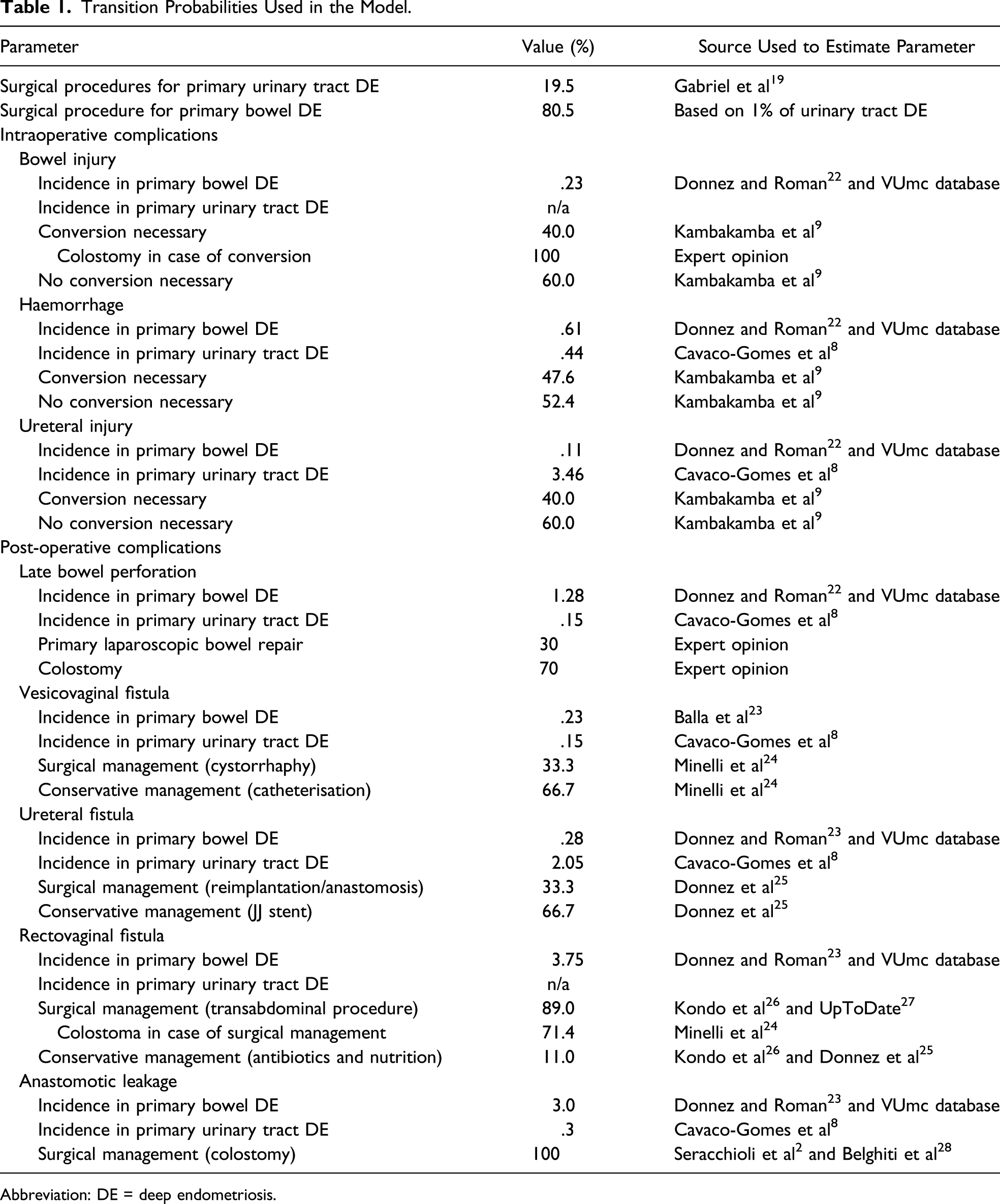
Abbreviation: DE = deep endometriosis.
Costs
Overview of all Costs per Type of Complication.
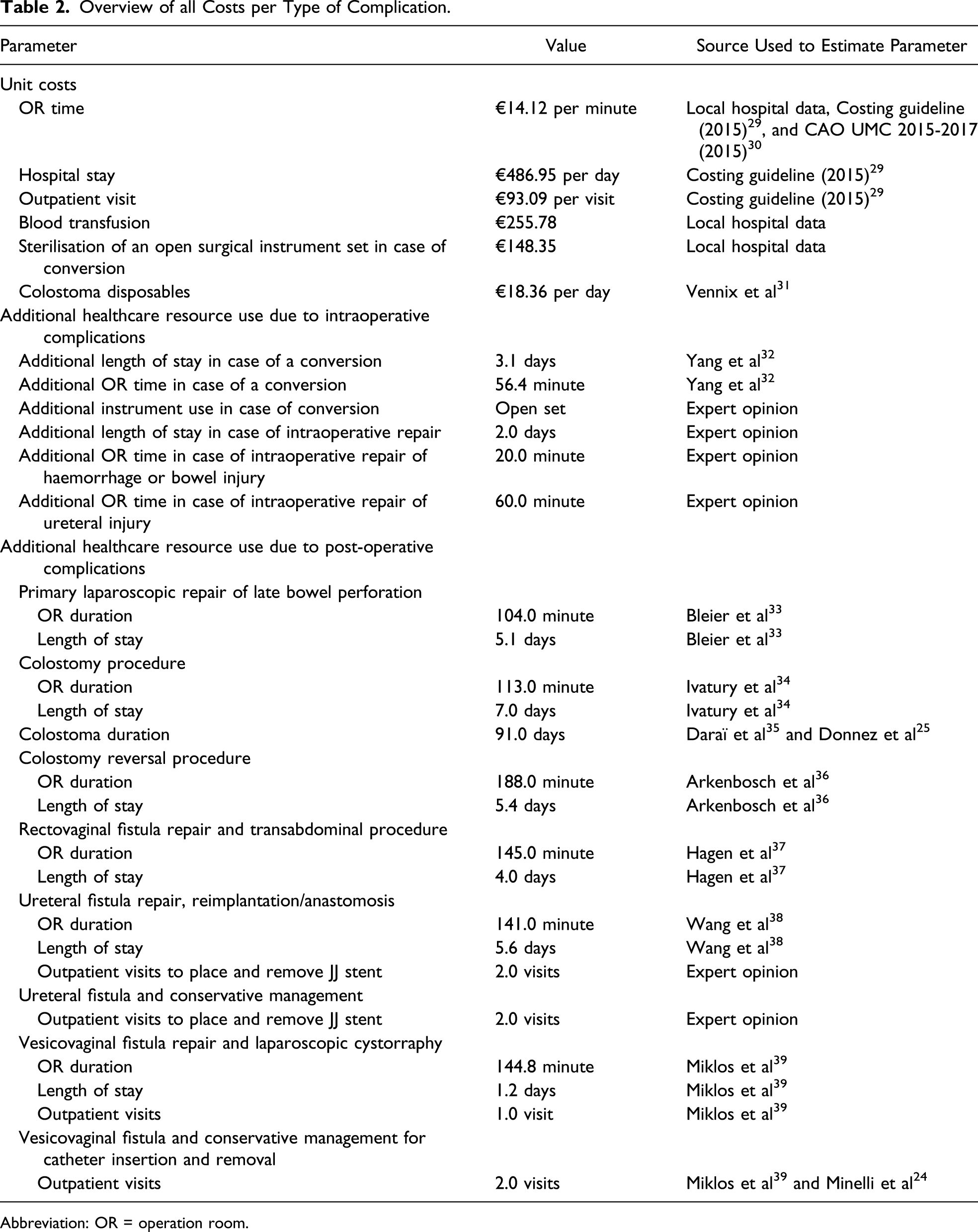
Abbreviation: OR = operation room.
Assumptions
Some assumptions had to be made due to the limited amount of available data or for the simplicity of the model. It was assumed in the model that no complications occur during or following a reintervention. Also, patients were assumed to have either an intraoperative or a post-operative complication and no elevated probability of a post-operative complication after an intraoperative complication.
Based on expert opinion and the overall strategy in the Netherlands, it was assumed that in case of conversion for intraoperative bowel injury, most patients receive a temporary colostomy. The reasoning behind this assumption is that conversion to laparotomy is usually performed when serious intraoperative injury occurs, for which colostomy would also be indicated. For late bowel perforations, it was assumed that 70% of patients undergo a colostomy procedure and the remaining 30% undergo a laparascopic resuturing procedure.40,41
Analyses
Since haptic feedback in laparoscopic graspers is not yet widely implemented and used, there is no clinical evidence on the effect it may have on intraoperative and post-operative complications. Therefore, a headroom analysis was conducted which shows the value of haptic feedback in case it would be able to prevent all selected intraoperative and post-operative complications occurring in primary bowel and urinary tract DE, that is the maximum potential value. The costs of the laparoscopic grasper with haptic feedback are currently unknown and therefore not included in the model.
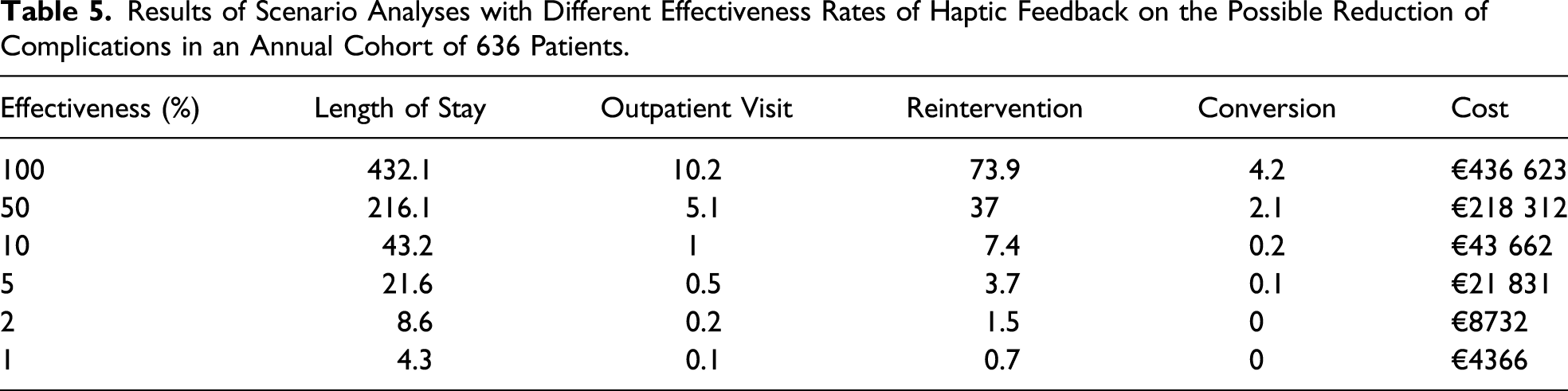
Since the real performance of haptic feedback is likely to be lower than 100% (as assumed in the headroom analysis), we performed scenario analyses to get insight into the potential value of haptic feedback with different levels of effectiveness on reducing complications. In sensitivity analyses, we varied the value of several input variables to assess their influence on the outcomes.
Results
Base Case Analysis Results, Number of Complications Occurring Annually in Primary Bowel and Urinary Tract DE in the Yearly Cohort of 636 Patients.
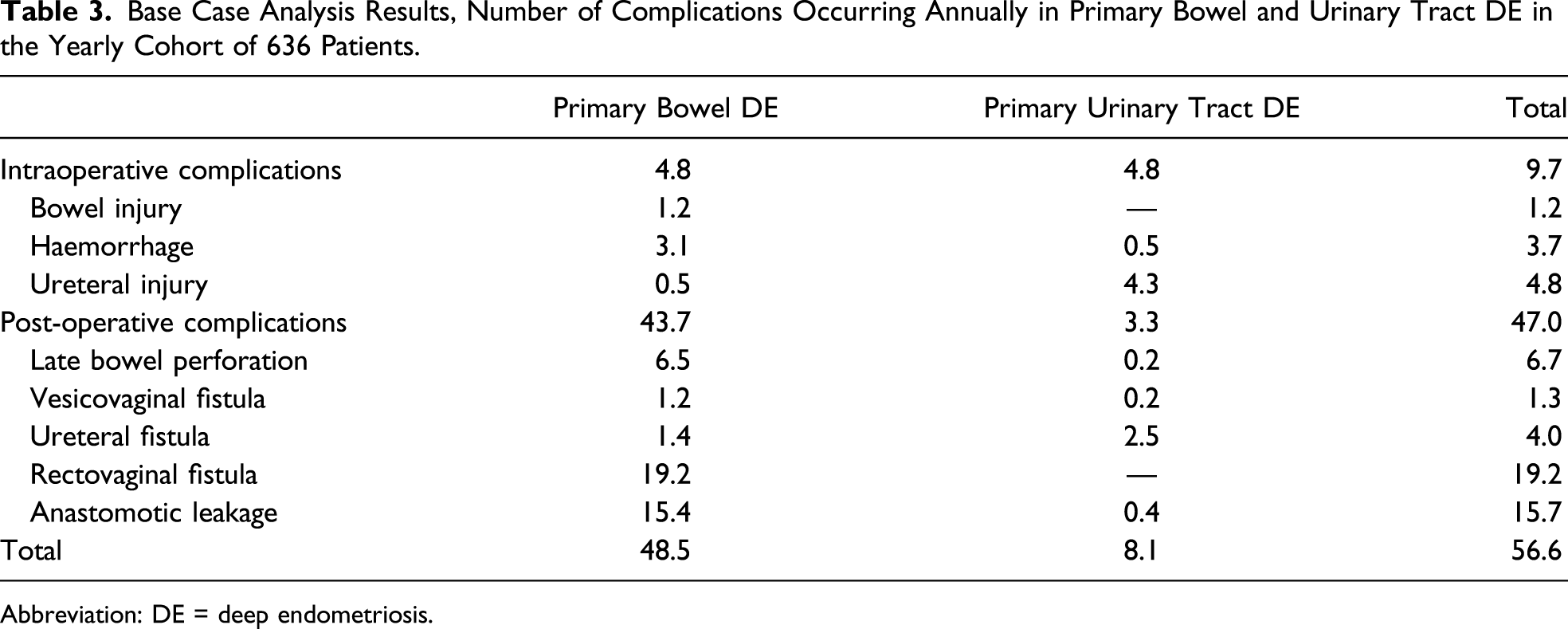
Abbreviation: DE = deep endometriosis.
Base Case Analysis Results, Annual Consequences of Intraoperative and Post-operative Complications for the Yearly Cohort of 636 Patients.
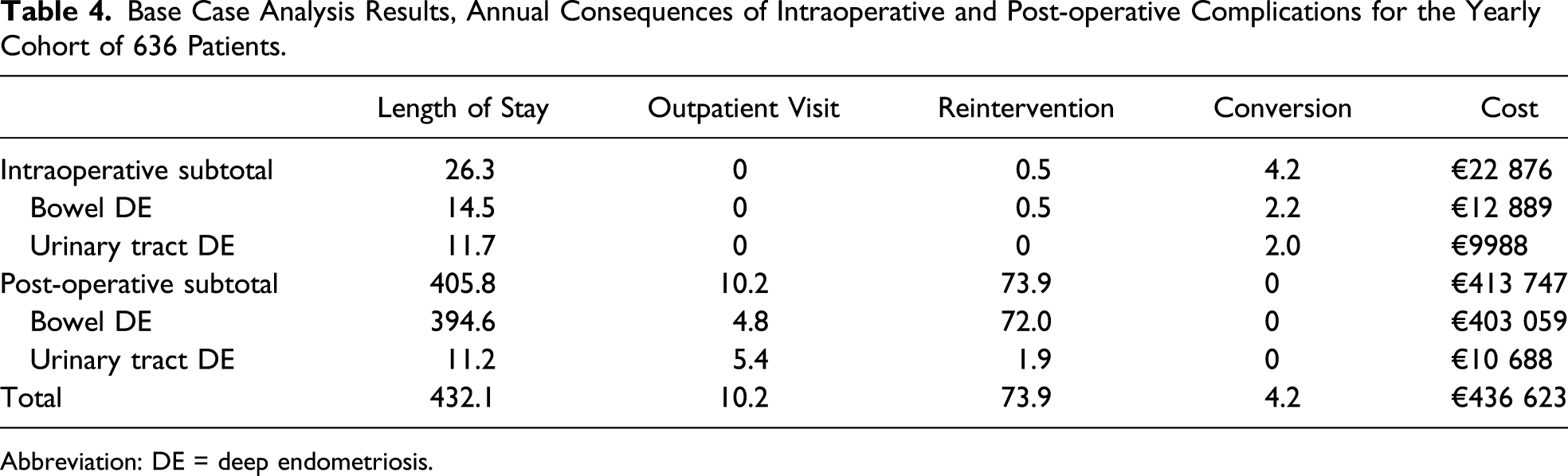
Abbreviation: DE = deep endometriosis.
Results of Scenario Analyses with Different Effectiveness Rates of Haptic Feedback on the Possible Reduction of Complications in an Annual Cohort of 636 Patients.
Results of Sensitivity Analyses Showing the Total Annual Costs Related to Complications According to the Distributions in Primary Bowel and Urinary Tract Deep Endometriosis Lesion Sites.
Discussion
This study aimed to assess the potential value in reduction of surgical complications and costs due to the use of haptic surgery during DE surgery. This was done through the use of decision analytic modelling by comparing the current standard of care, in which laparoscopic endometriosis surgery without haptic feedback is performed, and the strategy with haptic feedback added to laparoscopic instruments. Annually, a total of 57 complications could be prevented in 636 surgical procedures for DE in the Netherlands. The majority of these complications occur post-operatively. By preventing all complications included in the model, €436 623 could potentially be saved annually, which equals to €687 per patient. The largest part of these costs arises from post-operative complications, especially from late bowel perforations, rectovaginal fistulas, and anastomotic leakages. This maximum potential value (headroom) is expected to rise further when societal costs (eg costs caused by loss of work related productivity while having a colostomy) would be included in addition to healthcare costs, which were considered in this assessment. Also this study focussed on Clavien–Dindo grade III complications, while several Clavien–Dindo grade I/II complications, such as voiding dysfunction, also result in increased medical costs and social impairment. 43 In addition, complication rates in smaller centres with less experience in treating DE are likely to be higher than the rates reported by expert centres for DE in the literature, which were used as input for the model.
There is considerable variation in the literature on the reporting of complications after bowel or urinary tract surgery, which greatly influences the outcomes of the model, as is shown by the sensitivity analyses. In addition, the literature on surgical treatment of DE is of mediocre to poor quality overall, consisting mostly of case series and retrospective cohort studies, which is believed to result in overestimating the beneficial effect of surgery and under-reporting the total number of complications. Therefore, the room for improvement might be larger in practice.
Since the effectiveness of haptic feedback on reducing intraoperative and post-operative complications in complex endometriosis surgery is currently unknown, we first of all conducted a headroom analysis which did not include costs of research and development. Results of the headroom analysis show the room for improvement in this disease area, if haptic feedback would be able to prevent all selected complications. However, a 100% reduction of complications is unrealistic. We therefore also showed the potential value in case haptic feedback would be able to reduce less complications, although no literature describes the effectiveness of haptic feedback on reducing complications yet.
Some study limitations merit consideration. Since there was no clinical literature available on which types of intraoperative and post-operative complications haptic feedback might have an effect, an expert panel (consisting of leading gynaecologists and surgeons) made a selection of both intraoperative and post-operative complications (due to undetected intraoperative injury) on which they expect a reduction by using haptic feedback. Their selection was based on the available literature which has proven the assumed benefits of haptic feedback in preclinical and veterinary studies.11,12,21 The assumed effects which were taken in account are reduced applied gripping forces and better recognition of tissue properties including arterial pulsations resulting in a reduction of a selection of surgical complications.
According to SAGES guidelines, the first step for introducing a new technology or technique should be a HTA to assess potential improvement in health care and potential reduction of associated costs. 17 The next step is preclinical research, for which excellent results are reported in in vitro 11 and in vivo models 21 regarding the added value of haptic feedback in laparoscopic instruments. Finally, this technology should be introduced in clinical practice; however, physicians should be trained first and patients should be informed pre-operatively. 17
The weakness related to the use of HTA is in general the dependence on the assumptions that have to be made to build the models. These assumptions are made on literature, interviews for clinical experience, and in this study, interview according the to a Delphi procedure. However, in this study, we had to use the distribution of incidence of complications reported in the literature which showed a wide variation in outcomes. Moreover, as has been mentioned earlier, the exact impact of haptic feedback in the clinical practice is also unknown and has to be estimated based on scarce preclinical studies and personal experience. However, this study demonstrates that the potential value for improvement in DE by using haptic feedback instruments is considerable, mostly caused by the potential prevention of major post-operative complications. Sensitivity and scenario analyses showed that the number of complications which could be prevented and the potential cost savings are still considerable when key model parameters are varied.
This study demonstrated that the potential value for improvement in DE laparoscopic surgery by using haptic feedback instruments is considerable, mostly caused by the potential prevention of major post-operative complications.
Supplemental Material
SRIB_10.1177_1553350620944267 – Supplemental Material for Potential Value of Haptic Feedback in Minimally Invasive Surgery for Deep Endometriosis
Supplemental Material, SRIB_10.1177_1553350620944267 for Potential Value of Haptic Feedback in Minimally Invasive Surgery for Deep Endometriosis by Stijn L. Vlek, Rens Burm, Tim M. Govers, Michel P. H. Vleugels, Jurriaan B. Tuynman and Velja Mijatovic in Surgical Innovation
Footnotes
Author Contributions
Study concept and design: Stijn L. Vlek, Rens Burm, Tim M. Govers, Michel P. H. Vleugels, Jurriaan B. Tuynman, and Velja Mijatovic
Acquisition of data: Rens Burm, Tim M. Govers, and Michel P. H. Vleugels
Analysis and interpretation: Stijn L. Vlek, Rens Burm, Tim M. Govers, and Michel P. H. Vleugels
Study supervision: Michel P. H. Vleugels, Jurriaan B. Tuynman, and Velja Mijatovic
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.