
Abstract
Background. Retention of surgical sponges in patients is a relatively frequent medical malpractice. To prevent it, the surgical sites are scanned using X-ray. However, using radiography in the operation room induces X-ray exposure for both patients and staff. To prevent such issues, a novel sponge counting system was developed. Each surgical sponge used in common hospitals is composed of single radiopaque fibers. Methods. The proposed system scans surgical sponges to estimate their fiber length (EFL) and returns the number of it. In this study, an optimal image acquisition protocol was determined that allows an accurate count of sponges. X-ray doses and multi-angle image procedures were tested. Results. Measurement trials were performed and compared for both dry and blood-soaked sponges. As a result, the X-ray dose of 50 kV and 600 μA and the acquisition of 180 images per sample yielded an accurate EFL. The 180-image protocol achieved good performance in this study and allowed counting of one package of 10 sponges in 226 seconds. For these settings, a significant correlation was found between the actual number of sponges and the estimated fiber lengths. Additionally, the performance of the system was similar for either dry or blood-soaked items. Conclusion. The proposed system could accurately count surgical sponges and is a promising option in preventing the accidental retention of surgical sponges.
Introduction
According to the World Health Organization (WHO), the retention of surgical sponges inside patients’ bodies is a major medical malpractice. 1 It is reported that this can cause serious complications such as malignant gossypiboma, whereby a granuloma forms around a foreign object such as sponges.2-4 Although preventive measures are taken by hospital staff, to date several such cases have been reported in the literature.
Accidents involving retained surgical items (RSIs) occur once in every 10 000 surgeries, 69% of which involve surgical sponges. 5 Perioperative nurses are usually required to count sponges manually during the surgery. To comply with WHO guidelines, double-checking should also be performed routinely. 1 However, the manual method alone is somewhat ineffective in significantly reducing the risk of surgical sponge retention.6,7 For instance, Gawande et al noted that counting was recorded as correct in 88% of RSI accidents. 5
Because surgical sponges already have one radiopaque polypropylene fiber, scanning the surgical site using X-rays is the preferred prevention method to remove uncertainty about the presence or absence of such items within a patient’s body.8,9 However, this procedure induces additional exposure to X-rays, and RSI accidents are recurrently reported in the literature.10-14 Because the surgical environment is highly complex, human error can easily occur without technical support. New technology should therefore be developed to facilitate surgical sponge counting and address the issue of the risk of surgical sponge retention. 15
To support the perioperative staff, a new system that is able to count surgical sponges externally during the operation using low-dose X-ray scanning to count sponges was designed. The present study has two goals: To determine the optimal X-ray dose and number of images necessary to realize a scan of surgical sponges. To assess the performance of the system by counting both dry and blood-soaked sponges.
Method
Description of the System
The system is composed of a radiographic unit and computer (Dell PC with Windows 7) (Figure 1). The radiographic unit consists of an X-ray tube, a flat panel detector (FPD), and a rotating platform. For measurement, sponges are inserted in a container, which is placed on the platform in the radiographic unit. X-rays go through the container and are detected by the FPD. The platform is able to rotate to allow for multi-angle image acquisition. The internal wall of the radiographic unit is made from lead, which prevents radiation leakage. During the system’s conception, leakages were measured and found to produce no more than .5 μSv/h at a dose of 50 kV and 600 μA. Surgical sponge counting system.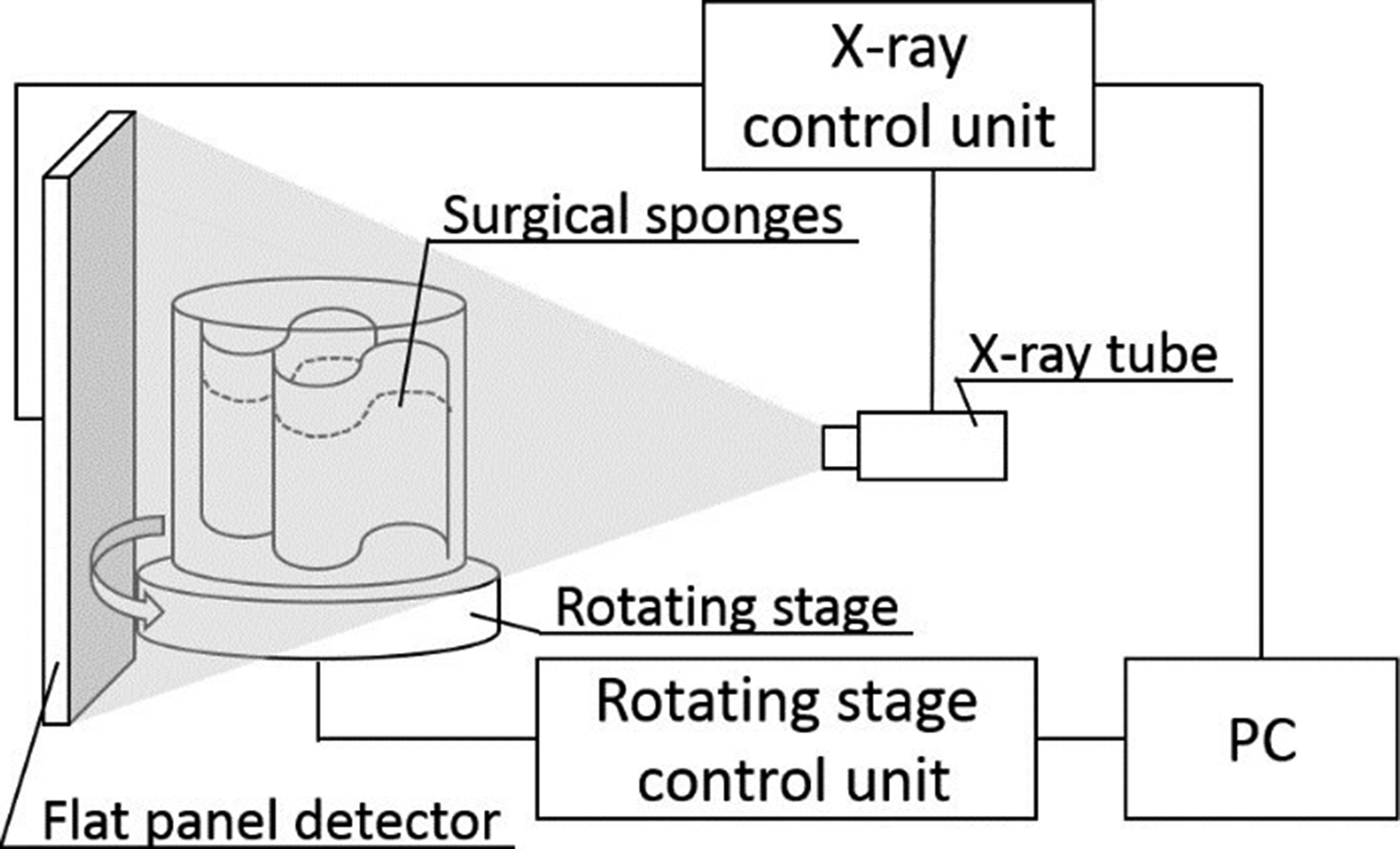
Sponge Preparation and Measurements
The measurement protocol is conceived to match as far as possible the method currently used by perioperative nurses to manually count sponges. To achieve this task accurately and efficiently, the sponges are gathered and crumpled to make small packages of 5 or 10 items. The number of sponges per package depends on the hospital guidelines. 1 After surgery, these packages that were used and extra sponges that were used and unused, each less than 10 items, are counted by nurses. They compare the totals counted before and after surgery. Finally, medical staff counts the packages during surgery and the extra sponges after surgery.
The new radiographic system in this study also requires sponges to be bundled into 1- to 10-item packages. Finally, each package is inserted into each container, which is placed on the platform in the radiographic unit (Figure 1). In these evaluations, the system used a particular type of sponge (Hakujuji Co, Ltd, Multi XP gauze BK, 300 mm × 300 mm) that is used in abdominal surgery and already has a radiopaque polypropylene fiber.
Multi-angle image acquisition allows reconstruction of 3-dimensional (3-D) images by giving information not only on the object’s width and height but also its depth. As surgical sponges are 3D objects, multi-angle acquisition was considered the best imaging strategy to count them accurately. The platform rotates 2π rad in a horizontal direction and can stop every specified degree.
Estimate Number of Sponge Method Using Image Processing
A common computed tomography algorithm was used to reconstruct the 3D images, as shown, for example, by Scarfe and Farman.
16
Voxel 3D coordinates are determined, and the volume and surface of the fibers are estimated. Figure 2 shows the stereoscopic image of a radiopaque fiber that can be identified using our system. We assumed that fibers have the shape of a square prism, and the diameter can be calculated as follows Two-dimensional to three-dimensional reconstructed image of a surgical sponge fiber.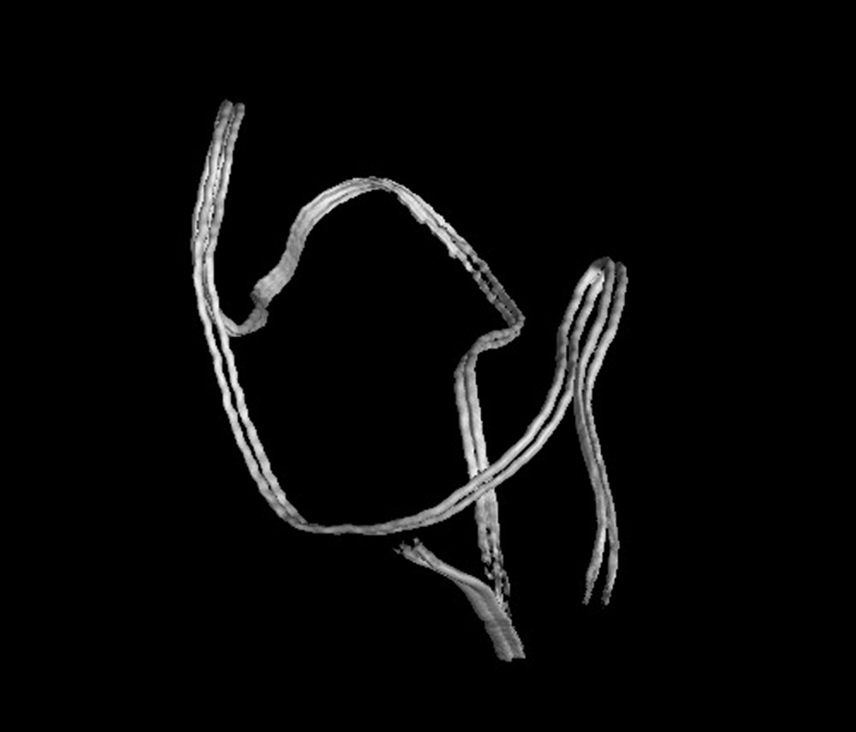




Determination of the Optimal X-ray Dose
The contrast of radiographic images is affected by the X-ray dose. For instance, if the power (ie, voltage and current) is too high, most of the X-rays go through the sponges. As a result, there is no contrast between radiopaque and nonradiopaque objects in these images. By contrast, if the power is too low, X-rays cannot go through the sponges.
Therefore, measurements were performed at different power levels. Three different voltages (40, 45, and 50 kV) and 3 different currents (400, 500, and 600 μA) were changed sequentially, resulting in nine possible experimental conditions. First, 5 dry sponges were crumpled and placed in the container to be measured. Following it, the same test was repeated with a package of blood-soaked sponges. Swine blood was used to soak sponges.
Evaluation of the Number of Images
To make the method more suitable for perioperative duties, we attempted to shorten the time of measurements by determining the minimal number of images necessary to accurately count the sponges. Five blood-soaked sponges were crumpled and placed in the container. Then, 360 images were completed with the platform stepping every π/180 rad. The operation was repeated with the platform stepping at 2π/180, 4π/180, and 8π/180 rad acquiring 180, 90, and 45 images, respectively. For each condition, the EFL was assessed, and the coefficient of variation was calculated. The whole protocol was completed 5 times with the same sample. For these measurements, the optimal X-ray dose determined as described in the previous section was used. To evaluate accuracy, coefficient of variation was calculated.
Repeatability of EFL Value
The coefficient of variation that average values were divided by the SD has to be less than ±5%. Otherwise, for instance, a package of 10 sponges could be miscounted as 9 or 11 items. Four sets of 1, 3, 5, and 10 blood-soaked sponges were crumpled and placed in the container and exposed to X-rays. For each set, the measurement was performed 5 times and the variance between EFL values was calculated. For these measurements, the optimal X-ray dose and the optimal number of images determined as described in the 2 previous sections were used.
To estimate the number of surgical sponges based on the EFL, examining the correlation between the number and EFL is required. Thus, this study is required to evaluate the ability of our system to count 10 items. First, packages of 1-10 dry sponges were processed by the system to determine EFL values. Then, the sponges were soaked with blood, crumpled in packages of 1-10 sponges and measured again. For each condition, measurements were performed 3 times using the optimal X-ray dose and the optimal number of images determined as described above. The system produced an EFL value for each package and each measurement (total 60 measurements). EFL values were compared with the actual number of sponges by a Pearson correlation test using SPSS Ver.20 (SPSS, Chicago, Illinois, USA).
Result
Optimal X-ray Dosage and Number of Images
EFL values are presented in Figure 3. Dry-sponge EFL values remained relatively stable regardless of voltage (40-50 kV) or current (400-600 μA). For blood-soaked sponges, EFL values showed important variability at 40 kV depending on the current. Such a magnitude of error is thought to induce miscounting. Estimated fiber length values of each X-ray dose given in the count system: Values are presented as one data point corresponding to one measurement.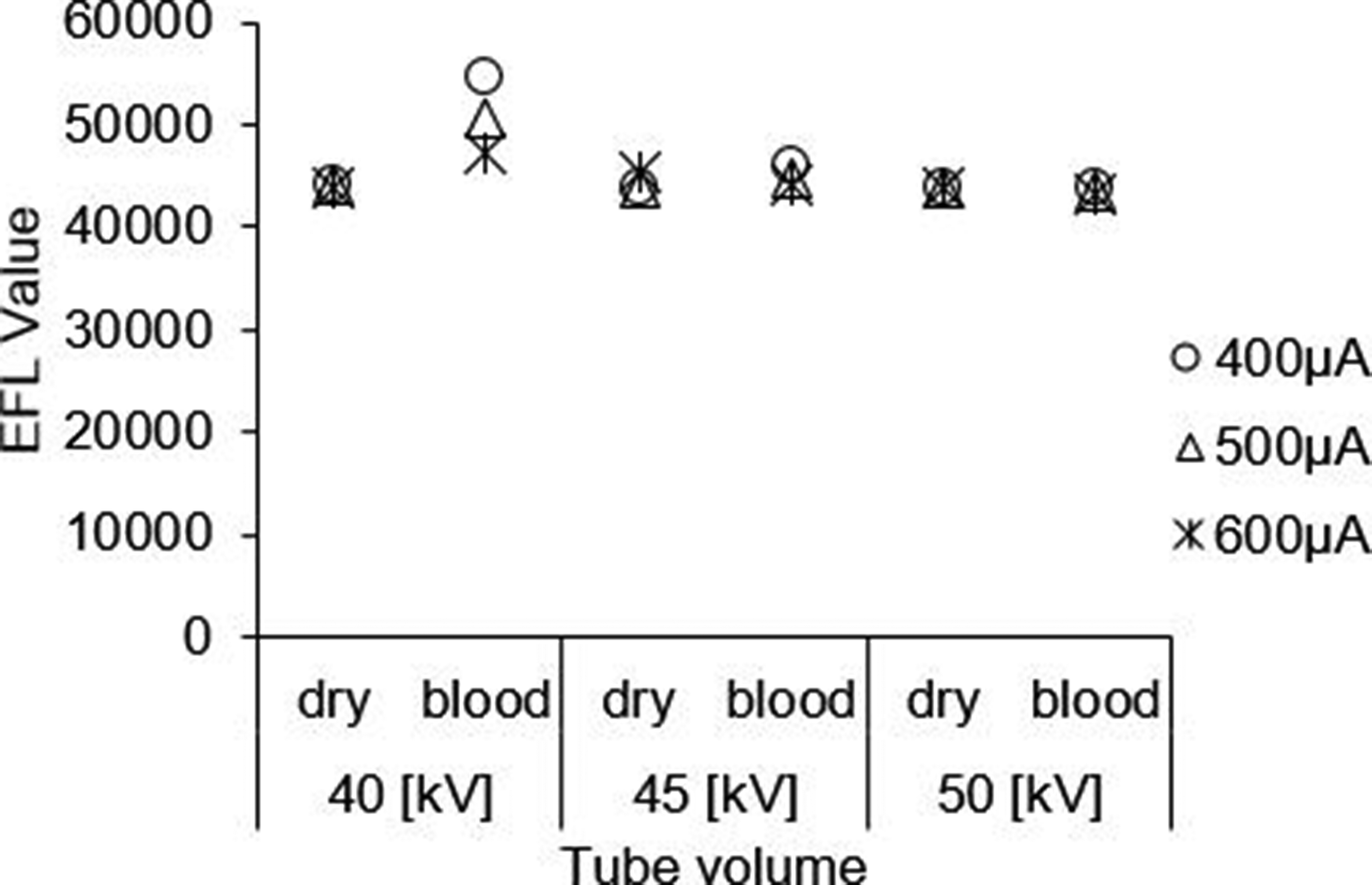
Validation of the Number of Radiographic Images.

From the above results, measurements for the remaining experiments were performed at 50 kV and 600 μA and performed using 180 images.
EFL Value and Reproducibility
Repeatability of an Estimated Fiber Length Value Using the Sponge Count System.

Sponge count validation was performed, and the EFL value rose as the number of sponges increased (Figure 4). EFL values from both dry and blood-soaked sponges correlated with the actual number of sponges (R2 = .99 for both conditions). Estimated fiber length value obtained for each number of surgical sponges.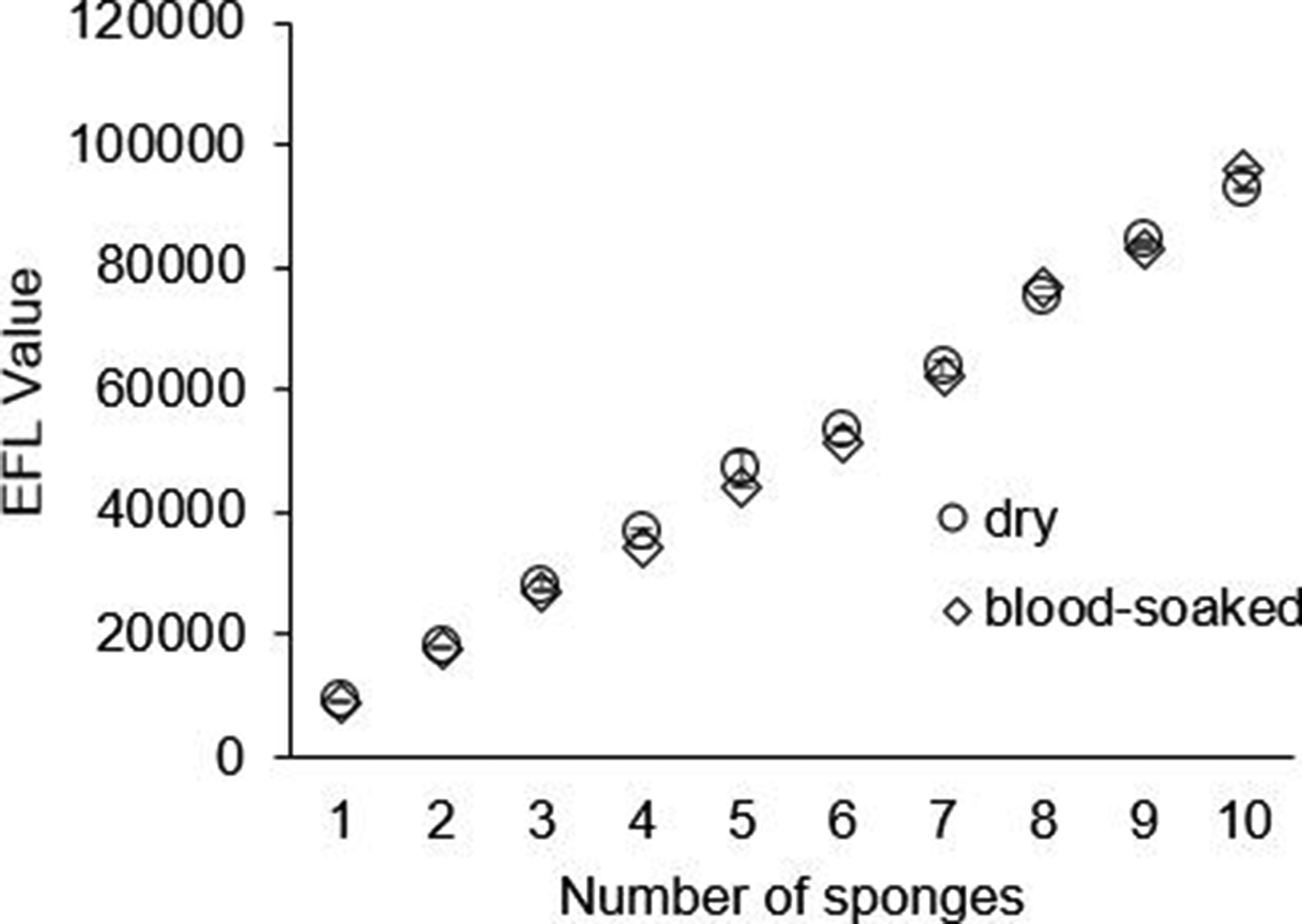
Discussion
Comparison with Other Methods
In several studies, various technologies have been proposed to assist the perioperative staff in managing surgical instruments and sponges.
One possibility consists in attaching bar codes to sponges or sponge packs. 17 This inexpensive method allows noncontact scanning with a standard barcode reader. However, 2 important limitations are mentioned. First, bar codes become unreadable if they are covered with blood. Second, bar codes have to be read one by one, which significantly lengthens the duration of the counting process. Therefore, it is difficult to use these systems during surgery.
A second method consists of attaching radiofrequency identification tags, allowing detection of sponges inside the patient’s body and instant counting.14,18-20 However, when using this method, it is necessary to attach radio frequency identification (RFID) tags to all sponges. Therefore, the system takes a lot of time before surgery. Additionally, RFID tags are costly, if single used items are attached to them.
By contrast, the radiographic method presented herein overcomes some of the aforementioned limitations. Blood-soaked sponges can be scanned and counted with the same level of accuracy as dry sponges. Additionally, normal surgical sponges without any specific attachment or tag can be used.
Optimization of Image Acquisition Procedure
The systems performance depends on the X-ray dose (ie voltage and current). The magnitude of error for blood-soaked sponges at 40 kV would induce miscounting of sponges. Measurements dedicated to the optimization of X-ray dose returned an EFL value of 45 000 for 5 sponges. To assume a positive linear relationship between the number of sponges and the magnitude of EFL, it was reasonable that the EFL value of 1 sponge would be ±9000. An EFL of 55 000 as returned at 40 kV/400 μA would potentially induce a miscount for 5-sponge packages, and an EFL of 50 000 as returned at 40 kV/500 μA would potentially induce a miscount for 10-sponge packages.
Another candidate was 45 kV. While measurements showed less variability, long-term use of radiographic systems usually induces an alteration of the X-ray tube, subsequently lowering the effective X-ray voltage. To prevent any dose-related miscounting, we selected a voltage of 50 kV to pursue the experiment. Similarly, 600 mA was selected to continue the experiment because higher current limits the magnitude of errors.
The number of images per sample is also a critical parameter. Usually, more images lead to higher quality of 3D reconstruction. In the present study, 45 and 90 images did not provide sufficient resolution, inducing important variability between successive measurements of the same sample (23 878.6 and 559.4, respectively; coefficient of variation: 15.75% and 1.15%). However, 180 images provided less EFL variation than 360 images. The measurement duration for 180 images was also shorter than for 360 images (226 vs 398 seconds). Therefore, to facilitate time management, the 180-image scanning procedure appears to be the best setting, especially if implementation of the perioperative environment is considered.
The two aforementioned settings (X-ray dose and number of images) provided repeatable EFL values. The coefficients of variation were indeed very low, between .04% and .45% depending on the number of sponges in the unit. In addition, a high correlation was found between the actual number of sponges (regardless of whether they were dry or blood-soaked) and the output EFL values. These results indicate that the selected settings yield a suitable level of performance for surgical sponge counting.
Implementation in the Current Perioperative Workflow
The specificity and size of the proposed equipment, as well as the protocol used for this study, would allow maintenance of the usual sponge-counting activity workflow. Indeed, depending on their workplace guidelines, nurses can continue to make packages of 5 or 10 sponges before inserting them into the X-ray compartment. So far, no contraindication would appear to prevent the use of such a counting system in the operating room.
The 180-image protocol achieved good performance in this study and allowed counting of one package of 10 sponges in 226 seconds (ie, 3 minutes 46 seconds). At the current medical workflow, total number of surgical sponge is counted just before the end of surgery. If this system is used, the system method requires more time than current method. Therefore, nurses count sponges using the system when 10 pieces of the sponge used have accumulated during surgery in the system workflow. By operating gauze counting in parallel with surgery, extra time for gauze counting is unnecessary. However, further studies conducted in the clinical environment are necessary to assess the usability of this system in the current perioperative workflow.
Leakage measurements performed at 50 kV and 600 μA showed a satisfying level of permeability, that is, .5 μSv/h, allowing the system to be used in clinical settings. Indeed, considering a working time of 8 h per day, 5 days a week, the occupation-related annual radiation dose would be less than 1.04 mSv for the perioperative nurse in charge. This is much lower than the 20 mSv recommended by the International Commission on Radiological Protection (ICRP). 21 By comparison, staff members operating gastrointestinal X-ray examinations are exposed to an annual dose of 3-5 mSv. Furthermore, if you were exposed to similar radiation doses during pregnancy, your total radiation exposure for 40 weeks would be .8 mSv. For pregnant women, ICRP recommends an annual radiation dose of 1 mSv or less. The system meets these requirements.
The limitation of our study is that only one product of sponge is used in this evaluation. Because various types of sponges are used in routine surgery. If different sponges are mixed in the same package when the system scans it, it may have difficulty in identifying each kind of sponge. Therefore, the counting system will be required to validate different items. However, the system concept is not completely based on automated counting but also supports manual surgical counting by nurses. Steady implementation of the new system and double-checking against nurses’ counting protocol will ensure the accuracy of the counting system.
Conclusion
This study presented a new perioperative device that is able to accurately count surgical sponges while avoiding unnecessary X-ray exposure to patients and staff. Similarly to the current manual counting protocol, sponges are collected and wrapped into 5- or 10-sponge packages and inserted into the device, which operates at low X-ray power, that is, 50 kV and 600 μA. An excellent correlation was found between the number of sponges and the device output for both dry and blood-soaked items. Our forthcoming study will focus on the effective usability of the system in a clinical setting. The implementation of such a system in the perioperative workflow has the potential to reduce the number of X-ray scans performed on the surgical site for RSI-related issues.
Footnotes
Acknowledgments
We would like to thank Dr Julien Tripette who supported editing of manuscript in English and provided us with valuable discussion.
Author Contributions
Study concept and design: Kaori Kusuda and Kazuhiko Yamashita
Acquisition of data: Kaori Kusuda
Analysis and interpretation: Kaori Kusuda, Kazuhiko Yamashita, Kiyohito Tanaka, and Shinichi Tanaka
Study supervision: Kazuhiko Yamashita and Yuji Ohta
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from the Japan Society for the Promotion of Science (grant no. KAKENHI/17K12806).