
Abstract
Background. Gatekeeper (GK) has shown to be safe and effective in patients with fecal incontinence (FI). We aimed to understand its mechanism of action by comparing pre- and post-implant change in the external anal sphincter (EAS) contractility. Methods. Study of EAS contractility was conducted in 16 FI females (median age = 69 years) before and after implant of 6 GK prostheses. Muscle tension (Tm), expressed in millinewtons per centimeter squared, mN(cm2)−1, was calculated using the equation Tm = P(ri)(tm)−1, where P is the average maximum squeeze pressure and ri and tm the inner radius and thickness of the EAS, respectively. The effect of a predefined set of covariates on Tm was tested by restricted maximum likelihood models. Results. Compared with baseline, despite unchanged tm (2.7 [2.5-2.8] vs 2.5 [2.2-2.8] mm; P = .31 mm), a significant increase in P (median = 45.8 [26.5-75.8] vs 60.4 [43.1-88.1] mm Hg; P = .017), and ri (12.4 [11.5-13.4] vs 18.7 [17.3-19.6] mm; P < .001) resulted in an increase in Tm (233.2 [123.8-303.2] vs 490.8 [286.9-562.4] mN(cm2)−1; P < .001) at 12 months after GK implant. Twelve-month follow-up improvements were also observed on Cleveland Clinic FI score (8-point median decrease; P = .0001), St Marks FI score (10-point median decrease; P < .0001), and American Medical Systems score (39-point median decrease; P < .0001). Restricted maximum likelihood models showed that years of onset of FI was negatively associated with change in Tm (P = .048). Conclusions. GK-related EAS compression positively influences muscle contractility by increasing ri, with consequent increase in Tm (length-tension relationship). Further studies are needed to confirm the long-term effectiveness of GK.
Keywords
Introduction
Fecal incontinence (FI) is a common and socially disabling condition affecting 7.8% to 9.1% of noninstitutionalized adults living in the United States, with similar sex distribution and increased prevalence with age.1-3
Pathophysiology relies on several mechanisms, a number of which are suprasphincteric, 4 explaining the wide range of investigations conducted in specialist centers for examining the morphology and function of the colon and anorectum.
Four main muscular structures maintain closure of the anal canal: the smooth muscle of the internal anal sphincter (IAS), the mixed smooth/striated longitudinal muscle, the striated muscle of the external anal sphincter (EAS), and the striated puborectalis muscle. Structural and/or functional abnormalities of the IAS and EAS are more common in females than males with FI, 5 often secondary to traumatic vaginal delivery. 6
EAS surrounds the area of highest pressure in the anal canal, both at rest and during voluntary squeeze, 7 hence playing a key role in maintaining continence. Optimal voluntary EAS contractions depend on both integrity of neural input (ie, pudendal nerves) and sarcomere length. Previous studies explored active and passive length-tension characteristics of EAS in vivo and in vitro to determine its optimal and operational length in rabbits.8,9 In a seminal work, 8 surgical manipulation of the EAS sarcomere length was first proposed as possible treatment of FI. However, restoration of the EAS sarcomere to its optimal length may not be optimally achieved by overlapping sphincteroplasty, where the degree of muscle overlap is arbitrary and not based on any scientific principles, with poorly sustained outcomes in the long term. 10
Gatekeeper (GK) is a novel therapeutic approach of FI consisting of self-expandable prostheses placed into the upper-middle intersphincteric space of the anal canal. 11 It has shown to be safe and effective in adults with FI.12,13 Based on preliminary studies exploring length-tension characteristics of EAS,8,9 we hypothesized that GK-related muscle compression may improve voluntary contractility. Therefore, we aimed to determine morphofunctional EAS changes after GK implant in a series of female patients with FI.
Material and Methods
The cohort was recruited from 23 female patients aged more than 18 years (median age = 68 [57-80] years) undergoing THD Gatekeeper Delivery System (THD SpA, Correggio, Italy) implant between October 2011 and May 2015.
The clinical outcomes of GK were explored by our group previously and the detailed description of the implant technique is published elsewhere.11,12 Inclusion criteria required symptoms of fecal ± flatus incontinence for at least 6 months prior to recruitment and occurring at least once a week, and failure of conservative management through the use of lifestyle changes or pharmacological agents. Patients with isolated flatus incontinence, inflammatory bowel diseases, uncontrolled diabetes, anal sepsis, and history of gastrointestinal cancer were excluded. Further exclusion criteria were previous history of anal surgery for FI (including injection of bulking agents), flatus incontinence in isolation, and IAS defects >45°.
Prospectively collected data at baseline and 12 months post-GK implant included the following: patient demographics; medical and surgical history; obstetric history (vaginal delivery was defined traumatic when involving the use of instruments and/or episiotomy and/or a perineal tear); Cleveland Clinic FI (CCFI) score 14 ; St Marks incontinence score 15 ; American Medical Systems score 16 ; and Fecal Incontinence Quality of Life score. 17
Study of EAS contractility was conducted before and after implant of 6 GK prostheses by measuring muscle tension (Tm), expressed in millinewtons per centimeter squared, mN(cm2)−1, and calculated using the equation Tm = P(ri)(tm)−1, where P is the intraluminal pressure during average maximum voluntary contraction, ri the inner radius of the EAS, and tm its thickness. Anorectal manometry (Model Solar GI, 24 water-perfused channels; EB Neuro, Florence, Italy) provided P, while ri and tm were measured by endoanal ultrasound (Model 1850, equipped with a system for 3-dimensional reconstruction; BK Medical, Copenhagen, Denmark). All baseline endoanal ultrasound measurements were performed in the middle anal canal (ie, level where the EAS forms a complete ring) at odd hours (1, 3, 5, 7, 9, and 11 o’clock). All measurements were repeated at 12-month follow-up post-implant at the same level, where possible. Mean values of ri and tm were derived and used to calculate Tm (Figure 1). The maximal cross-sectional distance (mm) between the cranial and caudal edges of the most proximal and distal prostheses, respectively, was also measured as a surrogate of longitudinal prosthetic displacement at 12-month follow-up post-implant.
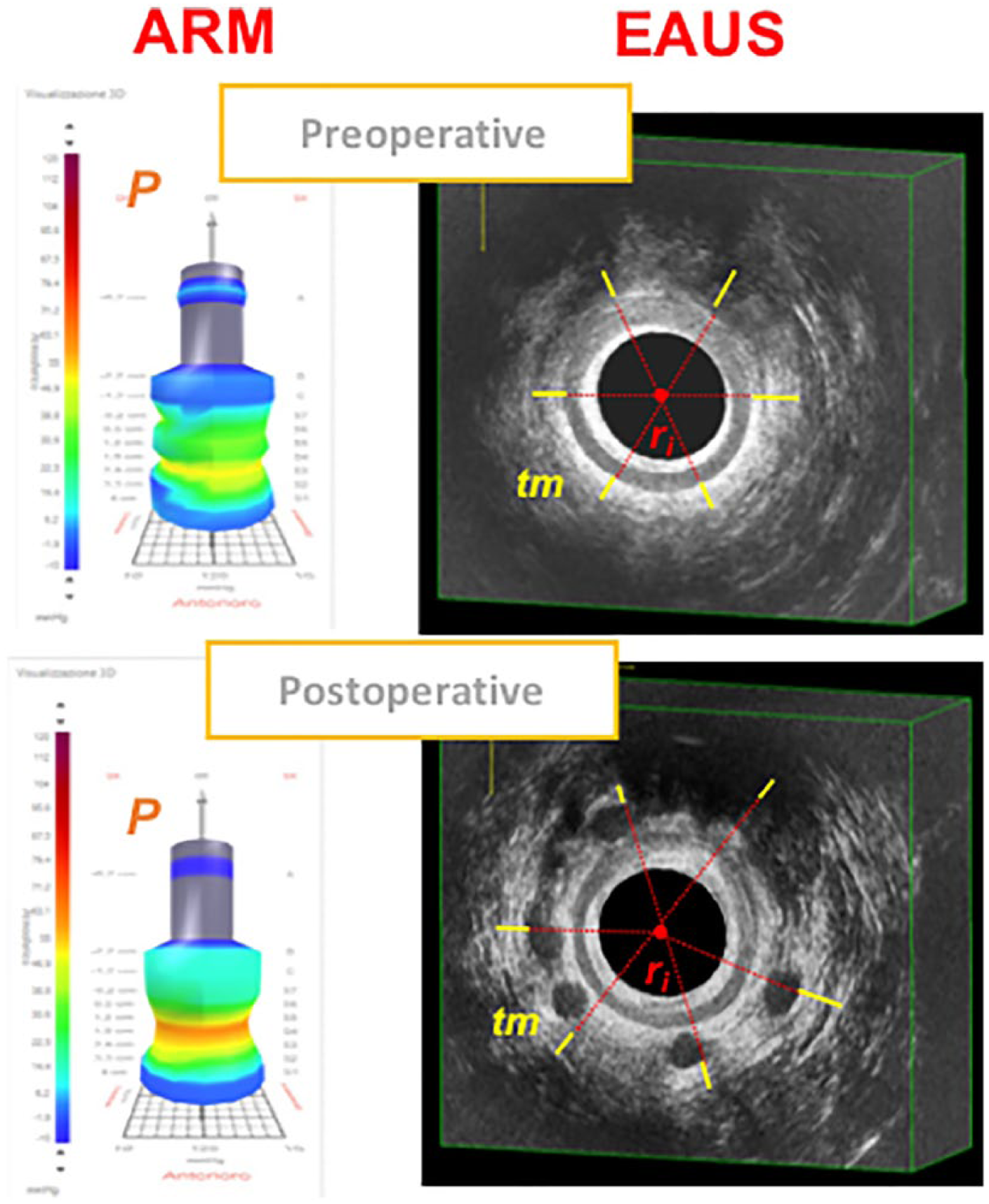
Morphofunctional changes of the external anal sphincter (EAS) detected by ARM (anorectal manometry and EAUS (endoanal ultrasound) before and 12 months after Gatekeeper implant. P = intraluminal pressure during average maximum voluntary contraction; ri = inner radius of the EAS; tm = EAS thickness.
Anatomical sphincter defects were defined by a discontinuity of the muscle ring. Degeneration/atrophy was identified by thin, poorly defined sphincters, usually with heterogeneous increased echogenicity, often making them difficult to distinguish from surrounding structures.
Rectal sensory testing was assessed by inflating a latex balloon with air at 2 mL/s and determining the threshold volumes for first constant sensation, defecatory desire (DDV), and maximum tolerable volumes (MTV). Rectal hypersensitivity (RH) was defined by a DDV <60 mL and/or a MTV <90 mL. 18
All studies were performed with patients in the left lateral position and by the same investigator (LD) who was blinded at follow-up to baseline results.
Statistical Analysis
Continuous data were presented as median with first and third quartiles. Pre- versus post-implant data were compared using the Wilcoxon signed-rank test due to skewed distribution. Fisher’s exact test was used for analysis of categorical data.
To take into account the between- and within-person variability, univariable and multivariable linear mixed models were fitted by restricted maximum likelihood: mean post- versus pre-implant change in Tm was adjusted by age, number of years since first onset of FI, number of vaginal deliveries, history of traumatic vaginal delivery, and CCFI score.
A simple linear regression was fitted between ΔCCFI (post-implant − pre-implant values) and longitudinal prosthetic displacement at 12 months post-implant.
All analyses were performed in STATA 15 (StataCorp LLC, College Station, TX).
Results
Twenty-three patients underwent GK implant in the study period. Of these, 7 patients were excluded for the following reasons: previous history of anal surgery for FI (n = 3); flatus incontinence in isolation (n = 2); and IAS defects >45° (n = 2).
Median age was 69 years (first and third quartiles = 67-76 years). A total of 14/16 (87.5%) patients had history of vaginal deliveries, with 12/14 (85.7%) being traumatic (Table 1).
Patients’ Characteristics at Baseline.
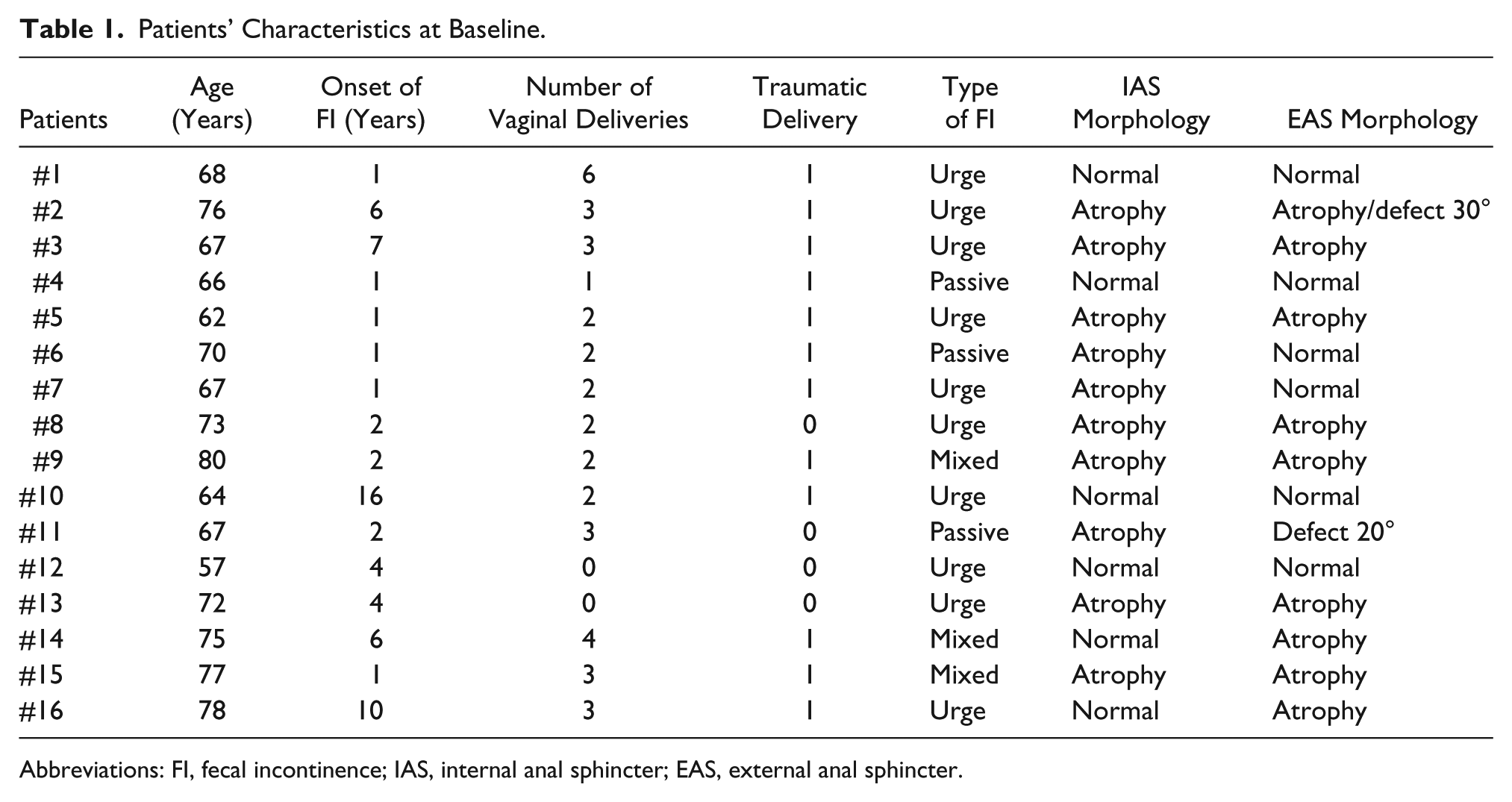
Abbreviations: FI, fecal incontinence; IAS, internal anal sphincter; EAS, external anal sphincter.
Isolated IAS defects and degeneration/atrophy were found in 0 (0%) and 10 (63%) patients, respectively. Isolated EAS defects or degeneration/atrophy were found in 2 (12.5%) and 8 (50%) patients, respectively. One (6.3%) patient expressed both EAS abnormalities. Combined IAS/EAS abnormalities were found in 8 (50%) patients. Compared with baseline, sphincter morphology remained unaltered at 12-month follow-up.
Change in EAS Muscle Tension (Tm)
Compared with baseline, despite unchanged tm (2.7 [2.5-2.8] vs 2.5 [2.2-2.8] mm; P = .31mm), a significant increase in P (median = 45.8 [26.5-75.8] vs 60.4 [43.1-88.1] mm Hg; P = .017) and ri (12.4 [11.5-13.4] vs 18.7 [17.3-19.6] mm; P < .001) resulted in an increase in Tm (233.2 [123.8-303.2] vs 490.8 [286.9-562.4] mN(cm2)−1; P < .001) at 12 months after GK implant (Table 2).
Study of the EAS Contractility at Baseline and 12 Months After Gatekeeper Implant a .
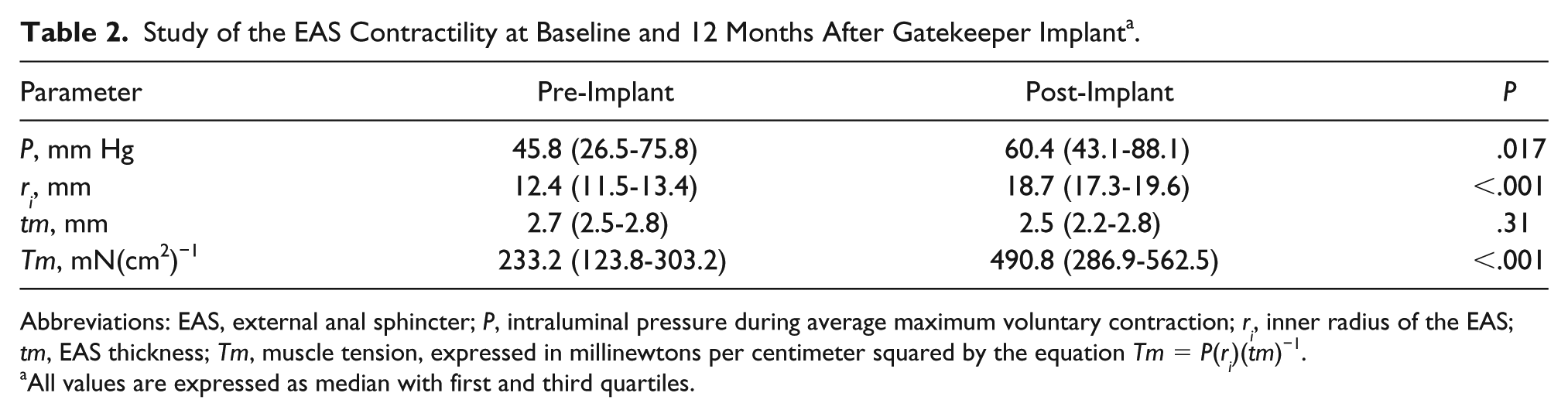
Abbreviations: EAS, external anal sphincter; P, intraluminal pressure during average maximum voluntary contraction; ri, inner radius of the EAS; tm, EAS thickness; Tm, muscle tension, expressed in millinewtons per centimeter squared by the equation Tm = P(ri)(tm)−1.
All values are expressed as median with first and third quartiles.
The univariable model estimated a ΔTm (post-implant − pre-implant values) of 227.9 mN(cm2)−1 (95% confidence interval [CI] = 159.0-296.9), which was statistically significant at P < .0001. Change in Tm was smaller after accounting for the predefined set of covariates, amounting to 176.3 mN(cm2)−1 (95%CI = 53.8-298.8) and remaining statistically significant at P < .001 (Table 3).
Restricted Maximum Likelihood Mixed Models to Examine the Effects of Fixed Variables on Change in Muscle Tension (Tm) After Gatekeeper Implant.
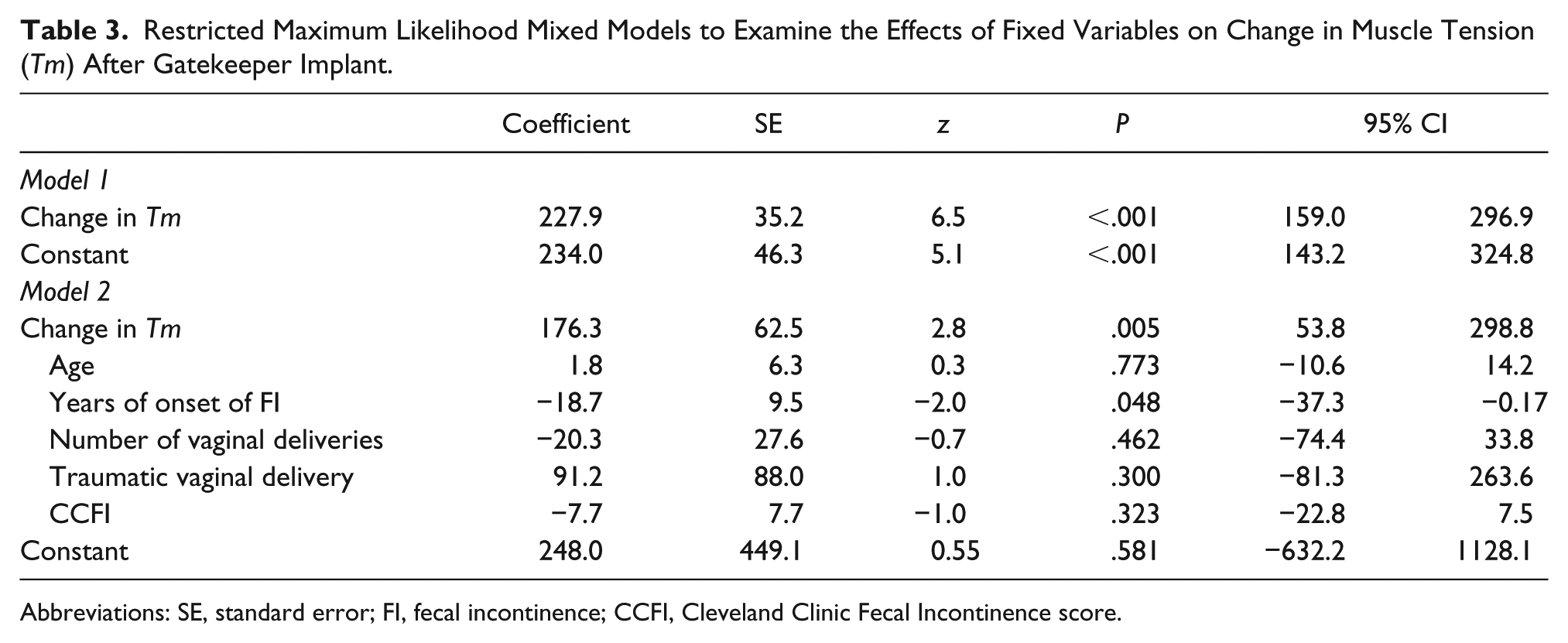
Abbreviations: SE, standard error; FI, fecal incontinence; CCFI, Cleveland Clinic Fecal Incontinence score.
The association between the set of covariates and Tm showed that Tm decreased by 18.7 mN(cm2)−1 (95% CI = −37.3 to −0.17) per each year of onset of FI. Such finding was borderline statistically significant at P = .048.
Rectal Sensory Testing
Compared with baseline values, no significant changes on all rectal sensory thresholds were found at 12-month follow-up (first constant sensation, median with first and third quartiles = 50 [41-60] vs 50 [40-60] mL, P = .68; DDV = 100 [83-120] vs 100 [80-113] mL, P = .39; and MTV = 160 [123-180] vs 140 [100-175] mL; P = .46). RH was diagnosed in 3 (19%) patients preoperatively and 2 (13%) patients postoperatively.
Clinical Outcomes
Statistically significant improvements in CCFI, St Marks Incontinence, and American Medical Systems scores were observed at 12-month follow-up, with median pre- versus post-implant decrease of 8 (P = .001), 12 (P < .001), and 39 points (P < .001), respectively (Table 4). Furthermore, a higher proportion of patients were able to defer defecation for more than 5 minutes following GK implant, although not reaching statistical significance (4/16 vs 12/16, respectively; P = .25). Moderate improvements in all 4 FI Quality of Life domains were observed at last follow-up, with the largest increase achieved in self-perception (median pre-implant = 3.2 [2.0-3.9] vs post-implant = 3.8 [2.5-4.3]; P = .03; Table 3).
Change in Symptoms and Quality of Life Scores From Baseline to 12 Months After Gatekeeper Implant a .
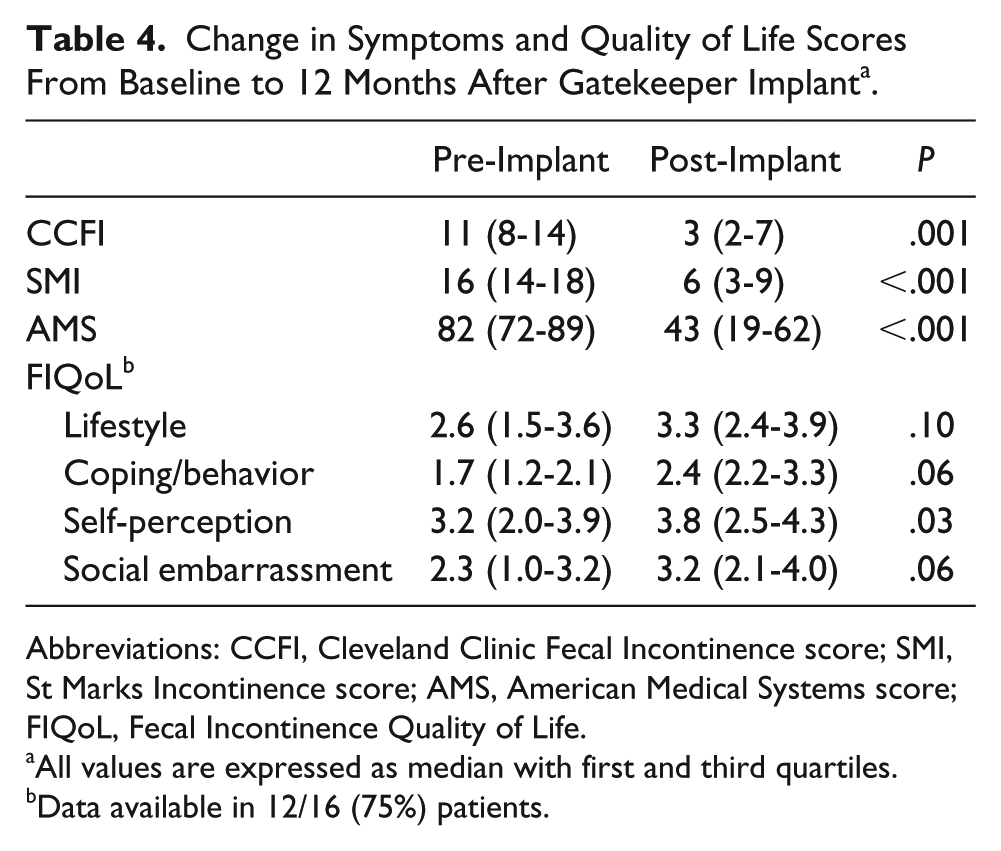
Abbreviations: CCFI, Cleveland Clinic Fecal Incontinence score; SMI, St Marks Incontinence score; AMS, American Medical Systems score; FIQoL, Fecal Incontinence Quality of Life.
All values are expressed as median with first and third quartiles.
Data available in 12/16 (75%) patients.
Simple linear regression showed a negative correlation between ΔCCFI (post-implant − pre-implant values) and cross-sectional distance between the most proximal and distal prostheses (median with first and third quartiles = 35 [30-38] mm), with 0.29-point per mm decrease in CCFI score (P = .017; Figure 2). The proportion of variability (R2) explained by this model was equal to 34.3%.
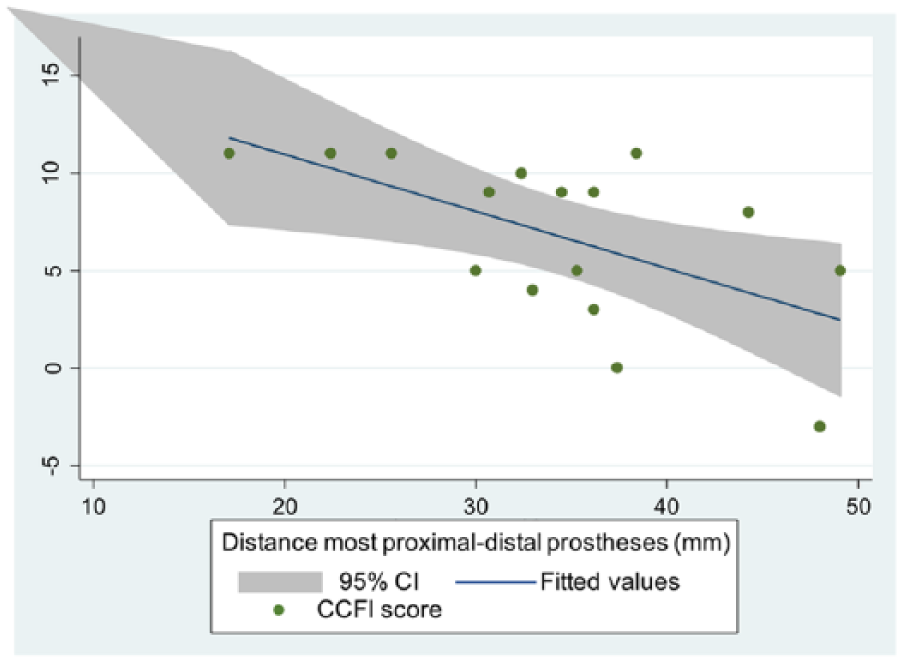
Simple linear regression showing the correlation between ΔCCFI (post-implant − pre-implant values) and cross-sectional distance between the most proximal and distal prostheses. CCFI = Cleveland Clinic Fecal Incontinence score; 95% CI = 95% confidence interval.
Discussion and Conclusion
Key Results
Quantitative estimates of EAS compression after GK implant, expressed as change in Tm, can be easily assessed using conventional diagnostic tools. Our data showed that female patients with FI achieve significant improvements in voluntary contractility after GK implant in the medium term. Longitudinal prosthetic displacement negatively correlates with symptom improvement.
Limitations
The current study has several limitations, including its retrospective nature and small sample size. However, restricted maximum likelihood inference with unstructured covariance matrix was adopted to overcome the limitations of other statistical approaches when dealing with small sample sizes, skewed predictors, and nonindependence in the outcome data, producing unbiased estimators. 19 The correlation between longitudinal prosthetic displacement and symptom improvement was meant to be exploratory, and it deserves confirmation on a larger patient population and adjusting for potential confounders.
Interpretation
Despite the above-mentioned limitations, this is the first study supporting the hypothesis that morphofunctional changes in EAS may lead to improved squeeze function after GK implant.
Interestingly, previous animal studies from the same institution showed that the optimal muscle length is longer than the muscle length at which EAS operates in vivo,8,9,20 suggesting that restoring EAS sarcomere length to its optimal length by surgical plication may improve anal canal function with sustained effects over time. 9 However, compared with overlapping sphincter repair, restoration of the optimal EAS sarcomere length is much more difficult to achieve by GK implant, not least for a less reliable tactile feedback inherent in the mini-invasive nature of the technique. We hypothesize that the SphinKeeper procedure 21 may further enhance sarcomere length by providing the implant of a larger number and longer prostheses than GK.8-12 Future research should address whether anal sphincter distensibility (already known as indirect marker of suboptimal muscle length) 22 may predict outcome after GK or SphinKeeper implant.
Obstetric trauma is considered the principal etiologic factor for FI in women. 23 In our series, this was sustained by 86% of females with history of vaginal deliveries. Prevalence of combined IAS/EAS abnormalities was 50%, similar to that reported by Townsend et al in a cohort of 100 females (47%). 5 An in vivo rabbit study suggested that altered EAS muscle healing (eg, increase in the collagen content and loss of normal myoarchitecture) represents the main pathophysiological mechanism of impaired EAS function 3 months following experimental injury. 24
Compared with baseline, a higher proportion of patients achieved ability to defer defecation for more than 5 minutes. However, this did not reach statistical significance, primarily likely due to the small sample size. Indeed, in a previous multicenter prospective study of 54 patients (69% females) a 23% improvement on this outcome was observed at 1 year following GK implant (P < .001). 12 Furthermore, a nonnegligible proportion of patients in our series were diagnosed with RH (19%), which is known to correlate with increased bowel frequency, reduced ability to defer defecation, increased pad usage, and negative lifestyle effects. 18
Generalizability
GK-related EAS compression improves EAS contractility by increasing ri, with consequent increase in Tm (length-tension relationship). Such a functional gain should not be considered as a learnt effect since none of the patients underwent pelvic floor physiotherapy after GK implant.
Nevertheless, our findings should be interpreted with caution as exclusively based on analysis of female patients. Hence, they are not generalizable to the entire population of patients with FI. Future studies with a larger sample size are needed to validate these results, with possible outcome comparison between GK and SphinKeeper.
Footnotes
Author Contributions
Study concept and design: UG and CR
Acquisition of data: UG, VDS, FL, LD, MG
Analysis and interpretation: GLDT, UG, and CR
Study supervision: CR and AP
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CR pioneered Gatekeeper™ in patients with fecal incontinence; he has served as a speaker, consultant, and proctor during several congresses and training courses on Gatekeeper. UG, VDS, AP, FL, LD, GLDT, and MG declare no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.