
Abstract
Objective. The aim of this study is to compare the cosmetic evaluation of autologous fat transfer (AFT) for various indications between surgeons and different laymen groups. Background Data. Despite the upsurge in AFT scientific/clinical interest, objectifying satisfaction has only recently progressed beyond simple Likert-type/Visual Analog Scales. Furthermore, differences in satisfaction between laymen and surgeons has not been thoroughly studied. Method. A photo comparison study between European plastic surgeons and different laymen groups was conducted to investigate agreement on cosmetic evaluation of AFT. Three sets of preoperative/postoperative photographs illustrating patients treated with External Vacuum Expansion (EVE) + AFT for various indications in breast surgery were scored according to the Harris Scale, and the interrater agreement was analyzed using Cohen’s κ. Results. The overall agreement between the surgeons and the groups of former augmentation, control group, and deep inferior epigastric artery perforator patients was fair, moderate, and substantial, respectively. Interrater agreements among different laymen groups and surgeons from different countries among themselves was substantial to almost perfect. Finally, we found that laymen are generally more optimistic about postoperative results than surgeons. Conclusion. In our study, former augmentation patients showed the lowest agreement with surgeons, in the cosmetic appreciation of EVE + AFT and this group might benefit from a more thorough preoperative consultation regarding expectations when choosing AFT. However, overall laymen tend to be more optimistic about postoperative results and surgeon education in general does not seem influenced by surgeon nationality. The significant differences between surgeons and laymen in the cosmetic evaluation of EVE + AFT justifies further studies that focus on the qualitative aspects of these differences to further balance patients’ and surgeons’ expectations.
Introduction
Autologous fat transfer (AFT) is becoming increasingly popular in various aspects of plastic surgery. Concerning the female breast, the first description dates from 1893 with Neuber attempting transfer of bulk volumes of fat. 1 Since then, other notable developments have been the advent of liposuction with Bircoll, in 1987, describing the injection of autologous fat to the breast,2-4 and the prohibition of its use, the same year, by the American Society of Plastic Surgeons because of the possible carcinogenic effects and the induction of radiographic changes that could impede future diagnostics. 5 Furthermore, with the first standardized protocol described by Coleman in 1995 6 leading to an increase in the number of objective and reproducible study designs, the Fat Graft Task Force of the American Society of Plastic Surgeons, in 2009, stated that the procedure was no longer prohibited. 7 This resulted in large volume studies, systematic reviews, and meta-analysis, showing the efficacy and safety in terms of improving volume retention and acceptable oncological and radiological safety, respectively.8-12 With this gradual reassurance of the safety of the technique, the authors believe the aim for further research is to lean more toward efficacy since this is an area where improvement is still to be gained. Some studies describe volume retention but in a heterogenetic way. Moreover, patient satisfaction is being described occasionally, and only recently with the use of validated questionnaires like the Breast-Q.13-16 Also, the satisfaction of patients and surgeons is generally reported in rates, and comparisons in the cosmetic appreciation of the procedure between groups of surgeons and patients based on background and experience has not been thoroughly studied. Finally, in a recently conducted European survey study, performed by the same authors, the surgeon satisfaction in general (based on their own experience with AFT) did not differ between countries; however, it is interesting to see if the same holds true in the cosmetic evaluation of AFT on a preoperative/postoperative photographical basis for different breast surgery indications.
Therefore, the aim of this study is to report on the interrater agreement between European surgeons mutually as well as between surgeons and different groups of laymen in the cosmetic evaluation of visual illustrations of patients treated with EVE (also known as Breast Enhancement and Shaping System or BRAVA) + AFT.
Methods
An international, cross-sectional, observational, photo comparison study among European plastic/breast surgeons and Dutch laymen was conducted. The photographs were collected from a high-volume center in the United States (Miami Breast Center, Biscayne, FL, courtesy of Dr R. Khouri) and displayed the pre- and postoperative appearance of patients treated with EVE + AFT for various indications (eg, breast augmentation, breast reconstruction, and contour defects), shot in direct anteroposterior and bilateral oblique directions. The photographs were stripped of any information that might identify the patient and were presented using an online questionnaire (SurveyGizmo, Boulder, CO) supplemented with a brief explanatory text of the procedures leading up to the postoperative effect (see Figures 1-3). The respondents were asked to score the photographs using the Harris Scale (HS): excellent, good, fair, or poor.
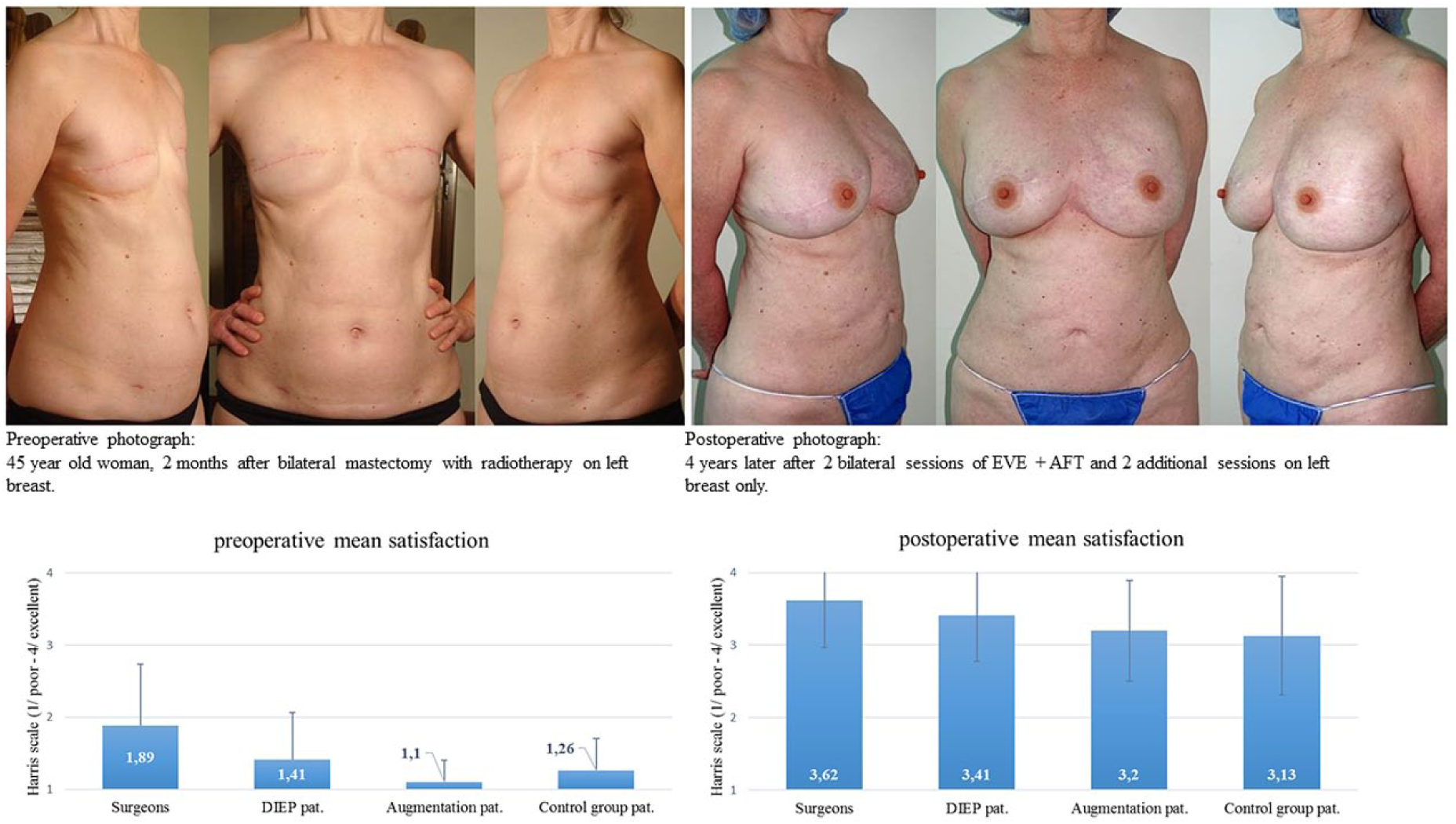
Pre- and postoperative appearance of EVE + AFT in total bilateral breast reconstruction and mean satisfaction scores (Harris Scale).
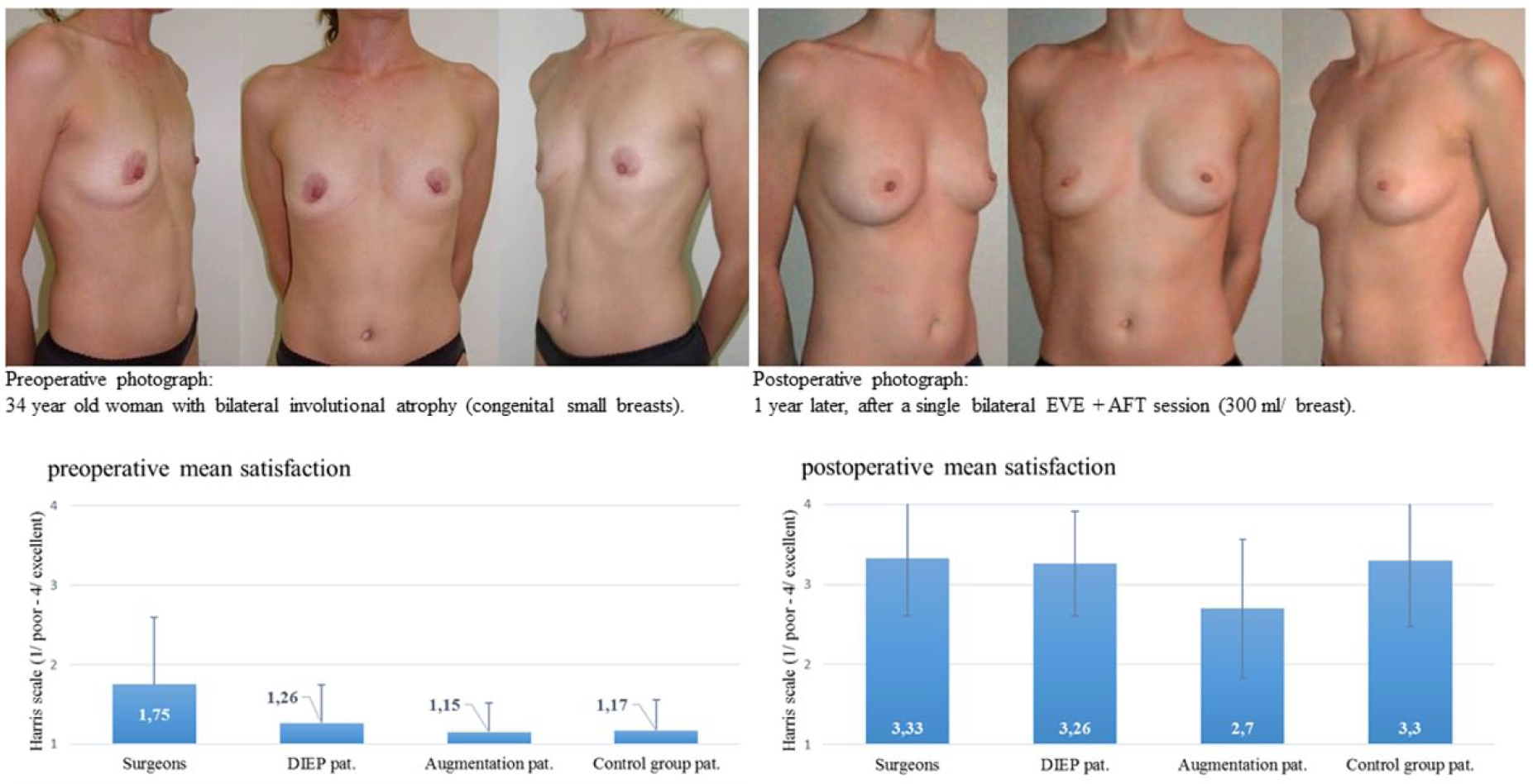
Pre- and postoperative appearance of EVE + AFT in total bilateral breast augmentation.
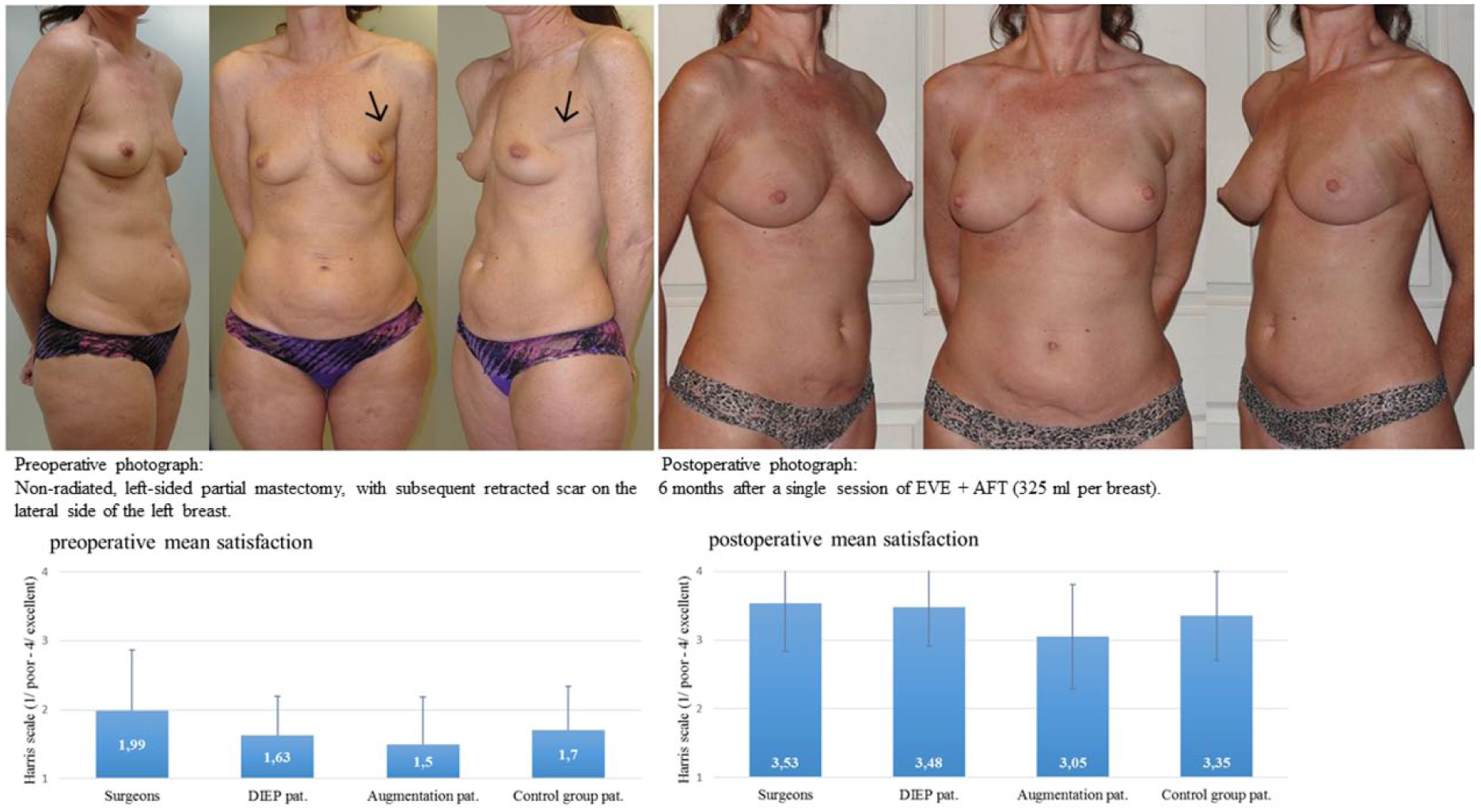
Pre- and postoperative appearance of EVE + AFT for local defect correction after lumpectomy.
Plastic surgeons from 10 European countries (The Netherlands, Belgium, Germany, Great Britain, France, Spain, Austria, Switzerland, Italy, and Greece) were contacted either directly through their national professional organization or indirectly by email with an invitation to score the pre- and postoperative photographs. A reminder was sent by email after 2 weeks. In addition to the physician rating, former patients (laymen) from 2 local hospitals (VieCuri Medical Center, Venlo/Zuyderland Medical Center, Sittard, Limburg, The Netherlands) were contacted according to the ethical guidelines from the Maastricht University Medical Center and asked for participation in this study. Three laymen study groups were contacted as follows.
Group 1: composed of female patients previously treated by deep inferior epigastric artery perforator (DIEAP) reconstruction in the period 2014 to 2016, with or without additional AFT.
Group 2: composed of female patients who underwent breast augmentation, somewhere in the period of 2014 up to April 2017.
Group 3: functioned as the control group and was composed of female patients not previously treated (either surgically or otherwise) for breast-related pathology.
Eligibility Criteria
Eligible laymen were defined as female patients, between the age of 18 and 70 years, without previous or current medical training and were included when able to understand the implications of the photographs or explanation of the AFT technique (as judged by the investigator). Emotionally unstable women—due to current or previous breast cancer–related mental trauma (as judged by the investigator)—in whom the photographs might aggravate anxiousness or negative emotions were excluded.
Patient Recruitment
Groups 1 and 2 were recruited in a retrospective matter. A recruitment letter was sent by the treating physician, in which the patient was informed of the study and subsequently asked if they may be contacted by phone for further information and possibly inclusion (checkbox yes or no option). Once approval was received the laymen was contacted by phone by the researcher (JG) and an understandable explanation about the content and methodology of the study was provided, at the end of which the laymen was asked for participation in this study. On accordance the laymen received the questionnaire including the photographs through an online (SurveyGizmo) link followed by an informed consent letter with retour envelop send through conventional mail. The photographs were supplemented with an explanatory text of the procedures leading up to the postoperative effect in understandable Dutch, and the laymen were asked to grade the difference according to the HS. Group 3 laymen were included in a prospective consecutive manner in which the initial (non breast related) consultation was concluded with the treating physician inquiring if the patient was willing to participate in a study. On agreement the patient was approached by the researcher (JG) in the same clinical setting and recruited in the same manner as the other groups with the only exception that patient information and informed consent letters were handed out and subsequently collected physically during the follow-up consultation (minimum of 2 weeks).
Statistical Analysis
Agreement between the evaluations of different groups of raters (surgeons, former DIEP/augmentation/control group patients) was calculated by the agreement index (κ) suggested by Vanbelle and Albert.17,18 A κ score equal or below 0 will be considered to indicate poor agreement; 0.01 to 0.20 slight agreement; 0.21 to 0.40 fair agreement; 0.41 to 0.60 moderate agreement; 0.61 to 0.80 substantial agreement; 0.81 to 0.99 almost perfect; and 1.00 perfect agreement. The sampling variance of κ was determined with the Jackknife method, as suggested by Vanbelle and Albert.17,18 The confidence interval for κ was derived from the sampling variance. After the agreement between different groups of raters, the agreement between surgeons from different countries was assessed in a similar way. In addition to analyzing the interrater agreement between groups on the pre- and postoperative photographs themselves, the authors wanted to examine the agreement on the increase (or possibly decrease) in cosmetic evaluation between the pre- and postoperative photographs, that is, the scoring trend. Therefore, the difference in the cosmetic evaluation between the pre- and postoperative photographs based on the Harris Score was calculated for every individual respondent per group. These differences were categorized as follows: (1) negative difference (ie, postoperative photograph scored lower than preoperative photograph), (2) postoperative HS = preoperative HS + 0, (3) postoperative HS = preoperative HS + 1, (4) postoperative HS = preoperative HS + 2, and (5) postoperative HS = preoperative HS + 3. Kappa was calculated for the agreement on the scoring trend between the surgeons and the laymen groups, and the laymen groups among each other, for all sets of photographs. The difference in scoring trend per set of pre/post photographs between the groups of raters was evaluated by ordinal regression analysis.
Results
A total of 312 plastic surgeons completed the questionnaires out of 520, and these were included for analysis. Despite the fact that surveys were distributed among (members of) European plastic surgery associations only, some of the respondents worked outside of Europe. Table 1 illustrates the distribution among countries, with most respondents practicing from the Netherlands (37.2%), France (18.9%), or Belgium (11.5%). The mean age of respondents was 45.9 years (SD = 10.6) with the majority being plastic surgeon (97.8%) followed by breast surgeons (1.6%) and other (0.6%, mostly German gynecologists). Eighty-two percent completed their medical specialty, with a quarter of the respondents having more than 20 years of practicing experience. When asked about familiarity with AFT, 91.3% disclosed having practiced AFT, either for general purposes (32.7%) or in addition to breast surgery (58.7%). Of the active practicing respondents, the majority performed AFT alone (73.7%), in <10 (28.4%) or between 10 and 30 (43.5%) procedures per year, and the vast majority considered himself or herself to be either experienced (48.1%) or moderately experienced (42.8%).
Participating Countries and Patients.
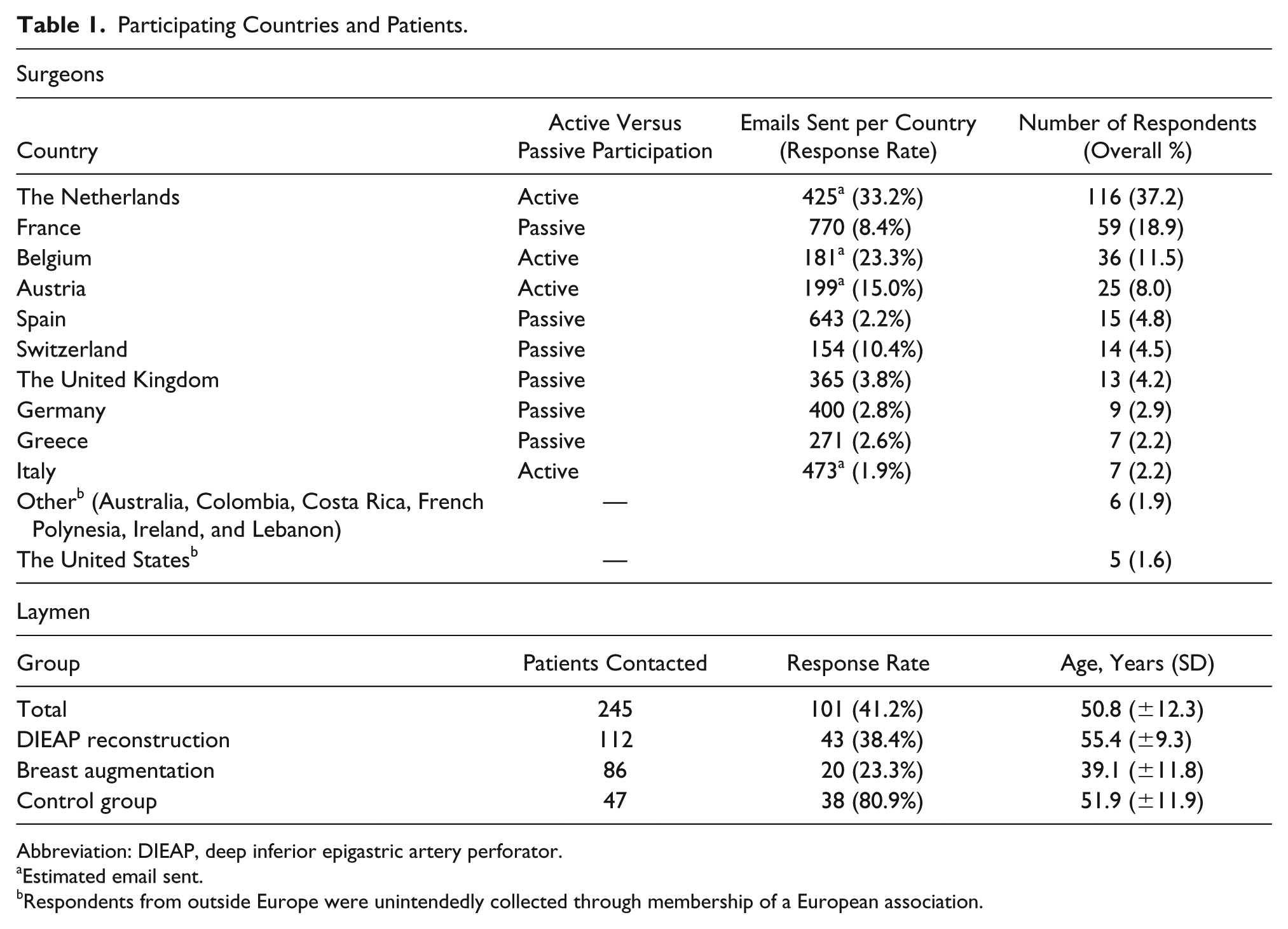
Abbreviation: DIEAP, deep inferior epigastric artery perforator.
Estimated email sent.
Respondents from outside Europe were unintendedly collected through membership of a European association.
Approximately 100 laymen, out of 245 (41.2%), responded and were included in the final analysis. Group 1 was composed of 43 former DIEAP patients, with Group 2 containing 20 patients after breast augmentation and Group 3 including 38 control patients. The response rate between groups ranged from 23.3% in Group 2 to 80.9% in Group 3. The mean age overall was 50.8 (SD = 12.3) years, with Group 1 (55.4/SD = 9.3) and Group 3 (51.9/SD = 11.9) respondents being significantly older than respondents from Group 2 (39.1/SD = 11.8), P < .001.
Interrater Agreement: Surgeons and Laymen
The interrater agreement between the total group of surgeons and the total group of laymen over all sets of photographs was considered moderate (0.45-0.55, depending on the set of photographs). The interrater agreement between the surgeons and respondents from Group 1 over all sets of photographs was substantial with a κ of 0.63 (95% confidence [CI] = 0.49-0.76), but a moderate agreement was found in the evaluation of the results of EVE + AFT for breast reconstruction (Figure 1 and Table 2). The interrater agreement between the surgeons and respondents from Groups 2 and 3 over all sets of photographs was considered fair and moderate, with κs of 0.36 (95% CI = 0.23-0.48) and 0.51 (95% CI = 0.38-0.63), respectively. In addition, a moderate agreement (κ = 0.45) was found between the surgeons and Group 2 respondents on the evaluation of EVE + AFT for local defect corrections (Figure 3 and Table 2) besides a fair interrater agreement (κ = 0.39) between the surgeons and Group 3 respondents on evaluating BRAVA + AFT in breast reconstruction (Figure 1 and ‘Table 2).
Interrater Agreements Scores Per Set of (Preoperative/Postoperative) Photographs Among Groups.
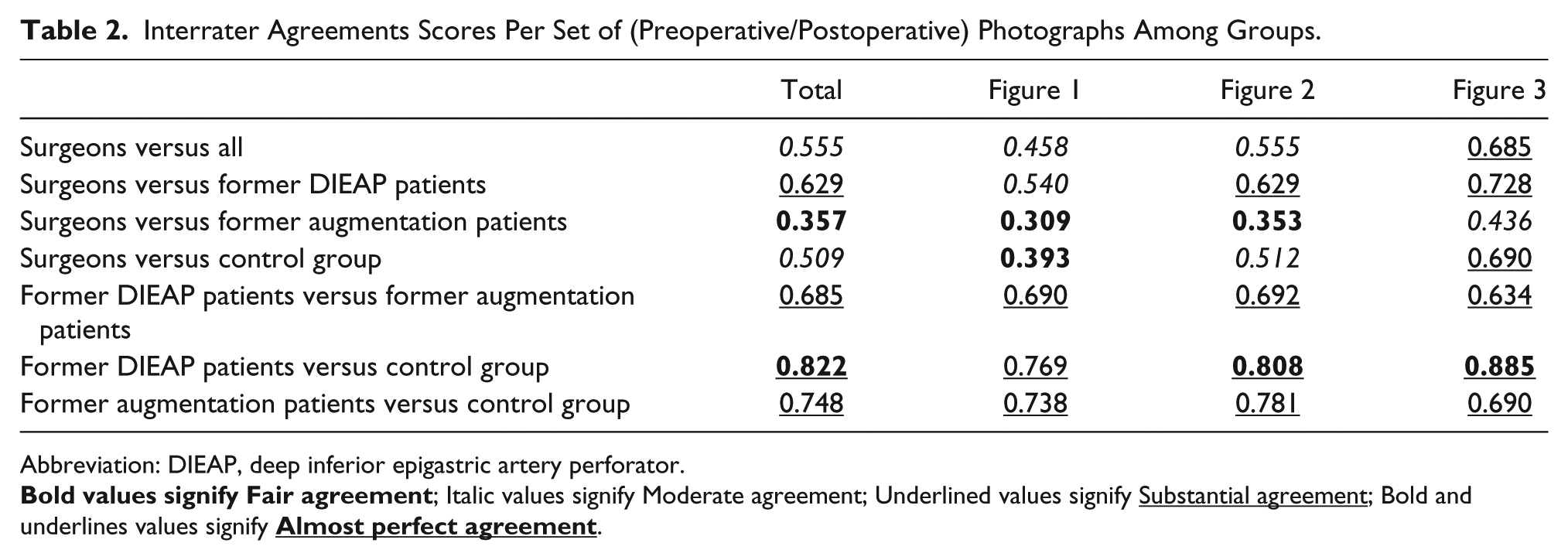
Abbreviation: DIEAP, deep inferior epigastric artery perforator.
Interrater Agreement: Between Laymen Groups
In comparing the different laymen groups, we found a substantial interrater agreement over all sets of photographs between the Groups 1 and 2 (κ = 0.69; 95% CI = 0.56-0.81) and Groups 2 and 3 (κ = 0.75; 95% CI = 0.61-0.89), respectively. Furthermore, an almost perfect interrater agreement was found between respondents from Groups 1 and 3, with a κ of 0.82 (95% CI = 0.74-0.90).
Scoring Trend: Difference Between Pre- and Postoperative Photograph
Only very low or negative interrater agreements between all groups (laymen-laymen and laymen-surgeons) were found when looking at scoring trends, that is, increase (or possibly decrease) in cosmetic evaluation between the pre- and postoperative photographs per set. Ordinal regression analysis shows that the laymen groups are generally more optimistic about the improvement than the surgeons, with significant differences between Group 1 and the surgeons (P = .042) for the first set of photographs (Figure 1), and between both Groups 1 and 3 compared with the surgeons (P = .003 and P = .004) for the second set of photographs (Figure 2).
Interrater Agreement: Surgeons per Country
The interrater agreement between surgeons from 4 different European countries over all sets of photographs ranged from substantial to almost perfect. A substantial interrater agreement was found in comparing the cosmetic evaluation of surgeons from the Netherlands with the evaluation of surgeons from France, Austria, and Belgium with κs of 0.73 (95% CI = 0.59-0.87), 0.79 (95% CI = 0.68-0.91), and 0.73 (95% CI = 0.62-0.85), respectively. Furthermore, a substantial interrater agreement (κ = 0.70; 95% CI = 0.57-0.82) was found between surgeons from Belgium and surgeons from Austria and an almost perfect score (κ = 0.81;95% CI = 0.65-0.96) was found between surgeons from France and surgeons from Belgium. Finally, the only moderate interrater agreement (κ = 0.60; 95% CI = 0.42-0.79) was found in comparing the cosmetic evaluation of surgeons from France and surgeons from Austria.
Discussion
The current innovative and popular characteristic of AFT makes it one of the fastest developing surgical techniques in plastic surgery. This trend is noticeable in various different aspects of AFT, such as the technique, its indications, and the way we try to increase its results through supplementation or external expansion (EVE). While most of these developments are not new, improvements in the way we measure its efficacy and patient satisfaction have only recently began to evolve. Up until 2011, most studies only superficially mentioned good patient/surgeon satisfaction with only a few using some sort of Likert-type scale. Since then, the value of patient-reported outcomes measurements (PROM) has gradually permeated in the world of AFT with several studies reporting patient satisfaction of AFT after breast reconstruction with either study-specific PROMs 19 or validated questionnaires like the Breast-Q.15,16,20 However, the Breast-Q, like other PROMs, primarily reports on patient satisfaction and comparisons between the cosmetic evaluation of AFT from patients and surgeons cannot be made. At the same time a quantitative objectification of the difference between what the doctor describes as “beautiful” and what a laymen’s perception thereof is, might actually prove very helpful in the consultation room when discussing expectations preoperatively.
The overall agreement between the surgeons and respondents from Groups 1 to 3 was substantial, fair, and moderate, respectively, over all sets of photographs. This indicates that overall, former DIEAP patients are more likely to share the same cosmetic appreciation as surgeons—when it comes to the use of EVE + AFT for various indications. However, Group 2 only showed a fair interrater agreement with the surgeons and patients seeking AFT breast augmentation might, therefore, benefit from a more extensive form of preoperative patient education, specifically highlighting the surgeons’ expectations of the postoperative effect. While the agreement between surgeons and laymen groups varied, laymen among each other, for the larger part, shared the same cosmetic evaluation on all EVE + AFT indications. In addition, we observed that surgeons from different European countries shared the same cosmetic values. This indicates that patient education, performed by a surgeon from a neighboring country, is not colored by differences in the cosmetic appreciations of the procedure inherited from the native country. The scoring trend only showed very low interrater agreements between groups. This indicates that while the interrater agreement between groups ranges from substantial to almost perfect per photograph, no such agreement could be found between groups, when looking at the increase of cosmetic appreciation. Fortunately, laymen tend to be more optimistic regarding the difference between the postoperative results compared with the preoperative appearance. This was especially true for former DIEAP patients compared with surgeons on the indication that mattered most for this group (Figure 1, breast reconstruction after mastectomy). This suggests that there is a chance that the patient is more satisfied with the end result than what would be expected based on the information provided by the surgeon preoperatively.
Limitations
This study is limited by its design. Most studies report the satisfaction of patients with their own breasts, and this satisfaction might significantly differ from the appreciation of cosmetic results of a procedure based on photographs from another woman. Furthermore, all photographs illustrate the postoperative effect of EVE + AFT, which is generally better than solitary AFT and are therefore not reproducible for the latter. Finally, patients from Groups 1 and 2 were studied postoperatively and their cosmetic evaluation of the photographs might have differed when studied preoperatively.
Conclusion
This study illustrates, for the first time, the interrater agreement and scoring trends between European plastic surgeons and different laymen groups in the cosmetic evaluation of EVE + AFT for various indications in breast surgery. The most quantitative similarities were found between surgeons and former DIEAP patients. However, former DIEAP patients are generally more appreciative of the cosmetic results of EVE + AFT for breast reconstruction after total mastectomy and patients seeking breast augmentation tend to agree the least with surgeons. Further studies should focus on the qualitative nature of the differences between surgeons and both laymen and patient appreciation with this technique in order for us to increase the quality of patient-surgeon communications. In the meantime, it might be beneficial for surgeons to elaborate more on expectations when educating the patient seeking EVE + AFT for breast augmentation purposes.
Footnotes
Author Contributions
Study concept and design: Jan-Willem Groen, Andrzej A. Piatkowski, John H. Sawor
Acquisition of data: Jan-Willem Groen, Andrzej A. Piatkowski, Roger K. Khouri, Rene R. J. W. van der Hulst
Analysis and interpretation: Janneke A. Wilschut, Marco J. P. F. Ritt, Jan-Willem Groen
Study supervision: Roger K. Khouri, Rene R. J. W. van der Hulst, Marco J. P. F. Ritt
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Medical Ethics Committee of Maastricht University Medical Center (METC-16-4-167.1/ab).