
Abstract
Background. Questions remain about the therapeutic durability of transoral incisionless fundoplication (TIF). In this study, clinical outcomes were evaluated at 5 years post-TIF 2.0. Methods. A total of 63 chronic gastroesophageal reflux disease (GERD) sufferers with troublesome symptoms refractory to proton pump inhibitor (PPI) therapy, absent or ≤2 cm hiatal hernia, and abnormal esophageal acid exposure were randomized to the TIF group or PPI group. Following the 6-month evaluation, all patients in the PPI group elected for crossover to TIF; therefore, all 63 patients underwent TIF 2.0 with EsophyX2 device. Primary outcome was elimination of daily troublesome regurgitation and atypical symptoms at the 5-year follow-up. Secondary outcomes were improvement in symptom scores, PPI use, reoperations, and patient health satisfaction. The cost-effectiveness of TIF 2.0 was also estimated. Results. Of 63 patients, 60 were available at 1 year, 52 at 3 years, and 44 at 5 years for evaluation. Troublesome regurgitation was eliminated in 88% of patients at 1 year, 90% at 3 years, and 86% at 5 years. Resolution of troublesome atypical symptoms was achieved in 82% of patients at 1 year, 88% at 3 years, and 80% at 5 years. No serious adverse events occurred. There were 3 reoperations by the end of the 5-year follow-up. At the 5-year follow-up, 34% of patients were on daily PPI therapy as compared with 100% of patients at screening. The total GERD Health-related quality-of-life score improved by decreasing from 22.2 to 6.8 at 5 years (P < .001). Conclusion. In this patient population, the TIF 2.0 procedure provided safe and sustained long-term elimination of troublesome GERD symptoms.
Keywords
Introduction
Following major changes in technique since the early iterations of endoluminal fundoplication (ELF) and transoral incisionless fundoplication (TIF) 1.0 (gastrogastric fundoplication), the TIF 2.0 procedure (esophagogastric fundoplication) performed with the EsophyX2 device (EndoGastric Solutions, Redmond, WA) has emerged as a safe and effective therapy for chronic gastroesophageal reflux disease (GERD) in patients with minimal anatomical deterioration of the gastroesophageal junction and the diaphragmatic hiatus. Other studies have documented the lack of serious adverse events (SAEs) and demonstrated the ability of TIF 2.0 to eliminate GERD symptoms, heal reflux esophagitis, normalize or reduce pathological distal esophageal acid exposure, and reduce proton pump inhibitor (PPI) use in a subset of chronic GERD patients.1-5 Despite these successes, the durability of these outcomes remained in question.
The TIF 2.0 EsophyX vs Medical PPI Open label (TEMPO) trial is a multicenter, controlled, randomized study with 3 prior publications.3-5 In these reports, the superiority of the TIF 2.0 procedure compared with high-dose PPIs in a select group of chronic GERD sufferers with small or absent hiatal hernias was established. The safety of the procedure, a very low incidence of associated postfundoplication side effects, and sustained positive outcomes up to 3 years post-TIF 2.0 have been reported.3-5
The outstanding feature for the cohort of patients included in this study is that they represented ideal surgical candidates for an antireflux procedure because of their longstanding documented reflux, incomplete response to optimized medical therapy, and willingness to seek a surgical cure. Analysis of the 5-year follow-up data offers the opportunity to assess the durability of symptomatic control, quality-of-life outcomes, reoperation rates post-TIF, PPI use, and patient satisfaction. This is the first study to assess long-term clinical outcomes beyond 3 years in patients in the United States. The authors expected that the determination of reoperation rates 5 years post-TIF could offer preliminary cost comparisons for the TIF procedure versus the more traditional laparoscopic Nissen fundoplication (LNF). Finally, we hoped to use the results of this long-term follow-up to propose a role for the TIF procedure in the antireflux armamentarium for select patients.
Methods
Study Design
This was a randomized, multicenter, open-label study, with a crossover arm, carried out at 7 community-based practices in the United States. The study design has been described in detail previously.3-5 Briefly, eligible patients were randomly assigned to receive either TIF 2.0 or maximum dose PPI therapy with a target allocation ratio of 2:1. After their 6-month evaluation, all patients in the PPI arm elected to undergo the TIF 2.0 procedure. Therefore, for the purpose of this report, each patient served as his or her own control as compared with the baseline assessment. The institutional review board of the participating institutions approved the extension of the study, and written consent was obtained from all participants prior to the 5-year follow-up. The study was prospectively registered and updated to reflect the study extension with the clinicaltrials.com (NCT01647958). The authors had access to the study data, and the coauthors reviewed and approved the final manuscript.
Study Patients
All included patients were chronic GERD sufferers with daily troublesome regurgitation and/or atypical symptoms refractory to PPI therapy, pathological esophageal acid exposure confirmed by 48-hour pH monitoring off PPI therapy (percentage time pH <4 greater than 5.3%), and history of PPI use for at least 6 months. 3 Patients with hiatal hernia >2 cm, Hill grade III or IV, esophagitis of grade C or D (Los Angeles classification), and Barrett’s esophagus >2 cm were excluded from randomization. Furthermore, patients with class 2 or 3 obesity (body mass index [BMI] > 35 kg/m2), esophageal motility disorders, and previous gastric or esophageal surgery were also excluded.
Study Procedures
Prerandomization patient characteristics, baseline assessments, TIF procedure data, and follow-up evaluations up to 3 years postprocedure have been previously reported.3-5 This included symptomatic assessment with validated disease-specific questionnaires on and/or off PPI therapy as well as esophagogastroduodenoscopy and 48-hour pH-metry off PPIs at prespecified time intervals. 5 All patients in this study underwent the standard TIF 2.0 procedure using the EsophyX2 device under general endotracheal anesthesia. 5 The TIF 2.0 procedure created a full-thickness, partial gastroesophageal fundoplication secured above the Z-line with polypropylene “H” fasteners that were delivered through the thickness of the apposed stomach and esophageal walls.
The length and circumference of newly built TIF 2.0 gastroesophageal valves was determined by performing an immediate postprocedure endoscopy and using well-described standardized methods. The valve length is measured as the distance in centimeters from the apex of the fundus to the valve lip, as measured at the incisors in endoscopic retroflexion. 6 The valve circumference is defined as the distance in degrees between the 2 most distant fasteners used to secure the fundoplication. 7 The count of contributing fasteners was conducted during the immediate postprocedure endoscopy.
Assessments and Follow-up
The TEMPO trial was initially designed to follow enrolled patients for up to 3 years after TIF. After completion of the 3-year follow-up, all investigators agreed to continue following the patients for an additional 2 years. Data were collected on elimination of troublesome symptoms, PPI use, reoperation, adverse events, and patient satisfaction.
Troublesome symptoms were defined according to the Montreal consensus definition as mild symptoms occurring 2 or more days a week, or moderate to severe symptoms occurring more than 1 day a week. 8 In the TEMPO trial, the Reflux Disease Questionnaire (RDQ) was used to assess elimination of troublesome regurgitation.3-5 RDQ is a 12-item questionnaire that was designed to assess the frequency and severity of heartburn (4 items measuring the frequency and severity of pain and burning behind the breastbone), regurgitation (4 items measuring the frequency and severity of acid taste in the mouth and movement of the material upward from the stomach), and dyspeptic complaints (4 items measuring the frequency and severity of pain or burning in the upper stomach). 9 Response options range from 0 (not present) to 5 (daily) for frequency and 0 (not present) to 5 (severe) for severity. Each patient’s score is calculated as the mean of item responses, with higher scores indicating more frequent and/or severe symptoms.
The Reflux Symptom Index (RSI) questionnaire was used to assess elimination of atypical symptoms. RSI is a 9-item validated questionnaire used to measure atypical GERD symptoms such as hoarseness, throat clearing, excess throat mucus, dysphagia, and cough. 10 The scale for each individual item ranges from 0 (no problem) to 5 (severe problem), with a maximum total score of 45 and a normality threshold of ≤13.
GERD Health-Related Quality of Life (GERD-HRQL) was used to evaluate typical GERD symptoms, quality of life, and patient satisfaction with their current health condition. A higher total GERD-HRQL score (range from 0 to 50) indicates more severe GERD. 11
PPI use was self-reported by patients as complete cessation, occasional use (<3 d/wk), or daily use. Individual investigators reported adverse events and reoperation rates. Patient satisfaction with their current health condition was reported as part of the GERD-HRQL, with 3 possible answers: satisfied, neutral, or dissatisfied.
For the purpose of cost analysis, the Optum healthcare database (data from 2011 to 2013) was used to determine cost and resource utilization for TIF and LNF up to a 2-year follow-up. Standardized costs were computed for inpatient and outpatient visits and medical therapy.
Primary End Points
Primary end points were elimination of troublesome regurgitation and elimination of all troublesome atypical symptoms at the 5-year follow-up as evaluated by the RDQ and RSI, respectively.
Secondary End Points
Secondary end points were improvement in symptom scores (RDQ, RSI, GERD-HRQL), PPI use, reoperations, and satisfaction with current health condition. We also compared the cost-effectiveness of TIF versus LNF based on data obtained from the Optum group.
Data Collection and Statistical Analyses
An independent clinical research organization collected the patient-reported outcomes and entered the data points into the password-protected electronic database. Postoperative data at 1-, 3-, and 5-year intervals were compared with preoperative data using the repeated-measures analysis of variance (ANOVA) followed by the post hoc Tukey-Kramer honestly significant difference multiple comparison procedure. In general, continuous variables were reported as means (SDs); categorical variables were reported as percentage, counts, and 95% CIs and were tested for significant difference using McNemar’s test. All 3 TIF failures (patients who underwent a revisional procedure) were included in the analyses and were assigned the worst outcomes observed during the study from the timing of revisional surgery going forward. The statistical significance was prespecified by a P value of <.05.
Results
A total of 196 patients with chronic GERD were assessed for study eligibility between June and August 2012. Of these 196, 32% (63) met the study inclusion/exclusion criteria and were randomized (40 patients into the TIF group and 23 patients into the PPI group). 3 The most commonly cited cause for ineligibility was the absence of pathological distal esophageal acid exposure (Figure 1). Of the randomized patients, 70% (44/63) completed the 5-year follow- up assessments.
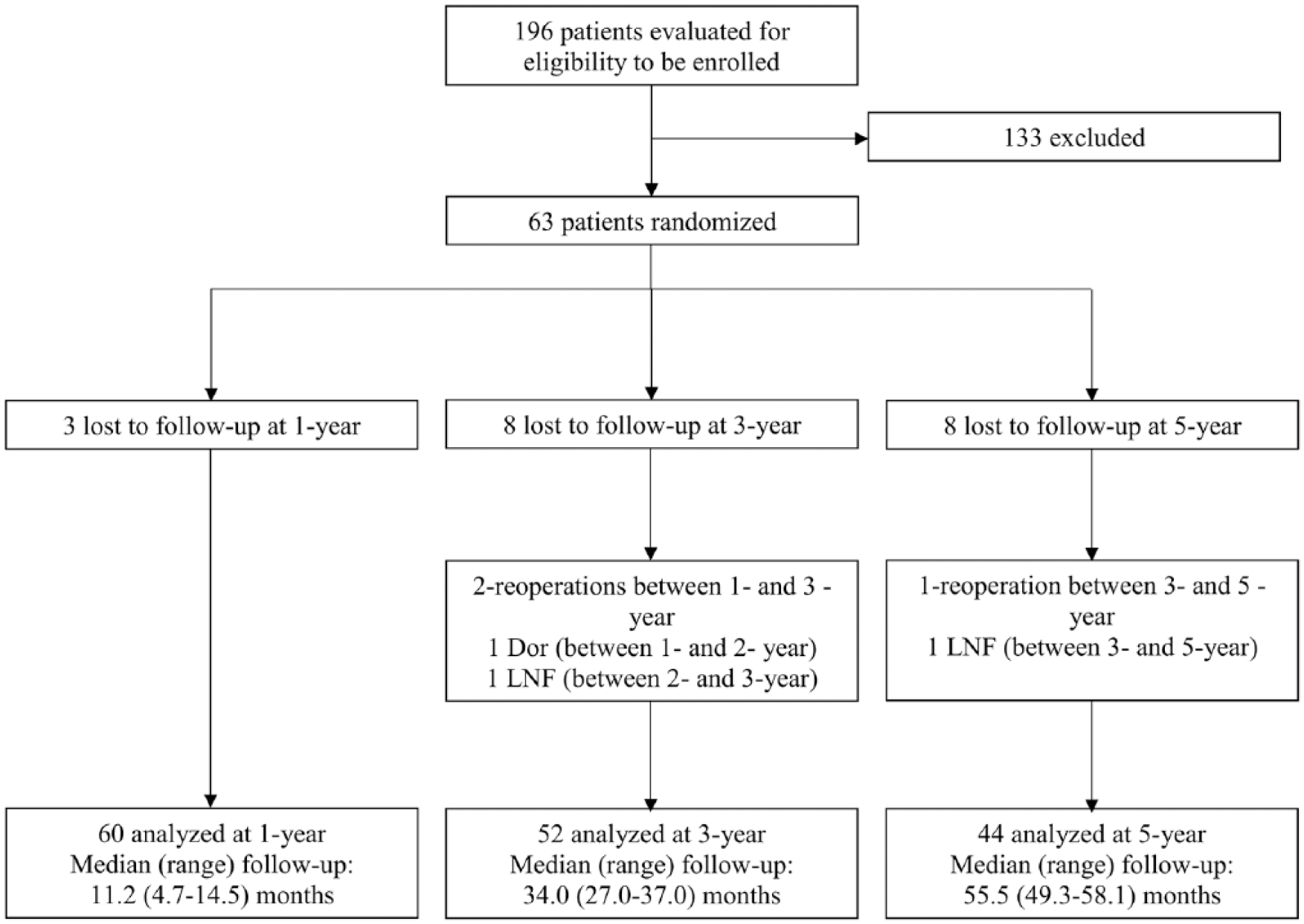
Study flowchart of treated and analyzed patients. Of the 85 patients not meeting eligibility criteria, 45% (38/85) had normal pH test, 36% (31/85) had hiatal hernia >2 cm in axial length or greatest transverse dimension, 13% had Hill grade >II, 2% had reflux esophagitis grade C or D (Los Angeles classification), 2% had body mass index >35 kg/m2, and 1% (1/85) had Barrett’s esophagus >2 cm. 5 Additionally, 32 patients declined to participate, and 16 were excluded for other reasons. 3
Patient Demographics and Baseline Characteristics
The study population (n = 60) was 55% female (33) and 45% male (27%). The average age at the time of enrollment was 51.5 ± 10.3 years. The largest age segment was the 50- to 65-year-old segment (52%, 31). Of the remaining patients, 40% (24) were younger than 50 years, and only 8% (5) were older than 65 years. The average BMI was 28.5 ± 3.7 kg/m2. GERD symptom duration was 11.2 ± 9.8 years; PPI therapy duration was 8.6 ± 6.5 years. Only 2% (1) of patients had the short-segment variant of Barrett’s esophagus.
Safety and Procedure Data
No SAEs reported or any other complication associated with the TIF 2.0 procedure occurred in this study.3-5 As assessed by immediate postprocedure endoscopy, TIF 2.0 created valves with an average length of 2.8 ± 0.5 cm and a circumference of 290° ± 20°. On average, 21 ± 4 fasteners were used to secure the newly created valves.
Two revisional interventions were previously reported (1 Dor fundoplication in the second year and 1 LNF in the third year). 5 Since that last report, 1 additional patient underwent a reoperation (LNF). Therefore, the reoperation rate for this cohort was 5% (3/60). All surgical revisions were performed on patients with recurrent daily troublesome GERD symptoms that persisted on PPI therapy. Endoscopic findings for the 3 patients undergoing revisional surgery included recurrent hiatal hernia and varying degrees of disruption of the TIF 2.0 valve. Before revisional procedures, all patients had abnormal distal esophageal acid exposure. At baseline, in addition to daily troublesome regurgitation and/or atypical symptoms, all 3 patients suffered from daily troublesome heartburn on twice-daily PPI therapy. Severity of GERD in these patients was further confirmed by percentage total time of pH <4 before the TIF 2.0 procedure (7.5, 16.8, and 19.5).
Primary Clinical End Point
Of 44 patients who underwent the 5-year follow-up, 98% (43) suffered from troublesome regurgitation on PPI therapy at screening. At the 5-year follow-up, elimination of troublesome regurgitation was achieved in 86% of patients (37/43, 95% CI = 72%-94%). Similar findings were observed at the 1- and 3-year follow-ups (Figure 2). Elimination of troublesome atypical symptoms occurred in 80% of patients at 5 years (31/39, 95% CI = 64%-89%), 88% at 3 years (42/48, 95% CI = 75%-95%), and 82% at 1 year (45/55, 95% CI = 70%-90%). No statistically significant differences in elimination of troublesome regurgitation or atypical symptoms were found between assessments at years 1, 3, and 5. Results are reported regardless of PPI use at the time of assessment (on or off PPI therapy).
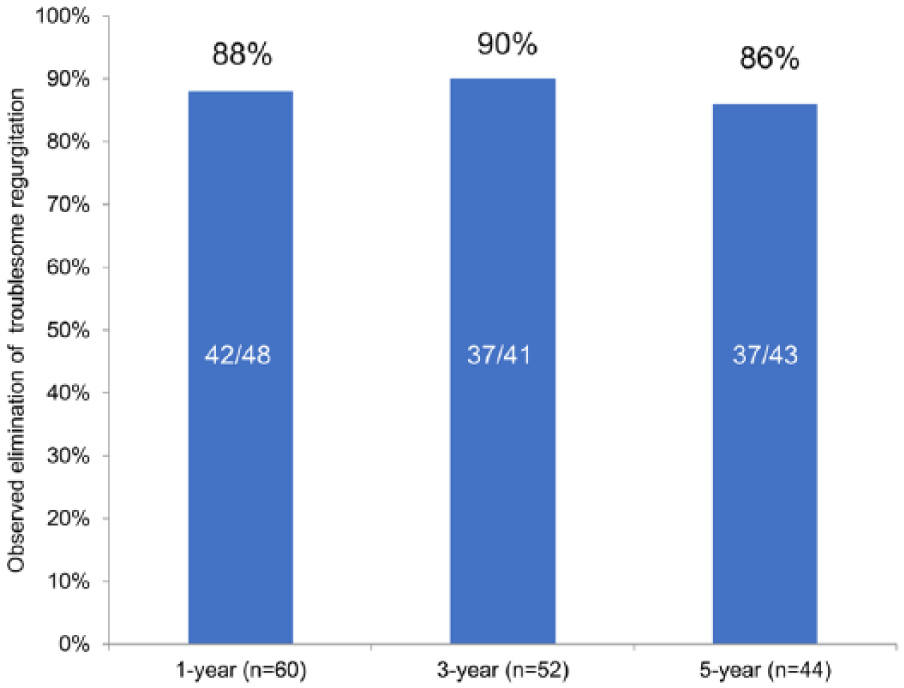
Elimination of troublesome regurgitation, as assessed by the Reflux Disease Questionnaire at the 1-, 3-, and 5-year follow-ups.
Secondary End Points
The total regurgitation score (assessed by RDQ) improved significantly by falling from 3.0 on PPIs at screening to 0.7 at the 5-year follow-up (P < .001). There was no statistically significant difference between the total regurgitation scores at the 1-, 3-, and 5-year follow-up (Figure 3). The total RDQ score improved significantly by decreasing from 3.0 at screening to 0.8 at the 1-year, 0.6 at the 3-year, and 0.7 at the 5-year follow-up (P <.001 in all cases vs screening).
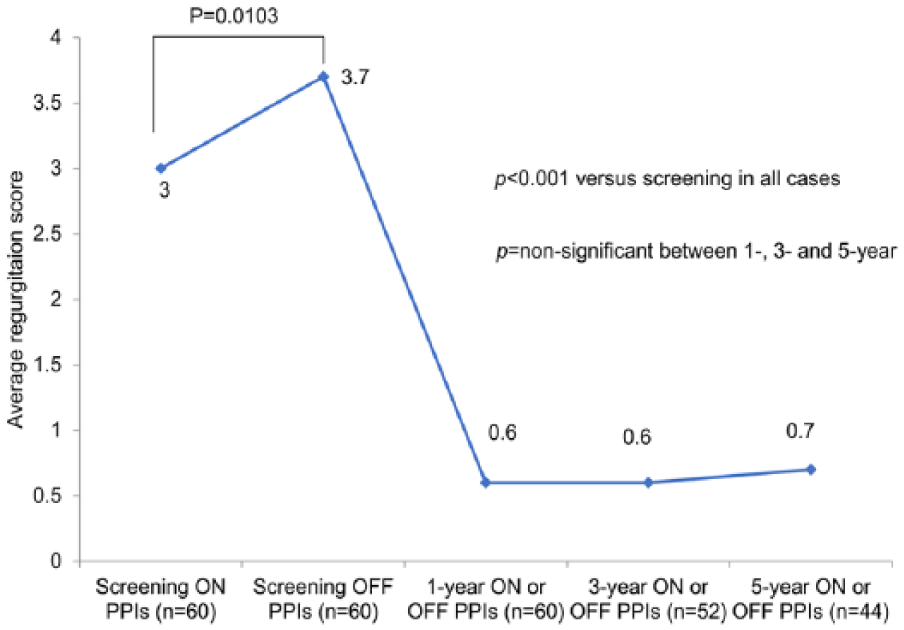
Regurgitation score, as assessed by the Reflux Disease Questionnaire, at screening and the 1-, 3-, and 5-year follow-ups.
The total RSI score improved by decreasing from 22.2 at screening to 6.3 at the 5-year follow-up (P < .001). There was no statistically significant difference between the total RSI scores at 1-, 3-, and 5-year assessments (Figure 4). The improvement in total GERD-HRQL score was stable between the 1-, 3-, and 5-year follow-up assessments (Figure 5).
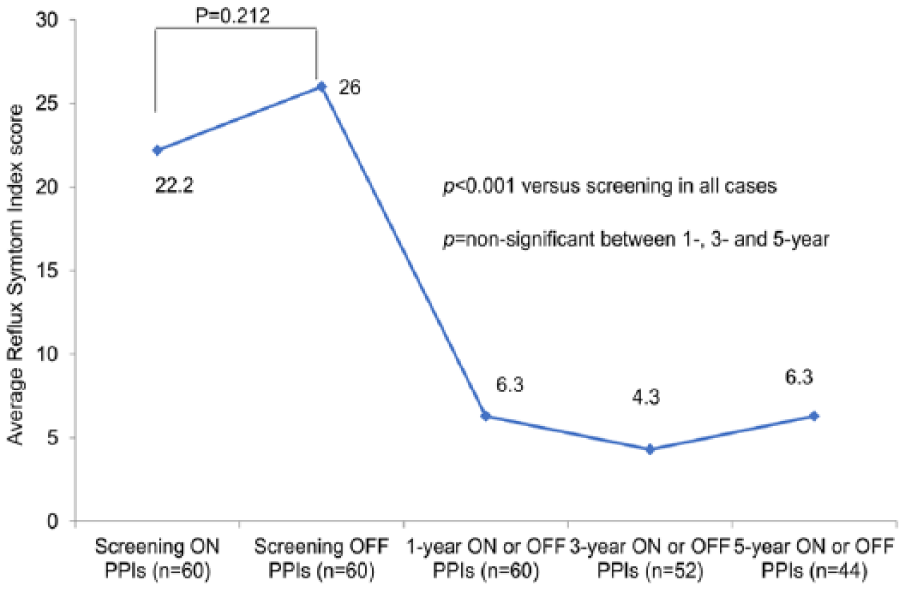
Reflux Index Score at screening and 1-, 3-, and 5-year follow-up assessments.
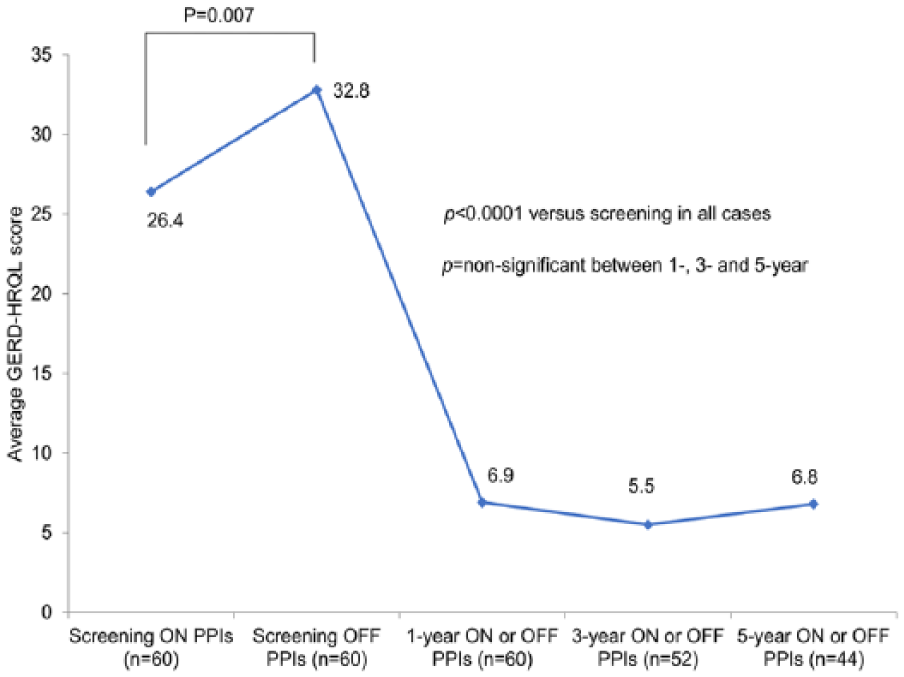
Gastroesophageal Reflux Disease Health-Related Quality of Life (GERD-HRQL) questionnaire, at screening and 1-, 3-, and 5-year follow-up assessments.
All patients were on daily PPI therapy at screening. At the 5-year follow-up, 34% (15/44, 95% CI = 22%-49%) of patients were on daily PPI therapy. An additional 20% (9/44, 95% CI = 11%-35%) of patients were taking PPI medication occasionally. Therefore, complete cessation of PPI therapy was achieved in 46% (20/44, 94% CI = 32%-60%) of patients who completed the 5-year follow-up (Figure 6).
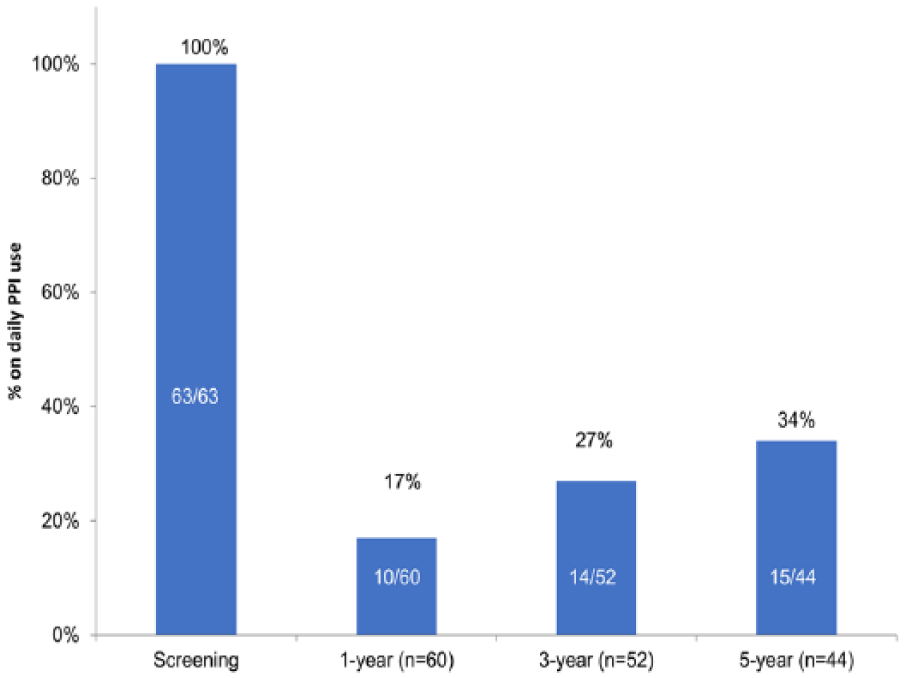
Percentage of patients on daily proton-pump inhibitor (PPI) therapy at screening and 1-, 3-, and 5-year follow-up assessments.
Patient satisfaction with current health condition, as assessed by GERD-HRQL, before treatment was 2% (1/60, 95% CI = 0%-10%) and improved to 75% (45/60, 95% CI = 63% -84%) at 1 year, to 83% (43/52, 95% CI = 70%-91%) at the 3-year follow-up, and to 70% (31/44, 95% CI = 56%-82%) at 5 years (P <.001 vs screening in all cases).
At 3 years post-TIF, all esophageal pH parameters, with the exception of duration of longest reflux, improved significantly as compared to baseline, with 40% (16/40) of patients achieving pH normalization. 5 Of the 24 patients with elevated levels of distal esophageal acid exposure at 3 years (defined as percentage total time of pH <4 greater than 5.3%, as measured by 48-hour pH testing), 22% (5/24) were not available for the 5-year follow-up. Of the remaining 19 patients, 63% (12/19, 95% CI = 41%-81%) reported complete cessation of PPI therapy at 5 years; 16% (3/19, 95% CI = 5%-38%) reported taking PPIs occasionally, and 21% (4/19, 95% CI = 8%-44%) reported taking PPIs daily.
Cost Analysis
In the Optum database, 2734 LNF patients and 73 TIF patients were available for the cost analysis. The average total cost over 2 years per LNF patient was $99 256, as compared with $71 691 per individual TIF patient (Table 1). The total average health care utilization for LNF and TIF is shown in Figure 7.
Average Cost, With Breakdown by Category, Associated With TIF 2.0 and LNF, as Accrued Over a 2-Year Follow-up Period (Data Obtained From the Optum Database).
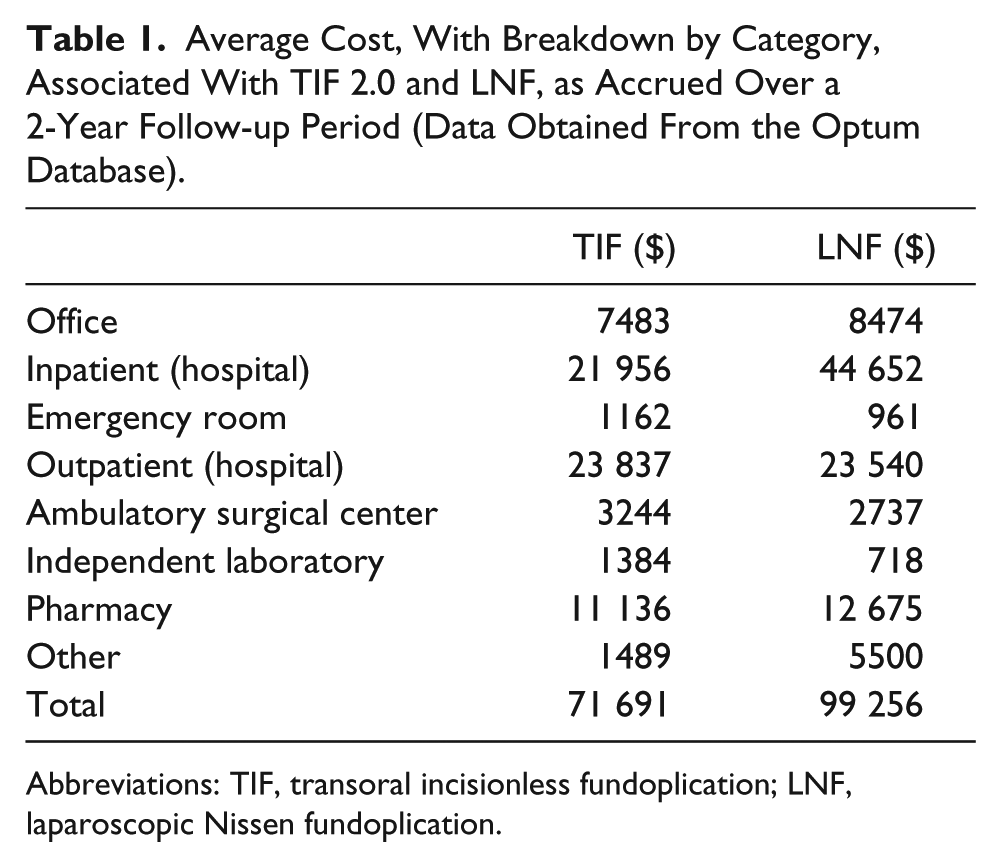
Abbreviations: TIF, transoral incisionless fundoplication; LNF, laparoscopic Nissen fundoplication.
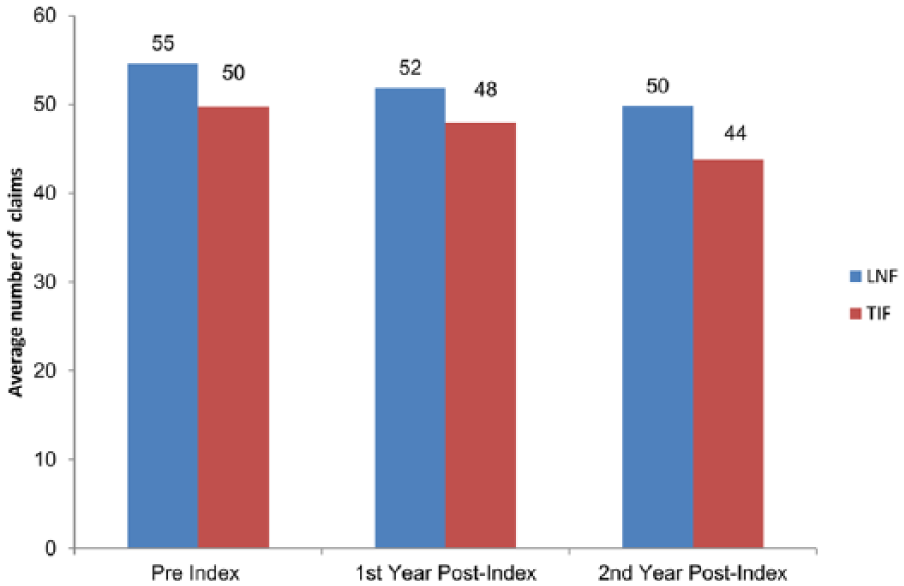
The Optum database average utilization of health care resources (number of claims) for laparoscopic Nissen fundoplication (LNF) and transoral incisionless fundoplication (TIF) over 2 years.
In the subgroup of patients with resource utilization in the top quartile (ie, most refractory PPI patients), the average cost of care (preindex, first and second year postprocedure) summed over a 2-year period for a LNF patient was $124 000, as compared with $66 000 for a TIF patient.
Discussion
The TEMPO trial is the first trial to assess the long-term outcomes (5-year follow-up) of the TIF 2.0 procedure in a US patient population. Patients suffering from troublesome regurgitation and atypical symptoms despite optimized acid-reducing therapy represent a common clinical challenge. This validated the crossover randomized design of this trial, allowing patients in the PPI arm to undergo TIF 2.0 after their 6-month follow-up. Of note, all of them chose this option, recognizing that the TIF 2.0 procedure may offer a valuable alternative.
The major contribution of this report is that it offers conclusive evidence that the early benefits reported with the TIF 2.0 procedure in previous shorter-term prospective multicenter randomized reports3-5 and prospective multicenter observational studies12-14 are sustained at the 5-year follow-up. This is a milestone that has not been achieved by previous GERD endoluminal therapies (eg, EndoCinch, Enteryx, Gatekeeper, NDO Plicator, ELF, and TIF 1.0), which, with the exception of the Stretta procedure, are no longer available because of safety concerns and/or lack of effectiveness. The quality and durability of the long-term symptomatic outcomes achieved in this study set apart the TIF 2.0 procedure from these earlier GERD treatment modalities. These results were achieved without unwanted SAE and postfundoplication side effects. 5 Importantly, the elimination of regurgitation, atypical symptoms, and heartburn, as evaluated by validated, disease-specific questionnaires (RDQ, RSI, GERD-HRQL), was maintained without significant deterioration over time. Therefore, this study establishes the ability of the TIF 2.0 procedure to provide long-term and durable resolution of troublesome GERD symptoms, improvement of quality of life, and reduction in PPI utilization in well-selected chronic GERD patients.
Our study design included patients who were selected to demonstrate that the TIF 2.0 procedure would be beneficial for a subset of chronic GERD patients who failed maximal medical therapy (hiatal hernia ≤2 cm, esophagitis Los Angeles grade A or B, Hill grade valve I or II). These patients had been experiencing intractable symptoms and sought a minimally invasive surgical cure without side effects. The TIF 2.0 procedure has repeatedly proven to avoid postfundoplication symptoms such as gas bloat, flatulence, dysphagia, and diarrhea. 5 The authors reiterate that comparable results can only be achieved by expert endoscopists with appropriate training in the standardized TIF 2.0 technique and by adhering to stringent selection criteria similar to what was used in this study.
The reoperation rate in this report was determined to be 5% (3/60) after 5 years, which is comparable to the published rates of reoperation after LNF (3%-6%).15,16 In our study, 3 patients underwent Laparoscopic Nissen (2) and Dor (1) fundoplication post-TIF without difficulty, as was previously suggested by others. 17 In contrast, studies with earlier iterations of the device and techniques no longer used (ELF and TIF 1.0) reported higher rate of reoperations (11%-52%).18-20 Additionally, the higher reported reoperation rates from the European studies can be attributed to patient selection because patients with large hiatal hernias (>2 cm), Hill grade valves III and IV, and esophagitis C or D were often enrolled.
Limitations of the study include the relatively small number of patients, which can be partially explained by the challenges involved in enrolling patients with such highly selective criteria. The study was, however, appropriately powered for statistical significance and had a respectable follow-up rate of 70% at 5-year assessment. We could also be criticized for not performing functional tests and endoscopies at the 5-year mark, though they were performed and reported in the 3-year follow-up. 5 We note that a poor correlation between postintervention GERD symptoms and physiological parameters has consistently been reported with all therapies, including traditional antireflux surgery,21,22 the TIF procedure,5,23 and during PPI therapy (17% to 80% of patients demonstrated abnormal esophageal acid exposure while being asymptomatic on PPI therapy).3,24-27 An additional potential limitation of this study is that the results are reported regardless of PPI use at the time of postprocedure assessment (on or off PPI therapy). We felt justified to use this methodology because all patients in the study experienced daily troublesome regurgitation and/or atypical symptoms on optimized PPI therapy before the TIF 2.0 procedure. Achieving control of troublesome symptoms and improving quality of life with the use of PPIs after an endoscopic antireflux procedure in patients whose symptoms were refractory to high-dose PPIs before intervention should not necessarily be considered a treatment failure. 4 In these cases, the TIF procedure may be viewed as a useful therapeutic adjunct to PPIs.
Although every patient enrolled in the TEMPO trial experienced intractable GERD symptoms despite daily PPIs (per inclusion criteria), more than two-thirds of patients remained off daily PPIs 5 years after undergoing the TIF procedure. Others have suggested that return to PPI utilization is a poor indicator of recurrent GERD. 28 In our study, patients who were still on occasional or daily PPIs had benefited from improved symptomatic control after TIF 2.0, with 95% of patients enrolled not having sought corrective surgery after 5 years.
The TIF 2.0 procedure appears to be cost-effective. Medicare data suggest that the average reimbursement for a TIF procedure ($4, 510.81) is about half the rate for a LNF ($8, 573.99). A simulation applying these reimbursement rates to the 60 TEMPO patients (who were candidates for either procedure) reveals a potential procedure-related savings of $238 543.40 for performing TIF 2.0 instead of LNF. Considering that the preprocedure evaluation is the same for the TIF candidates and the LNF candidates, and that the reoperation rate established in this study for TIF is similar to that of LNF, we believe that TIF may be a cost-effective alternative to LNF. In the top quartile of medical resource utilization, such as in GERD patient populations with similar characteristics as our TEMPO patients, the potential savings may be even more significant. Indeed, in that subgroup, the approximate total accrued cost reached $124 000 for a single LNF patient versus $66 000 for TIF for the first 2 years postprocedure. Out of the 63 patients enrolled in this study and who underwent the TIF procedure, 5% had corrective surgery within 5 years, leaving 95% of patients who underwent a less-invasive procedure, with virtually no side effects and at a significant overall cost savings compared with more invasive GERD surgery.
Based on these results and the authors’ personal experience, and in an attempt to define the role of TIF in the antireflux armamentarium, we suggest that in the appropriate patient population, the TIF 2.0 procedure could be considered the definitive alternative therapy to PPIs in a majority of patients undergoing the procedure. Indeed, our study shows that at 5 years, a majority of patients had enjoyed the combined benefits of not having undergone any kind of additional corrective surgery, not being back on daily dose of PPIs, experiencing complete resolution of their troublesome symptoms, and being satisfied. In a minority of patients, it appears that TIF 2.0 represented a useful adjunct therapy to be used in conjunction with various regimens of acid-reducing therapy. In this subgroup of patients, our study shows that the TIF procedure helped eliminate or improve difficult-to-control symptoms such as regurgitation and atypical symptoms that had been intractable and refractory to PPIs prior to the procedure. Finally, in a very small group of patients, estimated at approximately 5% after 5 years, the procedure would have represented a noninvasive first-line therapy without “burning any bridges” or compromising the ability to perform additional surgery such as a LNF. 15
Conclusions
Five years after undergoing TIF 2.0, the great majority of TEMPO trial patients experienced durable elimination of all types of troublesome GERD manifestations, including regurgitation and atypical symptoms. There were no SAEs or any safety concerns associated with the TIF 2.0 procedure. It also appears that in the appropriate patient population, the TIF 2.0 procedure could be a cost-effective alternative to LNF.
Footnotes
Author Contributions
Study concept and design: Karim S. Trad
Acquisition of data: Karim S. Trad, William E. Barnes, Elizabeth R. Prevou, Gilbert Simoni, Jennifer A. Steffen, Ahmad B. Shughoury, Mamoon Raza, Jeffrey A. Heise, Mark A. Fox, Peter G. Mavrelis
Analysis and interpretation: Karim S. Trad, Elizabeth R. Prevou
Study supervision: Karim S. Trad
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KST, MR, and GS have received speaking honoraria from EndoGastric Solutions. WEB, ABS, PGM, JAH, and MAF have no conflicts of interest or financial ties to disclose. ERP and JAS have no conflicts of interest or financial ties to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The TEMPO study was supported by EndoGastric Solutions, Inc, Redmond, Washington.