
Abstract
Background. Laparoscopic splenectomy and azygoportal disconnection (LSD) using many different surgical techniques has become increasingly popular for treatment of cirrhotic patients with bleeding portal hypertension and secondary hypersplenism. Surgical procedures with the least possible impairment are consistently expected by both surgeons and patients. Here, we report a clinical cohort of 10 patients who underwent LSD with a new technique and present the advantages of less impairment during performance of this new technique. Methods. A cohort of 10 cirrhotic patients with bleeding portal hypertension and secondary hypersplenism treated with LSD were studied. During the procedure, an electromechanical morcellator allowed for easy extraction of the entire massive splenic tissue without a cumbersome intracorporeal bag, enlarged incision, or hand-assisted incision. Various perioperative data were recorded. Results. LSD was successful in all patients. There was no conversion to open operations or significant perioperative complications. The operative time was 288.0 ± 53.9 minutes, the spleen removal time was 39.3 ± 15.1 minutes, and blood loss was 240.0 ± 217.1 mL. Conclusions. This new technique involving the use of an electromechanical morcellator provides expedient recovery and minimal postoperative pain and scarring. LSD with this technique is a feasible, effective, and safe surgical procedure, and embodies all the benefits of minimally invasive surgery for cirrhotic patients with bleeding portal hypertension and hypersplenism.
Introduction
With the recent significant progress in laparoscopic skills and advances in technical instruments, endoscopic surgery involving improved and advantageous techniques is performed in almost all fields of conventional abdominal surgery. However, the laparoscopic technique is much more challenging when performed in patients with cirrhosis, portal hypertension, and splenomegaly. Laparoscopic splenectomy and azygoportal disconnection (LSD) has gradually become more accepted as a treatment for cirrhotic patients with bleeding portal hypertension and secondary hypersplenism. Many different surgical techniques for LSD are currently performed by different surgeons. These techniques include the use of cumbersome intracorporeal bags to draw massively enlarged spleens, creation of enlarged incisions to morcellate and draw splenic issues, and hand-assisted laparoscopy.1-10 Because of the poor condition of patients with these diseases and the potential for development of many perioperative complications, incisions impairment of the techniques should be controlled. Here, we report LSD with a new technique that greatly reduces impairments. Massively enlarged spleens are removed from the abdominal cavity through the existing incision using an electromechanical morcellator. To the best of our knowledge, this is the first report of the use of an electromechanical morcellator to extract the entire massive splenic tissue in LSD.
The purpose of this article was to report 10 patients who underwent LSD with this new technique and present the feasibility, decreased impairment, and advantages of using an electromechanical morcellator during the procedure. This technique eliminates the need for large and cumbersome intracorporeal bags and the creation of hand-assisted or enlarged incisions to remove the spleen.
Materials and Methods
Patients
Between February 2012 and March 2012, a clinical cohort of 10 patients underwent LSD with the aforementioned new technique in our department. The clinical records of the patients were retrospectively analyzed. The preoperative diagnostic workup confirmed that all patients had liver cirrhosis, bleeding portal hypertension, and secondary hypersplenism.
The following data were prospectively collected: age, gender, etiology of cirrhosis, spleen size, Child–Pugh class, Model for End-Stage Liver Disease score, preoperative hemoglobin value, preoperative platelet count, operative time, spleen removal time, blood loss, postoperative hospital stay, perioperative complications, and length of follow-up.
Among of this cohort, none have transjugular intrahepatic portosystemic shunt (TIPS). To the best of our knowledge, TIPS is available for portal hypertension, and has its greatest usefulness as a bridge to transplantation. There are several reasons for why not select the technique of TIPS. TIPS can only reduce the portal pressure to prevent recurrent gastroesophageal variceal bleeding, but it cannot solve the problem of secondary hypersplenism. On the other hand, it was associated with a certain rate of portosystemic encephalopathy.
Patient Characteristics
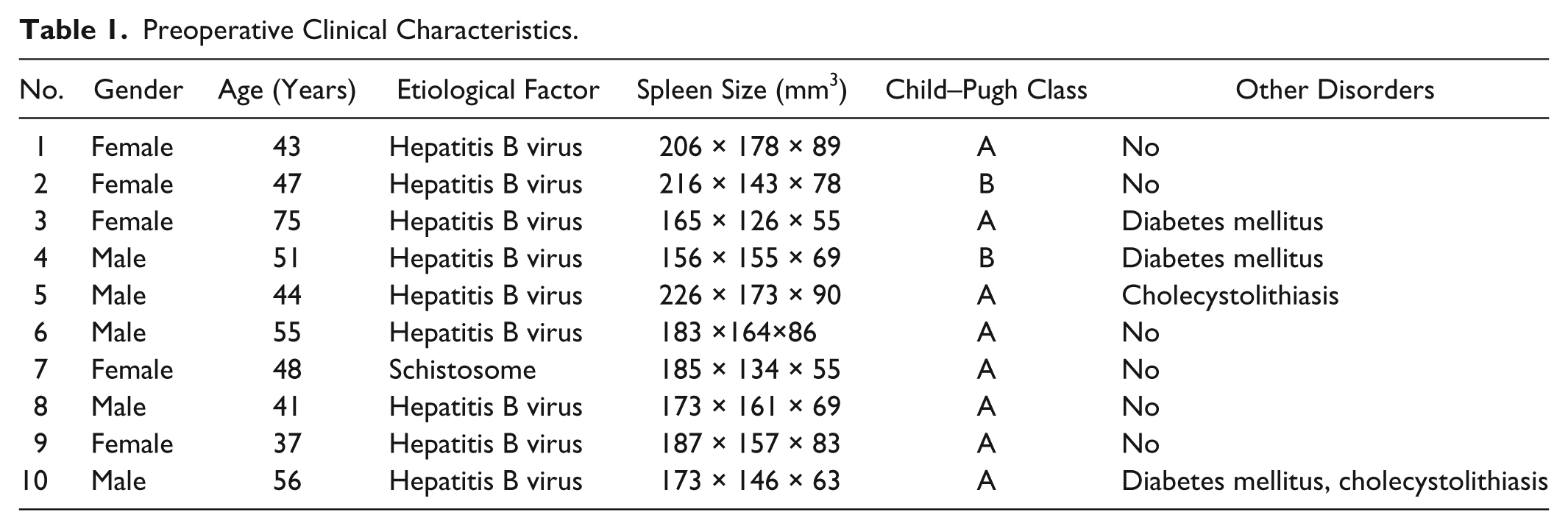
The 10 patients comprised 5 males and 5 females with a mean age of 49.7 ± 10.7 years (range = 37-75 years). Liver damage was caused by chronic hepatitis B virus in 9 patients and schistosomiasis in 1 patient. Three patients had type 2 diabetes mellitus. Two patients underwent combined LSD and laparoscopic cholecystectomy because of the experience of acute cholecystitis in their medical history and the presence of cholecystolithiasis on preoperative ultrasound. All patients had hypersplenism with an enlarged spleen. The spleen longitudinal diameter was 187.0 ± 22.6 cm. The severity of liver cirrhosis was Child–Pugh A in 8 patients and Child-Pugh B in 2 patients. Model for End-Stage Liver Disease score was 9.5 ± 1.8 (range = 6-12) with a median score of 9. All pathologic examinations of spleens revealed congestive splenomegaly. The preoperative clinical characteristics are shown in Table 1.
Preoperative Clinical Characteristics.
Surgical Technique
An orogastric tube was placed after successful induction of general endotracheal anesthesia. Urinary catheters were necessary. The positions of patients and surgeons differed based on the stage of the laparoscopic procedure. Using the Hasson (open) technique, a 10-mm trocar was placed in the umbilicus. Through this port, a 10-mm, 30°-angled laparoscope was introduced. Under direct visualization, 4 additional ports—two 5 mm, one 10 mm, and one 12 mm—were placed as illustrated in Figure 1. Only after successful LSD was laparoscopic cholecystectomy performed. The three trocars used in laparoscopic cholecystectomy were port 2, port 3 (inserted by the laparoscope), and port 4 (as the main port).
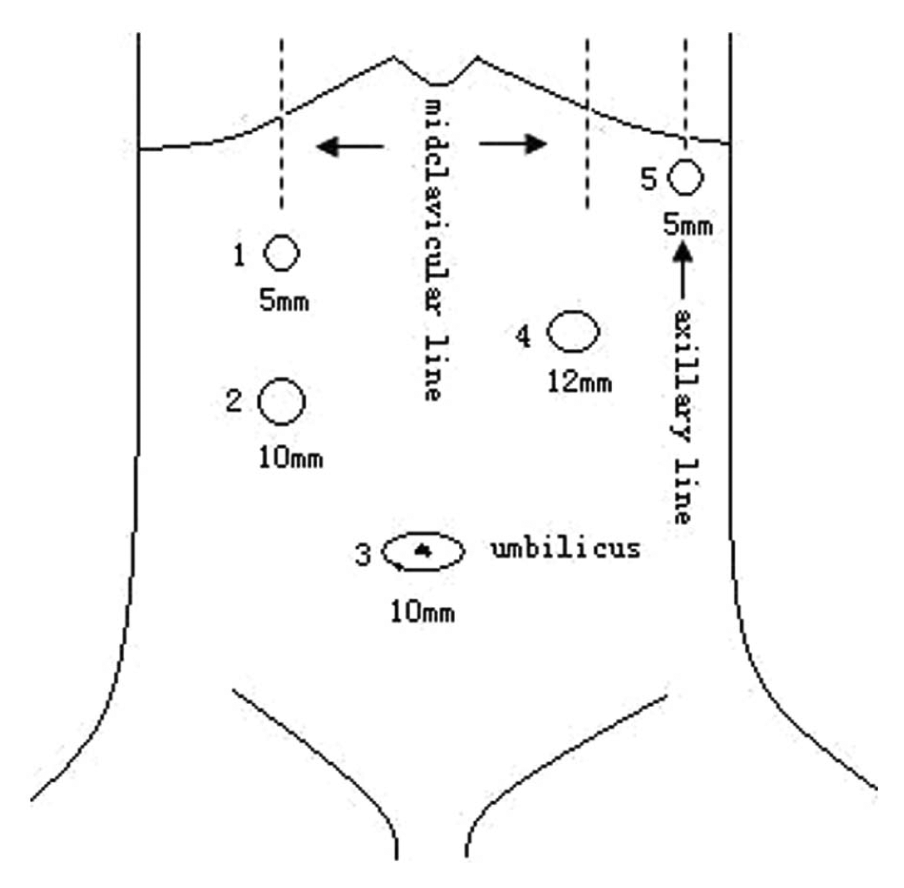
Port placement for laparoscopic splenectomy and azygoportal disconnection.
The procedures were performed as follows. Patients were first placed in the parted-legs position. When disposing of the splenic artery, the reverse Trendelenburg position was used; the surgeon stood at the right side of the patient, and port 2 was the main port used with the LigaSure vessel-sealing device (Covidien, Boulder, CO). During laparoscopic splenectomy (LS), the operating table was slightly tilted so that the left side was up at a 30° angle; the surgeon stood between the patient’s legs, and port 4 was the main port used with the LigaSure vessel-sealing device. During laparoscopic azygoportal disconnection, the position was restored to the reverse Trendelenburg position; the surgeon stood at the right side of the patient again, and port 2 was the main port used with the LigaSure vessel-sealing device. This position was maintained during removal of the spleen using the electromechanical morcellator. The surgeon preferred to be positioned between the patient’s legs, and port 4 was the main trocar used with the electromechanical morcellator.
Laparoscopic Splenectomy
The most important manipulation in this stage is blocking up the splenic artery. This can reduce the rate of conversion to an open surgical procedure and should thus be performed as early as possible at the beginning of LSD. The procedure began by opening the gastrocolic ligament to enter the lesser sac. After dividing the splenogastric ligament (excluding the short gastric vessels for the time being), the splenic artery was carefully separated from the tail of the pancreas under excellent visualization (Figure 2), then tightly tied or clipped by a hemo-locker. After ensuring good exposure of the lower pole of the spleen when lifted up by a single 5-mm splenic retractor (also known as a “liver retractor”) or the bar of a tube-type forceps, the splenocolic ligament was divided. The posterior view of the splenic wall was best obtained by gradually moving the above-mentioned instruments from the lower to the upper pole of the spleen. The retroperitoneum between the left diaphragm and the posterior margin of the spleen, the splenorenal ligament, and the splenophrenic ligament were then dissected. The use of an electrocoagulator with a dissecting spatula, rather than the LigaSure vessel-sealing device, sometimes made it easy to dissect the retroperitoneum, especially in the corners of the lower and upper poles of the spleen. At this time, because most of the surrounding ligaments of the spleen were separated, the short gastric vessels were usually better exposed using a 5-mm fan retractor or the bar of a tube-type forceps to elevate the proximal stomach in the upper right direction for easy dissection (Figure 3). Ultimately, after laparoscopic mobilization of the spleen, splenectomy was performed by carefully dissecting the splenic hilum to protect the tail of the pancreas and perform en bloc transection of the splenic artery and vein using a linear laparoscopic vascular stapler (EndoGIA, Ethicon, Cincinnati, OH) through port 4 (12 mm). The dissected spleen was then placed in the left subphrenic space.
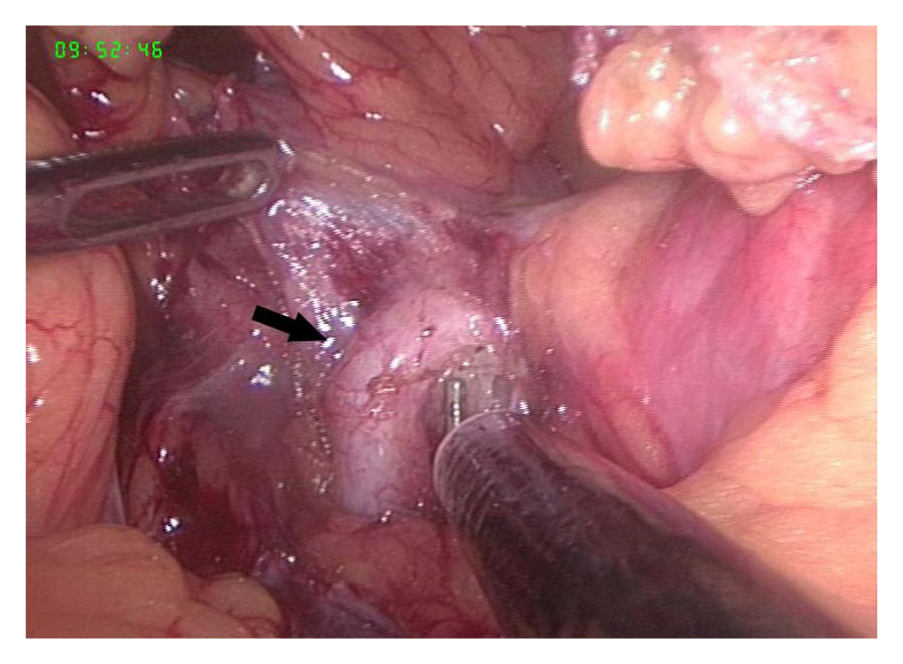
Separation of splenic artery (black arrow, the first maneuver during laparoscopic splenectomy).
Division of short gastric vessels by the LigaSure vessel-sealing device (black arrow, the final maneuver during laparoscopic splenectomy).
Laparoscopic Azygoportal Disconnection
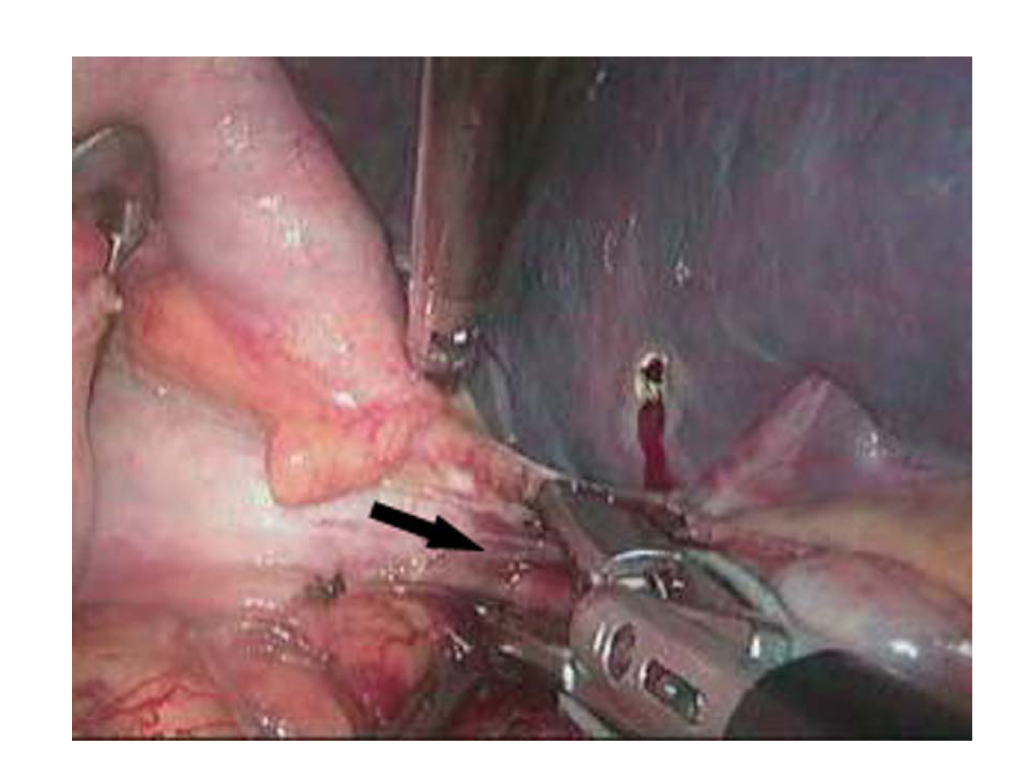
The patient was placed in the reverse Trendelenburg position. In the authors’ view, laparoscopic azygoportal disconnection should be performed in the following order: (a) paries posterior gastricus (including the vena gastrica posterior) above the superior border of the pancreas, (b) left lateral wall of the distal esophagus (length ≥8 cm), (c) left inferior phrenic veins, (d) paries posterior of the distal esophagus (length ≥8 cm), (e) gastric coronary vein (the greater curvature of the stomach is lifted and the vein dissected after having been clipped at the proximal aspect by a hemo-locker), (f) paries anterior of the distal esophagus (length ≥8 cm), (g) gastrohepatic ligament (from the front of the stomach and along the lesser curvature of the stomach), and (h) right lateral wall of the distal esophagus (length ≥8 cm). Thus, all paraesophageal venous collaterals were divided (Figure 4). The principle obeyed by these steps was as follows: from back to front, from below to above, and from left to right. The advantages of this procedure are that it is ordered, convenient, and fast. The LigaSure vessel-sealing device is continuously used during this procedure.
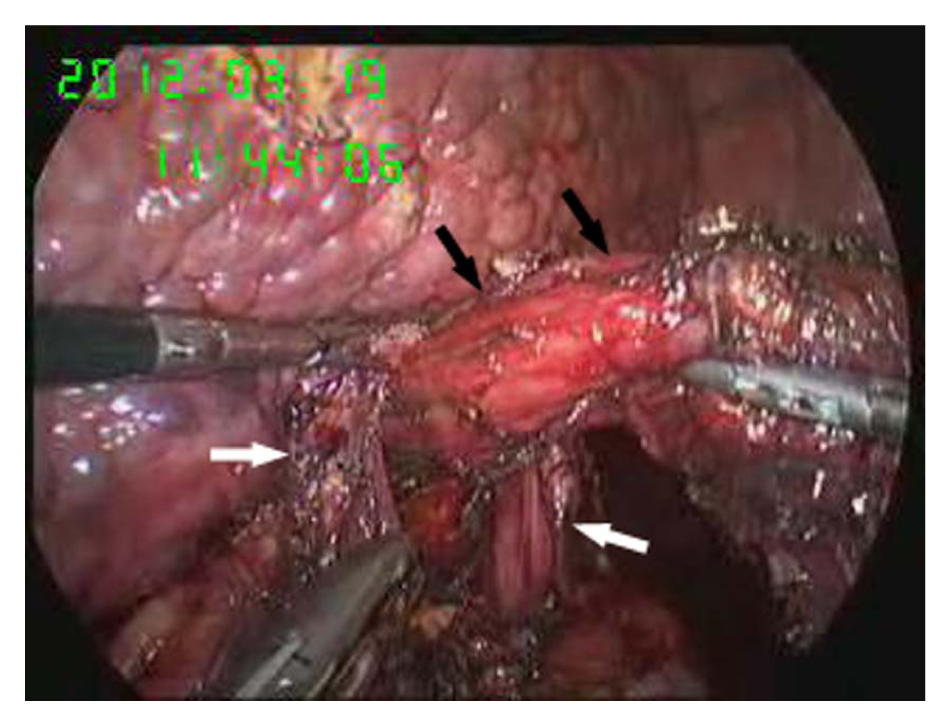
Disconnection of the distal esophagus (black arrow) between the 2 diaphragmatic crura (white arrow).
Laparoscopic Spleen Extraction Methods
All patients’ spleens were removed from the abdominal cavity using an electromechanical morcellator (TSCS, Hangzhou, China), which comprises a motor-driven cutting tube that can be inserted directly into the abdominal cavity through a 12-mm port and a large claw forceps. By using the reverse Trendelenburg position and the splenic retractor or the forceps to raise the upper pole of the spleen, the spleen was kept in the ideal location. The electromechanical morcellator was then used through port 4. The spleen was grasped by the large claw forceps through the motor-driven cutting tube, and the forceps was then pulled back while pressing the splenic tissue against the cutting edge of the rotating tube (Figure 5); the rotation could be triggered using a hand switch. A cylindrical tissue sample could be cut down and pulled out from the tube by applying a measured pulling force. This manipulation was repeated until the entire spleen was removed by the electromechanical morcellator (Figure 6). The entrance of the tube should be in view during the entire procedure to prevent damage to the surrounding organs. The entire upper quadrant was irrigated, and the operation area was carefully inspected for either residual tissue or bleeding.
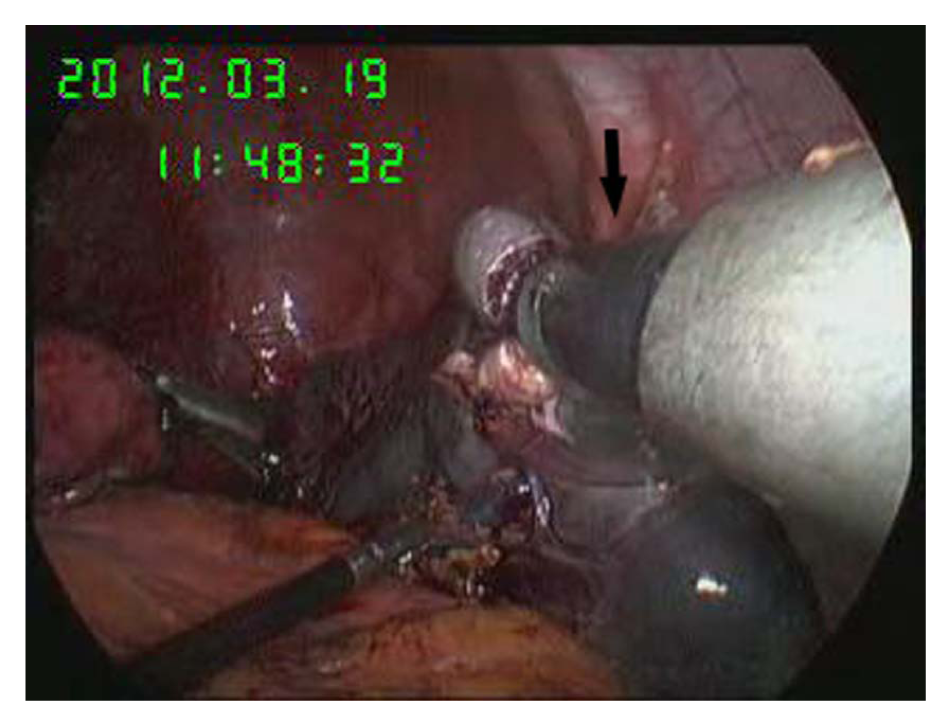
Extraction of spleen with the electromechanical morcellator (black arrow).
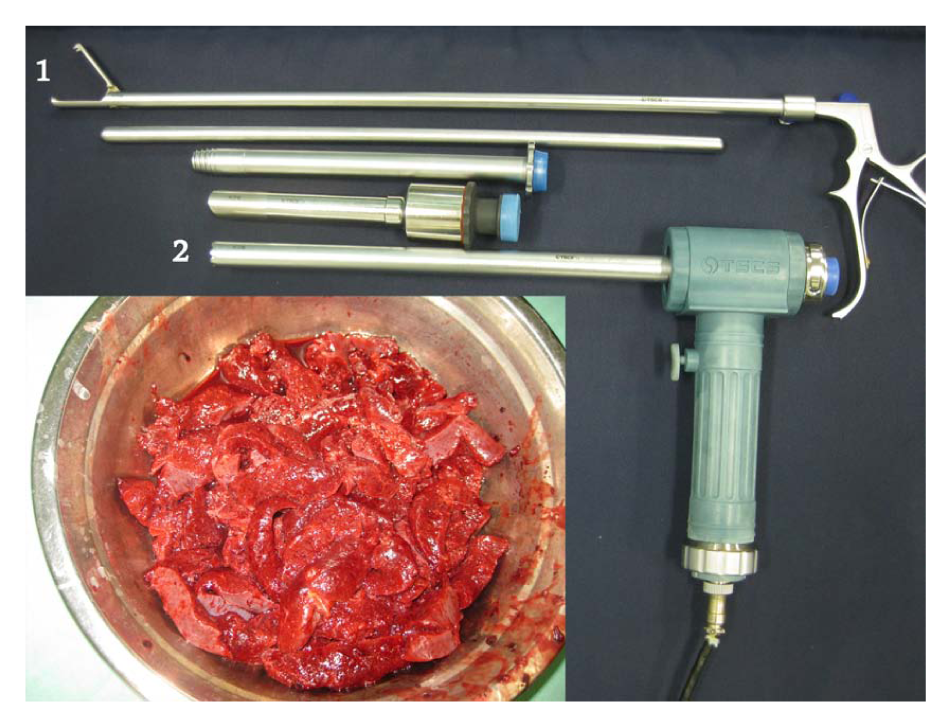
Cylindrical sections of the splenic tissue and an electromechanical morcellator (1 = large claw forceps, and 2 = motor-driven cutting tube).
Statistical Analysis
Statistical analysis was performed using SPSS for Windows, version 12.0 (SPSS, Chicago, IL). All data values are expressed as mean ± standard deviation.
Results
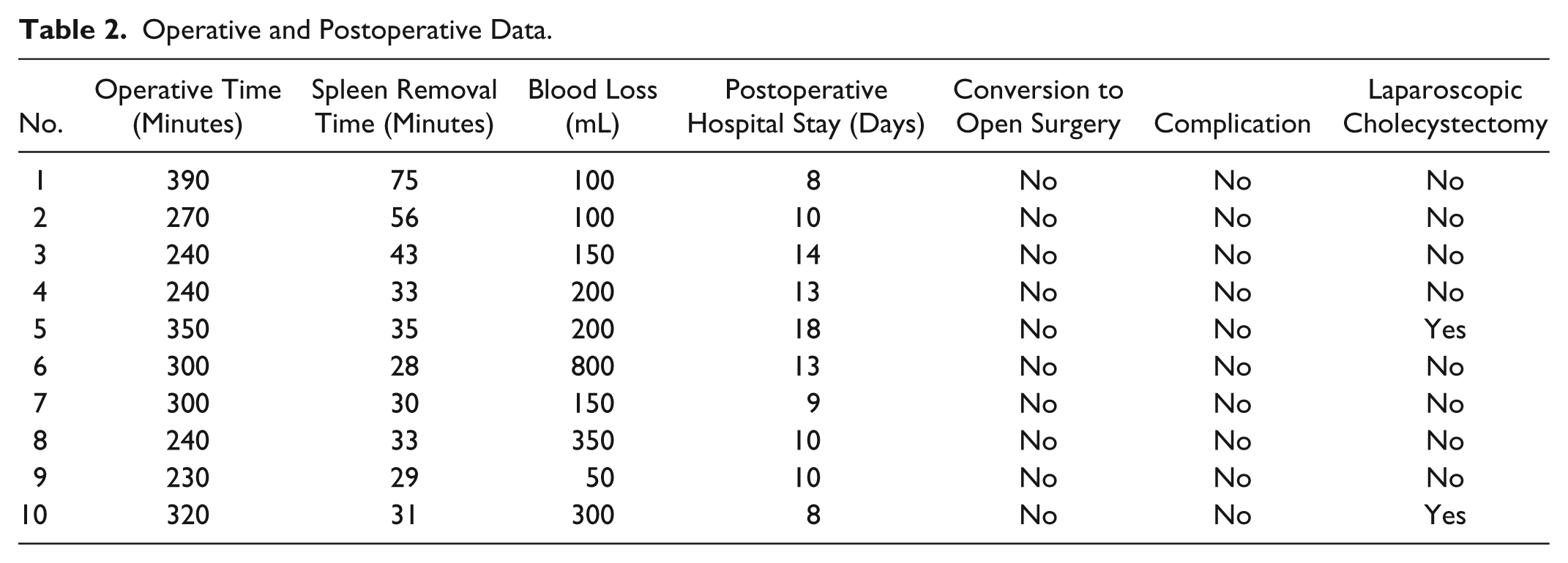
Laparoscopic splenectomy and azygoportal disconnection with the new technique described here was performed successfully in all patients. No patients were converted to open surgery. There were no intraoperative or postoperative episodes of massive bleeding. Operative and postoperative data are shown in Table 2. The operative time was 288.0 ± 53.9 minutes, the spleen removal time was 39.3 ± 15.1 minutes, blood loss was 240.0 ± 217.1 mL, and the postoperative hospital stay was 11.3 ± 3.2 days.
Operative and Postoperative Data.
Follow-up
No patient was lost to follow-up. During the mean follow-up period of 3.5 months, neither esophagus variceal bleeding nor encephalopathy occurred in any patient. All patients underwent routine blood examinations, liver function tests, and so on, at 1 and 2 weeks postoperatively, and then every 2 or 3 months. Postoperative electronic gastroscopy was performed 3 months postoperatively and revealed that the esophagogastric varices had disappeared in all patients. Examinations continue every 6 months.
Discussion
Most studies describe the use of cumbersome intracorporeal bags or the creation of a large counter or hand-assisted incision for extraction of the splenic remnant during LSD. The technique of laparoscopic spleen extraction using an electromechanical morcellator during LSD has not been previously reported. Only a few articles reported this technique 13 years ago. It was only used during LS for pediatric and adult patients with hematological disorders or other diseases.11-13
There are many risks and challenges for surgeons when LSD is performed in cirrhotic patients with bleeding portal hypertension and secondary hypersplenism. Portal hypertension and severe coagulation disorders are risk factors for high intraoperative blood loss during LS. 14 In addition, it is difficult to remove the extremely enlarged spleen because of a higher conversion rate. 15 The ideal surgical procedure is to effectively control bleeding with little impairment of liver function and a low rate of encephalopathy. 4 Bleeding is the most critical complication during LSD. This problem can be avoided with the use of advanced instruments and a skillful technique. The LigaSure vessel-sealing device is more competent than harmonic shears for disconnection. In general, the LigaSure vessel-sealing sealing system is safe, but the advantages of the electrocoagulator are ingenious. The electrocoagulator is sometimes necessary, especially in limited spaces with few vessels. Application of endoscopic linear vascular stapling facilitates dissection of the splenic hilum. These instruments reduce the rate of bleeding to a certain extent.
In our experience, 2 important manipulations must be successfully performed during LS. First, the splenic artery should be clipped or tied; second, short gastric vessels should then be dissected after all ligaments surrounding the spleen have been dissected. The effect of successful disposal of the splenic artery and short gastric vessels is not secondary to these advanced instruments, and the reasons are as follows: (a) Blocking up the splenic artery can reduce the spleen size, the risk of bleeding, and the degree of surgical difficulty, and it also has a certain autotransfusion effect. (b) Exposure of short gastric vessels before complete laparoscopic mobilization of the spleen is usually very difficult. Poor exposure may lead to bleeding or impairment of the wall of the proximal stomach.
During the 43 days from 6 February 2012 to 19 March 2012, all 10 patients underwent successful LSD with the new technique. During the LSD procedure, we extracted the spleen using the electromechanical morcellator. In our opinion, the procedure should be performed from interior to exterior, from front to back, and from the lower to the upper pole when the rotating tube extracts the splenic tissue. The time to remove the spleen was 75 minutes in the first patient, but with mastery of the surgical principals and function of the morcellator, the speed was quickly increased. A massively enlarged spleen can currently be removed with a morcellator within 30 minutes. The specimen is then collected for analysis, and the pathologist is still able to obtain detailed histological information because the excellent cutting effect prevents damage to the tissue architecture.
Makoto Hashizume et al 13 reported a method for removing the spleen in LS. The spleen is inserted into a nylon surgical sack and then removed by the morcellator while in the sack. In our view, this may lead to 2 problems. One is that the sack may be broken by the morcellator because the splenic capsule is against the sack. Thus, the fragment of the spleen may drop into the peritoneal cavity. Another is that damage to organs or tissues surrounding the sack may be caused by the morcellator because the peritoneal cavity and cannot be kept in the surgeon’s view simultaneously.
A follow-up technetium nuclear scan confirmed the absence of any splenic tissue and showed no evidence of splenosis in all patients. Follow-up will be continued for the duration of these patients’ lifetimes because splenosis from a tiny, invisible fragment may require a long period of time. In addition, if splenosis occurs, a long period of time may also be required from splenosis to hypersplenism. Although the splenic vein and artery have been dissected, there is no evidence that the veins of splenosis don’t belong to portal hypertension. Therefore, patients should undergo long-term evaluation of hemoglobin levels, white blood cell counts, and platelet counts.
In cases of massive splenomegaly, most surgeons are reluctant to perform LSD. Because placement of the spleen into an intracorporeal bag is quite challenging and creation of an enlarged incision or hand-assisted incision is necessary for removal of the spleen, the advantages of laparoscopic surgery are obviated. These patients are often at high risk for postoperative complications as a consequence of the surgical stress and insult these results from large surgical incisions. Patients who undergo conventional extraction techniques have complained of pain associated with the enlarged incision or hand-assisted incision. The technique involving the morcellator is a feasible method for solving the age-old problem of intracorporeal morcellation. The morcellator was found to safely, efficiently, and rapidly remove splenic tissue without an intracorporeal bag, an enlarged incision, or a hand-assisted incision. It provides expedient recovery and minimal postoperative pain and scarring. This new technique should enable and encourage surgeons to perform LSD, even in patients with massive splenomegaly. The technique will be easily grasped and popularized.
Laparoscopic splenectomy and azygoportal disconnection with the new technique may become the gold standard for removal of massively enlarged spleens with use of an electromechanical morcellator. This technique will extend the advantages of laparoscopic surgery to a number of patients that are likely to benefit the most, namely cirrhotic patients with bleeding portal hypertension and hypersplenism.
Footnotes
Authors’ Note
Drs Guoqing Jiang and Jianjun Qian contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.