
Abstract
Objective
The present study investigated the neural correlates of cognitive control in youth with Attention Deficit Hyperactivity disorder (ADHD) and comorbid learning disability (N = 75, ages 11-17 years) who participated in a 20-week mindfulness martial arts intervention compared to a waitlist control.
Method
EEG was recorded pre and post intervention during a blocked Go/NoGo task. Peak amplitude was measured for the inhibitory NoGo N2 and P3 ERP components.
Results
A significant group by time interaction was found for NoGo N2 amplitudes, indicating that waitlist control participants had significantly attenuated N2 amplitudes over time whereas the intervention group maintained similar levels of medial frontal activity during response inhibition. The maintenance of the individual differences in N2 amplitudes were robust in the intervention group.
Conclusions
These findings suggest that participation in mindfulness martial arts may buffer against reductions in N2 activity during adolescence for youth with ADHD
Keywords
Introduction
Attention Deficit Hyperactivity disorder (ADHD) is one of the most commonly diagnosed neurodevelopmental disorders in children. 1 Core symptoms of inattention, impulsivity and hyperactivity are first evident in childhood and continue to impact multiple domains of function across the lifespan.2,3 Symptoms of ADHD often manifest as difficulty paying attention in school, managing time, and maintaining task focus 1 and can significantly impact the quality of social interactions and social-emotional well-being. 3 In adulthood, ADHD increases risk for substance use, mood disorders, and transportation accidents. 2 Collectively, pharmacological treatments produce significant and large effects on ADHD symptoms (inattention, hyperactivity/impulsivity 4 ). Despite the efficacy of pharmacological intervention, approximately 30% of youth with ADHD do not respond to currently available pharmacological treatments, 5 and small non-significant effects of ADHD pharmacotherapy have been found for anxiety and depressive symptoms. 6 It has also been demonstrated that compliance with pharmacological ADHD treatment decreases in adolescence.7–9 Given complex symptom profiles and individual differences in treatment response, it has been suggested that a multimodal approach be taken for treating ADHD. 10 It is therefore important to investigate alternative, non-pharmacological treatments for ADHD in terms of their efficacy in addressing ADHD symptoms, compliance/engagement, and their impact on functioning.1,2
One mode of treatment is mindfulness-based interventions1,2 that focus on training attention regulation and awareness through meditation practices founded in Buddhist principles. 11 Mindfulness is based on the notion of focusing on the present without judgment, with an accepting mindset, rather than a reactive one. 11 Mindfulness engages cognitive and emotional processes that are commonly affected in ADHD, including sustained attention and non-reactivity. 12 As such, its efficacy in youth with ADHD has been increasingly explored. In addition to attention and impulsivity, difficulties with self and emotion-regulation are also symptoms that significantly influence functioning in youth with ADHD. 13 Mindfulness interventions may address these areas over and above pharmacological treatments. 14 Overall, mindfulness-based interventions have been linked to improvements in ADHD symptomatology, including specific improvements in attention. 12 Although mindfulness-based interventions for ADHD have shown improvements based on parent and self-reports, 15 and/or behavioral outcomes on the stroop task or continuous performance tasks, 16 less is known about changes that may occur at a neural level, particularly in the medial frontal cortex. Both fMRI17,18 and EEG19–23 studies have shown that ADHD is associated with reduced activity in medial frontal regions which are important for cognitive control.
Go/Nogo tasks have been used extensively to index response inhibition in children and adults. 24 During the task a participant is required to make frequent responses to a stimulus and inhibit their response to less frequent NoGo stimuli. These paradigms reliably engage cognitive control processes related to inhibition and evoke the Nogo N2/P3 ERP components. 24 Other response inhibition paradigms, such as a stop signal task or continuous performance tasks also elicit the Nogo N2/P3 ERP complex following successful inhibition of prepotent motor responses. 24 The NoGo N2 has been shown to increase (become more negative) in amplitude during successful response inhibition. 25 In addition, the N2 can be evoked by stimulus presentations that involve a conflict in two competing response options, 24 suggesting that the Nogo N2 may also capture a general cognitive control process that is linked to motor response inhibition.24,26,27 In ADHD, N2 amplitude has been shown to be significantly reduced, which is thought to reflect clinical deficits in inhibitory processes and attention.19,20,23,28,29 Another ERP component that is consistently evoked is the P3, which is also larger when prepotent responses are inhibited. 21 Unlike the Nogo N2, the Nogo P3 seems to be directly related to the inhibition of a motor response.24,26 Similar to the NoGo N2, P3 amplitude has been shown to be smaller in children with ADHD during selective attention tasks19,21 and positively correlated with improved response inhibition. 21
Mindfulness training is thought to engage and improve cognitive processes that are impacted by ADHD 12 and has been shown to impact the Nogo N2/P3 ERP complex. EEG studies of adults (without ADHD) who regularly participate in mindfulness meditation practice have shown larger N2 and P3 amplitudes on an auditory oddball inhibition task when compared to a control group, suggesting that meditators allocate more attentional resources to task-relevant stimuli compared to non-meditators. 30 Furthermore, Pozuelos et al, 31 demonstrated that, compared to waitlist controls, adults who participated in a 3-week mindful breathing program displayed enhanced Nogo N2 amplitudes and improved inhibitory control. Mindfulness training in inexperienced adolescents also led to increased N2 amplitudes during response inhibition, 32 suggesting that mindfulness related gains in attentional resource allocation may be captured by the frontal NoGo N2, in both adults and adolescents.
Despite the link between ADHD symptoms and ERP components indexing inhibitory control, only a handful of studies have used EEG measures to investigate mindfulness intervention in ADHD. In a study of mindfulness based cognitive behavioral therapy (MCBT) in individuals with ADHD, Schoenberg et al 33 found significant increases in NoGo-P3 amplitude post-MCBT, which correlated with reduced hyperactive/impulsive symptoms. Previous work investigating mindfulness martial arts (MMA) training found that children with ADHD showed a decrease in theta/beta ratio during a Go/NoGo task, perhaps reflecting increased sustained attention allocation. 34 Although mindfulness-based interventions, including MMA, have shown an impact on neural indices of attention and cognitive control, there is still much to be learned about how event related cortical markers of inhibitory control, specifically the Nogo N2/P3 complex, respond to mindfulness interventions in youth who have ADHD.
The Present Study
Mindfulness interventions have been suggested to improve response inhibition, demonstrated by modulation of the Nogo N2/P3 complex in samples of healthy adults and typically developing children. Although there is a paucity of EEG studies which investigate mindfulness interventions in youth with ADHD, these existing studies have produced similar results. The present study aims to assess the impact of the MMA intervention on the Nogo N2/ P3 complex in a subset of youth with ADHD seeking treatment due to concerns about function and social-emotional well-being. We expected that NoGo N2 and P3 amplitudes would increase from pre- to post-treatment in the treatment group, and not in the waitlist control group.
Methods
Mindfulness Training Program
The intervention group participated in a MMA intervention, a group intervention designed to treat attention, inhibition, and self-regulation symptoms in youth with ADHD. MMA uses mindfulness meditation instruction, yoga, cognitive behavioral therapy, and martial arts in a health promoting, non-stigmatizing environment. Youth attended weekly 90-min sessions for 20 weeks. Sessions were conducted by one of two instructors, both of whom were child and family therapists holding a Master's degree in Social Work. More detail on MMA can be found in Milligan et al. 35
Participants
The study sample consisted of 44 treatment participants (7 female) ages 11-17 (M = 12.90, SD = 1.77), and 31 waitlist control participants (3 female) aged 11-16 (M = 12.76, SD = 1.43). Complete EEG recordings at both time points were available for 27 (6 female) individuals aged 11-17 (M = 12.96, SD = 1.85) in the treatment group and 18 individuals (3 female) aged 11-16 (M = 12.63, SD = 1.32) in the waitlist control group. This sample of children with ADHD were recruited from a community-based children's mental health center for youth with learning disabilities (LD). Admission to the program required a diagnosis of an LD from a registered psychologist. Many children admitted to the MMA program had prior diagnoses of ADHD. In the sample used for this study, all treatment and control participants met the diagnostic criteria for ADHD, which was screened once admitted to the program through the Mini International Neuropsychiatric Interview for Children and Adolescents- Parent Version (MINI KID-P). 36
Procedures
Participants and their parents attended two testing sessions 20 weeks apart. Informed consent was obtained from the caregiver at each session, and child assent was also obtained before proceeding. All participants were compensated for their participation. This is a secondary analysis of historically collected data, at the time the data was collected, there was no Canadian requirement for clinical trial registration. During the pre-treatment session, parents completed a diagnostic interview (MINI KID-P), ADHD rating scales, and provided demographic information. At both testing sessions, youth completed a computerized task while EEG was recorded. EEG was recorded using the BioSemi ActiveTwo system, with 64 scalp channels in the international 10/20 layout, plus 8 exogenous electrodes to capture muscle activity related to eye movements, blinks, and facial EMG. The zero-reference principal voltage values (each site quantified relative to the driven right leg and common mode sense loop) were digitized at a rate of 512 Hz.
Measures
MINI KID-P
ADHD diagnoses were confirmed using the parent version of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI KID-P 36 ).
Conners- 3 (CPRS)
The Conners 3-Parent (Conners 3-P 37 ) is a 110-item parent questionnaire assessing a child's ADHD symptom presence and severity. Parent ratings can be obtained for youth from ages 6-18. Items are scored on a four-point Likert scale (never, occasionally, often, very often). The assessment includes multiple scales which assess different ADHD concerns such as inattention, hyperactivity, and executive function. 37 Internal consistency is high with Cronbach's alpha ranging from .77 to .97.
Behavior Rating Inventory of Executive Function (BRIEF)
The Behavior Rating Inventory of Executive Function Parent Form (BRIEF 38 ) is an 86-item questionnaire designed to assess executive functioning in youth ages 5-18. The scale consists of two indexes (behavioral regulation and metacognition) in addition to a global executive composite. 39 Internal consistency is high with coefficients ranging from .9-.98.
Blocked Go/NoGo Task
A modified Go/NoGo task 40 was employed that requires participants to respond as quickly as possible to target go stimuli and withhold responses to infrequent NoGo stimuli. The response stimulus was a plus sign that was black or white (counterbalanced across participants), the color of which indicated whether the current trial was Go or NoGo. The plus sign was presented inside a central square border that periodically changed color, every 2-8 trials, simultaneously with the onset of a Go stimulus. The color of the border defined the current response block, which included either all Go trials or a combination of Go and NoGo trials (See Figure 1). All the information about task, trial types, and color-context associations were provided to participants. With prior briefing, individuals did not need to learn these associations or task rules through trial and error, and instead could use the response cue information to modify their attention and behavioral control for optimal performance. The task included a total of 444 Go trials, evenly distributed between the response blocks (222 during all Go trial blocks, 222 during mixed Go/NoGo trial blocks), and 72 NoGo trials. The visual angle for plus sign stimulus in this task was approximately 0.24 × 0.24 degrees, and 0.72 × 0.72 degrees for the border. Go and NoGo stimuli were presented for 50 ms and were followed by a 2-s response window, with an intertrial interval selected randomly between 400 and 900 ms after the response. E-prime v.2.0 (Psychology Software Tools, Inc.) software package was used to control stimulus presentation.
EEG Pre-Processing and Data Reduction
EEG data were processed using the EEG Integrated Platform-Loss (EEG-IP-L) pipeline 41 on the Shared Hierarchical Academic Research Computing Network (SHARCNet), in Octave 3.6.3. EEG-IP-L employs a standardized approach to assess signal quality through data annotation of channels, time periods, and independent components (ICs) that reflect stereotypical artifacts (eg, eye-blinks, cardiac responses, muscle tension) and relative periods of non-stationarity (available here: https://github.com/BUCANL/EEG-IP-L). For each assessment measure, the continuous data are epoched into 1-s non-overlapping time windows and the distribution values of interest (eg, voltage variance) are examined against a criterion threshold (eg, interquartile range) and data are then classified and flagged if they are consistent outliers (eg, 20%). A single dipole was fit to each independent component and the ICLabel extension for EEGLAB was used to classify components into seven source categories (brain, eye, muscle, heart, channel noise, line noise, and other 42 ). IC categorical classification was retained if the predicted value was above 30%. In cases where the predicted value was less than 30%, the IC category was set to ‘other’. ICs were flagged for removal if classified as eye, muscle, heart, or channel noise, or when residual variance in the dipole fit was greater than 20%. Following the automated procedures, a semi-automated interactive quality control was performed to review decisions on signal quality assessments. Figure 2 provides a schematic summary of the signal quality assessment measures, criterion threshold, outlier flagging, and the percentage of data that were identified as containing unreliable signals. Channels, time points, and independent components were removed from the continuous data if flagged during pre-processing or quality control review.
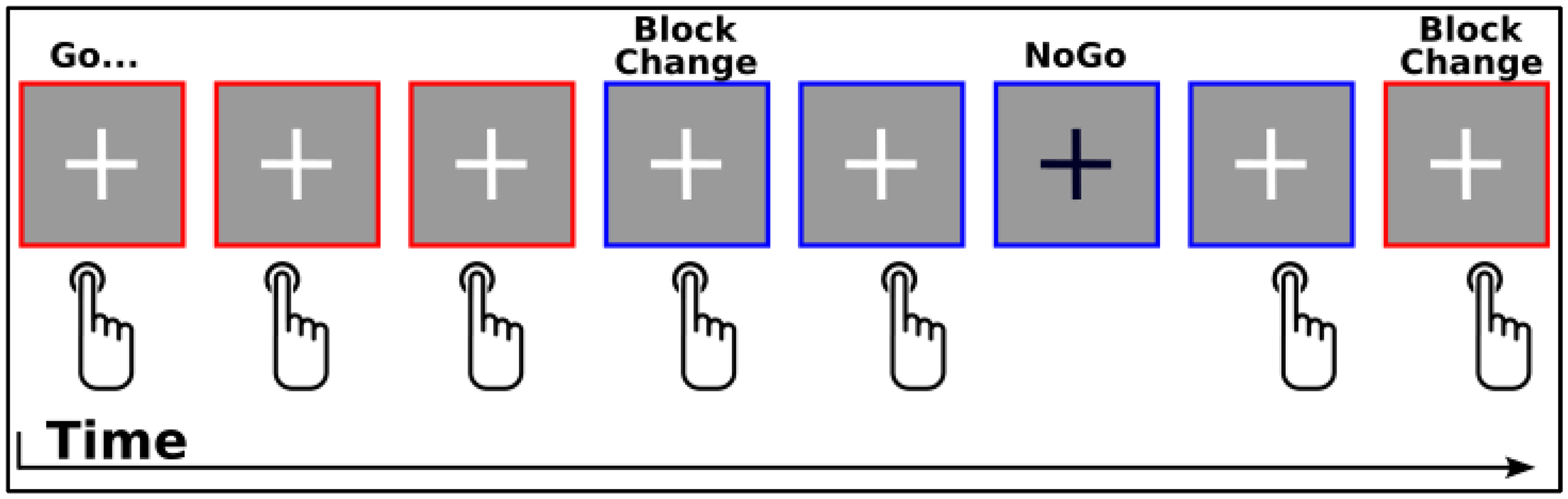
Visual Example of Blocked Go/NoGo Task.
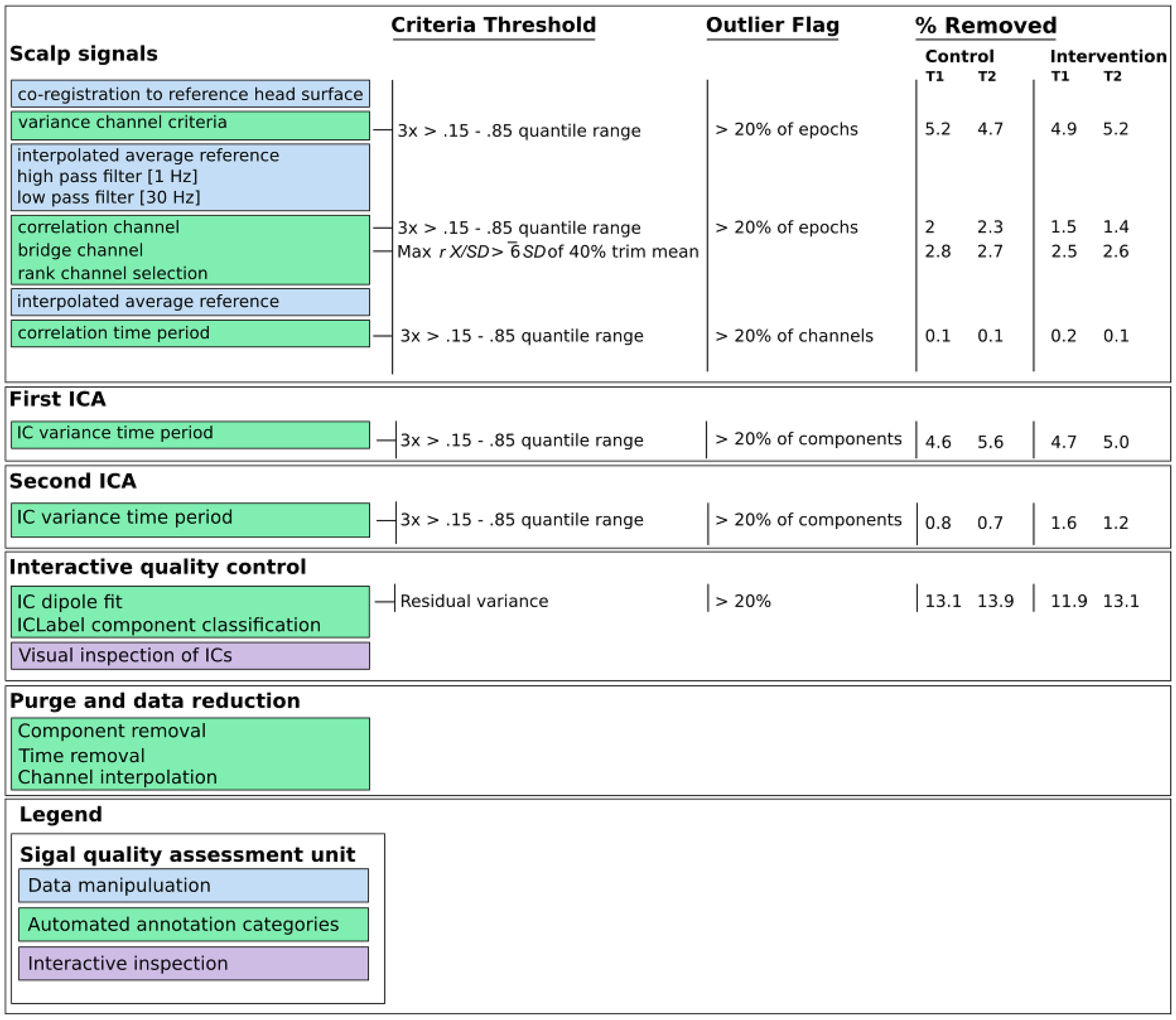
Overview of Data Processing.
Overall, EEG recordings were stable such that, on average, 93.8% of in-task time (Mrange of 93.5% to 94.5%), 90.55% of channels (Mrange of 90% to 91.1%), and 51.61% of components (Mrange of 49.29% to 53.93%) were retained
EEG Signal Extraction
Similar to previous studies the NoGo N2 was scored as the minimum voltage from a fronto-central26,27 channel cluster (corresponding to Cz, FCz, and Fz locations) during the 200-350 ms window. The NoGo P3 was scored as the maximum voltage from the fronto-central channel26,27 cluster (corresponding to Cz, FCz, and Fz) during the 300-600 ms window.
Statistical Analyses
Data were analyzed using EEGLAB and IBM SPSS 27, including independent samples t tests and one way ANOVA to explore pre-treatment group differences, as well as mixed repeated measures analysis of pre-post intervention changes in task performance and ERP amplitudes.
Results
Participant Characteristics
Independent samples t tests were used to assess pre-treatment group differences. The results of these analyses are presented in Table 1. The only measure found to be significantly different between groups was the inattention scale on the CPRS; t(71) = 2.12, P = .04, with the intervention group having lower inattention scores (but still within the clinical range). One way ANOVA revealed that there was no difference in ADHD subtype diagnosis between the groups F(1,51) = .43, P = .51.
Summary of Demographic Information and Independent Samples t-Tests on Pre-Treatment Group Differences.
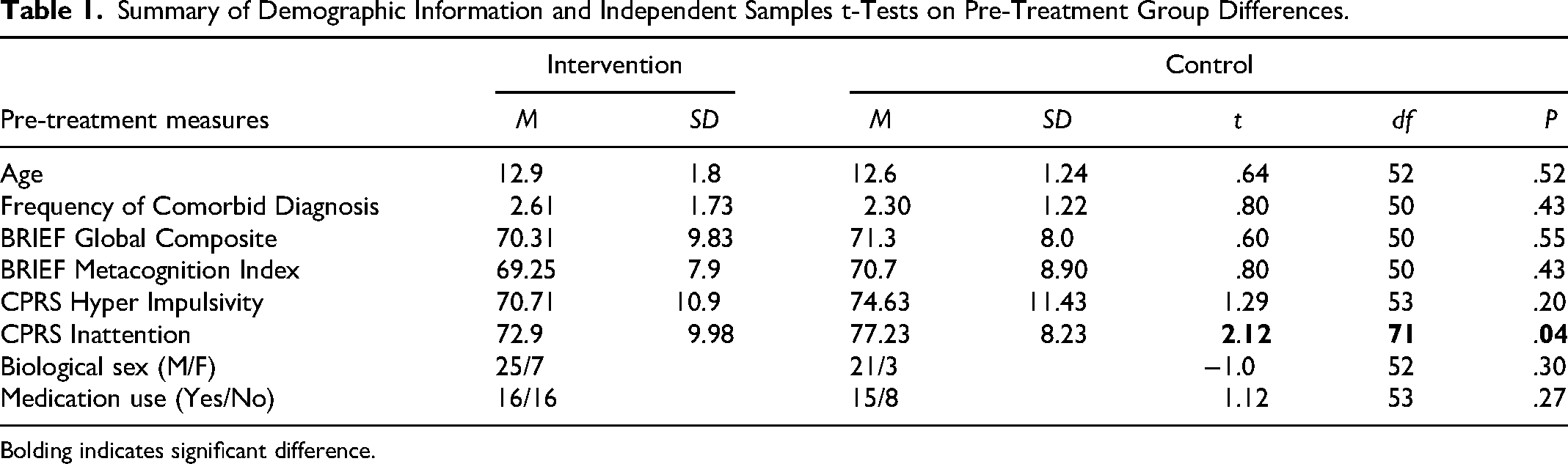
Bolding indicates significant difference.
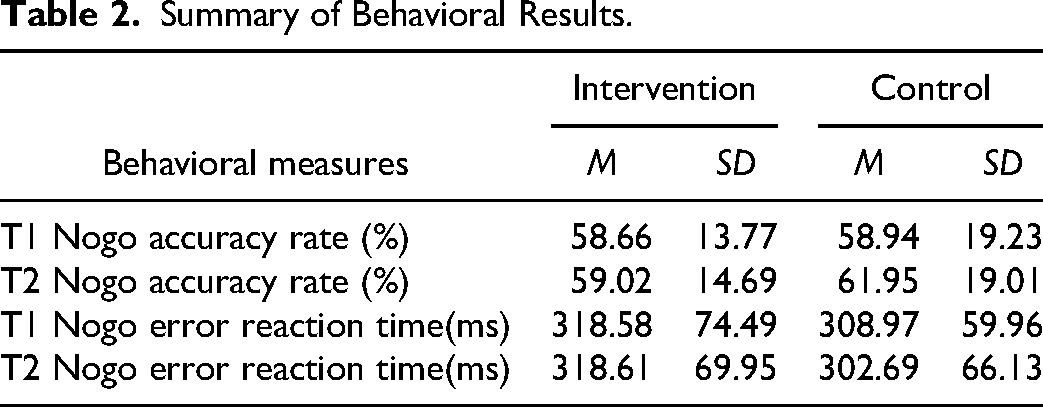
Summary of Behavioral Results.
Response Queuing Task
Task Performance
Task performance was assessed using a 2 (group: treatment, control) × 2 (time: pre, post) mixed ANOVA with repeated measures on the last factor. There were no significant main effects of group F(1,40) = .24, P = .63, η²p = .006 the effect of time was at alpha F(1,40) = 3.9, P = .054, η²p = .09 and the interaction was not significant F(1,40) = .06, P = .80, η²p = .002 for NoGo error reaction time. Similarly, there were no significant main effects were found for group F(1,42) = .96, P = .34, η²p = .022; time F(1,42) = .184, P = .67, η²p = .004; or the interaction F(1,42) = .20, P = .65, η²p = .005 for NoGo response accuracy. The findings indicate that waitlisted control and intervention groups performed comparably at both time 1 and time 2 sessions (See Table 2).
NoGo N2/P3
To examine treatment group differences in ERP amplitudes, 2 (group: treatment, control) × 2 (time; pre-test, post-test) mixed ANOVA with repeated measures (RM) on the last factor were used. The RM ANOVA for NoGo N2 amplitudes revealed no significant main effects of group F(1,40) = .67, P = .42, η²p = .016; or time F(1,40) = 2.35, P = .13, η²p = .056. A significant group by time interaction F(1,40) = 4.8, P = .03, η²p = .108, was observed. Follow-up paired sample t-test indicated that the control group showed a significant reduction with large effect in NoGo N2 amplitude across time t(15) = −2.9, P = .01, Cohen's d = .73. Follow up tests in the intervention group showed no significant change with a small effect t(25) = .49, P = .63, Cohen's d = . 097.
In contrast, a RM ANOVA revealed no significant effect of group, F(1,40) = 1.07, P = .31, η²p = .026; time, F(1,40) = .056, P = .81,η²p = .001; or group by time interaction, F(1,40) = .014, P = .90, η²p < .0001, were observed for NoGo P3 amplitudes. See Figure 3.
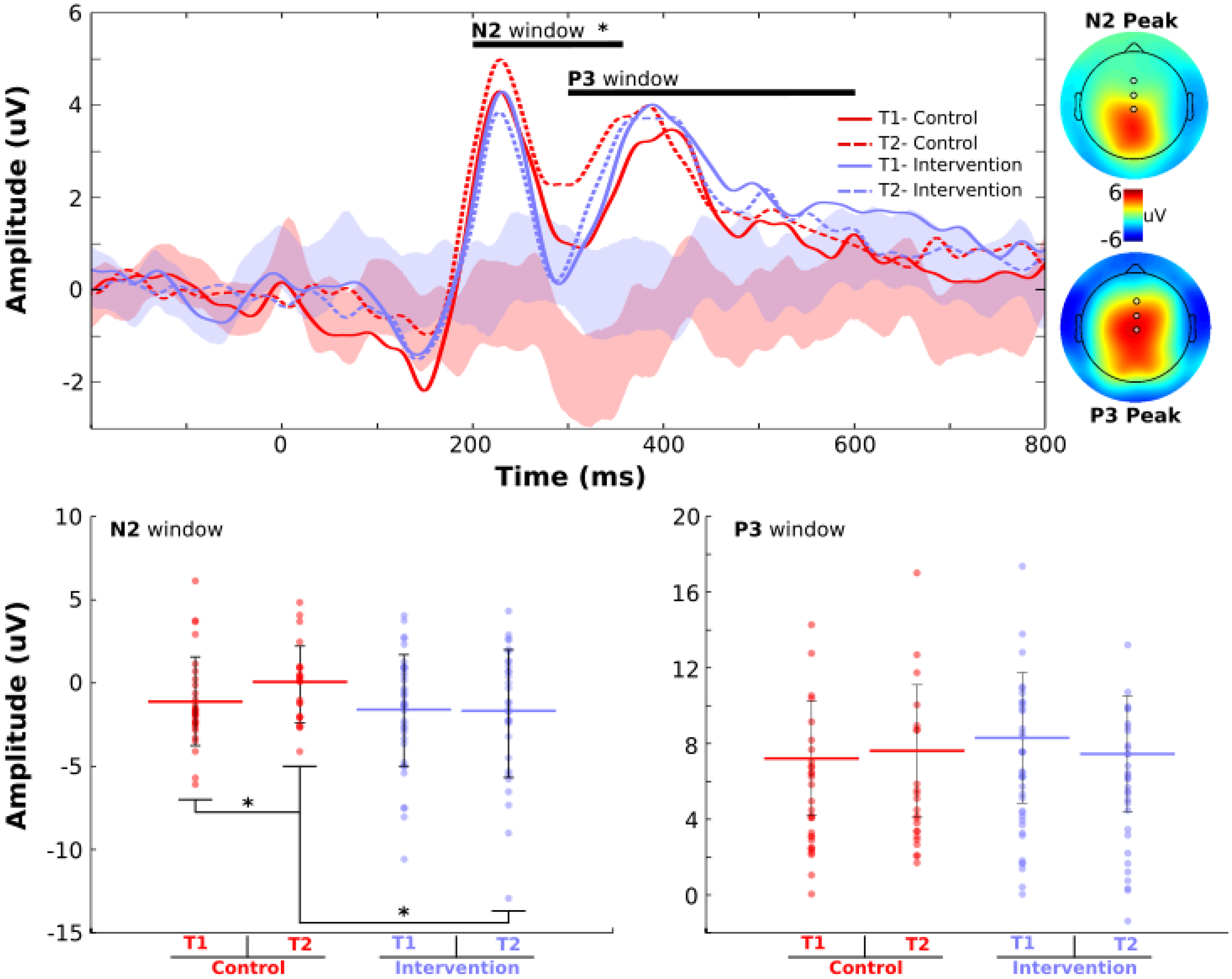
Grand Averaged ERP Waveforms (Top) and Peak Topographical Maps. NoGo N2/P3 Waveforms from Fronto-Central Midline ROI and 95% Bootstrapped Confidence Intervals of the Differences for Each Group Across Time. Bottom Panel: NoGo N2 and P3 Peak Amplitudes. Individual Participants Represented by Dots, Group Mean by Horizontal Colored Bars, and Error Bars of ±1 SD. *P < .05.
Difference Wave
To better isolate specific differences between trial types, we calculated the difference wave (NoGo - Go) between NoGo and Go trials from the mixed blocks that contained both trial types. A 2 (group: treatment, control) × 2 (time; pre-test, post-test) mixed ANOVA with RM on the last factor were used. RM ANOVA for the N2 difference wave revealed no significant main effects of group F(1,30) = .314, P = .58, η²p = .01, or time F(1,30) = 1.16, P = .88, η²p = .001. A significant group by time interaction F(1,30) = 5.7, P = .023, η²p = .161, was indicated.Follow up paired samples t-test indicated a marginal small effect size for the intervention group t(19) = 1.89, P = .075, Cohen's d = .42. Follow up testing also indicated a non-significant change with a moderate effect size within the control group t(11) = −1.8, P = .10, Cohen's d = .52. This pattern of results reflects a cross-over interaction, whereby the difference between NoGo and Go trials across time was in opposing directions between the intervention and control groups. Specifically, the difference between NoGo and Go trials in the intervention group became more negative over time. Given that the NoGo N2 amplitude was stable in the intervention group, this change condition difference was due to an attenuated peak to Go trials at time 2 compared to time 1. Conversely, although not statistically robust, the control group demonstrated a larger condition difference that was driven by an attenuated NoGo N2 amplitude over time. See Figure 4.
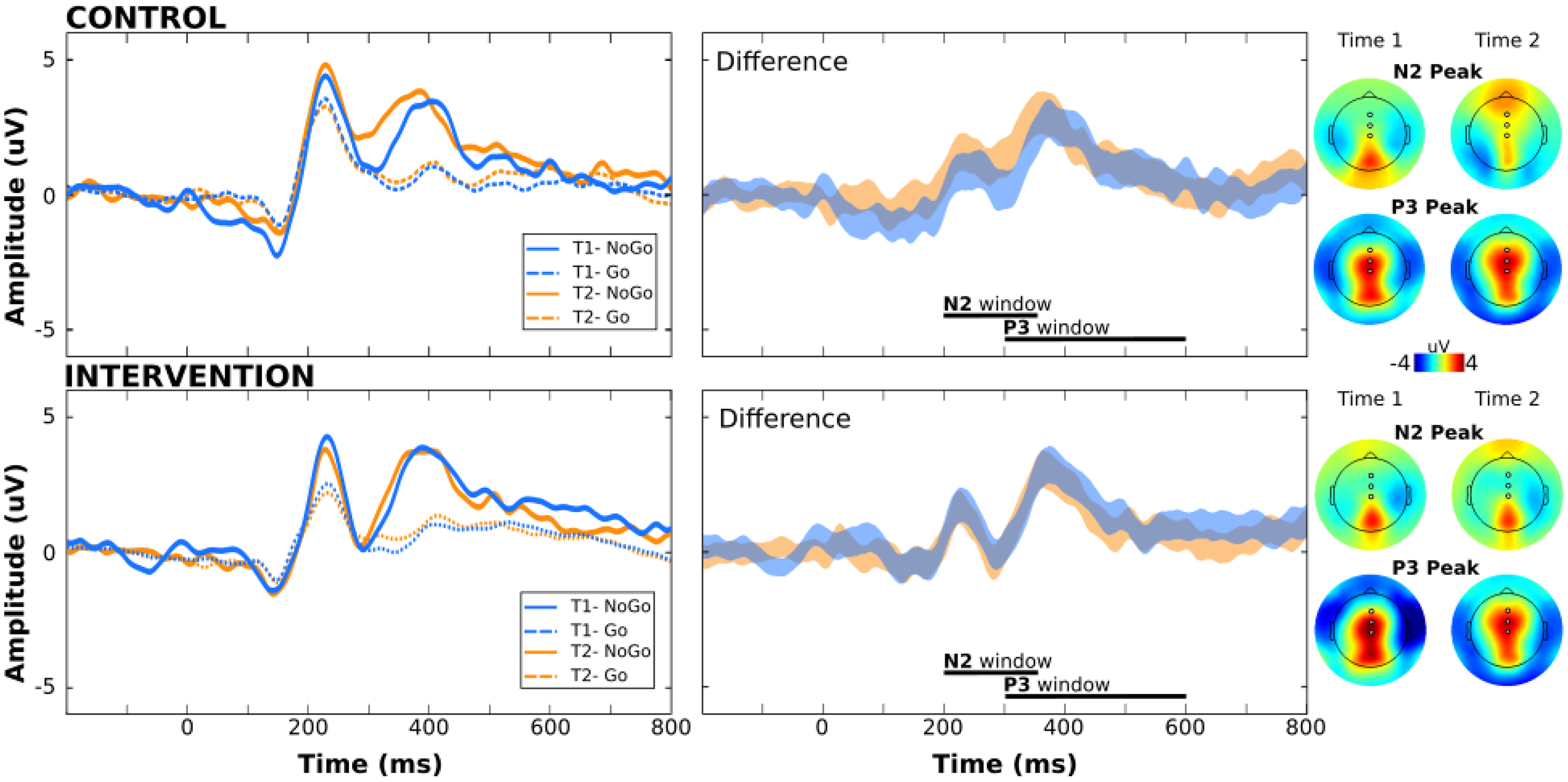
Grand Averaged ERP Waveforms (Left) and for NoGo (Solid) and Go (Dashed) Trials for the Control (Top) and Intervention (Bottom) Groups, for Time 1 (Blue) and Time 2 (Orange) Sessions. The 95% Bootstrapped Confidence Intervals of the Condition Differences (NoGo - Go) for Each Group Across Time Are Shown to the Right, with Corresponding Topographical Difference Maps for the N2 and P3 Peaks.
RM ANOVA for the P3 difference wave revealed no significant main effects of group F(1,30) = .131, P = .72, η²p = .004; or time F(1,30) = .68, P = .415, η²p = .022. No significant group by time interaction was indicated F(1,30) = .129, P = .72, η²p = .004.
Individual Differences: NoGo N2/P3
To further investigate the group by time interaction for N2 amplitudes, a series of non-parametric correlation (Spearman's Rho) bootstrap tests were conducted by group between time 1 and time 2 for N2 and P3 amplitudes. Examining these individual differences was done to examine whether the lack of change in the intervention groups reflects a stability in N2 amplitudes over time. Specifically, individual paired values (eg, N2 amplitudes at time 1 and time 2) were randomly sampled, with replacement, to create a surrogate distribution, which was winsorized at 10% to minimize potential outliers before calculating the correlation coefficient. The process of resampling, winsorizing, and calculating the correlation coefficient was iterated 5000 times to generate the Rs distribution and 95% confidence intervals. N2 amplitudes were significantly correlated in the intervention group (Rs = .56, P = .006), but were not robust in the control group (Rs = .34, P = .48). P3 amplitudes were similarly robust in both the intervention (Rs = .45, P = .04) and control groups (Rs = .47, P = .048). See Figure 5.
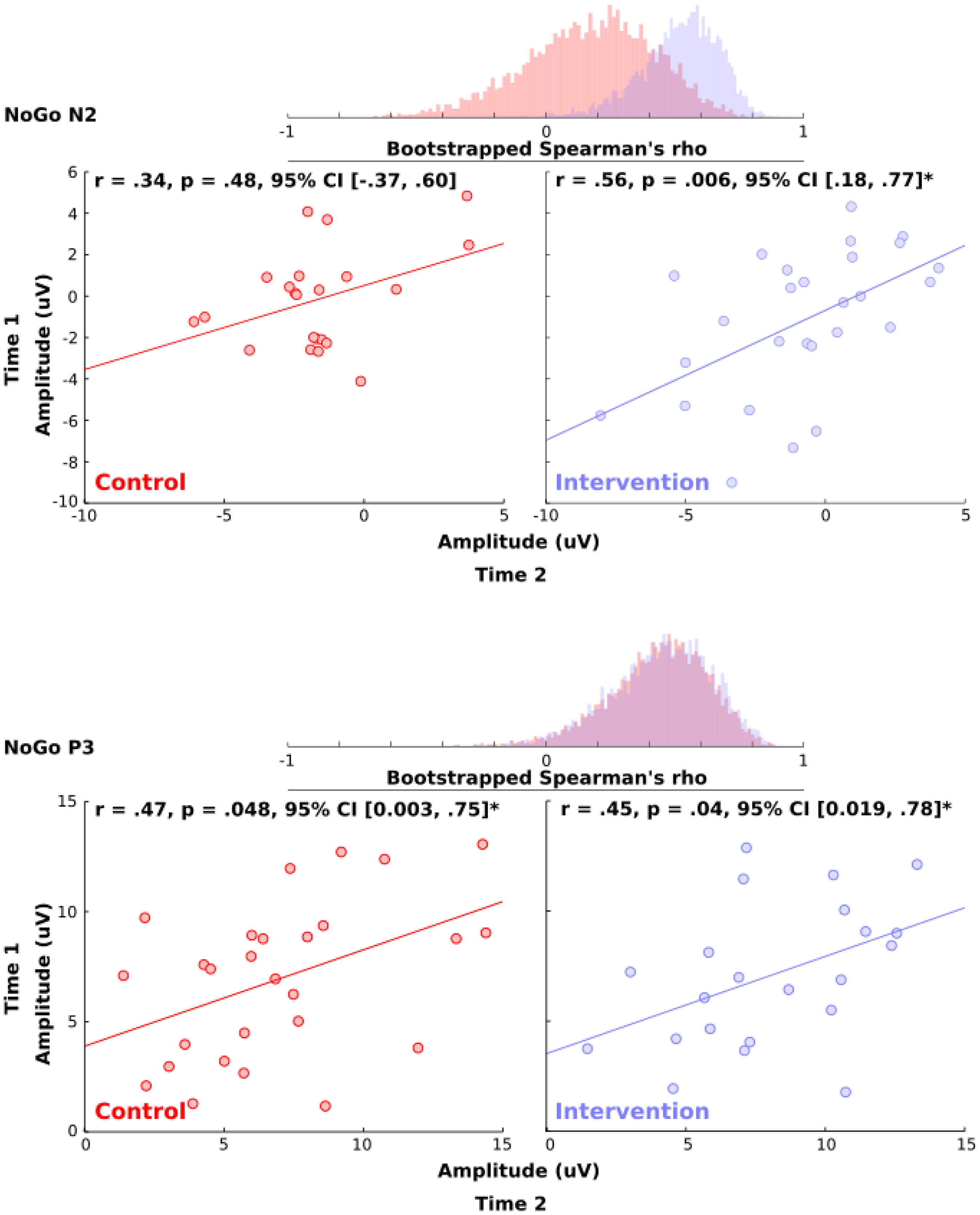
Scatter Plots for NoGo N2 (Top) and P3 (Bottom) Amplitudes from Time 1 to Time 2 in the Control (Left) and Intervention (Right) Groups. *P < .05.
Discussion
We investigated whether a mindfulness intervention impacts ERP markers of cognitive control and response inhibition which have been found to be altered in ADHD. We found that there was a significant decrease in NoGo N2 amplitude across time for those who were part of the waitlist control group, while those in the intervention group did not show significant change. The present findings suggest that not participating in this mindfulness intervention predicted a significant decrease in medial frontal function, indexed by the Nogo N2. We hypothesized that there would be a significant increase in Nogo N2 amplitudes from pre- to post-treatment in the intervention group. Although the increase in Nogo N2 from pre- to post-treatment did not reach statistical significance in the intervention group, the amplitude change was in the expected direction. We found that the waitlist control group showed a significant reduction in NoGo N2 amplitudes from time 1 to time 2, suggesting that the MMA intervention perhaps buffers against attenuation of medial frontal function as reflected by NoGo N2 amplitude. Accordingly, maintenance of medial frontal activity in the intervention group resulted in a significantly larger NoGo N2 amplitude following treatment compared to the waitlist control group. The result of a cross over interaction for the NoGo - Go difference wave indicated that youth in the intervention group showed a marginal reduction in N2 amplitude to Go trials over time while maintaining similar levels of N2 activation during inhibitory control. Youth in the control group, however, showed similar levels of medial frontal activity over time during Go trials, but had a significant reduction in N2 activity during inhibitory. In addition, NoGo N2 amplitudes were correlated over time in participants who took part in the intervention, while there was no robust association of N2 amplitudes across time for the waitlist control group. These results, taken together with prior findings where NoGo N2 amplitudes have been shown to be reduced in those with ADHD,19,20,22,23 and shown to be increased in cases of successful response inhibition in healthy controls, 25 it appears to be the case that the MMA intervention buffered against the reduced N2 that is typical of ADHD.
These findings partially support our hypotheses, also shown by trend level increases in NoGo N2 amplitude following treatment. The intervention group maintained a similar N2 amplitude from pre to post treatment, which suggests that the MMA intervention has maintenance effects on neural indicators of response inhibition. Taken in context with the significant reduction in the N2 seen in the control group, intervention participants maintained a similar level of medial frontal engagement when inhibiting responses compared to the control group. This supports findings from prior EEG studies on the same MMA intervention, which found improved theta/beta ratio in a Go/NoGo task, from pre to post-treatment, and suggesting that youth in the intervention condition were engaging in more active and focused thought versus unfocused thought in the context of inhibiting behavior. 34
Our results were not accompanied by post intervention improvements in task performance. However, prior review in non-clinical populations suggests that mindfulness related changes in the alerting system are subtle and may take time before manifesting as significant performance improvement, 44 while simultaneously suggesting that the N2 can be interpreted as a marker of inhibition that indexes improvements in attention shifting and alerting skills after mindfulness training.44,45 Our results are in line with these previous findings and indicate that NoGo N2 amplitude is a measure which is responsive to mindfulness based therapies in youth.
There were no significant changes in the NoGo P3 amplitudes during response inhibition, however a trend level decrease was observed in the intervention group (see Figure 2). Stimulant administration has been shown to increase P3 amplitudes,46–48 and in non- ADHD examinations of mindfulness, P3 amplitudes were shown to be larger in mindfulness groups,30,49 thus we hypothesized a treatment related amplitude increase. As mentioned above, the N2 is suggested as an index of attentional and alerting skills after mindfulness training, which may not necessarily be accompanied by performance improvement. 44 The lack of evidence for changes in P3 amplitude also aligns with previous studies indicating that the Nogo N2 may represent conflict detection and attentional allocation, while the Nogo P3 is more directly associated with inhibiting a motor response.24,26,27 Given we found no significant change in P3 activity accompanied by no difference in accuracy or reaction time, our findings are in line with the interpretation that the Nogo N2 is associated with cognitive control and attentional allocation, not necessarily active motor suppression. Furthermore, previous groups have found a high degree of functional overlap in medial frontal negativities, and suggest a unified function where medial frontal activation in different performance paradigms represents modulation of controlled attention.40,50 We suggest that the mindfulness related changes in the N2 seen here, and in previous work, 44 are related to shifts in these cognitive control processes rather than a direct marker of motor response inhibition.
While mindfulness practice may impact N2 amplitudes, the physical exercise component of MMA may also have contributed to the current findings. Yu et al 51 found that acute aerobic exercise produced larger N2 amplitudes in youth with ADHD who participated in moderate intensity aerobic exercise compared to a neutral video watching condition. These N2 changes also correlated with improved task performance. 51 Prior research has also shown that engaging in exercise has a positive influence on attention and ADHD symptoms. 52 Yu and colleagues 51 only assessed the acute effects of aerobic exercise on the N2 at 30- and 60-min post-treatment. Given that our data collection did not take place in the context of acute exercise, our results suggest that MMA may result in sustained impact on markers of cognitive control. Future research is needed that examines the independent and combined influence of mindfulness and martial arts (acute exercise and sustained impact of exercise) components of MMA on N2 amplitude to further our understanding of relative influence of treatment components and their acute or sustained nature.
Limitations and Future Directions
While this study adds to the literature in terms of increased understanding of the mechanisms by which mindfulness-based interventions may be efficacious for youth with ADHD, there are limitations that should be addressed in future studies. One limitation of this study is lack of control on medication. Much of the prior work which investigated mindfulness using EEG did so in typically developing populations where the effect of pharmacological treatment did not have to be considered. In many EEG studies for ADHD, participants are asked to abstain from medication the day of testing.46,51,53–55 Our study did not include such controls. As this study aimed to investigate the treatment effect of the MMA program, controlling medication administration may have reduced confounding influence on EEG measures that are known to be modulated by psychostimulants. 56
Another consideration when interpreting the results of the present study is the complexity of the sample. While our study investigated ADHD, many of the participants had comorbid diagnoses. It is common for individuals with ADHD to have comorbid diagnoses 2 and we did not find any pre - intervention relationships between comorbidities and outcome variables of interest. However, as noted in previous work on an MMA intervention, 34 larger samples are needed to gain the statistical power required to determine whether the type of comorbidity has an effect on neural indicators of response inhibition. To better isolate the specific neural activity associated with ADHD and mindfulness, one may wish to recruit a cohort which places more controls on comorbidities.
Finally, biological females were not well represented in our study population. Given well documented differences in frontal lobe development between sexes, 57 the fact that our sample was predominantly male may influence our results. Further study should seek to recruit more female participants with ADHD to better elucidate potential sex-based differences in medial frontal activity as indexed by the NoGo N2.
Conclusions
In conclusion this study suggests that mindfulness martial arts intervention buffers against reductions in neural indicators of cognitive control that are typical of ADHD. We found that control group N2 amplitudes were significantly reduced post-treatment while those who participated in MMA maintained a significantly higher level of neural response as indexed by N2 amplitude. This supports previous research suggesting MMA and other mindfulness-based interventions have positive effects on neural indices known to be clinically reduced in adolescents with ADHD.
Footnotes
Ethical Approval
This sub study was approved by the research ethics board at Mount Saint Vincent University and the parent study was approved by the research ethics board at Toronto Metropolitan University, thus both this sub study and the parent study comply with ethical standards of the 1964 Declaration of Helsinki and later amendments.
Informed Consent
Informed consent and child assent were obtained at all time points.
Funding
This work was partially funded by a research grant from the Scottish Rite Charitable Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available on request from the principal investigator, K.M. (karen.milligan@torontomu.ca). The data are not publicly available due to their containing information that could compromise the privacy of research participants.