
Abstract
Keywords
Anxiety disorders represent the most common mental health issue in the United States, 1 affecting 18.1% of adults. According to the anxiety and depression association of America (ADAA), this condition is especially prevalent in adolescents aged 11–18 years (31.8%). Mental health concerns in this demographic require diligent attention as the Children's Hospital Association documented 5485 emergency room or inpatient visits for suicidal thoughts and self-harm among 6- to-12-year-olds in 2019, up from 2555 in 2016. Anxiety can be a normal and adaptive response to a given stressor; however, when the anxiety, worry, or panic cause significant impairment to one's ability to function in daily life it is classified as an anxiety disorder. Specific categories or subtypes of anxiety disorders exist, including generalized anxiety disorder (GAD), panic disorder (PD), specific phobias, agoraphobia, social anxiety disorder (SAD), separation anxiety, and school avoidance. To optimize treatment programs for youth with anxiety disorders it will be advantageous to better understand how specific subtypes of anxiety relate to underlying neurophysiological characteristics. An overall enhanced classification of these subtypes could lead to more targeted and customized therapeutic approaches.
A common neurophysiological characteristic of anxiety disorder in both adults and children is the presence of greater right-than-left frontal brain activity or asymmetry, measured via resting-state electroencephalography (EEG).2,3 This has most commonly occurred through measurement of power in the alpha frequency (8–12 Hz) which is especially related to emotionality and has an inverse relationship with cortical activity (meaning decreased alpha power is reflective of increased engagement). 4 This has been illustrated in studies linking EEG with neuroimaging to show that as alpha increases, blood-oxygen-level-dependent (BOLD) response decreases in a given region.5,6 Therefore, the presence of right frontal alpha asymmetry reflects increased left brain activation, while increased left frontal alpha asymmetry signifies greater right brain activation. Previous findings have demonstrated that increased right-to-left frontal alpha is a mediator of underlying positive emotionality as well as approach-related behaviors, whereas increased left-to-right frontal alpha corresponds to negative emotionality and withdrawal-related behaviors. 4 Using this framework, 7 hypothesized that more left-to-right frontal alpha activity signifies a biological risk factor for the development of an anxiety disorder or other conditions marked by negative emotionality. Despite a consistent association with anxiety symptomology, this useful metric has seldom been explored in relation to specific components of child anxiety including panic, separation, school avoidance, and social. This is also true for other potentially informative resting-state EEG characteristics.
Wiedemann et al. 8 found that adult patients with PD displayed significantly enhanced left-to-right frontal alpha asymmetry both at rest and during anxiety-provoking exercises relative to the control condition (N = 25). The analyses yielded non-significant differences in parietal alpha asymmetry. Thoma et al. 9 replicated the finding of increased left-to-right frontal alpha asymmetry in 55 adults with PD compared to 42 control participants. Aspects of social anxiety have also been studied in relation to frontal alpha asymmetry both at rest and during stress-eliciting manipulations. Thus far, these investigations have yielded mixed results. Schmidt et al. 10 found enhanced left-to-right frontal alpha asymmetry in 26 adults with SAD at rest and during an impromptu speech situation. This metric also showed strong test-retest reliability at the 1-week follow-up. However, Beaton et al. 11 did not find differences in frontal alpha asymmetry between individuals with high levels of social anxiety and a control group with low levels, during the anticipation of a stress-inducing speech task. Harrewijn et al. 12 also found no group differences in frontal alpha asymmetry at rest, as well as during a stress-provoking situation between high social anxiety and low social anxiety (N = 33) participant groupings. Although research has not yet been applied to child samples, Campbell et al. 13 found that children of parents clinically diagnosed with social anxiety exhibited higher overall resting frontal EEG alpha activity compared to children of non-diagnosed parents.
In summary, left frontal alpha asymmetry has been found in adults with PD and in some instances social anxiety; however, this metric has not yet been examined in children and especially in relation to common childhood components of anxiety such as school avoidance and separation anxiety. Notably, there has not been a consensus regarding the ideal electrode placement for capturing differences in asymmetry as a function of anxiety disorders. Several studies have found associations with anxiety at mid-frontal sites (F3/F4) while others have identified meaningful group differences at lateral frontal locations (F7/F8).7–9 Additionally, some evidence suggests that different electrode placements will capture source activation from unique regions of the prefrontal cortex (PFC). For example, FP1 and FP2 correspond to the orbitofrontal cortex (decision making), while F3 and F4 align with the dorsolateral PFC (working memory), and F7 and F8 with the ventrolateral PFC (response inhibition).6,14 Therefore, it would be optimal to compare asymmetry across these different sites within the same study, especially considering the possibility that characteristics in one location may correlate more to one subtype of anxiety versus another. It is important to emphasize that despite some localization in the PFC there is still a high degree of overlap and co-activation between these regions. 14
Frontal alpha asymmetry has also been commonly associated with clinical depression and other depressive symptomology2,3,7; however, the utility of this marker requires further research as some null findings have occurred in the literature.15,16 Preliminary evidence has highlighted parietal alpha asymmetry as a useful measure for distinguishing the electrophysiological profiles of anxiety and depressive disorders. 2 found that individuals with high anxiety show enhanced right frontal and right parietal activity, while those with high levels of depression display enhanced right frontal but reduced right parietal activity. In accordance with this two-factor stress model, an anxious apprehension component is unique to depression (right frontal, left parietal asymmetry), while anxious arousal is more pertinent to anxiety disorders (right frontal, right parietal asymmetry).
Lastly, enhanced beta activity (13 to 30 Hz) in the right midline and posterior regions of the brain has also been associated with heightened anxiety in adults of all ages.17,18 Beta is considered to be a fast-frequency activity band and heightened levels in the temporal and parietal lobes (particularly in the right hemisphere) may signify toxic over activation of the sympathetic nervous system or fight-or-flight response. However, this measure has been examined in relation to mood disorders to a far lesser degree than alpha asymmetry. For these reasons, beta asymmetry was also included as a resting-state EEG measure in the current investigation.
The Use of EEG in Clinical Settings
Electroencephalogram measures are particularly advantageous for understanding neurological traits related to specific clinical symptoms in children as they are collected in a non-invasive manner and can be done so using machinery that is less noisy and financially costly than other neurological instruments. Many clinical psychiatric settings are now utilizing EEG, and there is evidence to support the utility of EEG measures for aiding in both the diagnosis and treatment selection process. For example, 19 utilized EEG measures to classify patients into major depressive disorder subtypes (frontal theta excess and frontal alpha excess). They found that the frontal alpha excess group was 87% responsive to antidepressant medications while the theta access group had 100% responsivity to stimulant medications.
Knott et al. 20 found that in 70 depressed patients treated with paroxetine, those with high delta and theta values at baseline yielded stronger response. Lastly, Bruder et al. 21 found that a group of 34 fluoxetine responders had enhanced left-to-right alpha asymmetry relative to a condition of 19 non-responders. The effects of neurofeedback, in which neuroanatomical sites are trained directly into specific frequencies of activation using operant conditioning mechanisms, are also enhanced when EEG is used to select protocols.22–24 suggested that a similar EEG-driven approach be applied to protocol selection in transcranial magnetic stimulation treatments.
Dimensional Approach and Current Study
An innovative positive psychology approach is to conceptualize psychiatric concerns on a dichotomous spectrum with well-being on one end, clinical diagnosis on the other, and with most individuals scoring somewhere in-between these extremes. 25 Approaching clinical psychology research with this strategy has the potential to eliminate the “all or nothing” approach of understanding and treating mental health disorders, theoretically alleviating common stigmatization. Additionally, this approach will place a greater emphasis on overall mental health management versus the common misconception that only individuals with clinical diagnoses should practice sound, evidence-based strategies for mental health management. In recent years, several research studies have highlighted the utility of operationalizing psychiatric concerns using a dimensional or transdiagnostic approach.26,27 Using this strategy, 28 found that non-diagnosed individuals with high levels of panic (anxious arousal) displayed heightened levels of right parietal activity relative to left during an emotional narrative task; however, those with high levels of worry (anxious apprehension) had more left activity than right. An analogous result occurred in Refs. 29 and 30, which collectively found that high levels of anxious apprehension related more to increased right frontal asymmetry in frontal and central cites compared to high levels of anxious arousal. The use of a dimensional approach in the classification of childhood anxiety could potentially reduce the rate of unrecognized cases, and thus allow more individuals access to effective treatments.
In the current study, the primary aim was to examine the association between specific aspects of childhood anxiety (general, panic, social, school, and separation) and various EEG measures in order to facilitate a better understanding of these unique neurophysiological profiles. It was expected that right frontal and parietal (alpha and beta asymmetry) would be related to general, panic, and social forms of anxiety based on previous findings in the literature. Exploratory findings were examined for school and separation components of anxiety which had not yet been studied in relation to neurophysiological measures.
Method
Participants
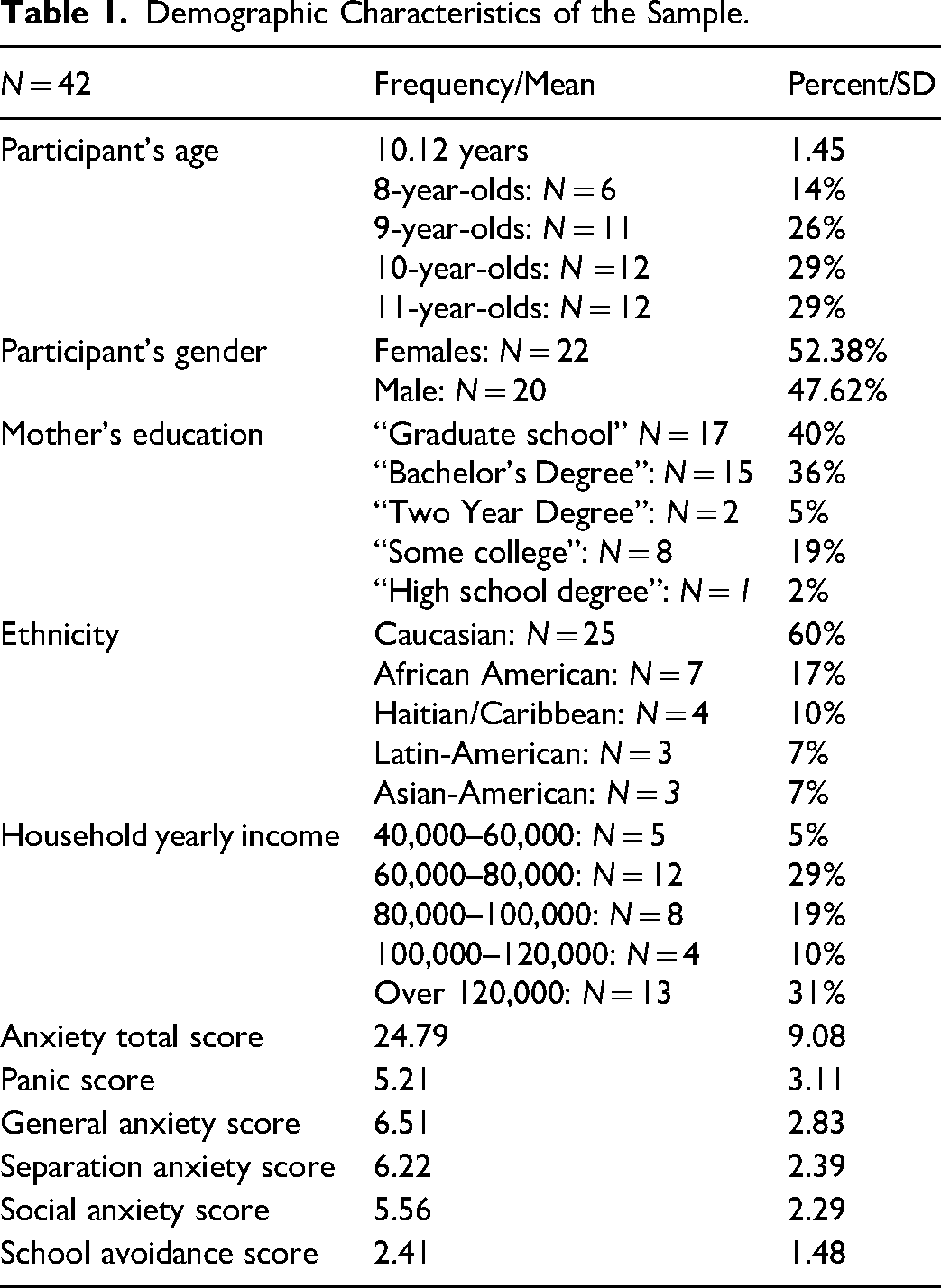
The participants consisted of 42, 8–12-year-olds (22 females and 20 males) with an average age of 10.12 years (SD = 1.25). All participants were sampled from fourth, fifth, and sixth-grade classrooms in various schools near a South Florida university. Children who had received a diagnosis of developmental disorder, learning disability, or neurological condition were not included in the final analysis. A complete summary of the demographic information can be found in Table 1. To determine the appropriate sample size for detecting significant effects in the regression analyses, the G*Power software version 3.1 31 was used a priori; the parameters were set with a power level of .80, alpha at .05, and an eta squared of .14. 32 The selected effect size was also guided by prior results on this topic which found eta squared values between .02 and .20.3,15,16 This was also used according to this analysis, the minimum recommended sample size to detect significant effects in the regression models was 29 participants. All participants were treated in line with the ethical principles of the APA, and there was no risk of harm greater than in normal classroom activities. Data from this sample was also used in Ref. 33, which included analyses on the effectiveness of a computerized training software for emotional executive functioning skills. Thus, all participants received access to this software (gFocus from IQ Mindware, which is normally a $10-20 value).
Demographic Characteristics of the Sample.
Procedure
All participants were accompanied by their mother for the study session. First, a parental consent and child assent was completed and then the participant's mother was given a demographic form capturing information related to age, ethnicity, and socio-economic status (SES). Next, the child participant completed the Screen for Child Anxiety Related Disorders (SCARED) instrument. Resting-state EEG was then recorded for 6 min in total for all child participants. Participants were instructed to remain still and keep their eyes open during the recording, while parents and research assistants were encouraged to remain still and quiet. Further elaboration of the procedure is outlined in Ref. 33.
Measures
SCARED Instrument
The SCARED is a 41-item inventory rated on a 3-point (0–2) scale that can be completed by a child or parent rater. 34 The purpose of the instrument is to screen for signs of anxiety disorders and symptomology in children. In this study, these forms were administered in-person by a trained member of the research team. For both the child and parent versions, the total score and the five-factor scores (panic/somatic, generalized anxiety, separation anxiety, social phobia, and school phobia) have demonstrated good internal consistency (a = .74–.93), test–retest reliability (intraclass correlation coefficients (a = .70–.90), and moderate parent–child agreement (r = .20–.47). 35 Higher scores are indicative of increased anxiety levels, and a total score of 25 or higher may indicate the presence of an anxiety disorder. In this sample, the parent–child agreement across items was moderately strong (r = .216–.626, p < .001) however, only the child reported scores were used for analysis. A total score of greater than or equal to 25 may indicate the overall presence of an anxiety disorder. The panic/somatic component is comprised of the average score across items 1, 6, 9, 12, 15, 18, 19, 22, 24, 27, 30, 34, and 38; an overall score of 7 may indicate the presence of a PD. The generalized anxiety sub-score is calculated by averaging items 5, 7, 14, 21, 23, 28, 33, 35, and 37 with an overall score of nine potentially indicating the presence of GAD. Separation anxiety is comprised of the average of items 4, 8, 13, 16, 20, 25, 29, and 31; a score of 5 may indicate the presence of separation anxiety disorder. Social anxiety is captured using the average of items 3, 10, 26, 32, 39, 40, and 41 (a score of 8 represents the potential for SAD). Lastly, the average of items 2, 11, 17, and 36 are used to capture school avoidance with a score of three signifying the possibility of significant school avoidance.
EEG Measures and Data Reduction
EEG was recorded for 6 min from pre-frontal (FP1, FP2), mid-frontal (F3, F4), lateral frontal (F7, F8) as well as parietal (P3, P4) leads which were referenced to the vertex (Cz). Prior to the positioning of the stretch lycra caps (manufactured by Electro-Cap, Inc.) head circumference was measured in centimeters, in order to fit the ideal cap size. Once positioned, Omni prep gel and electrode gel were inserted into each site in order to gently abrade and provide good conductance. Impedances were checked and deemed acceptable if they were less than 5 K ohms. Eyes open data was collected and analyzed, and therefore the participant's mother and research team were instructed to remain quiet during the procedure. The EEG signals were amplified using Grass Model 12 Neurodata Acquisition System amplifiers with filters set at 1 Hz high pass and 100 Hz low pass as well as a gain of 20,000, with 60 Hz notch filter on. Prior to data collection, the signal for each channel was calibrated using a 10 Hz sine wave. The analog output from the amplifiers was then digitized at a sampling rate of 512 Hz and digitized using 12-bit conversion (Analog Devices RTI-815 A/D board). The data were streamed to a computer screen and saved to a hard disk using data acquisition software (Snapstream, v. 3.21, HEM Data Corp. 1991).
The data were cleaned using the Artifact Subspace Reconstruction feature of the EEGlab toolbox in Matlab, which utilizes principle component analysis (PCA) to reject continuous data that is outside of five standard deviations of the cleanest point of data. The data were then submitted to a discrete Fourier transform using a 2-s Hanning Window with 50% overlap via the Matlab signal processing toolbox software (Mathworks). Subsequently, the data were segmented into alpha (8 to 12 Hz) and beta (13 to 30 Hz) frequency bins. For each participant, these analyses produced average power density values for the recorded regions of interest in each distinct frequency bin. In the current data set, the power values were skewed and leptokurtic; therefore, the natural logarithms of the absolute power values for data analysis. EEG asymmetry scores were calculated by subtracting the natural log transformed left hemispheric power value from the natural log transformed right hemispheric power value for the given site (i.e. (Ln(F4) – Ln(F3) for mid-frontal). Due to the inverse relation of alpha and beta power to activity, negative asymmetry scores reflected greater right than left activity, and positive scores reflected greater left than right EEG activity.
Data Analysis
A series of hierarchical linear regression models were conducted to examine the association between EEG measures of interest (prefrontal asymmetry, mid frontal asymmetry, lateral frontal asymmetry, and parietal asymmetry) and child anxiety subtypes (general, panic, separation, social, and school avoidance). In total, five models were generated to examine this association in two different frequencies of activation (alpha and beta), equaling 10 models in total. In each model, age was controlled for in step 1 and the four EEG measures of interest were entered as predictors in step 2, while the anxiety subtype score was entered as the outcome variable. To analyze the single effects of each EEG location of interest within each model, a Bonferroni correction was applied (.05/5 = .01).
For each significant association, follow-up independent samples t-tests were conducted to determine if significant differences in electrophysiology were present for participants meeting clinical criteria for a given anxiety condition versus those who did not.
Results
Alpha Frequency Band Regressions
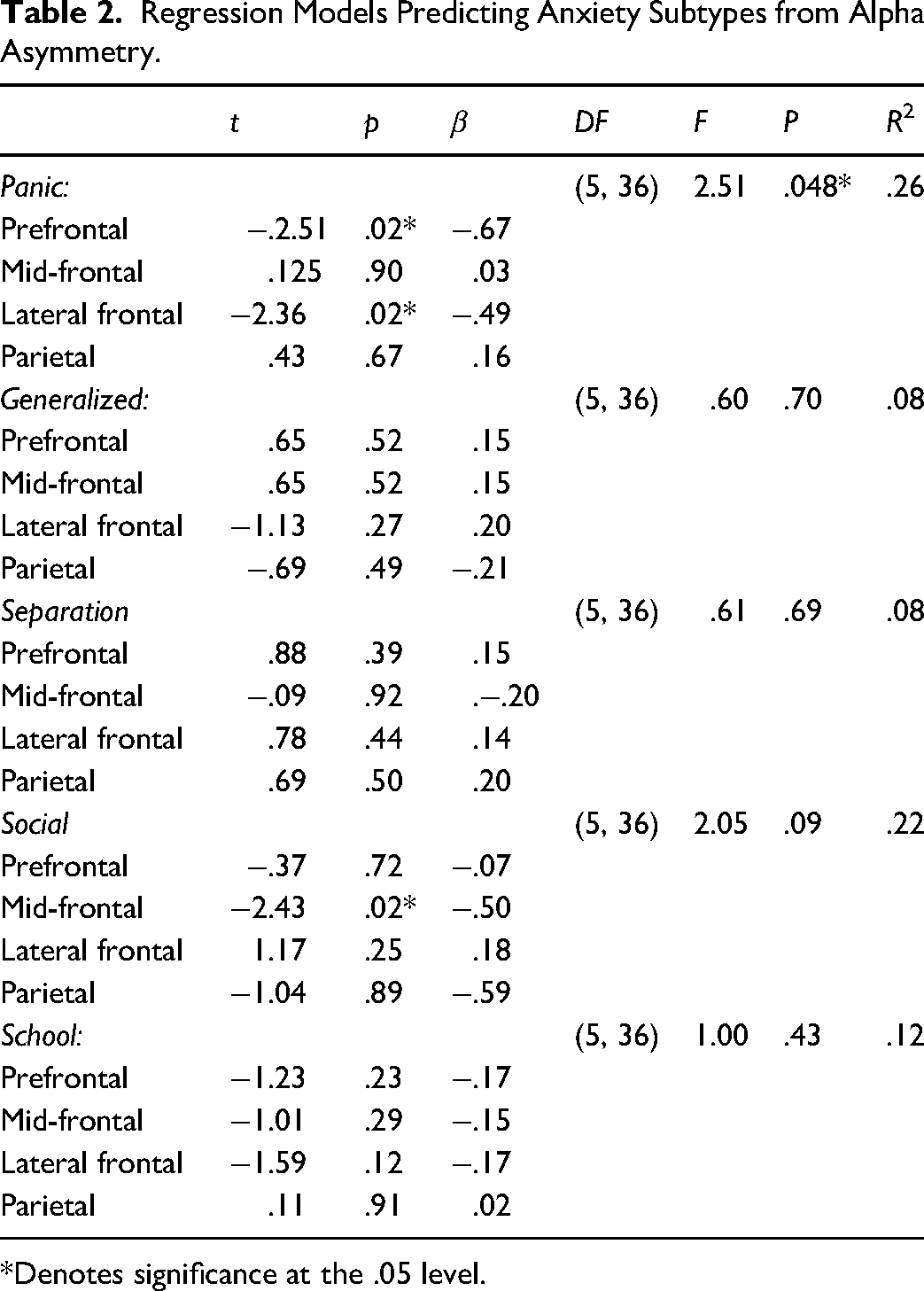
The model predicting panic from alpha EEG asymmetry measures was significant at step 2 (F(5, 36) = 2.51, p = .048, R2 = .26), and both prefrontal asymmetry β = −.67, t(41) = −2.51, p = .02 and lateral frontal asymmetry β = −.49, t(41) = −2.36, p = .02 were significant predictors prior to Bonferroni correction. The model predicting generalized anxiety was non-significant F(5, 36) = .60, p = .70, R2 = .08 as was the model predicting separation anxiety F(5, 36) = .61, p = .69, R2 = .08, with no significant individual predictors. Regarding social anxiety, the model was moderately significant at step 2, (F(3, 38) = 2.05, p = .09, R2 = .22) and mid-frontal alpha asymmetry emerged as a significant predictor, β = −.50, t(41) = −2.43, p = .02 (prior to Bonferroni correction). Lastly, the model predicting school avoidance was non-significant, F(5, 36) = 1.00, p = .43, R2 = .12. The entire set of alpha regression models is summarized in Table 2.
Regression Models Predicting Anxiety Subtypes from Alpha Asymmetry.
*Denotes significance at the .05 level.
Beta Frequency Band Regression Models
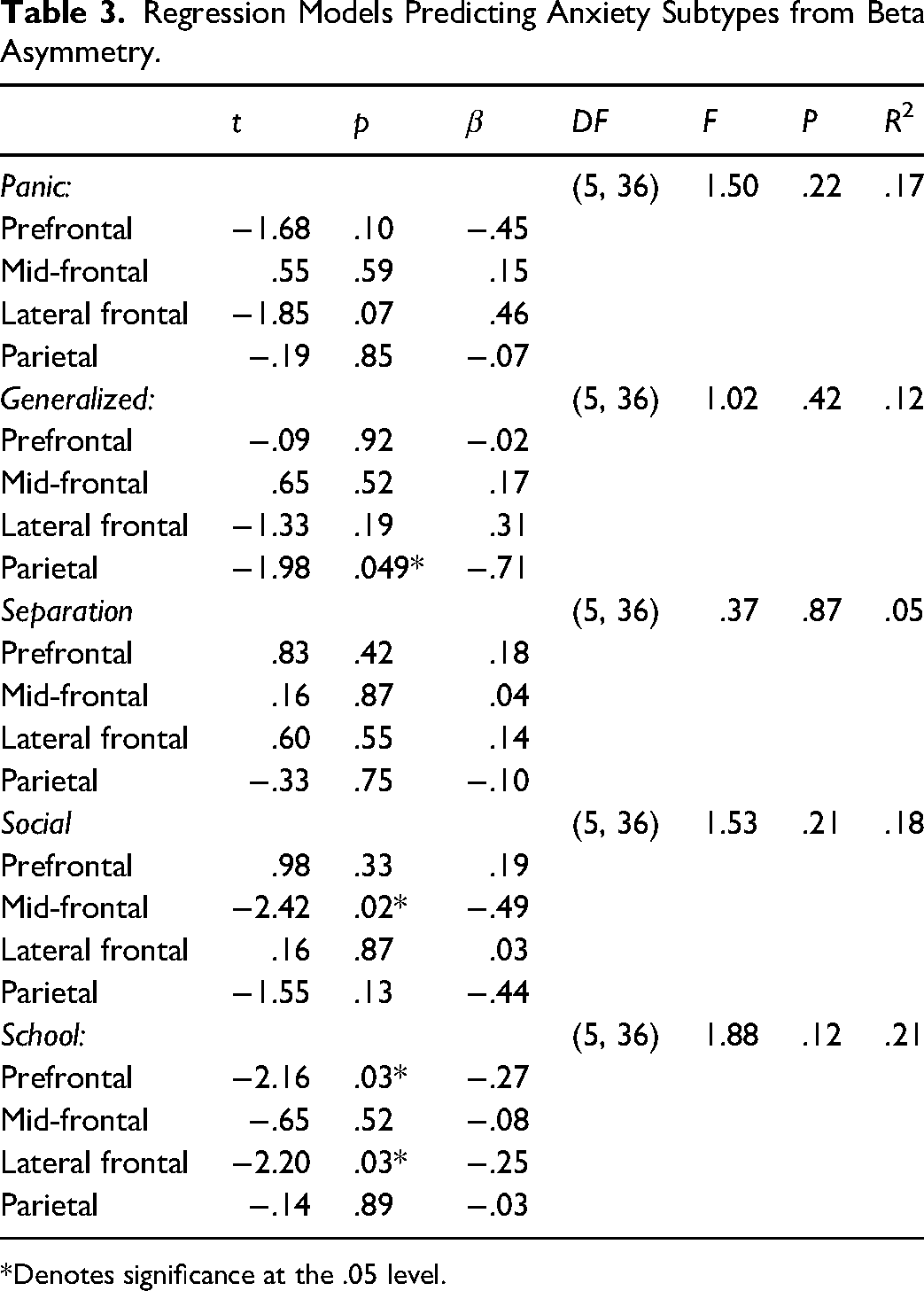
The model predicting panic from beta EEG asymmetry measures was non-significant F(5, 36) = −1.50, p = .22, R2 = .17 with no significant individual predictors. The model predicting generalized anxiety was also non-significant F(5, 36) = 1.02, p = .42, R2 = .12, however parietal beta asymmetry was a significant predictor β = −.71, t(41) = −1.98, p = .049 prior to Bonferroni correction. The model predicting separation anxiety from EEG asymmetry measures was non-significant F(3, 38) = .37, p = .87, R2 = .05, and no significant individual predictors emerged. The model predicting social anxiety was non-significant, F(3, 38) = 1.53, p = .21, R2 = .18; but notably, mid-frontal alpha power was a significant predictor β = −.49, t(41) = −2.42, p = .02 of this anxiety subtype. Lastly, the model predicting school avoidance was non-significant F(3, 38) = 1.88, p = .121, R2 = .21, however prefrontal beta asymmetry β = −.27, t(41) = −2.16, p = .03 and lateral frontal beta asymmetry β = −.25, t(41) = −2.20, p = .03 emerged as significant predictors prior to Bonferroni correction. The beta asymmetry regression models can be viewed in Table 3.
Regression Models Predicting Anxiety Subtypes from Beta Asymmetry.
*Denotes significance at the .05 level.
T-Tests Examining Clinical Levels of Symptoms
Panic Disorder
The independent-samples t-test examining differences in prefrontal alpha asymmetry between those meeting clinical criteria for PD (N = 9) and those who did not (N = 33) was nearing significance, t(41) = −1.92, p = .06, d = .72. However, the test assessing differences in lateral frontal alpha asymmetry t(41) = −.59, p = .56, d = .22 yielded no significance. Increased right frontal asymmetry was present in those meeting criteria for PD.
Generalized Anxiety
The independent-samples t-test assessing differences in parietal beta asymmetry between those meeting clinical criteria for GAD (N = 9) and those who did not (N = 33) was non-significant, t(40) = −.1.30, p = .20, d = .49. Increased right frontal asymmetry was still present in those meeting criteria for GAD.
Social Anxiety
The independent-samples t-test examining differences in mid-frontal alpha asymmetry between those meeting clinical criteria for SAD (N = 4) and those who did not (N = 38) was significant, t(40) = −2.31, p = .00, d = 1.61. Additionally, the test analyzing mid-frontal beta asymmetry between groups was also significant, t(40) = .−3.47, p = .00, d = 1.28. In both cases, increased right frontal asymmetry was present in those meeting criterial for SAD.
School Avoidance
The independent-samples t-test examining differences in lateral frontal beta asymmetry between those meeting threshold for school avoidance disorder (N = 15) and those who did not (N = 27) was significant, t(40) = −2.10, p = .04, d = 2.08. However, the test analyzing pre-frontal beta asymmetry between groups did not reveal significance, t(40) = −1.14, p = .26, d = 1.87. In both cases, increased right frontal asymmetry was present in those meeting criteria for school avoidance
Discussion
In the current study, the association between electrophysiological asymmetry measures and child anxiety subtypes was examined. Specifically, alpha and beta asymmetry values in prefrontal, lateral frontal, mid-frontal, and parietal regions were studied in relation to panic, general anxiety, social anxiety, separation anxiety, and school avoidance. Notably, panic trait levels were found to be significantly related to prefrontal and lateral frontal alpha asymmetry. General anxiety scores were predicted by parietal beta asymmetry measures while social anxiety levels were associated with both mid-frontal alpha and beta asymmetry. Lastly, school avoidance was significantly correlated with prefrontal and lateral frontal beta asymmetry scores. In all cases, negative correlations were identified suggesting that increased anxiety subtype scores related to a rightward shift in asymmetry. No significant findings were detected relating to separation anxiety which is considered unique to childhood anxiety.
This study provided preliminary evidence that right frontal asymmetry in frontal and parietal regions (a common marker of adult anxiety) should also be considered a marker signifying risk for elements of childhood anxiety.2,5 Greater right frontal alpha asymmetry was previously implicated in general anxiety and panic symptoms in adults,8,9 with more mixed evidence of an association with social anxiety traits. 10 Here, EEG asymmetry measures were examined in relation to specific subtypes of anxiety to allow better understanding of the neurophysiological mechanisms involved in each. Evidence emerged to support unique profiles of panic, general anxiety, social anxiety, and separation anxiety symptoms.
Right prefrontal and lateral frontal alpha asymmetry were most predictive of panic symptoms in this study. Wiedemann et al. 8 found right frontal alpha asymmetry at mid-frontal sites (F4 – F3) in relation to panic symptoms, while Thoma et al. 9 found the association in lateral frontal leads (F8 – F7). The findings of the current study are consistent with the later and also suggest that prefrontal alpha asymmetry may be uniquely related to child panic symptoms. The prefrontal and lateral frontal areas are strongly implicated in cognitive control, emotional reactivity, and interpretation of threats. 36 Therefore, it is unsurprising that the heightened physiological arousal and perception of fear associated with panic would be related to overactivity in the right hemisphere of these regions, which is more involved with emotion-guided response while the left side mediates top-down cognitive control. 37
Parietal beta asymmetry was the strongest predictor of generalized anxiety. Interestingly, frontal asymmetry had also been consistently found in relation to general anxiety traits in prior adult studies 30 ; however,28,29 found right parietal alpha asymmetry to be a notable marker of anxious arousal (anxiety) rather than anxious apprehension (anxiety + depression). To follow up on the possibility of right parietal asymmetry as a unique marker of childhood generalized anxiety, we examined a model predicting depressive symptoms from parietal beta asymmetry; this model was non-significant, p = 55. The parietal lobe is heavily involved in sensation and perception of the environment and overactivity in this anatomical location can lead to heightened perception of environmental cues, and thus anxiety. 37
Increased mid-frontal alpha and beta asymmetry in the right hemisphere predicted higher levels of social anxiety in this study. This is unsurprising as the medial frontal cortex has long been implicated in social cognition. 38 Further, the medial frontal cortex has shown to play a fundamental role in key social abilities in childhood such as self-reflection, person perception, and theory of mind. References 38 and 10 found group differences in mid-frontal alpha asymmetry between a group of participants with clinically diagnosed social anxiety versus those who did not. However, other studies on adults with social anxiety have yielded null results. Beaton et al. 11 examined mid-frontal asymmetry as a function of social anxiety in a non-clinically diagnosed sample and found no significant results. Harrewijn et al. 12 also found a non-significant association between mid-frontal alpha asymmetry and social anxiety when dividing participants into high and low socially anxious groups. Notably, mid-frontal asymmetry was calculated differently in this study (F4 + F6) – (F5 + F3). 12 It is possible that some of the inconsistencies in the adult literature are related to similar methodological concerns or that the correlation is stronger throughout earlier stages of life.
Additionally, school avoidance was uniquely related to right prefrontal and lateral frontal beta asymmetry patterns in this study. This specific trait had not yet been examined in relation to specific neurophysiological patterns. Despite being an under-researched condition, school avoidance is found in as many as 5% of children in the United States. 39 Determining the specific neurophysiological and cognitive underpinnings of the condition could prove highly valuable in tracking intervention-related progress over time. Prefrontal and lateral frontal asymmetry were also related to panic symptoms in this study in the alpha bandwidth. This is unsurprising as panic levels and school avoidance are highly co-occurring conditions. 39 Still, this finding highlighted the advantage of also exploring childhood EEG characteristics in the beta frequency. Prior studies in the adult literature had found some noteworthy findings in this frequency, but it has been studied to a lesser degree than alpha asymmetry. 18
Only two significant findings occurred when the data was reanalyzed by segmenting participants into two groups (meeting threshold for clinical diagnosis and not meeting criteria) and examining group differences in EEG characteristics. Those meeting criteria for social anxiety diagnosis scored significantly higher on right mid-frontal alpha asymmetry compared to those not meeting criteria. Additionally, those meeting diagnosis criteria for school avoidance disorder had higher right lateral frontal beta asymmetry compared to those not meeting criteria. The dimensional approach was advantageous here given that a formal diagnosis is less common for children in the age bracket of this study; however, it is still very common for children of this age to experience heightened anxiety coinciding with the rapid social development and increased degree of stress that presents with this age.
Limitations and Future Directions
A key limitation of this study was the relatively small sample size (N = 42) considering the large number of models that were analyzed to capture the five subtypes of anxiety. Additionally, it would have been advantageous to also include the Beck Anxiety Inventory or other scales that have traditionally been used with adult participants. This would have allowed a comparative analysis to determine the possibility that the SCARED inventory is more sensitive to capturing anxiety symptoms than inventories previously used in studies on this topic. Additionally, the school avoidance portion of the SCARED only contains four items so the addition of the School Refusal Assessment Scale would be highly valuable for further studying this subtype. Another potential limitation of this study was the use of the Cz (vertex) reference scheme when analyzing the EEG data. Although studies utilizing this reference point have yielded some of the largest effect sizes in the literature, 40 some recent work suggests that current source density (CSD) transformation may enable a more reliable measurement of individual variations in frontal asymmetry and mitigate interference from other electrical sources. 41
Further, the subscales of the SCARED Inventory were moderately and significantly correlated with one another (r's spanning from .51 to .64). This makes it more difficult to identify specific EEG biomarkers for each subtype with a high degree of confidence. Future investigations should explore administering separate scales to capture the subtypes of anxiety that have a lower degree of correlation. Lastly, none of the p-values passed the criteria for multiple testing correction and thus, the results of this study should be interpreted with caution. However, they do illustrate a proof of concept that should be extended to a large-sample investigation. Each of these limitations should be ameliorated in future studies looking to replicate or expand upon these findings. The possibility of matching clinical symptoms with EEG characteristics should continue to be explored in younger samples and should also be studied as a function of various intervention approaches. This can aid in the determination of the ideal therapeutic or medication approaches for treating specific aspects of clinical conditions. EEG-guided therapy could be particularly advantageous in the realm of cutting-edge treatment approaches such as transcranial magnetic stimulation (TMS). In TMS, the delivery of excitatory or inhibitory electromagnetic stimulation to specific regions of the brain (e.g., medial or lateral PFC) is possible.
In this study, preliminary evidence showed that several aspects of childhood anxiety (panic, general, and social) relate to unique electrophysiological profiles. Heightened panic symptoms were predicted by increased right lateral frontal asymmetry, while higher generalized anxiety was predicted by increased right parietal asymmetry and boosted social anxiety related to higher levels of right mid-frontal asymmetry. Some preliminary evidence occurred to support prefrontal beta asymmetry as a marker for school avoidance tendencies. EEG measures have promising potential for not only gaining a better understanding of the neurological mechanisms involved in specific clinical symptoms but also for fine-tuning and customizing treatment approaches that may be more impactful on one neuroanatomical location versus another.
Footnotes
Author Contributions
Nathaniel A. Shanok wrote the initial study proposal, collected and analyzed data, and assisted in the writing and editing of the manuscript. Nancy A. Jones assisted with the initial study proposal, provided guidance and oversight on data analysis, and assisted in the writing of the manuscript.
Statement of Ethics
This study protocol was reviewed and approved by [Florida Atlantic University IRB Office], approval number [1251543-6].
Consent to Participant Statement
Written informed consent was obtained by the child participants as well as their guardian.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.