
Abstract
A fundamental component of any military medical support system is medical evacuation. The main goal of evacuation is to reduce mortality among critically injured combat casualties. To achieve this goal, several decision problems including, the location of medical treatment facilities, relocation, dispatching, and routing have to be effective across all levels (tactical, operational, and strategic). This study concentrates on the three key types of medical evacuation (MEDEVAC) systems—forward, tactical, and strategic—and the related decision problems. Even though, over the last few years, some review papers have discussed the different topics of MEDEVAC systems (e.g., the evolution of MEDEVAC, evacuation timelines, and types of injuries), no research has been conducted on the full range (i.e., total care pathway) of MEDEVAC systems and the adoption of emerging technologies to improve future MEDEVAC. In this paper, a systematic review of the literature is described, including the decision problems involved in the total military medical evacuation process. This paper also reviews forecast challenges of future MEDEVAC and potential emerging technologies, concepts, and advanced decision-analysis methods to tackle these challenges. In future MEDEVAC processes, emerging technologies and concepts will be important to support improved medical capability; however, military planners will also need to adopt advanced decision-support techniques to efficiently employ these technologies.
Keywords
1. Introduction
Evacuating the wounded from the battlefield has been a persistent problem since the dawn of warfare, and it remains the same as today. 1 The movement of casualties is a significant part of military medical health systems. The military medical evacuation (MME) system is an intricate network of interconnected systems provides a range of medical treatments from the point of injury (POI) to healthcare facilities in the home country or another secure place outside of the joint operations area. 2 The medical evacuation (MEDEVAC) network establishes the crucial connections between the numerous care responsibilities required to keep the patient alive throughout transportation. In MME, emergency medical treatment and en route medical care are delivered in accordance with medical needs to improve the patient’s prognosis and decrease long-term impairments. 2 It is essential for preserving the lives of battle casualties and minimizing mortality and morbidity rates.
According to a US Army Techniques Publication, 2 there are two types of MEDEVAC support: (1) direct support and (2) area support. In direct support, an MEDEVAC unit provides dedicated support to a specific operational force, responding immediately to the supported force’s requests for assistance regardless of their geographical location. 3 In area support, the supplies, treatment services, and human services support any operational units requiring assistance within a specific geographical area; units located in or operating through their assigned zones receive help from logistical and healthcare support units (ground support units). 4
In MME, many decision problems are involved, and they are connected. Decisions in one phase can affect decisions in subsequent phases of the evacuation system. Therefore, to manage a successful evacuation, effective problem-solving techniques should be developed to enable precise dispatching procedures and most importantly timely responses. 5 Consequently, multiple decision-making methods that can address underlying uncertainty and minimize risk responsively are necessary for the MME system to support decision-makers to make optimal decisions. 6
The MME system/enterprise is complex. Safe and quick evacuation of combat casualties to an appropriate level of care facilities is the key concern of any emergency MEDEVAC. However, with only limited resources during combat operations, the most effective emerging technologies must be selected for acquisition, and they must be utilized efficiently in operations.
The global security environment is changing rapidly, and the military health system will need to deal with significant future challenges. In this regard, emerging technologies and related concepts can improve medical care delivery on the future battlefield. They can also support medical decision-making on the battlefield. 7 Advanced technologies have the capability to not only increase the responsiveness of care but also decrease fatalities caused by MEDEVAC accidents or operational complications due to severe weather and difficult terrain. 8 According to Lacdan 9 and Vella, 10 state-of-the-art technologies could streamline medical treatment and improve the performance of the evacuation system on the battlefield. For example, since the era of the Vietnam War, medics have had to manually perform rudimentary tasks such as measuring patients’ weight and calculating the amount of medication, that often slow down treatment. 9 With the help of emerging technology, medics should be able to have increased focus on patient care rather than spending time on basic tasks. In addition, advanced decision-making methods/techniques should allow planners and defense leaders to identify the capability of the MME system as well as assess the situation and the evacuation procedures’ time response.
Over the last few years, a small number of review papers have been published on MME systems. Some studies have discussed the evolution of military evacuation systems. 11 Other review papers focused on timelines 12 for a specific war or battlefield. However, no literature review has been conducted to bring a holistic view of the decision problems (e.g., resource allocation-relocation, dispatching and capability assessment) involved in the total care pathway of MME systems. The goal of this review article is to close this gap; i.e., the absence of reviews focused on MEDEVAC decision science (analysis and support). In addition, a number of research13–15 publications have discussed the applications of emerging trends and technologies in military operations. However, to the authors’ knowledge, the existing literature has not focused significantly on holistic analysis of emerging technologies, emerging concepts, and advanced decision-making techniques that can support emergency MME to deal with future challenges.
The paper’s primary contribution is to bring a decision science perspective and present a systematic literature review of the MME system from POI or casualty collection point (CCP) to post-hospital care, investigating each phase of the MME system. This study reviews the research work on the major decision problems that are involved in the total pathway of the evacuation system. This study pinpoints the possible future directions in this field and will be beneficial for those engaged in planning for the future development of the MME system.
The remaining sections are arranged as follows: Section 2 presents necessary concepts and definitions of MME; section 3 provides the research questions (RQs); the methodology to perform the systematic review is explained in section 4; section 5 describes the main results for each of the RQs; and, finally, the discussion of the systematic literature review findings and the conclusions are presented in section 6.
2. Concepts and definitions
MEDEVAC is generally a medical service for emergencies. Dynamic conditions, service quality, and travel times characterize the way the system operates in an unpredictable environment. 16 Providing proper care at an adequate service level within a short period of time makes this service challenging. Civilian healthcare has been advancing over time; however, since the American Civil War, the army’s philosophy for combat treatment has essentially not changed. 17 This section describes the subordinate MME concepts and definitions.
2.1. MME
Integrated health services are supported by the military medical system to expeditiously diagnose, treat, transport, and restore the patient/injured to duty. Pre-hospital care and MEDEVAC must be well-organized for effective medical support system in combat operations. 18
Generally, to evacuate battlefield casualties, there are two primary systems in place: (1) MEDEVAC and (2) casualty evacuation (CASEVAC);2,19 both systems seek to rapidly evacuate casualties from POIs or CCPs to medical treatment facilities (MTFs). MEDEVAC is carried out employing specialized medically prepared and standardized MEDEVAC platforms, designed specifically for the MEDEVAC task. In MEDEVAC, en route care of the wounded is provided by skilled medical experts. On the contrary, in CASEVAC, the transport of wounded personnel onboard non-medical vehicles or helicopters/airplanes and there may not en route care facilities.
2.2. Categories of MEDEVAC
According to North Atlantic Treaty Organization (NATO), there are three main categories of MEDEVAC, forward, tactical, and strategic: 20
Forward MEDEVAC. In forward MEDEVAC, the patient is transported as soon as feasible from the site of injury to the most appropriate care facilities, not necessarily the nearest facility. During forward MEDEVAC, it is of paramount importance that a casualty is provided appropriate care according to the 10-1-2 Timeline, a set of predetermined clinical time frames (i.e., bleeding control within 10 min, advanced resuscitative care within 1 h, and damage control surgery within 2 h).20,21
Tactical MEDEVAC. Tactical MEDEVAC concerns the transport of patients between different MTFs, generally, care levels increase from lower to greater. This evacuation happens within a Joint Operational Area.
Strategic MEDEVAC. Strategic MEDEVAC is the movement of ill or wounded personnel from the Joint Operational Area to a facility in their own country or to another safe location outside the theater. Treatment is a shared responsibility between the Force Commander and the contributing nations.
Figure 1 shows the MME system.
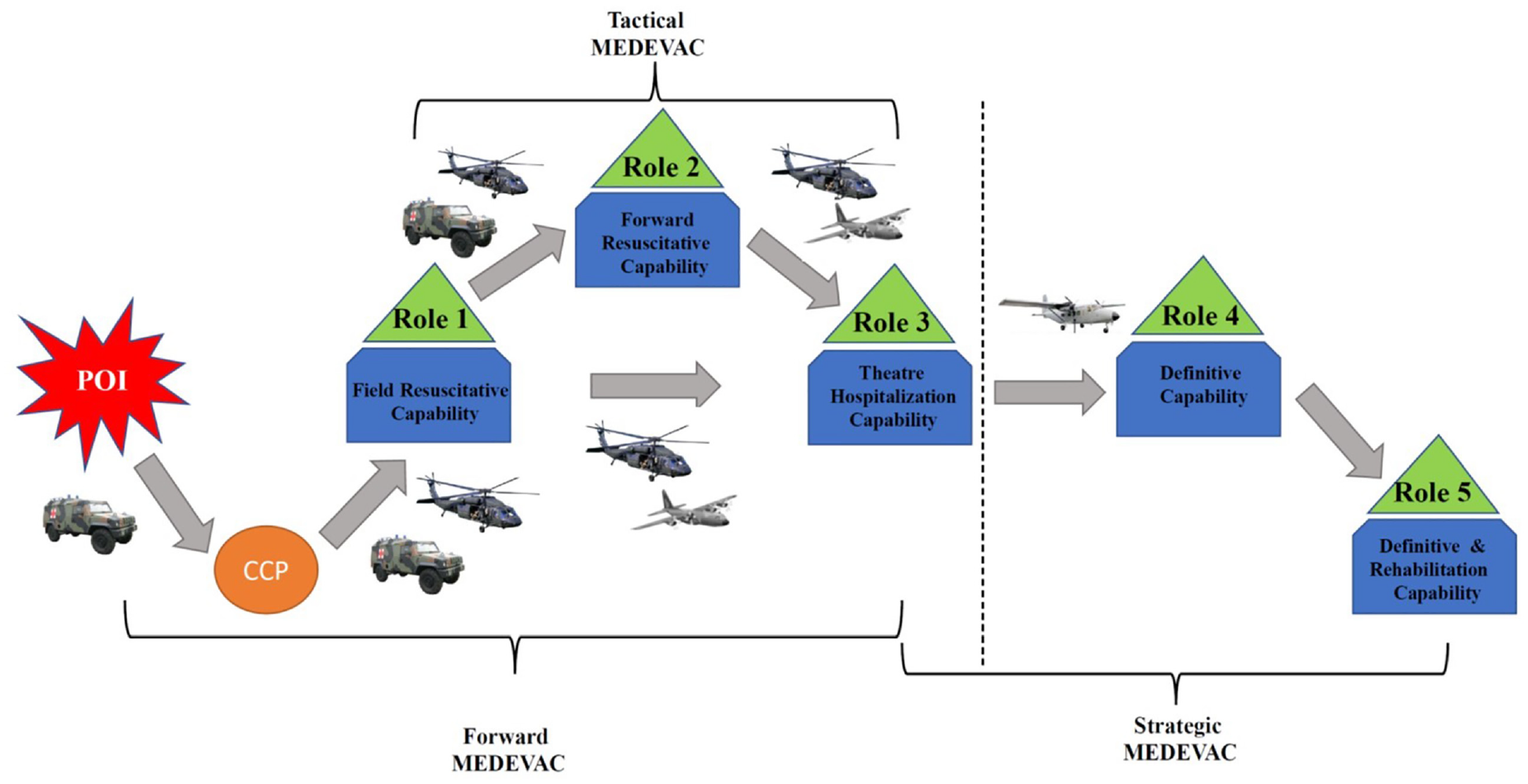
Military medical evacuation system.
2.3. The definitions of role of medical care facility as defined by NATO
Role 1 MTF—providing primary healthcare, specialist first aid, triage, resuscitation, and stabilization are the main responsibilities of a Role 1 MTF, which is a national obligation.
Role 2 MTF—a Role 2 MTF is distinguished from Role 1 facilities by its capacity for surgical interventions in addition to receiving and triaging casualties, as well as providing higher-level resuscitation and treating shock. The two primary categories of Role 2 MTFs are: (1) Role 2 Basic MTF and (2) Role 2 Enhanced MTF.
Role 3 MTF—secondary healthcare is generally provided in Role 3 MTF at the theater level.
Role 4 MTF—the complete range of definitive medical treatment which cannot be delivered to the operating theater, or would take too long to complete, is provided by a Role 4 MTF.
Role 5 MTF—the final phase of evacuation is Role 5 MFT. When receiving care at this stage, the patient is sent to an MTF close to their place of residence that is equipped to treat their specific wounds. 22 Definitive stabilization, reconstruction, or amputation and rehabilitative care facilities for extreme level casualties are performed at Role 5 MTF.
The sequencing of this movement depends on the goal, the adversary, the specific battle conditions, the climate, the support available, the amount of time, and civil considerations. Casualties are evacuated laterally from the POI or from one role to other role. 2 Well-established communication channels, command protocols, and well-equipped, capable MTFs can enable effective, premeditated evacuation from one sequential duty to the next higher position in a combat zone that is continuous. To ensure that all wounded receive the best care possible, the appropriate level of command must prepare an evacuation plan in cooperation with the command’s surgeon. 2
3. ReRQs
Systematic Literature Review (SLR) is a technique for analyzing the literature that finds, picks, assesses, and summarizes data regarding research questions, areas of concern, or a specific occurrence. 23
In this paper, three main research questions (RQs) and their subquestions are investigated that encompass solution methods, application of different decision problems concerned in the total military evacuation pathway, the possibility of the application of emerging technologies, concepts, and advanced techniques that support planners and defense leaders in decision-making in the military domain. The RQs considered in this literature review are shown in Table 1. These RQs are designed to inform the future research directions in MME. Defense leaders or planners could find the literature review related to RQ1 and RQ2 very effective, particularly in decision analysis/making during MME planning and development. The analysis based on the RQ3 could be beneficial for those who are looking to apply emerging knowledge (including on technology, concepts, and advanced decision-analysis techniques) in improving the operational and strategic outcomes of MME to prepare for the care of battle casualties in the future.
The research questions that are used to guide the systematic literature review.
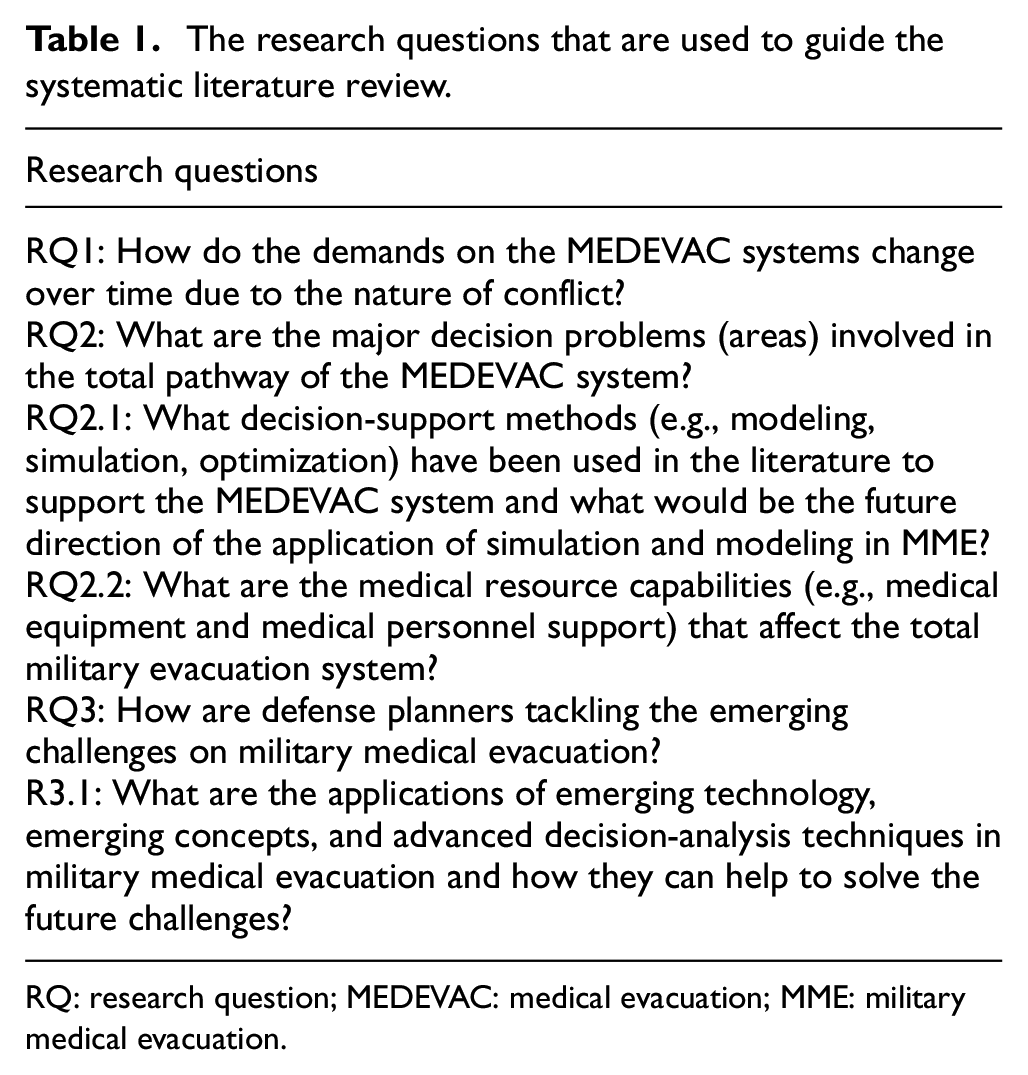
RQ: research question; MEDEVAC: medical evacuation; MME: military medical evacuation.
4. Method
This section explains the methodology of the SLR. In this study, the questions raised aim to better understand the decision problems in the military domain both in MEDEVAC and CASEVAC systems as well as identify the research gaps and future challenges. This research addresses three primary RQs and their subquestions related to the primary RQs as summarized in Table 1.
Search strategy: the content analysis is performed to address the RQs associated with the MEDEVAC system, and the published papers’ chronological, geographic, and analytical distributions among the analyzed corpus.
(1) This study considers articles focusing on MEDEVAC or CASEVAC systems for the military domain.
(2) We eliminate those papers that are related to MEDEVAC/CASEVAC but address topics like Non-traumatic Pulmonary Emergencies, blood transfusions, etc. (not related to decision-making and analysis).
(3) Only items published in English are included in the search queries.
Identification of sources and their criteria: the research and reports that are readily available are compiled in this review. This literature comprises of journal articles, conference proceedings, books, handbooks, and theses. The electronic research sources are: Google Scholar, Web of Science, and PubMed.
Search string/keywords: the following search phrases are taken into consideration while identifying the target articles for this literature review:
(1) Medical evacuation; MEDEVAC; CASEVAC; military emergency medical services.
(2) Present challenges in CASEVAC.
(3) Simulation model applied to (military medical evacuation) or (MEDEVAC) or (CASEVAC); decision-support tool in MEDEVAC, simulation, and (or) modeling in military medical evacuation.
(4) Deployment; medical capacity, alone or in combination.
(5) Simulation in military medicine, simulation in evacuation, simulation, and (or) modeling in healthcare.
On the basis of the selected works’ bibliographies, more publications were found.
4.1. SLR framework
There are seven steps to choose the records that most directly address the RQs. Figure 2 provides an outline of the research work’s methods. This figure presents the number of papers selected in each step.
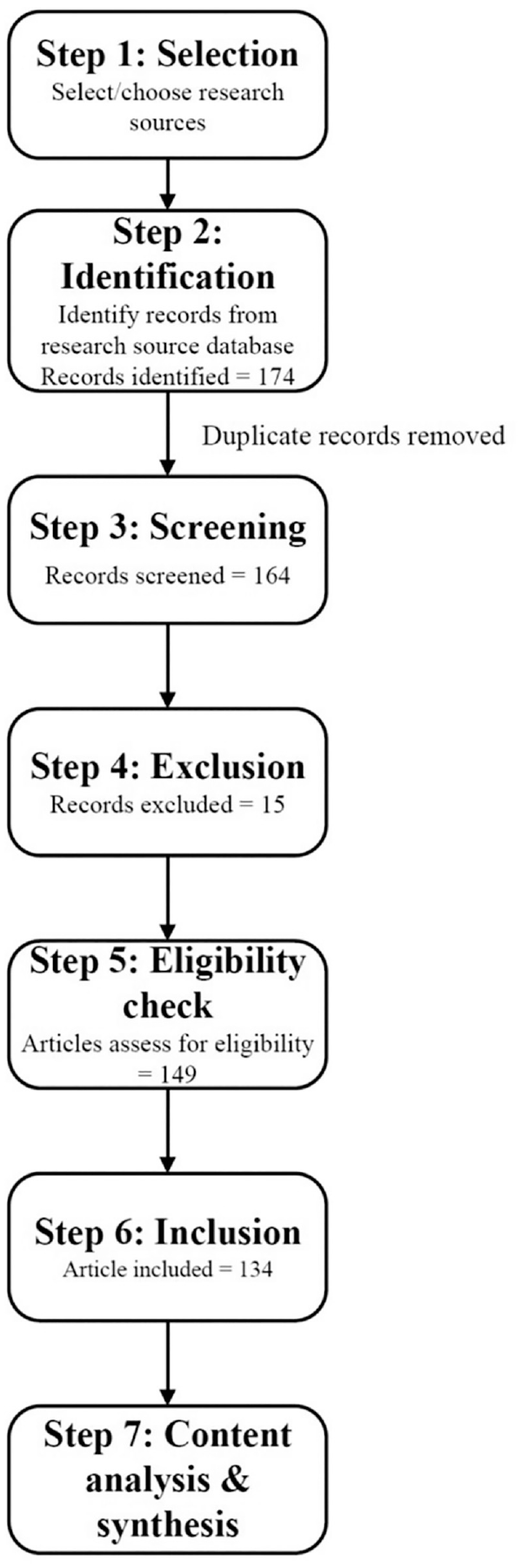
Flowchart of the study’s strategy of SLR.
In Step 1, scholarly databases are selected for the literature review. In the next step, articles are retrieved from different sources by utilizing the search string. The analysis excludes repetitions, redundant articles, and references lacking full texts. Step 3 applies a screening test by removing duplicate articles. Using a criterion in Step 4, articles without the entire text are removed, leaving 175 records accessible for eligibility assessment. The methodology for determining suitability is adapted from Hansen et al. 24 and Salim and colleagues25,26 to give a strict procedure for the acceptance and rejection of articles. Figure 3 illustrates the framework for the eligibility assessment.
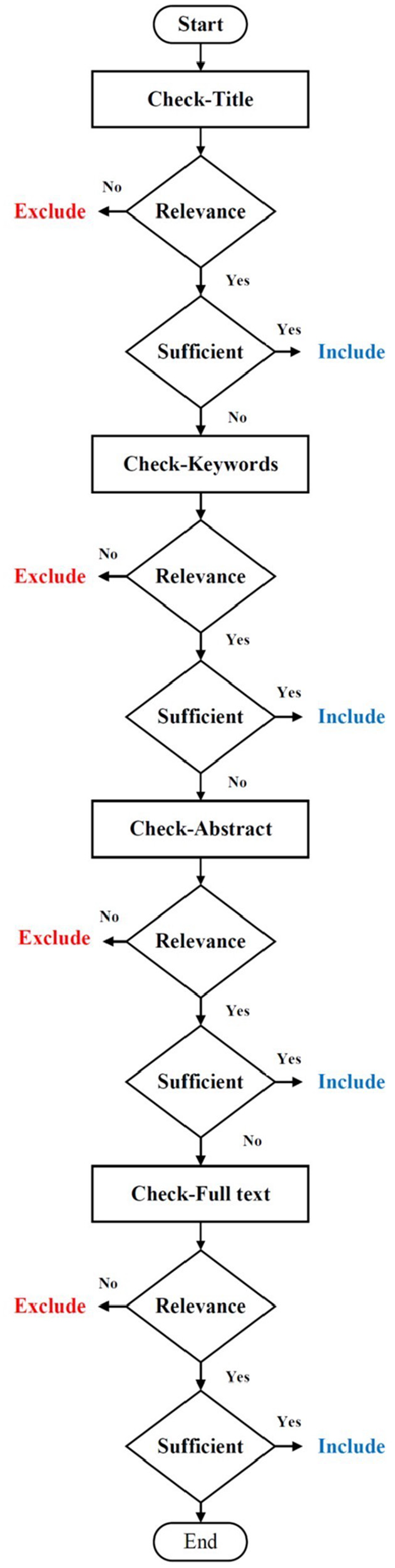
The eligibility assessment procedure of SLR.
In the eligibility check step, four stages of assessment 26 are used. The assessment procedure is applied to include or exclude the articles for analysis. The included papers should address decision problems involved in MME, emerging technologies, emerging concepts, advanced decision analytics techniques in military evacuation, and the evolution of MME. This review paper also analyzes articles which discuss different issues such as capability, management, or planning, as long as it considers emergency MEDEVAC in the military.
Finally, 134 articles are extracted in this literature review. This information aids in the accurate assessment of these studies’ contributions. 23 We have collected information about: (1) the major explored decision problems, (2) how MME has evolved over time, (3) which emerging knowledge—technologies, concepts, and decision analytics techniques—can be adoptable, and (4) which capabilities are utilized in which application context in the domain of MME.
5. Analysis and results
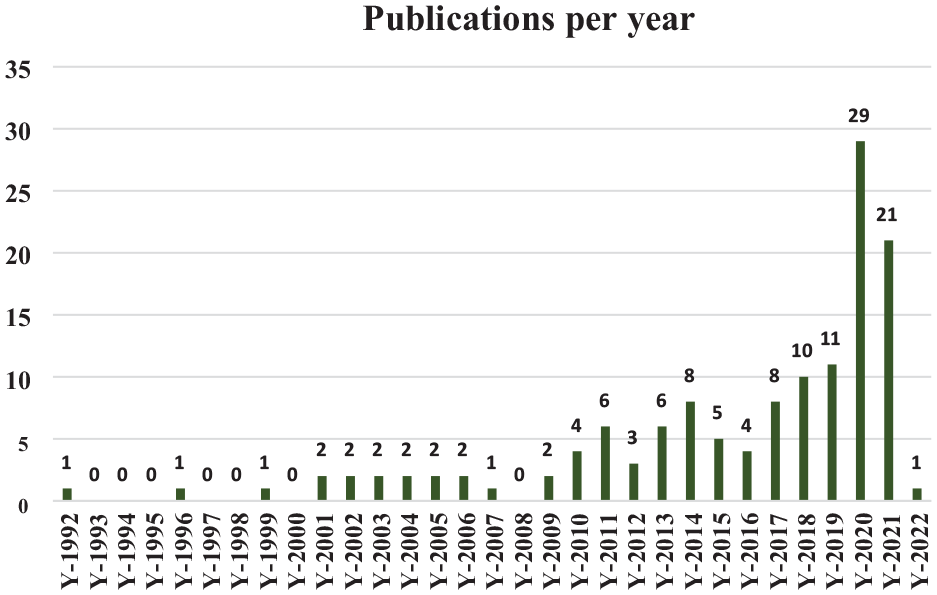
This work analyzes and synthesizes 134 records from 1997 through August 2021. Figure 4 shows the number of articles on the MME in accordance with our RQs that are analyzed in this study. In this analysis, we also considered some literature on non-military emergency evacuation and civilian healthcare. However, this covers only 16% of the total articles. Figure 4 shows that the research on MME was limited until 2010, with two articles on average each year. In the period 2012–2019, there is a gradual increase in the trend. However, with 2020 having the most articles per year (29) and 2020 accounting for 37% of the total literature, the 2020–2021 period appears to be the most productive.
The trend and the number of investigated articles.
It is also identified that a large number of articles address tactical MEDEVAC as well as forward MEDEVAC. However, articles on Strategic MEDEVAC are still limited. Figure 5 illustrate the decision problems and their percentages that are recognized through the analysis of our RQs.
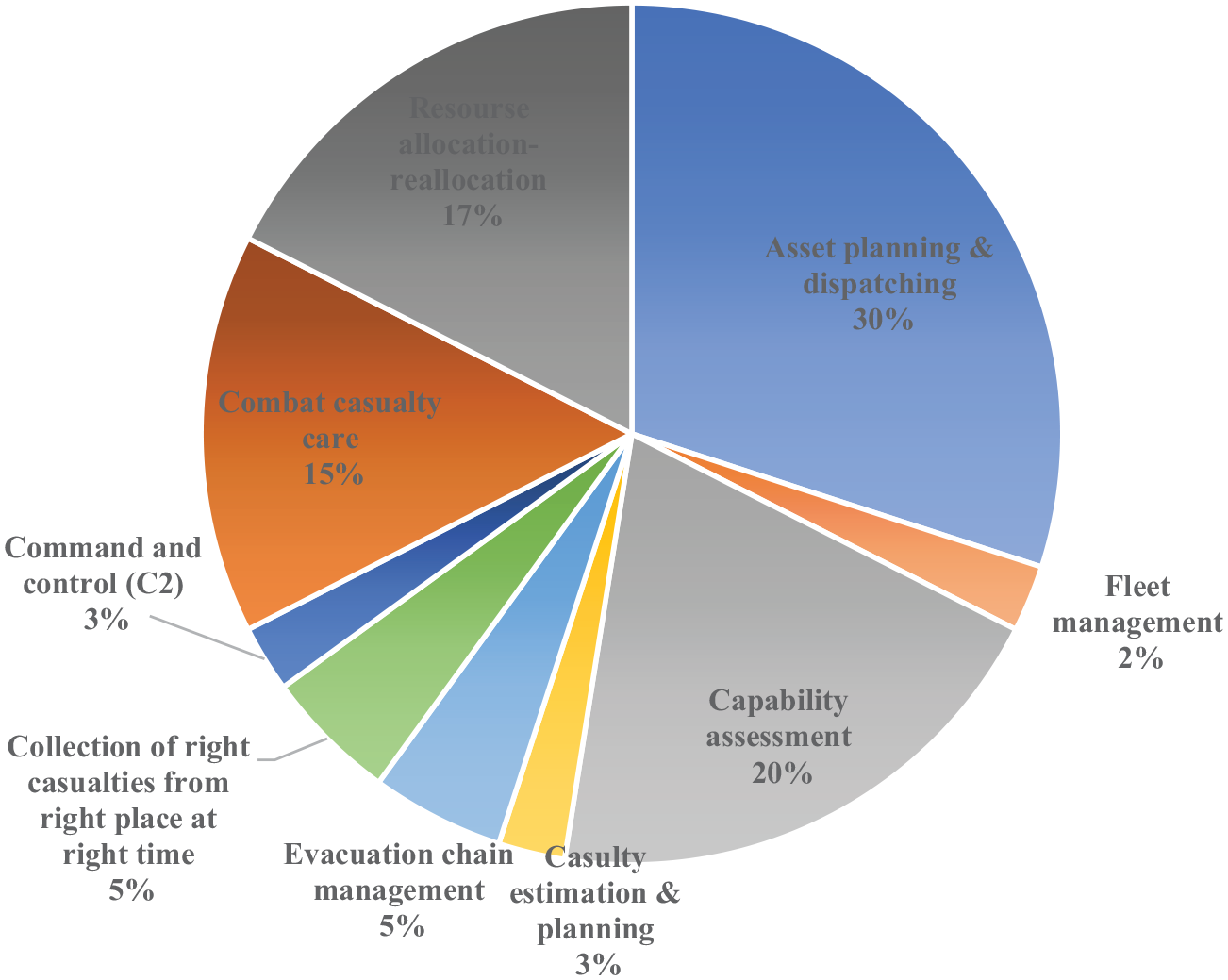
Proportion of decision problems and their percentages among the analyzed documents.
Figure 5 indicates that a large fraction of the literature addresses the asset planning and dispatching problems. It is also identified that the number of papers related to casualty estimation, fleet management, and command and control (C2) of an MEDEVAC system is limited. Moreover, it is observed that based on demographical criteria, the United States dominates the research in this field.
5.1. RQ1
RQ1 focuses on the history of the MME. This question seeks to trace the evolution of the MME system to determine how, due to the nature of conflict, it has changed over time to address the medical needs of a Defense Force that is continually changing. Figure 6 illustrates the review articles12,27–38 of MME, particularly focused on those that discuss the changing processes of the MME system over time.
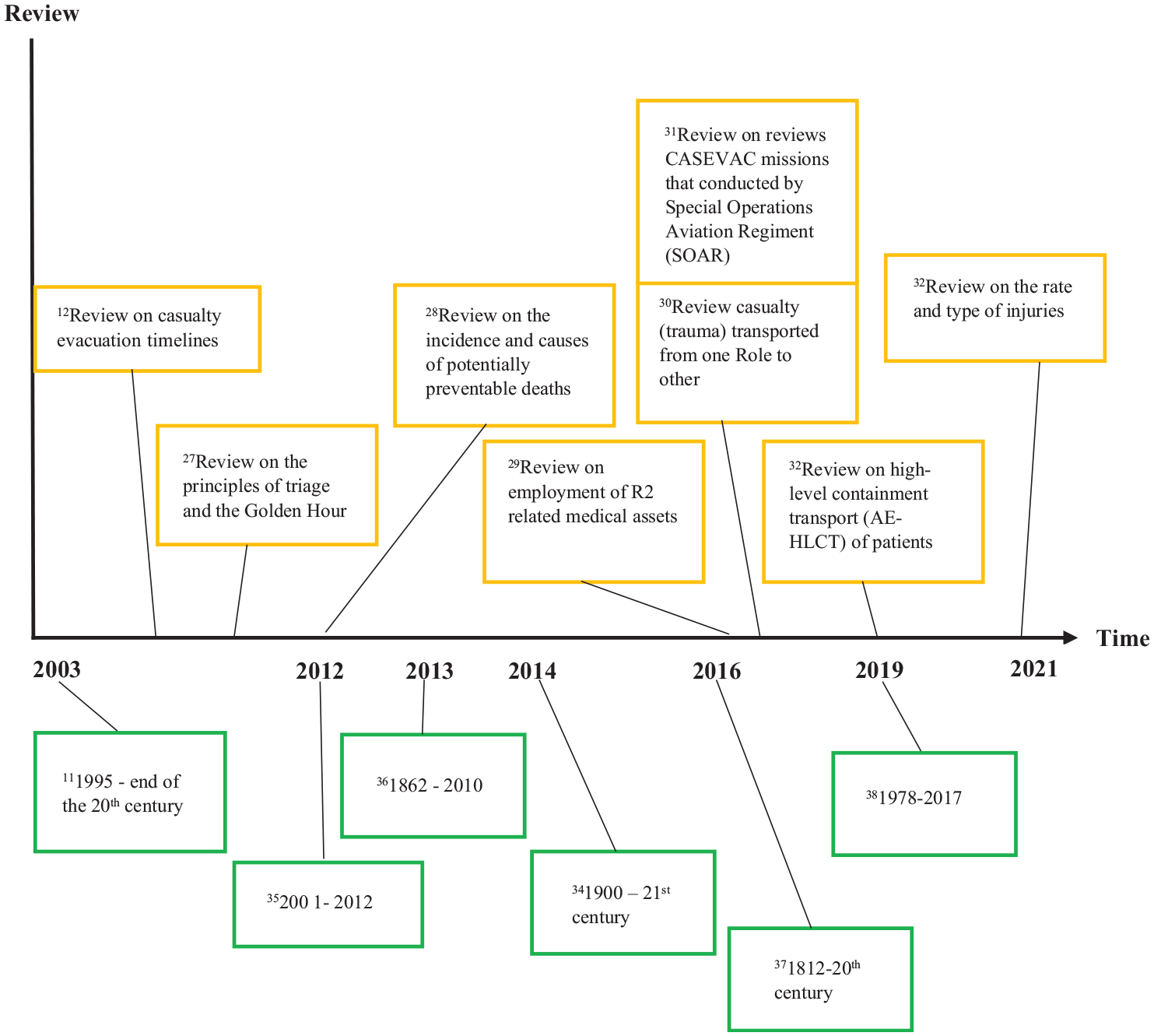
Literature on the review of MME system over time.
In the literature, Bricknell 11 explains how the British Army’s CASEVAC system evolved throughout the 20th century. Olson et al. 36 give a succinct overview of the development of military MEDEVAC of forward aeromedical evacuation (FAME). The authors outline the FAME platforms already in use in Afghanistan, highlight the lessons learned from previous research analyzing the effectiveness of the FAME platforms currently in use, and suggest the future of FAME in other wars. Griffin 34 researches the background of the combat military medical aide in his literature review article (medic)-Australian military medic. This article focuses on a survey of the literature that traces the development of modern military medical aides or medics from the stretcher carriers of the 1900s to their highly trained contemporary counterparts. Parker 12 provides a review of CASEVAC timelines. In this article, the 1:2:4 h principle (previously 1:2:6) serves as the foundation for UK military strategy, specifically, advanced first aid within 60 min, resuscitation treatment within a day, and definitive treatment within a 4-day period. The author reviewed the data about the causation (percentage of different types of injuries) and timing of mortality in war. Blackbourne et al. 35 analyzed the revolution in military medical affairs (RMMAs) that took place in the last decade (2001–2012) of combat casualty management and highlighted that key changes fall under the category of deployed hospital care and en route care. 27 Safdar examines the Golden Hour and triage principles in order to improve the procedure for the evacuation of wounded in accordance with contemporary ideas on modern battlefields. The authors contend that efforts should be made to shorten the time taken for critically wounded patients to be evacuated. Senel 38 performs a comprehensive examination of the literature on the development of military medicine. This study includes a scientometric analysis of international literature on military medicine. Knight et al. 17 discuss the change in army medical doctrine over time and emphasize the requirements to update it. Vanderburg 39 and Flarity et al. 40 discuss the history of aeromedical evacuation.
According to Olson et al., 36 in the course of the Civil War in 1862, Dr Jonathan Letterman founded the first military ambulance service for the Army of US. The ramifications of nuclear and chemical warfare in the 1950s are acknowledged as the main medical difficulties facing military medical system. 11 In this case, medical planning included “mass casualties” whereby the demand for care would outstrip the capability available. In the battlefield, ground ambulances are used to evacuate wounded, until the mid-20th century. The first air ambulance was used for the accomplishment of CASEVAC during World War I, but this was not a common capability. 36 The successive development of CASEVAC systems can be partially accredited to the emergence of new technologies as well as growing social advocacy, which was promoted by Henry Dunant and resulted in the establishment of the first Geneva Convention and the International Committee of the Red Cross. 36
From the review papers on MME, it is identified that the military evacuation system’s function and range of operations are constantly evolving and changing. 34 The environment of the global threat has changed, which has a significant impact on its evolution, changes in Government focus and funding, and also changes in policies. According to Griffin, 34 medical capabilities which use expensive technology and resources are under budget pressure to be cost-effective as the strategic focus and objectives of defense are reshaped. There is now a pervasive expectation from across defense personnel, and the community more generally, that future versions of the MME system should be able to transport casualties from POI to the site of primary surgical intervention, execute life-saving procedures, and start advanced resuscitative treatments in a highly effective and efficient manner.
5.2. RQ2
RQ2 focuses on the areas of major decision problems that are generally considered in the evacuation process of military operations.
5.2.1. Major decision problems in MME
In this literature review, it is identified that there are nine types of decision-making problems associated with the total MME. Figure 6 depicts the decision-making process (involved at the management and organizational level) during the MME, particularly for the senior medical personnel on the scene to decide to submit an MEDEVAC request and to determine the level of evacuation precedence based on the soldier’s (patient’s) condition and the tactical situation, and the evacuation process begins. It is vital to assign an MEDEVAC precedence because it gives the supporting medical unit and controlling headquarters information they can use to prioritize where to commit their evacuation resources.
According to the requirements of the Geneva Conventions, MEDEVAC resources are only used to support the medical mission and are therefore shielded from hostile attack. 2 The synchronized employment of MEDEVAC resources needs to be provided and maintained to uphold the smooth continuum of care from the POI through succeeding vital care responsibilities inside the theater. MME resources are utilized to evacuate the casualty, provide medical treatment, provide en route care, and move causalities within the theater from one MTF to another MTFs. Moreover, MME resources can be used to transport patients to the home nation’s hospital or hospitals out of the operational area. Hence, resources like ground vehicles, air ambulances, dispatching policy, numbers, types and locations of MTFs, fleet management, and allocation-relocation are very significant decision problems in MME.
On the contrary, a good capacity assessment is one of the requirements to provide effective and equitable administration of the entire MME system as well as proper casualty estimation and planning, such as, demand calculation of emergency, time of transport, and work capability. Estimating casualties has an impact on defense strategy, force design, and staffing requirements. By comparing agreed-upon defense planning assumptions and scenarios, the organization size of the military medical capacity that is necessary to sustain armed troops can be calculated. 41 Furthermore, by determining the distribution of medical supplies and the capacity of the system, the need for specialized medical capabilities in theater can be estimated as well as the required distribution of hospitals to areas in the theater. It also establishes the prerequisite for medical capability and capacity (surgical teams, hospital beds, intensive care unit (ICU) beds, imaging) as well as healthcare logistics (medical gases, medical consumables), and laboratory support (blood and related products, diagnostic facilities). In order to assign tactical medical units, the tactical casualty assessment determines the amount of wounded for each battle. 42
From Figure 7, it is found that the collection of casualties at right time from the right place is one of the significant decisions during MME. According to Westphalen, 43 getting the correct casualties to the right medical facilities at the right time, in the right order, by the right methods, and with the proper level of en route clinical treatment is the main goal of an efficient and effective CASEVAC system. Timely response at each level of the evacuation systems, especially when the casualties will receive their first care, is very significant. The evacuation timeline 1-2-4 principle, also known as clinical timelines, has been used by the UK military since 2006. In 2010, the UK military moved to the 10-1-2 principle, where the current Allied Joint Publication (AJP) 4–10 by NATO, 21 the 10-1-2 (2) + 2 principle is considered. 44 According to Scallan et al., 44 any extended hold at Deployed Hospital Care (Forward) (DHC(F)) over 8 h, there is a chance of a rise in morbidity and mortality. In order to give clinical care, longer timescales would also require more personnel, logistics, and equipment support. Therefore, decisions regarding the timelines are critical for MME and assets should be utilized efficiently to save as many people as possible. 12
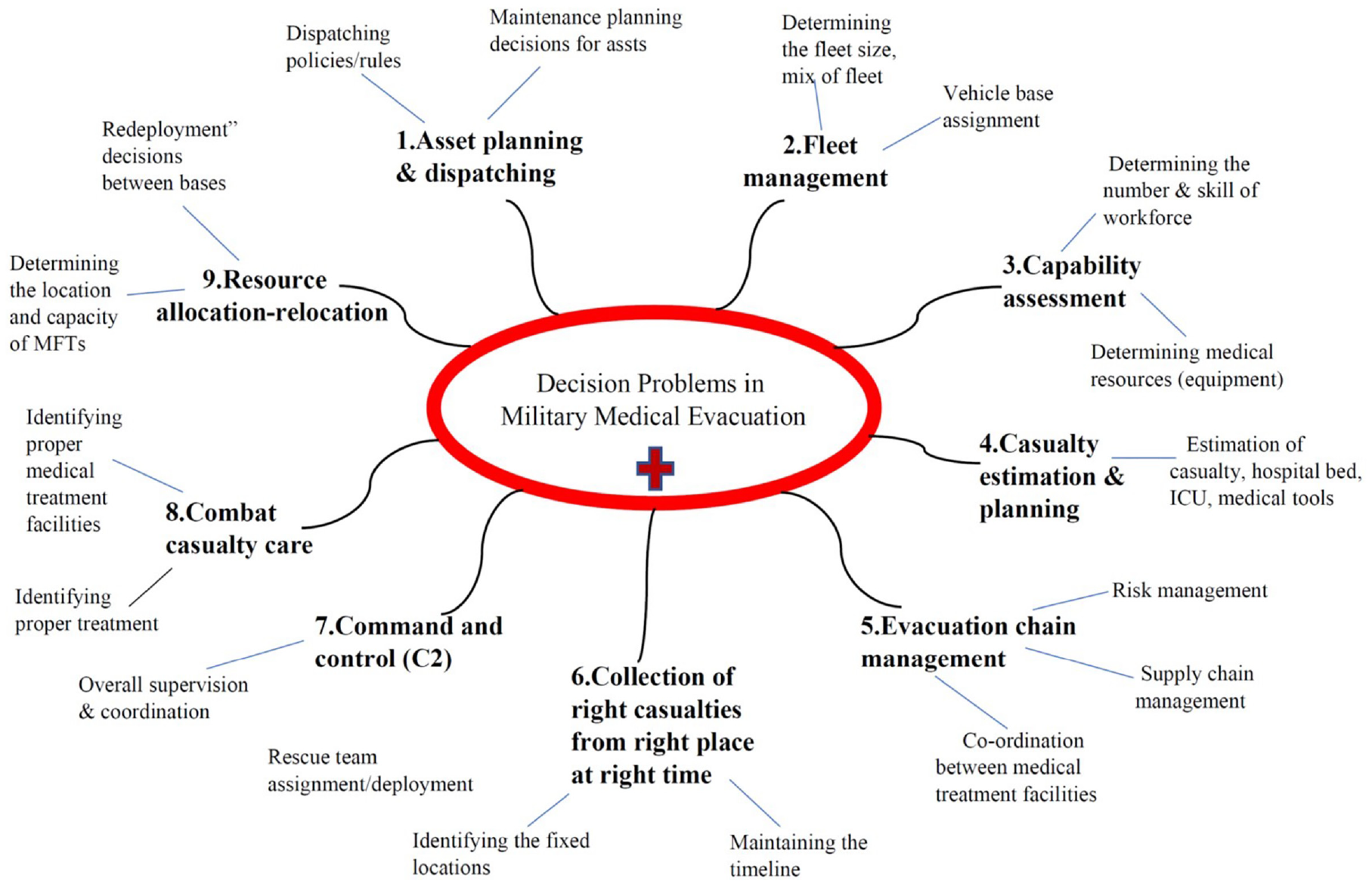
Decision problems in total military medical evacuation.
In addition, C2 are crucial for MME in terms of decision-making; for example, the platoon headquarters decide and control how to treat patients, submit requests, directs, manages, and supervises platoon operations where the C2 component of the unit is the platoon headquarters. 2 For ambulance unit operations, the ambulance/evacuation platoon provides C2. According to Chumer and Turoff, 45 for C2 to function, leadership decision-making 46 and all C2 functional constructs require the “commander’s intent” to be put forward. C2 infrastructure serves as a physical hub for communication, information technology, information systems, and the people who use technology to make decisions about where to put resources and how to distribute them during an emergency response to an evolving situation. 45 Therefore, another important prerequisite for emergency CASEVAC is the creation of a well-defined C2 structure in resource ownership and tactical/operational control. 15
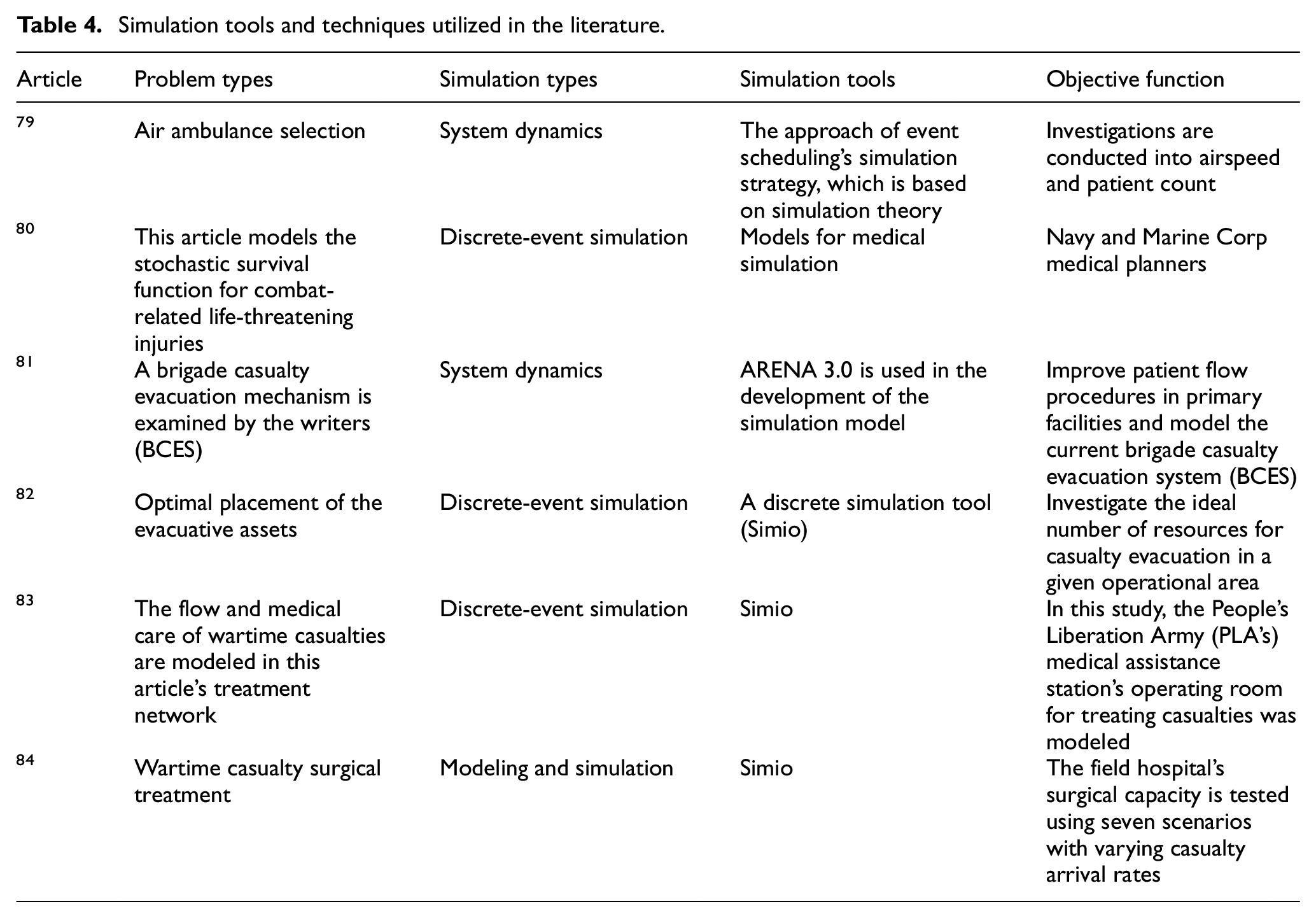
In our paper, we mostly focus on the decision problems associated with the MEDEVAC system and the decision-support techniques (e.g., simulation and modeling) utilized to solve these problems. Tables 2 and 3 present literature on several decision problems and solutions in the domain of MME. Table 2 also highlights the categories of MEDEVAC where the decision takes place. Table 4 provides literature on different simulation tools and techniques to deal with decision problems in MME. These tables relate to the questions RQ2 and secondary questions RQ2.1 and RQ2.2. Table 2–4 identify several decision-support methods, such as optimization, simulation, and geospatial-based decision-support methodology, to support the MME system.
Areas of decision problems and solution techniques utilized in MME.
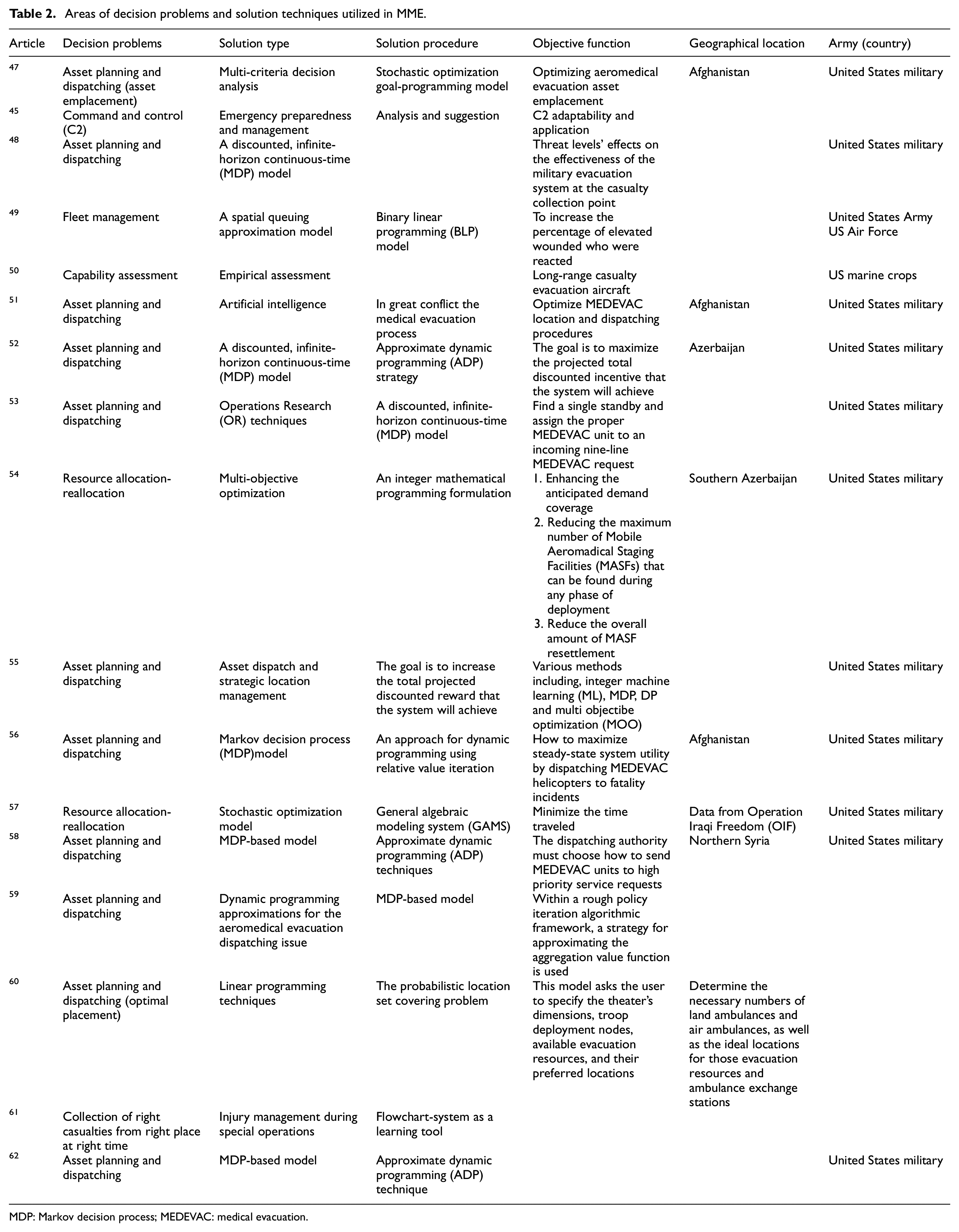
MDP: Markov decision process; MEDEVAC: medical evacuation.
Decision problems and decision-analysis techniques at different stages of MEDEVAC.
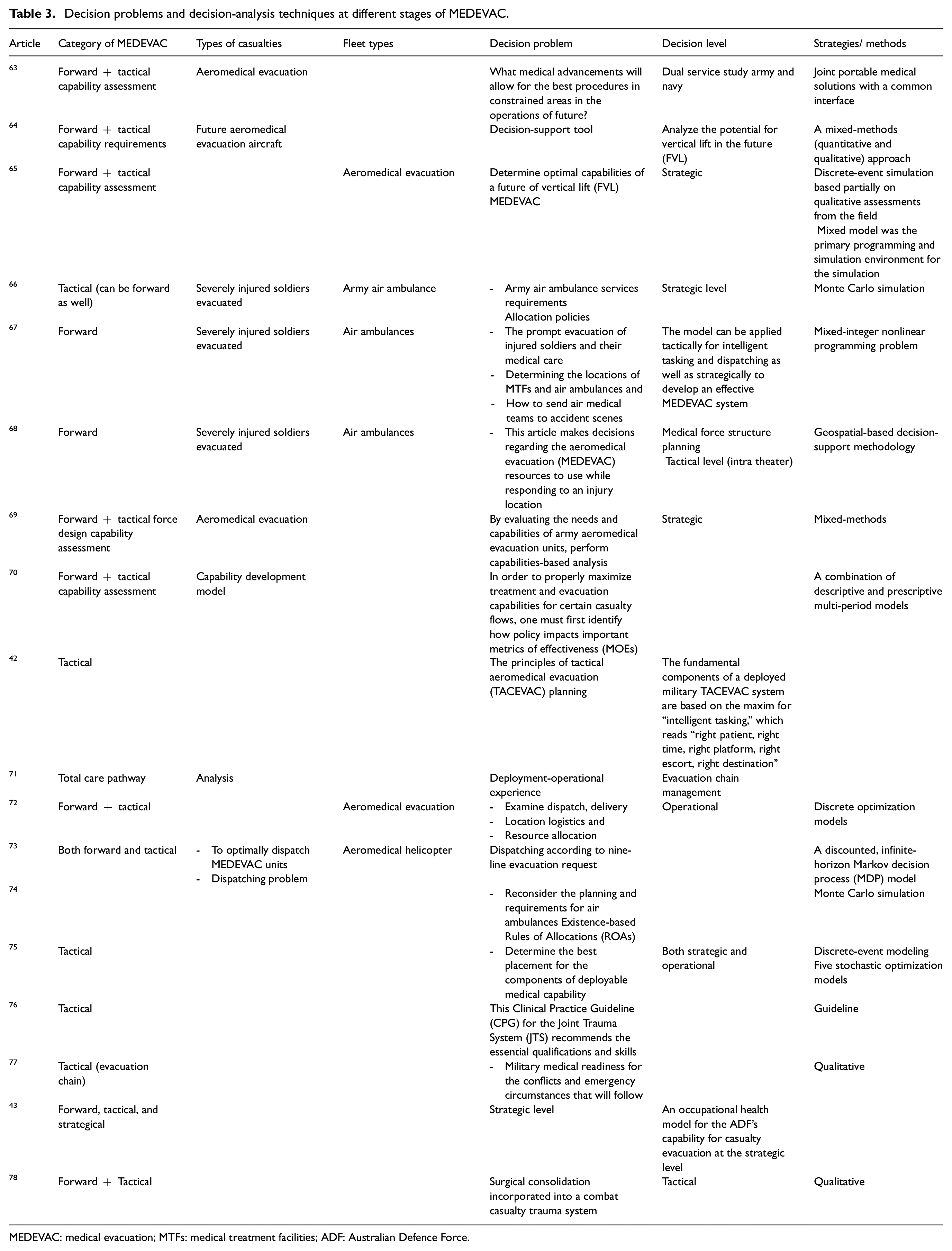
MEDEVAC: medical evacuation; MTFs: medical treatment facilities; ADF: Australian Defence Force.
Simulation tools and techniques utilized in the literature.
From Table 2, it is found that decision problem regarding asset planning and dispatching in MME is very popular. Most of the researchers work on improving this decision problem by utilizing several solution methods. In addition, Table 2 also shows that Markov decision process (MDP) model is a very popular method in this area where most of the researcher applied approximate dynamic programming (ADP) techniques. Several research works consider several criteria as their objectives to improve the effectiveness of the evacuation process. One of the interesting observations is that some researchers utilize emerging technologies such as artificial intelligence and machine learning to solve these issues.
From Table 3, it is found that a very good amount of research had been done based on forward MEDEVAC, and there is still a lack of study in strategic MEDEVAC area. Table 4 also illustrate that most of the research work emphasis on aeromedical evacuation and consider decision problems considering MME resources and capabilities.
Table 4 illustrates the extensive utilization of discrete-event simulation in this MME field. Discrete-event simulation’s ability to facilitate decision-making and optimization enables the testing of various scenarios, comparison of alternatives, evaluation of trade-offs, and identification of optimal solutions. From Table 4, it is also found that most of the research goals are to optimize the resource capabilities and improve the performance.
This paper also identifies the gaps in the literature and the future directions of the MME process. According to our knowledge, no article on MME emphasizes the challenges related to types of land operation and operation terrain together.
5.2.2. Future direction of the application of simulation and modeling in MME
There are several types of challenges during the MEDEVAC process. Based on the challenges related to the types of land operation and the non-permissive nature of rescue sites, we have articulated a framework. This framework can be used as a substantial asset to focus on the future directions of simulation and modeling of the evacuation process. Therefore, the framework can be a novel contribution in the field of MME.
In the framework, there are seven types of land operations, these are: (1) Combat Operations, (2) Peacetime Military Engagement Operations, (3) Peacetime Operations, (4) Stability/Support Operations, (5) Protection Operations, (6) Defense Assistance to Civilian Community, and (7) Humanitarian Assistance and Disaster Relief Operations (LWD 3-0 Operations). Table 5 represents the framework based on land operations.
Reviewed articles based on land operations.
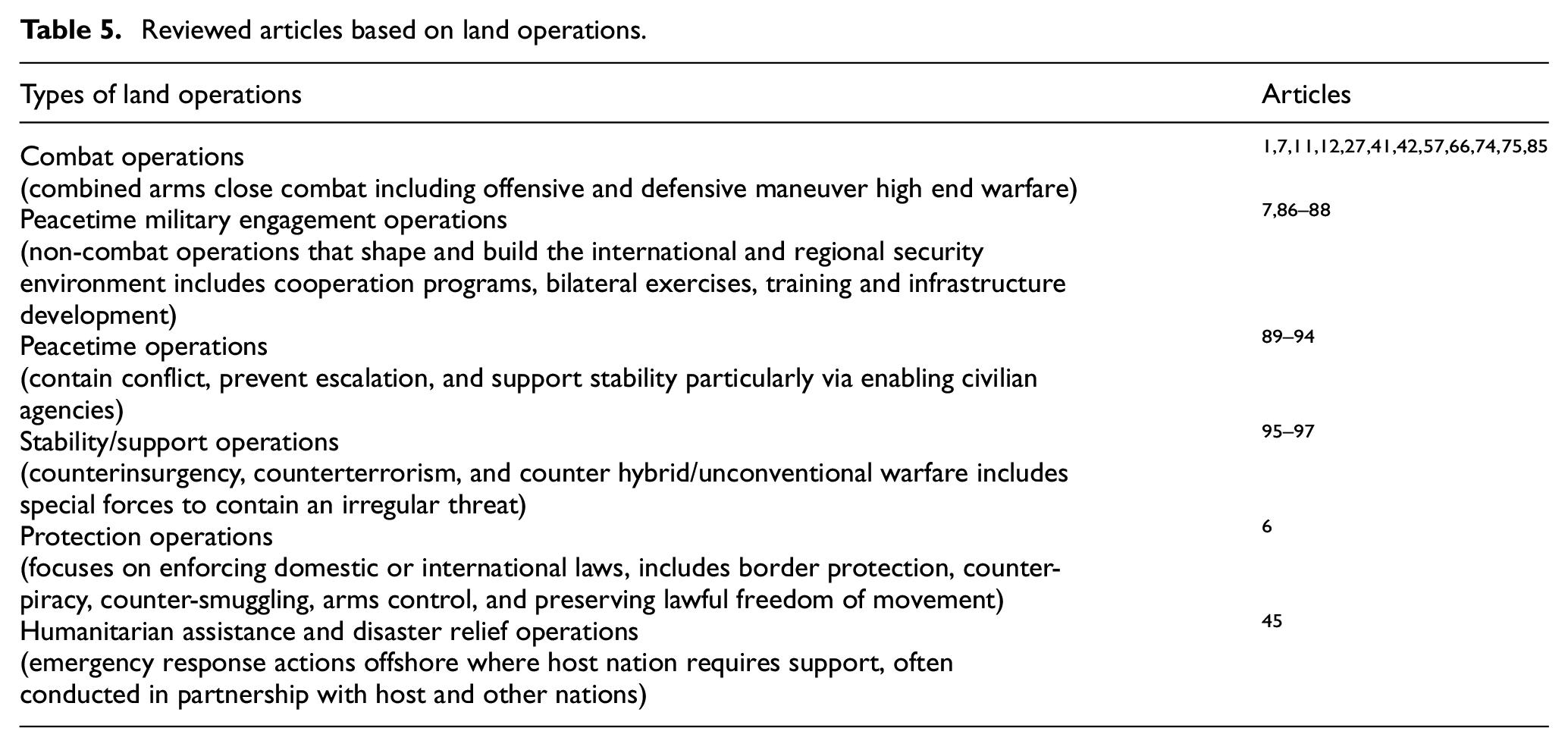
From the literature review, it is found that most of the MME-related articles highlight combat operations and very few literatures address other types of land operations regarding MME. Several articles1,7,11,12,27,41,42,57,66,74,75,85 discussed the MME in a combat operations. While four papers7,86–88 focus on the peacetime military engagement operations category of the framework, especially on training. Seven papers89–94 discussed the evacuation process. All of the authors discussed different simulation and modeling systems in evacuation, which is under the defense assistance to civilian community category of the framework. Under the category of defense assistance to the civilian community,95–97 the simulation process and hospital plant capacity models regarding the COVID-19 pandemic are discussed. Amorim et al. 6 proposed an integrated approach for emergency medical service and focus on peacetime operations. Yang 92 proposed an evacuation modeling for an emergency situation.
Grannan et al.49,72 discuss the terrain (geographical location) of Iraq and Afghanistan while considering dispatch, delivery, and location logistics for military casualties. Scallan et al. 44 also discuss the size and types of the geographical area of operation (Afghanistan). However, it is also found that the significance of terrain conditions in modeling and simulation is ignored in most of the literature on MME. To address this research, gap a framework is proposed where there are four categories of terrain (operational environment) for each operation type. These operational terrains are: (1) open (arctic, desert, woodlands), (2) complex-urban (including subterranean), (3) complex-physical (jungle, mountainous, rivers, and swamps), and (4) complex-littoral/archipelagic.
5.2.3. Capability analysis in MME
From the analysis of the literature, several medical capabilities are also recognized that are crucial in MME system management and planning. The results of the analysis regarding medical resource capabilities are as follows:
Workforce (number of doctors, nurse/medical staff, skill or training).
Hospital beds, treatment table, blood refrigerator, and shelter (basic equipment).
ICU beds, intermediate care ward (ICW) beds, and medical imaging (X-ray, computed tomography (CT), ultrasound scan (USS)).
Laboratory facility (blood products, diagnostic facilities).
Medical logistics (medical gases, medical consumables).
Medical supplies (drugs, medicines).
Medical resources such as medical staff and apparatus (e.g., medical sets, kits, outfits) are the core capability for treating and evacuating wounded soldiers or casualties from the combat zone. 98 The ability of a MME system to take care of casualties depends on evacuation team coordination and management, technical proficiency, and resources accessible for performing medical procedures or surgeries. 85 It has a significant effect on the battle-readiness of the MME process. Effective medical capabilities ensure better service for any casualty and help to increase the survivability rate.
Increasing the capability to meet the demand (e.g., reliable and fast bed usage data to track the availability of spare seats in comparison to the predicted casualty flow) and treating injuries and maintaining operational capabilities will depend on making sure staff can report for duty as soon as possible.99,100 Hence, medical supplies require a robust trade base. On the contrary, the capability of overall treatment could be improved through the training of first responders to strengthen the deployed forces’ capacity to give life-saving measures at the scene of incedent.99,100
5.3. RQ3
RQ3 focuses on how operational concepts could address the future challenges of the MME system. The military must prepare for potential upcoming operational challenges as the threat and overall security environment are continuously evolving. According to Scallan et al., 44 medical, logistical, and organizational issues will emerge as a result of expected future operational settings. It will be necessary to deal with these unidentified uncertainties such as injury information and high complex combat environment.
Several papers44,64,99 have discussed the future of the MME system. In summary, the identified challenges include the following:
High-intensity conflict environments (large number of casualties).
Dynamic global threat environment.
Coping with advanced technology and intelligence (high-accuracy, long-range artillery systems and other sophisticated capabilities, e.g., biological warfare, war drones, nuclear weapons, anti-tank weapons).
Assessment of medical logistics to meet requirements of the future fight.
According to Mabry and DeLorenzo, 101 the latest research indicates up to 25% of battlefield fatalities may be avoidable, and the majority of them occur in the pre-hospital context. Therefore, reducing the pre-hospital mortality gap is necessary for any significant potential enhancement in combat casualty outcomes. Due to the considerable structural difficulties in the current military medical service, pre-hospital treatment must be improved.
Injuries including burns, brain damage, and injuries to the extremities have increased due to the return of armored combat in contemporary conflicts. 102 Military needs to prepare for rapidly executed, large-scale conflicts where the opposition could be equipped with long-range, high-precision weapons that can cause a larger number of casualties with several types of injuries. 99 According to Thomas, 100 the global threat environment is evolving rapidly, and to treat wounded personnel in this setting, the MME system must be robust and reactive. It must improve medical capabilities and medical assistance to give the injured the optimum care possible in a required time frame. Military healthcare systems must increase their capacity for a flexible, robust, and globalized association of treatment centers. In addition, the military medical system requires preparation for a resilient industrial base for logistics support, especially in medical supplies.
The MME system requires advanced knowledge to enable effective management of the total system to support more effective casualty treatment, transportation of casualties from POI to the MTFs, or in between MTFs to reduce (the number of) mortality and morbidity. The success of MME depends on the proactive involvement of trained medical professionals in advance life-saving intervention and resuscitation. 36
On the contrary, defense leaders or planners must take many decisions in the total evacuation process. Advanced decision-making methods or techniques may support defense leaders or planners to make better decisions before operations commence. Emergency operations and warfare today remain difficult and demand continuous improvement 40 as the MME system must continuously evolve to pursue emerging technologies, emerging concepts, and advanced decision analytic techniques to improve the efficiency and the performance of the overall evacuation operation.
RQ 3.1 focuses on the emerging technologies and concepts and advanced decision analytics techniques in military operations that can be applicable in MME systems. Tables 6 and 7 present the literature on emerging technologies and emerging concepts, respectively, in the military domain.
Emerging technologies used in the literature of military operations.
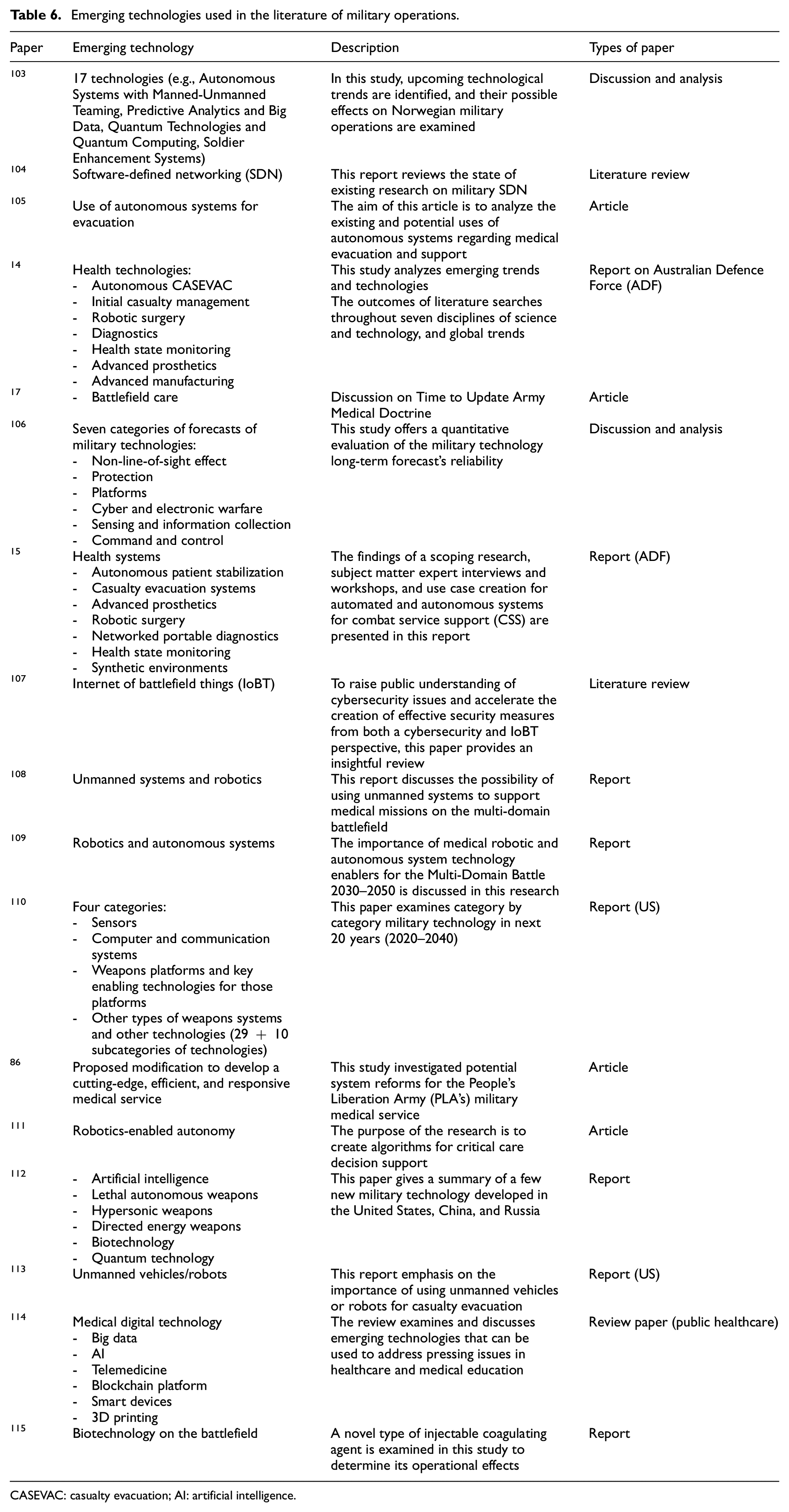
CASEVAC: casualty evacuation; AI: artificial intelligence.
Emerging concepts used in literature.
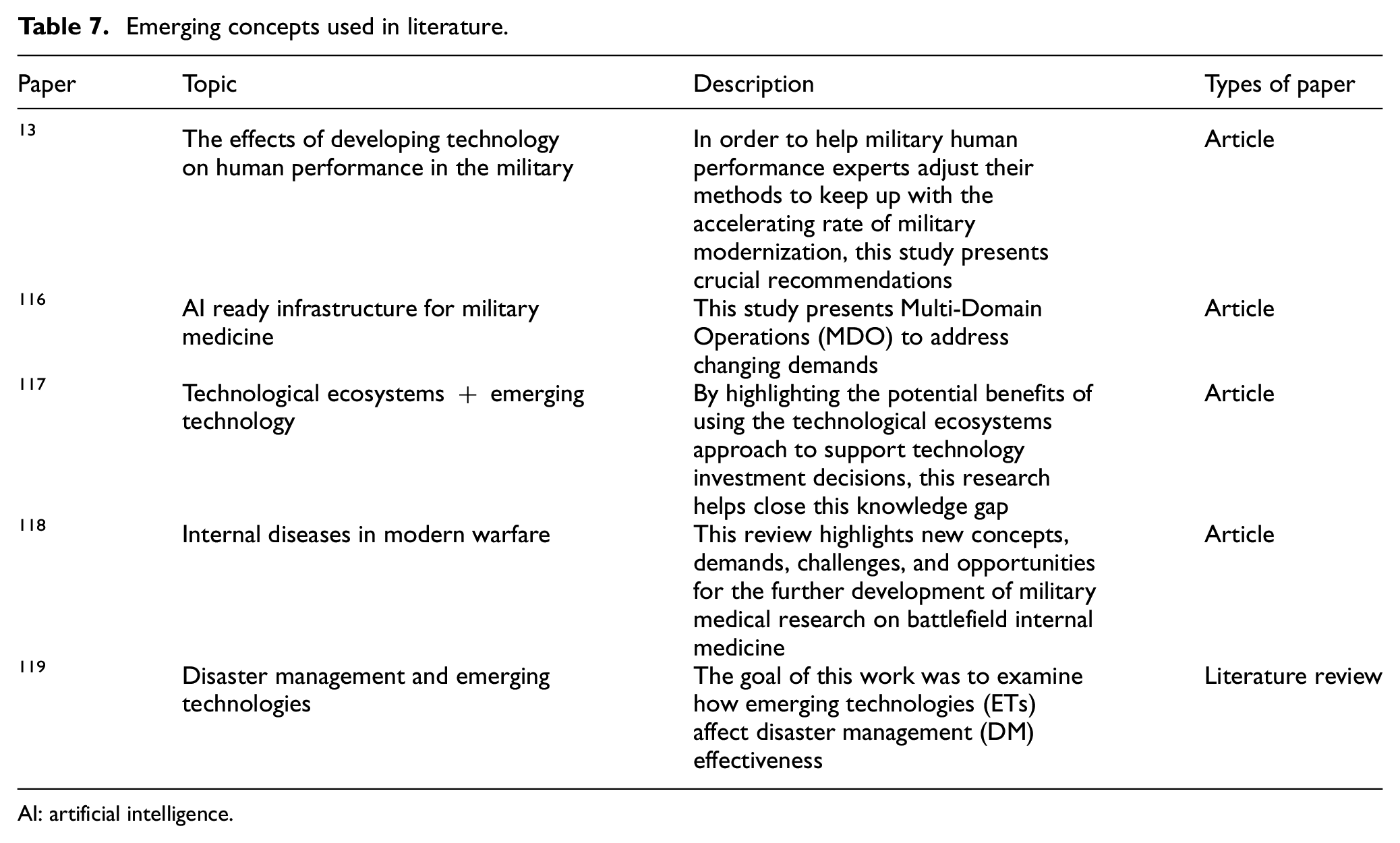
AI: artificial intelligence.
From the aforementioned analysis, emerging technologies (artificial intelligence (AI), autonomous systems, telemedicine, etc.) are recognized to be applicable for military evacuation to address future challenges. The VOSviewer diagram of emerging technologies is presented in Figure 8. From Figure 8, we also observe that telemedicine, autonomous systems, and artificial intelligence are highlighted emerging technologies that can be applied in military medicine. Table 8 shows the main application and possible applications of emerging technologies in the MME system.
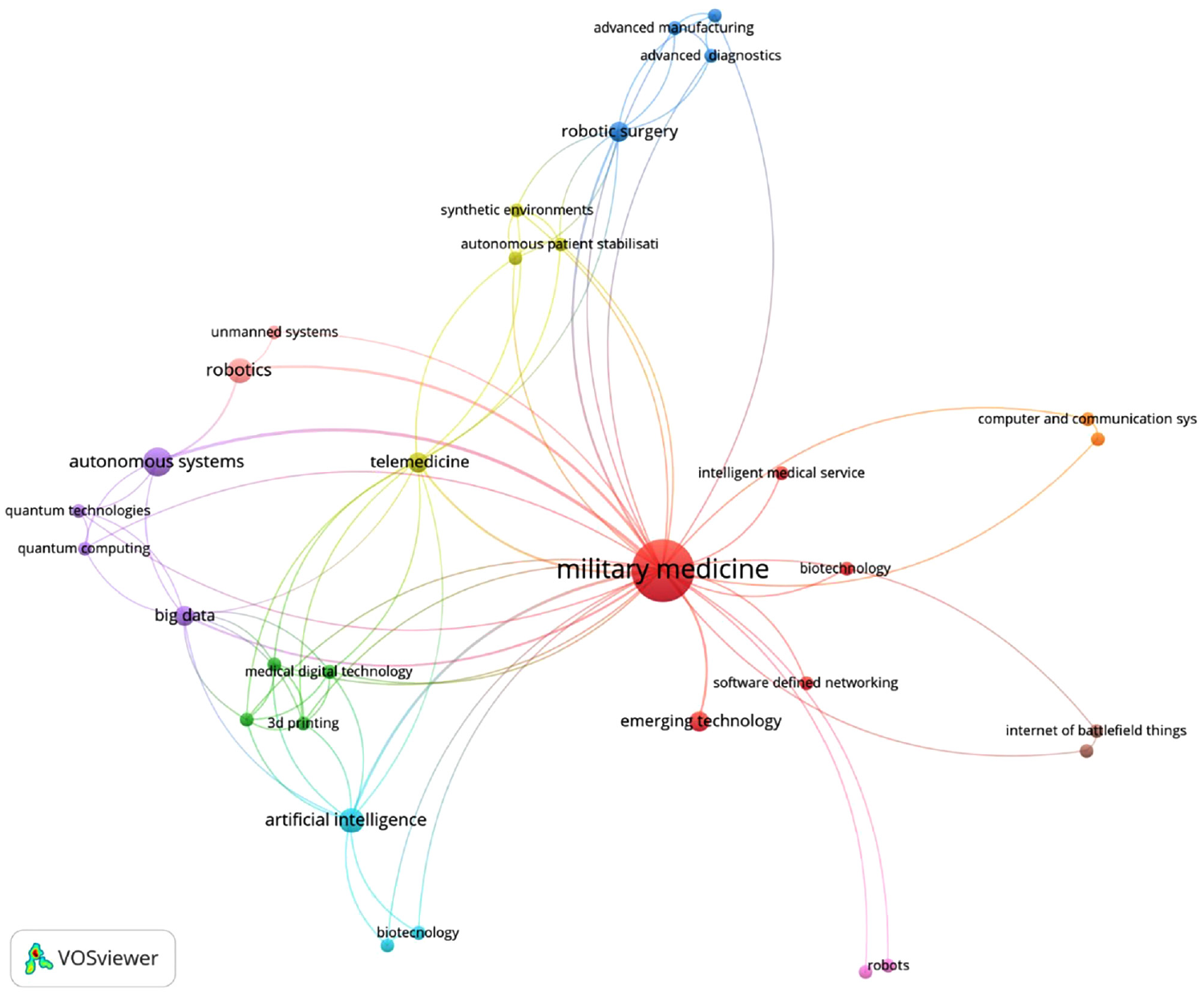
Different fields of emerging technologies in military medicine application and their interconnection.
Application of emerging technologies in the area of MME system.
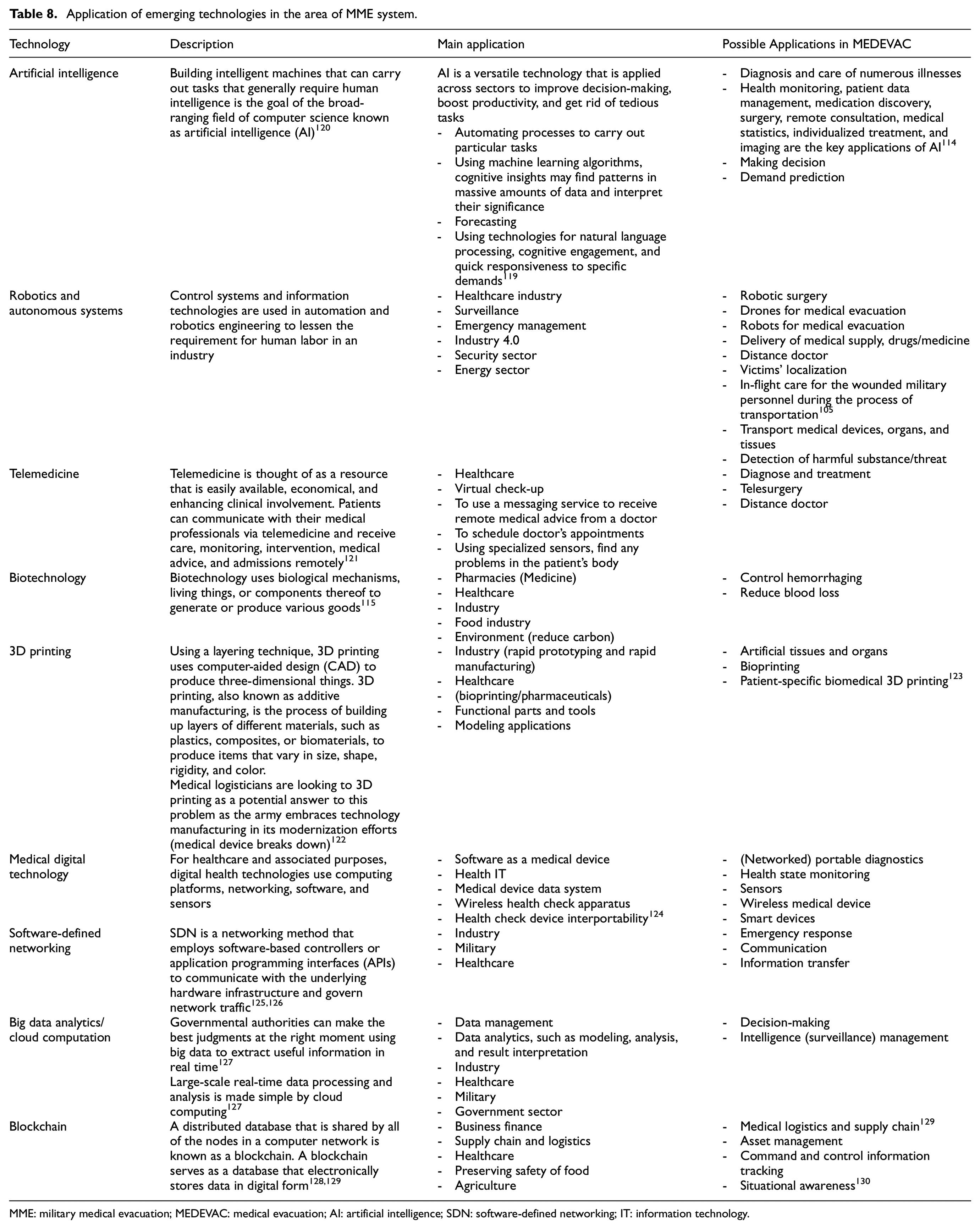
MME: military medical evacuation; MEDEVAC: medical evacuation; AI: artificial intelligence; SDN: software-defined networking; IT: information technology.
Simulation and modeling is used extensively to support analysis and planning in military medicine. 131 In this study, RQ3 also focuses on the advanced decision-support methods that are discussed in the literature. Table 9 lists several academic studies on the application of modeling and simulation to military medicine. Table 10 presents relevant literature on some advanced decision-support techniques in civilian healthcare as well as in evacuation.
Literature on advanced decision-analysis techniques in the field of military medical operations.
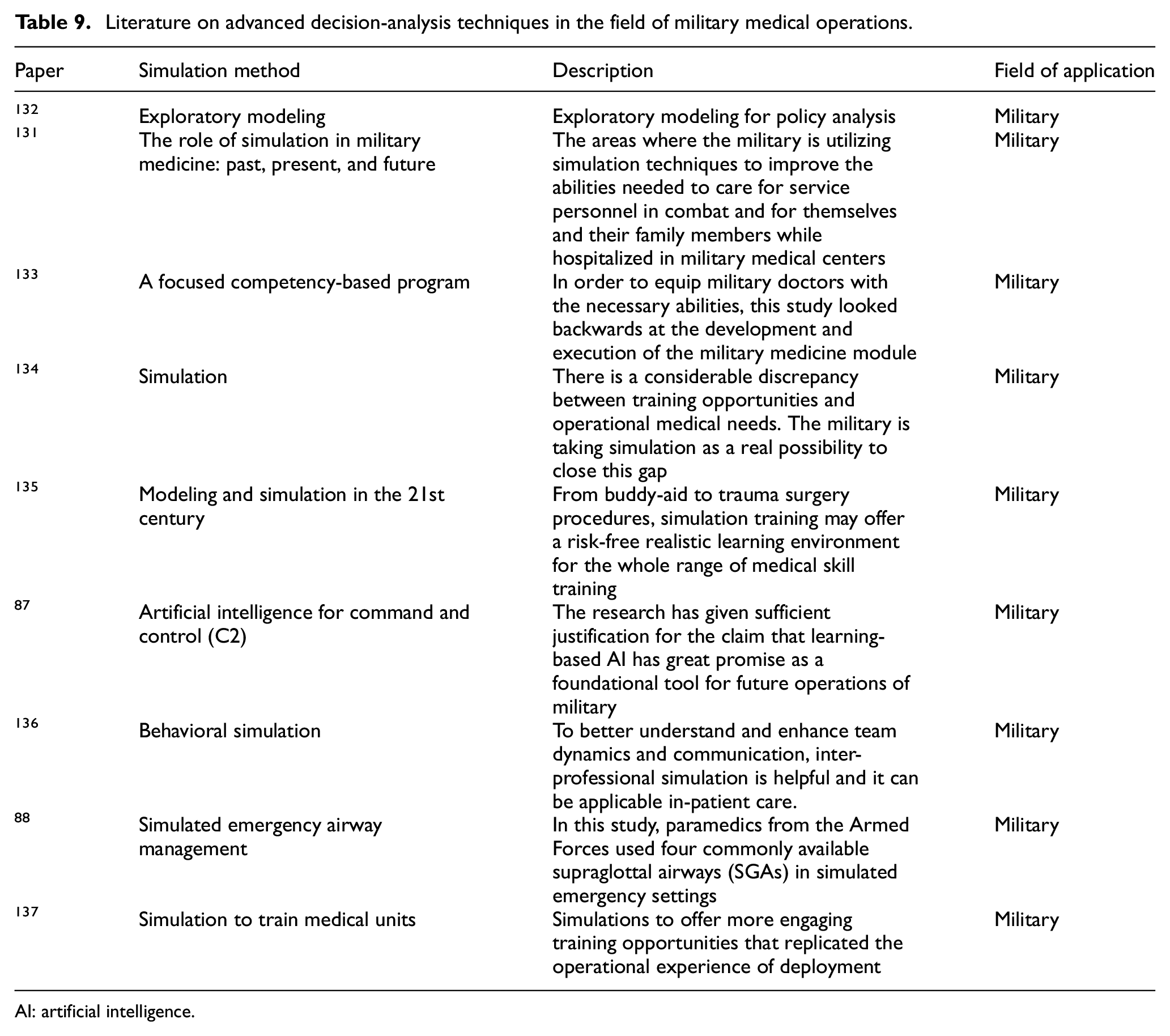
AI: artificial intelligence.
Literature related to advanced decision-analysis techniques in healthcare and evacuation.
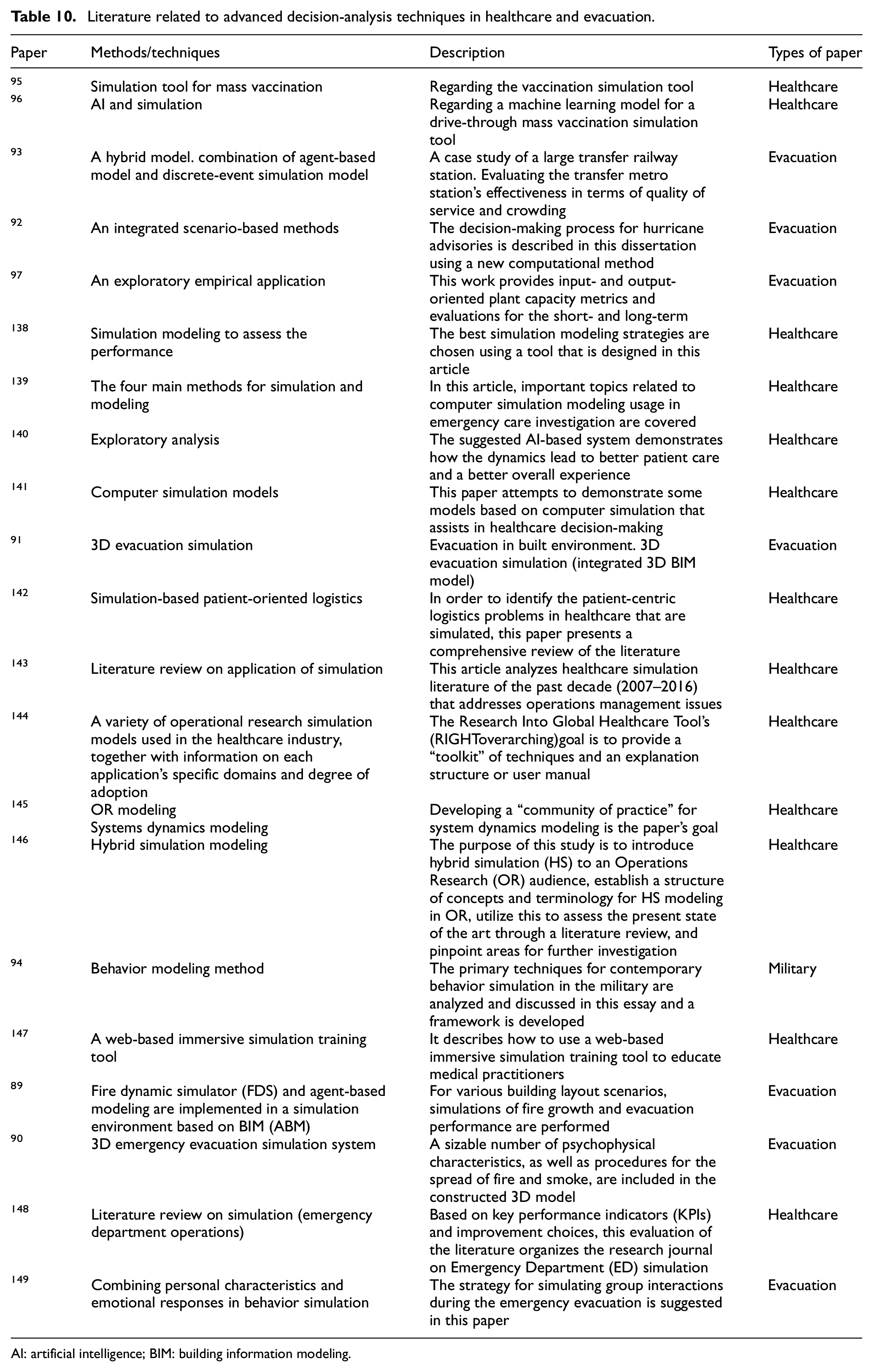
AI: artificial intelligence; BIM: building information modeling.
Decision-support techniques, such as simulation, will continue to be essential to training and skill maintenance in order to grow military medicine. 131 From the literature analysis (Tables 9 and 10), it is found that sophisticated decision-support methods such as hybrid simulation, artificial intelligence, behavioral simulation, virtual reality (VR) and augmented reality (AR), and screen-based simulation can be applied to solve the decision problems described in Figure 4. The literature analysis indicates six advanced decision-analysis techniques are identified. Figure 9 presents these emerging decision-support techniques that could assist defense planners to prepare for the battlefield.
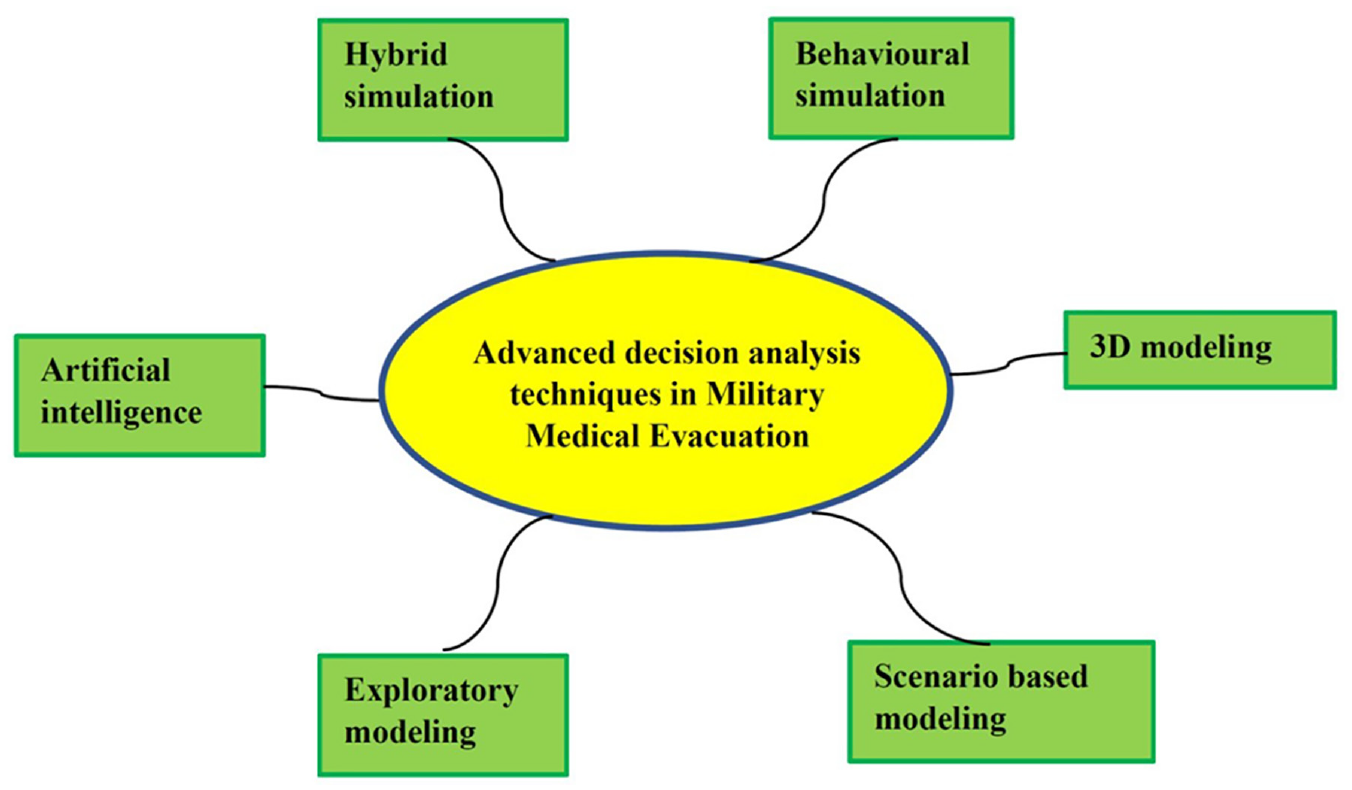
Advanced decision-support techniques for future MME system.
With the use of cutting-edge decision-support tools, the military can potentially put together the best possible team of clinicians, cadets, specialists, nurses, and doctors to support personnel in danger. Military medical simulation may be used in the future to develop remote surgical operations that would enable people serving on ships or in front-line combat to receive life-saving surgery from a distance. 131 Emerging concepts of decision-making techniques (e.g., hybrid simulation, artificial intelligence) can enhance the performance and effectiveness of the MEDEVAC procedures.
Based on the above analysis, it is evident that emerging technologies, advanced decision-analysis techniques, and novel concepts can effectively address future challenges. These cutting-edge tools also offer solutions to the decision problems identified in this SLR. For instance, the deployment of robots and autonomous systems proves particularly valuable in hazardous areas where human presence is perilous. Robotics, autonomous systems, and telemedicine show great potential in resolving decision problems related to combat casualty care and collection of right casualty, from the right place, at the right time.108,109,112
In tackling decision problems such as C2, casualty estimation and planning, and evacuation chain management, the application of IoT, blockchain, and artificial intelligence can be highly effective.103,107,115 Conversely, to enhance the performance of decision problems like asset planning and dispatches, fleet management, and resource allocation, hybrid simulation and exploratory modeling demonstrate relevance and applicability.47,131,146
Moreover, for capability assessment and evacuation chain management, the implementation of behavioral simulation and three-dimensional (3D) modeling proves to be advantageous. By utilizing these diverse techniques and technologies, we can effectively address a wide range of challenges and optimize decision-making processes across various critical areas.
5. Conclusion
Managing the entire MME system’s functionality remains a significant challenge due to the large number of factors, including the dangerous environment, resource constraints, a lack of suitably trained and equipped personnel, and the unpredictability of evacuation (time and skill level). To correctly assess, resuscitate, treat, evacuate, and return injured soldiers to duty requires a highly integrated system with well-informed decision support.
A thorough review of the literature on MME has been completed in order to identify decision problems and how decision-analysis methods are employed to address those decision problems. In this literature review, we have identified nine major decision problems (asset planning and dispatching, resource allocation and re-allocation, fleet management, capability assessment, casualty estimation and planning, evacuation chain management, collection of the right casualties from the right place at the right time, C2, and combat casualty care timelines) in the total care pathway of MME process. We also analyze several literature reports that utilize decision-analysis methods such as simulation and modeling to address these decision problems. Moreover, we have identified medical (resource) capabilities that are significant in the total process of military evacuation. Workforce, medical equipment, assets (such as ambulances), hospital bed, medical logistics, and medical supplies are some of the capabilities that are identified as crucial for MME.
In addition, this work investigates the evolution of MME and how the demands on the MEDEVAC systems have, and are expected to, change over time due to the nature of conflict. It has been determined that the military evacuation system’s practice and function continue to evolve over time. The strategic environment, changes in government focus and funding, and also changes in policies and technological advancement are the most important factors that influence the change.
This work also identifies the emerging challenges of future MME and how emerging technologies, emerging concepts, and emerging decision-making methods can be adapted to support MME to tackle all these challenges. High-intensity conflict environments, advanced technology and intelligence, and the dynamic nature of the global threat environment are some of the future challenges that must be confronted in future military evacuation processes. We have identified nine emerging technologies (e.g., artificial intelligence, robotics and autonomous systems, telemedicine, biotechnology, 3D printing, medical digital technology, software-defined networking, big data analytics/cloud computation, and blockchain) that could be adopted to tackle these future challenges. We also identify their possible application in the field of MME. In addition, six emerging decision-analysis methods/techniques (e.g., hybrid simulation, artificial intelligence, exploratory modeling, behavioral simulation, 3D modeling, and scenario-based modeling) have been identified that can support future military evacuation system analysis.
In combat care, the incorporation of advanced knowledge and technology in an optimal way will reduce mortality and morbidity. It is identified that the most significant reason for patient survivability is the rapid timely movement of casualties from the POI to higher roles/echelons of medical care. Therefore, this study can benefit defense leaders and planners, who should put an emphasis on emerging technologies and concepts to maximize medical capability as well as maximize the performance of MME. They also consider the benefits of adopting emerging decision-support techniques.
Footnotes
Acknowledgements
The research is supported by Capability Systems Centre, University of New South Wales, Canberra, Australia.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.