
Abstract
In this study, we integrate propositions of conservation of resources theory and role theory to examine between-person and reciprocal within-person relations among leader health, leader identity, and three forms of leadership behavior (i.e., transformational, contingent reward, and laissez-faire leadership). We collected monthly data from N = 1,244 leaders in a four-wave fully crossed and lagged panel study. To separate stable (i.e., between-person) differences from dynamic (i.e., within-person) relations, we analyzed the data using a random intercept cross-lagged panel model (RI-CLPM). At the between-person level, we found that leaders with better physical and mental health and reduced symptom experience engage in more transformational and contingent reward leadership and less laissez-faire leadership. At the within-person level, both symptom experience and mental health positively predicted laissez-faire leadership, and laissez-faire leadership positively predicted symptom experience. We did not find support for within-person relations between leader health and transformational and contingent reward leadership, and we found no evidence for mediating effects of leader identity in the relations between leader health and leadership behavior. We discuss these differential findings and their implications for promoting leader health in organizations and theorizing on temporal processes in research on leader health and leadership.
Associations between leadership and follower health have been extensively studied (e.g., Gottfredson & Aguinis, 2017; Montano et al., 2023), whereas the health of leaders has received less attention. This oversight may stem from the prevalent assumption that leaders are inherently healthier than other employees (Barling & Cloutier, 2017; Cloutier & Barling, 2023). However, leader health is not only important for leaders themselves, but is also essential for organizational success. For example, good health can facilitate an individual's attainment of a leadership position, whereas poor leader health is associated with increased leader turnover and reduced organizational performance (Keloharju et al., 2023). Additionally, research suggests that leader health has important implications for leadership behavior (Kaluza et al., 2020).
Based on conservation of resources (COR) theory (Hobfoll, 1989; Hobfoll et al., 2018), researchers have argued that good health constitutes a personal resource of leaders, which they can invest into constructive leadership behaviors (Kaluza et al., 2020). However, COR theory also provides arguments for the reverse direction, suggesting that leadership behavior can influence leader health by generating or depleting personal resources. Although both directions of effects have been widely acknowledged in the literature (e.g., Arnold et al., 2017; Wittmers et al., 2024), most research has focused on unidirectional effects and employed cross-sectional study designs (Harms et al., 2017; Kaluza et al., 2020), which cannot provide insight into the directionality of effects. Additionally, these static approaches conflate between-person and within-person variance and neglect that both health and leadership behavior are dynamic phenomena that fluctuate within leaders over time (Inceoglu et al., 2021; McClean et al., 2019).
In the present study, we consider these complex properties to provide insights into the between-person and reciprocal within-person relations between different forms of both leader health and leadership behavior. In terms of leader health, we examine physical health, mental health, and physical symptom experience (hereafter referred to as symptom experience) as complementary forms of health. While physical health refers to one's overall physical condition and perceived limitations in physical activities in daily life, mental health describes one's overall psychological condition and perceived limitations in daily social activities and emotional functioning (Ware et al., 1996). To consider specific manifestations of health problems, we also examine symptom experience, which refers to physiological and psychosomatic complaints, such as headache and sleep problems (Nixon et al., 2011).
Drawing from COR theory (Hobfoll, 1989; Hobfoll et al., 2018), we focus on transformational, contingent reward, and laissez-faire leadership as distinct leadership behaviors that vary in both the personal resource investment required from leaders and their potential to generate and deplete resources. Transformational leadership is highly resource-intensive for leaders, but also presents multiple opportunities for resource gains (Stempel et al., 2023). In contrast, contingent reward leadership requires fewer resources from leaders, but is also less likely to result in substantial resource gains (Arnold et al., 2015). Finally, laissez-faire leadership represents a passive approach, which requires minimal resource investment, but may result in resource depletion over time, as these behaviors are generally ineffective (Breevaart & Zacher, 2019) and harm the work environment (Klasmeier et al., 2022; Robert & Vandenberghe, 2022).
Furthermore, we complement the COR perspective with propositions from role theory (Biddle, 1986) to explore leader identity (i.e., the self-perception of being and thinking of oneself as a leader; Day & Harrison, 2007) as a potential explanatory mechanism underlying the relations between leader health and leadership behavior. According to role theory, role-related experiences can shape an individual's identification with the role, which, in turn, influences the behavior performed within that respective role (Anglin et al., 2022). We suggest that good health aligns with expectations associated with the leader role (Cloutier & Barling, 2023). When leaders feel healthy, they are likely to identify more strongly with their leader role. In turn, this may encourage them to engage in constructive leadership behaviors that align with the leader role. Healthy leaders should also refrain from laissez-faire leadership, as these behaviors are inconsistent with the leader role. Conversely, when leaders experience health problems, this may weaken their leader identity. Leaders may subsequently engage in lower levels of transformational and contingent reward leadership and higher levels of laissez-faire leadership.
Figure 1 shows our conceptual model. To test this model and provide insights into the relations between leader health and leadership behavior over time, we adopt a four-wave longitudinal study design across three months. We utilize a random intercept cross-lagged panel model (RI-CLPM; Hamaker et al., 2015), which allows us to separate stable between-person relations from dynamic and reciprocal within-person relations.
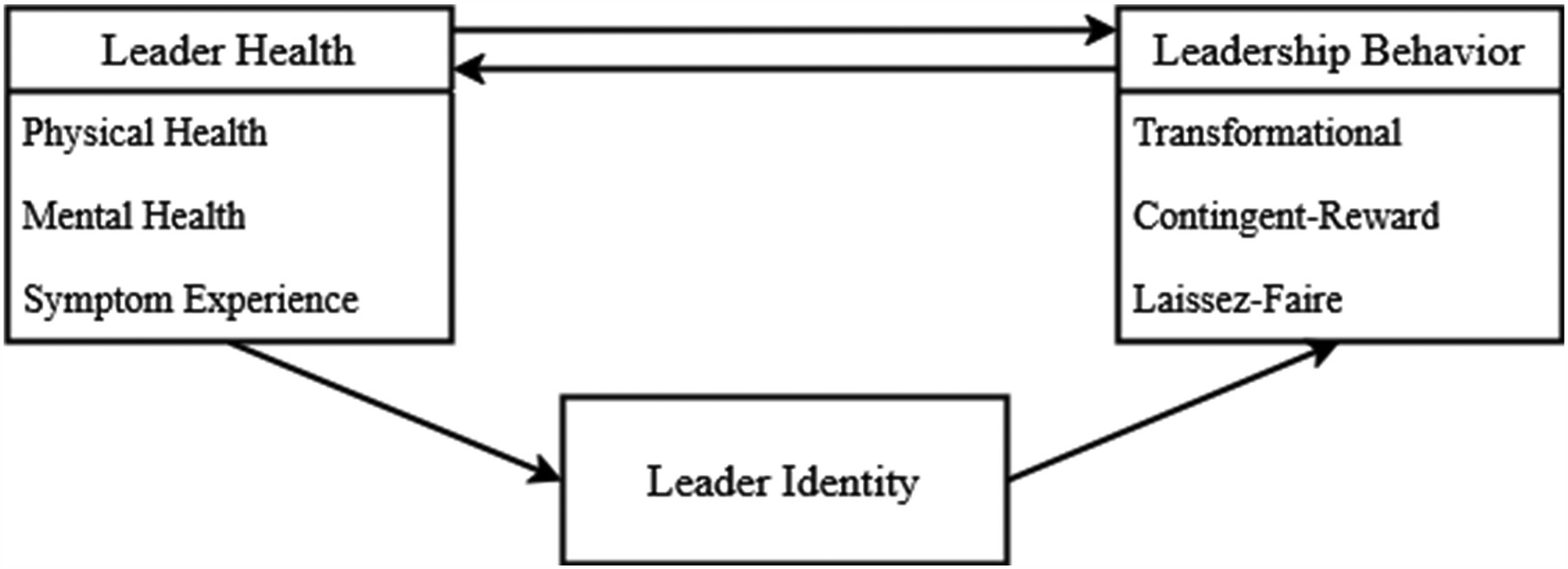
Conceptual model of the assumed direction of effects between leader health, leader identity, and leadership behavior.
The present study offers at least three important theoretical contributions. First, we contribute to research on leader health and leadership (Barling & Cloutier, 2017; Keloharju et al., 2023) by examining reciprocal within-person relations between leader health and leadership behavior over time. Most research in this area has adopted cross-sectional designs and focused on between-person relations (Kaluza et al., 2020), which does not allow conclusions regarding the directionality of effects. By separating stable, between-person sources of variance from dynamic, within-person sources of variance in leader health and leadership behavior, we provide insights into the temporal processes involved in their relations.
Second, we extend research on leader health and leadership that has primarily examined single construct pairs of leader health and leadership behavior (e.g., Geibel et al., 2022; Poetz & Volmer, 2024). By examining multiple, complementary forms of health and leadership behavior simultaneously, we advance the understanding of their relative importance and potentially distinct reciprocal effects on each other. This allows us to identify how different beneficial (i.e., physical and mental health) and detrimental health conditions (i.e., symptom experience) may influence both constructive (i.e., transformational and contingent reward leadership) and destructive leadership behaviors (i.e., laissez-faire leadership), and vice versa. This prevents overemphasis on a single leadership behavior and ensures that multiple relevant behaviors are considered simultaneously (Hancock et al., 2023).
Third, we expand theorizing on the leader role and leader identity beyond external events (Anglin et al., 2022; Nieberle et al., 2024) and complement research that focused on daily experiences influencing daily leader identity and work behaviors (e.g., Lanaj et al., 2023). By examining how leader health, leader identity, and leadership behavior are related to one another across one month, we advance the understanding of the longer-term and more gradual dynamics involved in leader identity. In terms of practical implications, our study may inform the development of leader training and development programs to address leader health and leader identity as a means to support the long-term engagement in constructive leadership behavior.
Leader Health and Leadership Behavior
Research has emphasized the importance of mental health for the work of leaders (e.g., Barling & Cloutier, 2017) and demonstrated that various health indicators can influence staffing decisions in top management (e.g., Keloharju et al., 2023). However, research has mainly focused on leader well-being more broadly (including general subjective well-being, such as life satisfaction, and job-specific aspects, such as work engagement), rather than on physical and mental health as specific aspects of well-being. Additionally, most studies have examined how individual characteristics of leaders and factors in their immediate work environment (e.g., colleagues, job characteristics) are related to leader psychological well-being, which is typically conceptualized as the outcome (Oc & Chintakananda, 2025). Although theoretical arguments suggest that leader health and leadership behavior are reciprocally related to one another, most studies have used cross-sectional designs (e.g., Kaluza et al., 2020; Oc & Chintakananda, 2025), which cannot provide insights into the directionality of effects. These studies suggest that passive leadership behaviors are associated with poor leader well-being, such as burnout (e.g., Arnold et al., 2017; Kaluza et al., 2020). In contrast, constructive leadership behaviors have been linked to both higher leader well-being (e.g., Kaluza et al., 2020; Lanaj et al., 2016) and short-term adverse consequences for leader well-being, which have been attributed to the personal resource investment required to engage in such behaviors (e.g., Lanaj & Jennings, 2020; Lin et al., 2019).
According to COR theory, people are motivated to obtain and protect resources (i.e., valued objects, characteristics, conditions, and energies) because resources can help achieve important goals, including basic survival, social needs, and status (Hobfoll, 1989, 2001). COR theory suggests that resources (e.g., leader health and leadership behavior) are linked to one another via dynamic feedback loops unfolding within individuals over time (Hobfoll, 2001). Specifically, leader health and constructive leadership behavior may create resource gain spirals, which describe the reciprocal reinforcement of resources (Hobfoll et al., 2018). When leaders feel healthy, they may invest personal resources into constructive leadership behaviors (e.g., positive interactions with followers), which, in turn, generate additional resources (e.g., feelings of success or being accepted as leader) that improve leader health (Kaluza et al., 2020).
Conversely, the loss of resources is assumed to trigger resource loss spirals (Hobfoll, 2001). In the context of leadership, health problems may lead leaders to reduce resource-intensive leadership behaviors and engage in more passive leadership behaviors (e.g., withdrawal from interactions with followers) to conserve personal resources. Although these behaviors may provide some short-term benefits for leaders, they can cause problems outweighing any positive effects over time (Hobfoll et al., 2018; Holmgreen et al., 2017). Specifically, disengagement from constructive leadership and engagement in passive leadership not only decreases the positive effects of interactions with followers, but may also result in follower performance issues and increased conflicts. Indeed, research has shown that such negative effects can unfold over relatively short timeframes. For example, weekly laissez-faire leadership has been associated with decreased follower trust in their leader (Breevaart & Zacher, 2019), which can reduce followers’ extra-role behaviors and performance (e.g., Burke et al., 2007). This, in turn, can increase the workload of leaders and their levels of strain, thereby harming their health.
In addition to stable differences between individuals, both health and leadership behavior are subject to substantial within-person fluctuations over time (e.g., Inceoglu et al., 2021; Rudolph et al., 2022; Sonnentag, 2015). Research suggests that the relations between leadership and its causes and outcomes can differ at the between-person level (i.e., differences between individuals) and within-person levels of analysis (i.e., fluctuations within individuals over time), depending on the timeframes considered (McClean et al., 2019). For example, constructive leadership behaviors may require leaders to invest high levels of personal resources (e.g., Tafvelin et al., 2019). Although this personal resource investment may contribute to resource depletion in the short term (e.g., daily, weekly), leaders engaging in constructive leadership likely experience resource gain over longer periods of time (e.g., Li et al., 2023; Lin et al., 2019). Conversely, refraining from resource-intensive leadership behaviors (e.g., avoiding interactions with followers) may help leaders conserve their personal resources in the short term. However, these behaviors contribute to creating destructive work environments, which results in resource loss over longer time periods (Arnold et al., 2015; Klasmeier et al., 2022). It is therefore important to separate stable between-person relations from dynamic within-person relations between leader health and leadership behavior and consider the timeframes over which the effects among these variables manifest.
Health Resources and Transformational Leadership
Transformational leadership encompasses demonstrating enthusiasm, inspiring followers, stimulating their creative thinking, and considering their individual needs (Avolio & Bass, 1995; Judge & Piccolo, 2004). In line with COR theory, research has shown that the ability to engage in transformational leadership strongly depends on the availability of personal resources (Stempel et al., 2023). This suggests that leaders with higher levels of health are more likely to engage in transformational leadership compared to leaders with poor health. Additionally, transformational leadership can generate resources for leaders, such as increased follower engagement (Bader et al., 2023; Breevaart et al., 2014), possibly contributing to more support. Research generally indicates that leader health is positively associated with transformational leadership at the between-person level of analysis (Geibel et al., 2022; Kaluza et al., 2020; Poetz & Volmer, 2024).
At the between-person level of analysis, physical health (H1a) and mental health (H1b) are positively, and symptom experience (H1c) is negatively, associated with transformational leadership.
Regarding within-person relations, we argue that improved health encourages leaders to engage in transformational leadership as a means to seek status affirmation and expand their resources (DeRue & Ashford, 2010; Hobfoll et al., 2018). Improvements in health are particularly valuable for motivating the engagement in these resource-intensive leadership behaviors, as better health is associated with higher internal control beliefs (Ng et al., 2006) and more pleasant affective experiences (Pressman & Cohen, 2005). Feeling in control of one's environment and experiencing positive affect boosts confidence in one's abilities and increases positive expectations, as well as the willingness to help others, which can encourage leaders to engage in inspirational behaviors (Howell & Avolio, 1993; Jin et al., 2016). Conversely, health problems can lead to feelings of overwhelming responsibility and diminished social and physical functioning among leaders, which can impede the ability to engage in stimulating and inspiring interactions with followers (Byrne et al., 2014; Dóci & Hofmans, 2015).
At the within-person level of analysis, physical health (H2a) and mental health (H2b) are positively, and symptom experience (H2c) is negatively, associated with subsequent transformational leadership.
Furthermore, increased transformational leadership likely leads to improved leader health. For example, transformational leadership facilitates positive interactions with followers and leads to higher engagement of followers beyond their formal duties (Keskes et al., 2018; Zacher & Jimmieson, 2013). This may facilitate the work of leaders, as engaged employees are more likely to perform effectively (Breevaart et al., 2016). Additionally, transformational leadership contributes to need fulfilment and favorable affective experiences among leaders (Lanaj et al., 2016), which contribute to better health and help prevent the development of health problems (Pressman et al., 2019).
Conversely, the personal resource investment required for transformational leadership can also deplete personal resources. Weekly transformational leadership is associated with higher levels of emotional exhaustion among leaders, as transformational leadership behaviors require emotion regulation, time, and energy to effectively manage interactions with followers (Lin et al., 2019). Additionally, supporting followers has been linked to increased daily negative affect (Lanaj & Jennings, 2020). However, these negative effects tend to emerge over relatively short timeframes (e.g., daily, weekly). In contrast, the positive effects of transformational leadership (e.g., increased follower engagement) may need more time to manifest. As we focus on within-person relations across one month, we expect that these longer-term benefits outweigh the short-term costs of resource investments associated with transformational leadership.
At the within-person level of analysis, transformational leadership is positively associated with subsequent physical health (H3a) and mental health (H3b), and negatively with subsequent symptom experience (H3c).
Health Resources and Contingent Reward Leadership
Contingent reward leadership is characterized by constructive exchanges between leaders and followers, in which leaders provide followers rewards in return for the fulfillment of expectations (Bass, 1999; Judge & Piccolo, 2004). Although contingent reward and transformational leadership are closely related (Hancock et al., 2023), research indicates that contingent reward leadership accounts for additional variance in leader performance and employee outcomes above and beyond transformational leadership (Breevaart et al., 2014; Judge & Piccolo, 2004). This highlights the need to treat these leadership constructs as distinct.
From the perspective of COR theory, engaging in contingent reward leadership requires a lower resource investment compared to transformational leadership (Arnold et al., 2015; Breevaart et al., 2014). This is largely because contingent reward leadership primarily involves structured, transactional exchanges between leaders and followers rather than the more complex interactions associated with transformational leadership (e.g., inspiring followers and stimulating creative thinking). However, the engagement in contingent reward leadership behaviors still requires a certain level of personal resource investment from leaders (Arnold et al., 2017; Buengeler et al., 2016). For example, assigning tasks and providing constructive feedback necessitate that leaders are attentive and actively engaged with their followers. Leaders in good health are more likely to have the personal resources (e.g., time and energy) to perform these contingent reward behaviors effectively. Supporting this notion, research on between-person relations indicates that leader health is positively related to leadership behaviors related to contingent reward, such as specifying job requirements and monitoring task fulfilment (Kaluza et al., 2020).
At the between-person level of analysis, physical health (H4a) and mental health (H4b) are positively, and symptom experience (H4c) is negatively, associated with contingent reward leadership.
Regarding within-person relations, we argue that improved health enhances leaders’ ability to engage in constructive exchanges with followers and perform contingent reward behaviors, such as clarifying expectations and providing rewards to followers. When leaders are in good health, they are more likely to actively engage with their followers and communicate effectively (Bartels et al., 2022; DeRue & Ashford, 2010). In contrast, declines in leader health likely impede interactions with followers, as contingent reward leadership depends on consistent resource allocation and exchange with followers (Buengeler et al., 2016). Declines in health can lead to fatigue, decreased cognitive function, and emotional distress (Ford et al., 2011; Kelloway et al., 2023). The associated negative affectivity can impair the current leader-follower relationship (Bartels et al., 2022), thus, it can be challenging for leaders to clearly communicate their expectations toward followers and provide constructive feedback and rewards.
At the within-person level of analysis, physical health (H5a) and mental health (H5b) are positively, and symptom experience (H5c) is negatively, associated with subsequent contingent reward leadership.
Furthermore, increased engagement in contingent reward leadership is likely to improve leader health. Specifically, contingent reward leadership leads to higher engagement among followers (Gaudet et al., 2014), strengthens leader-follower relationships, improves follower performance (Young et al., 2021), and reduces follower turnover (Buengeler et al., 2016). As a result, leaders may find their work more manageable and fulfilling. Additionally, when leaders engage in contingent reward leadership, they may encounter fewer negative emotional states among their followers (Montano et al., 2017). This, in turn, reduces the likelihood that leaders experience negative emotional states (Wirtz et al., 2017).
At the within-person level of analysis, contingent reward leadership is positively associated with subsequent physical health (H6a) and mental health (H6b), and negatively with subsequent symptom experience (H6c).
Health Resources and Laissez-Faire Leadership
Laissez-faire leadership is characterized by avoiding decisions, inaction, and lack of availability when needed (Judge & Piccolo, 2004). COR theory suggest that a lack of resources drives individuals to engage in resource-conserving behaviors (Hobfoll et al., 2018). The passive nature of laissez-faire leadership (Breevaart & Zacher, 2019) requires minimal effort from leaders, making it a potential strategy for leaders to conserve their resources. However, this avoidance of resource investment can impede any potential resource gain and contributes to maintaining low resource levels (Hobfoll et al., 2018). Laissez-faire leadership can deteriorate the work environment by increasing conflicts and performance difficulties (Klasmeier et al., 2022; Skogstad et al., 2007), thus is negatively related to leader health (Tóth-Király et al., 2024). Indeed, research suggests that leaders who experience poor health are likely to engage in more passive forms of leadership compared to leaders with good health (Kaluza et al., 2020).
At the between-person level of analysis, physical health (H7a) and mental health (H7b) are negatively, and symptom experience (H7c) is positively, associated with laissez-faire leadership.
Regarding within-person relations, deteriorating health conditions are likely to result in an increase of laissez-faire leadership. Poor health can undermine confidence in one's work abilities (Follmer & Jones, 2018; McGonagle et al., 2015) and may elicit fears that interactions with followers will result in negative evaluations and damage to one's professional image (DeRue & Ashford, 2010). This may lead leaders to engage in more passive, avoidant behaviors, as they might feel less capable of actively engaging with their followers. Indeed, research indicates that leader emotional exhaustion is associated with more laissez-faire leadership (Courtright et al., 2014).
At the within-person level of analysis, physical health (H8a) and mental health (H8b) are negatively, and symptom experience (H8c) is positively, associated with subsequent laissez-faire leadership.
Additionally, increased laissez-faire leadership may contribute to declines in leader health. Laissez-faire leadership can increase interpersonal conflicts and performance difficulties, which may result in higher work demands for leaders (Tóth-Király et al., 2024). Laissez-faire leadership behavior can lead to reduced voluntary work behavior among followers (e.g., Klasmeier et al., 2022), erode trust in the leader, and negatively affect perceptions of leader effectiveness (Breevaart & Zacher, 2019). These adverse outcomes of laissez-faire leadership can create an unsupportive work environment for leaders, increasing their stress levels and negatively impacting their health over time.
At the within-person level of analysis, laissez-faire leadership is negatively associated with subsequent physical health (H9a) and mental health (H9b), and positively with subsequent symptom experience (H9c).
Linking Health to Leadership Behaviors via Leader Identity at the Within-Person Level
Role theory complements the resource-based perspective of COR theory by emphasizing the importance of congruence between leader's characteristics and the characteristics typically associated with leaders in shaping leadership behavior. Specifically, this congruence influences the extent to which leaders identify with the leader role (Lord et al., 2020; Marchiondo et al., 2015). When leaders identify strongly with their leader role, they are more likely to effectively execute this role (Anglin et al., 2022). Leader identity refers to the self-perception of “being a leader or how one thinks of oneself as a leader” (Day & Harrison, 2007, p. 365). This identity is inherently dynamic, shaped by ongoing self-evaluations based on various personal characteristics (Gjerde & Ladegård, 2019; Nieberle et al., 2024; Walker et al., 2024).
We propose that health is an important personal characteristic that influences leader identity. Several personal characteristics typically associated with leaders, such as strength, dedication, and intelligence (Epitropaki & Martin, 2004; Lord et al., 2020), are inherently linked to good health. Furthermore, as people generally associate strong mental health and the absence of mental illness with leaders (Cloutier & Barling, 2023), these expectations of others can influence one's subjective leader identity and behaviors (DeRue & Ashford, 2010). For example, perceived discrepancies between self-evaluations and followers’ perceptions or expectations can encourage leaders to adjust their behaviors toward followers’ feedback (Oc & Bashshur, 2013). Accordingly, when followers communicate their expectations about leader health, or when leaders assume their followers hold such expectations, these perceptions may set standards for leaders’ self-evaluation of their leader identity. Consequently, when leaders experience better health, they are likely to feel more aligned with the leader role, which increases their leader identity. In contrast, health problems may create a sense of misalignment with the expectations associated with the leader role, which may lead leaders to question their suitability and effectiveness as a leader, thereby undermining their leader identity (Lanka et al., 2020).
Leader identity, in turn, motivates leadership behaviors that reflect a positive self-view (Hammond et al., 2017; Lord & Hall, 2005) and are associated with increased leader effectiveness (Day & Sin, 2011). This occurs because a strong leader identity encourages greater involvement and the pursuit of opportunities to demonstrate leadership (Anglin et al., 2022; DeRue & Ashford, 2010). Research indicates that on days when leaders experience higher leader identity, they tend to engage in more transformational leadership (Lanaj et al., 2023) and prioritize the needs of others (Lanaj et al., 2021). These findings support the notion that leaders are more likely to engage in transformational and contingent reward leadership when they strongly identify as a leader. Conversely, leaders with a diminished leader identity may feel uncertain about their influence as a leader and withdraw from interactions with their followers (DeRue & Ashford, 2010). These leaders are more likely to adopt laissez-faire leadership behaviors, as this passive approach enables them to avoid potential disapproval of their leader identity and devaluation by others.
At the within-person level of analysis, physical health (H10a) and mental health (H10b) are positively and indirectly, and symptom experience (H10c) is negatively and indirectly, associated with transformational leadership via leader identity.
At the within-person level of analysis, physical health (H11a) and mental health (H11b) are positively and indirectly, and symptom experience (H11c) is negatively and indirectly, associated with contingent reward leadership via leader identity.
At the within-person level of analysis, physical health (H12a) and mental health (H12b) are negatively and indirectly, and symptom experience (H12c) is positively and indirectly, associated with laissez-faire leadership via leader identity.
Method
Participants and Procedure
Data for this study were collected as part of a larger data collection effort with four measurement waves. No other manuscript based on this dataset has been published or is currently in preparation. The professional online panel company Bilendi was commissioned to recruit leaders from diverse organizational backgrounds in Germany. This company was selected due to its access to a sufficiently large pool of eligible participants. To be eligible, participants had to be at least 18 years old, work at least 20 hours per week, and hold a formal leadership position with direct reports. Bilendi collaborates with many academic institutions across different fields, such as sociology, psychology, and economics, and is ISO 20525:2019 certified, ensuring adherence to international quality standards for market, opinion, and social research. In line with their compensation policy, the panel company offered participants monetary rewards or vouchers, based on the number and duration of their survey participations.
From August to November 2022, participants were contacted at the beginning of each month to complete an online questionnaire. Determining appropriate time lags in research on health and leadership is challenging, as the effects can vary considerably based on the time intervals considered (Fischer et al., 2017; Rosado-Solomon et al., 2023). In this study, we focus on within-person relations between leader health and leadership behavior over the course of one month. This timeframe provides sufficient opportunities for leaders to engage in transformational, contingent reward, and laissez-faire leadership behaviors. Additionally, the one-month timeframe allows enough time for changes in physical and mental health (Jenkinson et al., 1997). Many of the positive effects of leadership behavior on leader health may need some time to manifest, as they involve improvements in the broader work environment, such as increased engagement and support from followers. Regarding laissez-faire leadership, one month is likely an appropriate timeframe to observe potential negative effects on leader health, as physical and mental health problems emerge from prolonged exposure to work stress (Ganster & Rosen, 2013). Generally, relatively short time lags, such as one month, have been recommended by methodologists (Dormann & Griffin, 2015) for longitudinal panel studies.
A total of 2,070 participants completed the survey at Time (T) 1. Of these participants, we excluded 576 participants who did not correctly answer the instructed response items designed to identify careless responders. Additionally, we excluded 223 participants who indicated that they did not hold a formal leadership position at T1 or reported a change in their leadership role during the study period. Furthermore, 27 participants were excluded because they indicated that they had no followers. Thus, the final number of participants was n = 1,244 at T1. At T2, 830 participants completed the survey; at T3, 821 participants completed the survey, and at T4, 772 participants completed the survey. A total of 560 participants provided data at all four measurement points. In total, the 1,244 individuals included in the final sample provided 3,667 monthly observations, corresponding to 2.95 observations per participant on average.
A total of 712 participants were male (57.2%), 531 female (42.7%), and one person indicated “other or no answer.” Their ages ranged from 20 to 78 years (M = 45.1; SD = 11.2). Mean tenure was 13.5 years (SD = 10.1). Regarding highest educational attainment, 22.9% reported lower secondary education, 27.0% reported higher secondary education, and 50.1% reported holding a university degree. In total, 1,136 participants indicated to be working full-time and 108 participants indicated to be working part-time. Participants worked in various industries and occupations, with the largest proportion working in manufacturing (14.3%), followed by the health and social sector (14.1%).
Measures
Physical and Mental Health
We assessed physical and mental health with six items each from the SF-12v2 survey (Ware et al., 1996) in its validated German version (Gandek et al., 1998). Physical health comprises functioning and limitations in various physical activities. The items cover four domains, including general health, bodily pain, physical functioning, and physical role limitations (i.e., limitations in role activities due to physical health problems). Mental health comprises mental constitution and limitations in various activities. The items cover the four domains mental health, vitality, social functioning, and emotional role limitations (i.e., limitations in role functioning due to emotional problems). Example items of physical health include, “During the past four weeks, how much did pain interfere with your normal work (including both work outside the home and housework)?” and “During the past four weeks, how much have you had any of the following problems with your work or other regular daily activities as a result of your physical health?” An example item of mental health is, “During the past four weeks, how much time have you felt downhearted and blue?” Participants responded on 5-point scales, e.g., from 1 (always) to 5 (never) for the example items.
We followed the scoring algorithm developed by the scale authors (Ware et al., 1998) to create scale scores for physical and mental health. In the first step, we calculated physical and mental health scores by applying weights to the raw scores and compute their sum. These weights were derived from a large normative sample. In the second step, we transformed the weighted physical and mental health scores into T-scores. T-scores are standardized scores with a mean of 50 and a standard deviation of 10. To facilitate model estimation and ensure comparability of the coefficients with the other variables in our model, we subsequently transformed the T-scores into 5-point scales without changing their informative value. For calculating Cronbach's alpha, we referred to the original twelve items and assigned six related items to physical health (between-person αrange = .80–.84; αwithin = .62) and mental health (between-person αrange = .83–.85; αwithin = .57), respectively.
Physical Symptom Experience
We assessed physical symptom experience with the 18-item version of the physical symptom inventory (PSI; Spector & Jex, 1998; between-person αrange = .93–.94; αwithin = .89). Participants indicated on a 5-point scale ranging from 1 (not at all) to 5 (every day) how much they experienced each of the specific somatic symptom, such as “eye strain,” “stomach cramps,” or “trouble sleeping” in the past four weeks.
Leader Identity
Leader identity was measured with four items developed by Lanaj et al. (2021), which we adapted for monthly assessment (between-person αrange = .86–.89; αwithin = .70). An example item is, “I believe I have the characteristics of a leader.” Participants responded on a 5-point scale ranging from 1 (not at all) to 5 (completely true).
Transformational, Contingent Reward, and Laissez-Faire Leadership
We measured leadership behavior with 28 items from the multifactor leadership questionnaire-form 5X (MLQ 5X; Bass & Avolio, 1995). Transformational leadership was assessed with 20 items (between-person αrange = .93–.96; αwithin = .87). Contingent reward leadership was assessed with four items (between-person αrange = .67–.78; αwithin = .50). Laissez-faire leadership was assessed with four items (between-person αrange = .75–.77; αwithin = .46). The items were scored on 5-point scales ranging from 1 (not at all) to 5 (frequently, if not always).
Analytical Approach
Prior to testing the hypotheses, we conducted attrition analyses to estimate the potential effects of participant drop-out over time on our findings (Goodman & Blum, 1996). We used a multiple logistic regression model to estimate the amount of variance in attrition explained by demographics (i.e., age and sex) and the focal study variables at T1. The predictors accounted for 8.4% of the variance in observed attrition (R2CoxSnell = .084). Given the rather small amount of explained variance, we do not consider systematic attrition to be a major problem for our analyses. We also conducted confirmatory factor analyses (CFA) to determine the fit of the proposed measurement model and test longitudinal measurement invariance.
We tested the hypotheses simultaneously with a random intercept cross-lagged panel model (RI-CLPM; Hamaker et al., 2015) using the lavaan package (Rosseel, 2012) in R. An advantage of the RI-CLPM is the separation of between-person and within-person variance, which allows us to examine temporal processes. Figure 2 displays a schematic representation of the RI-CLPM. In the RI-CLPM, we included data from all 1,244 individuals and accounted for observed missingness by using full information maximum likelihood (FIML) estimation. Data, R code, and detailed results of the analyses are available in our online supplemental materials: https://osf.io/xq9wr/.
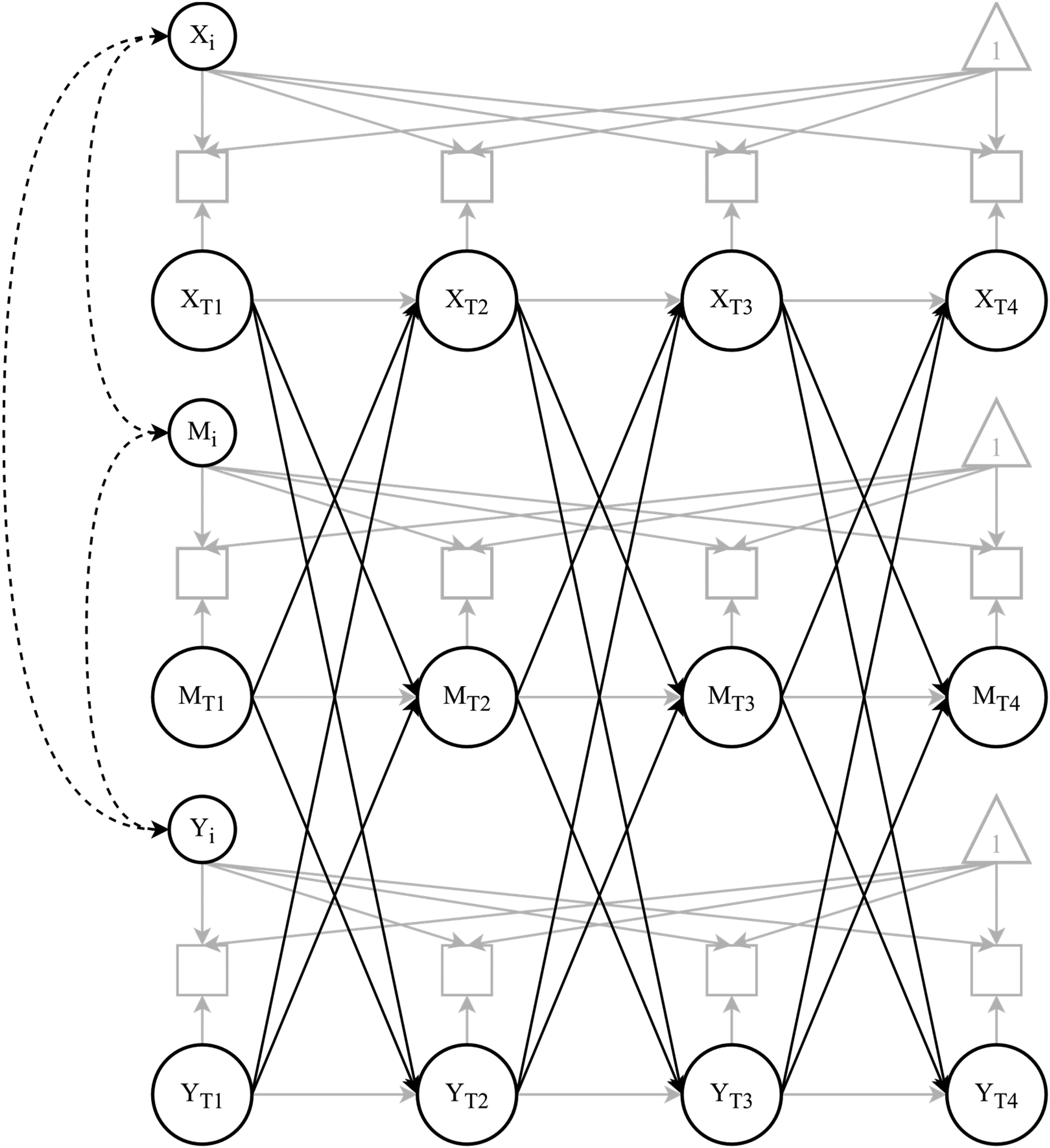
Schematic illustration of our focal Random Intercepts Cross-Lagged Panel Model (RI-CLPM); XT1– XT4 represents measurement of health, MT1– MT4 represents measurement of leader identity, and YT1– YT4 represents measurement of leadership behavior over time; for the sake of clarity, indicators for health and leadership behavior are combined into one representation; black solid lines depict cross-lagged parameters of interest at the within-person level; black dashed lines depict parameters of interest at the between-person level.
Results
Descriptive statistics and correlations, as well as intraclass correlation coefficients (ICC1) are shown in Table 1 and Table 2, respectively. The ICC1 values indicate that the proportion of within-person variance relative to total variance ranged from 27% to 42%.
Means, Standard Deviations, and Correlations of Study Variables
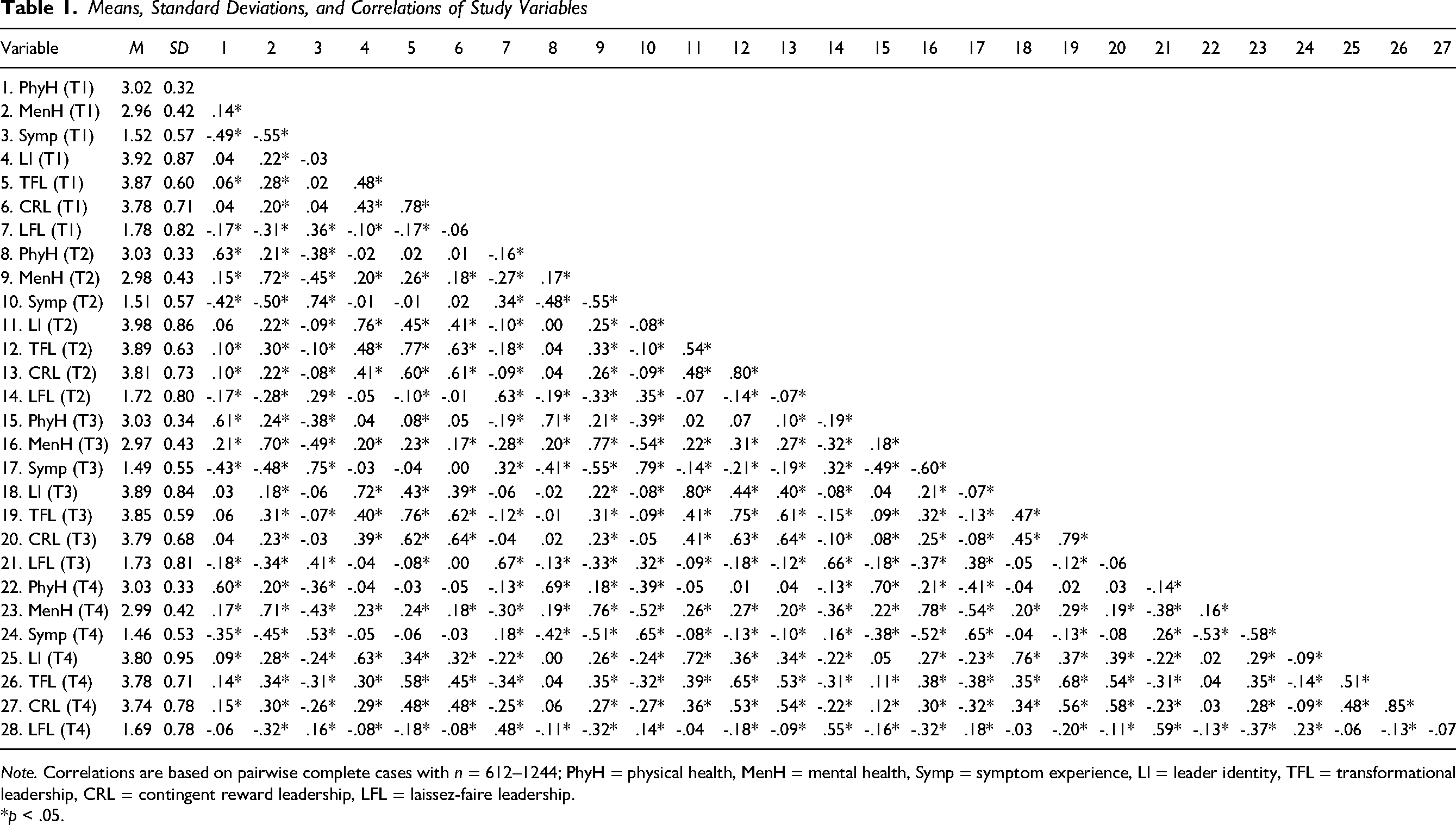
Note. Correlations are based on pairwise complete cases with n = 612–1244; PhyH = physical health, MenH = mental health, Symp = symptom experience, LI = leader identity, TFL = transformational leadership, CRL = contingent reward leadership, LFL = laissez-faire leadership.
*p < .05.
Intraclass Correlation Coefficients (ICC1) and Between- and Within-Level Correlations.
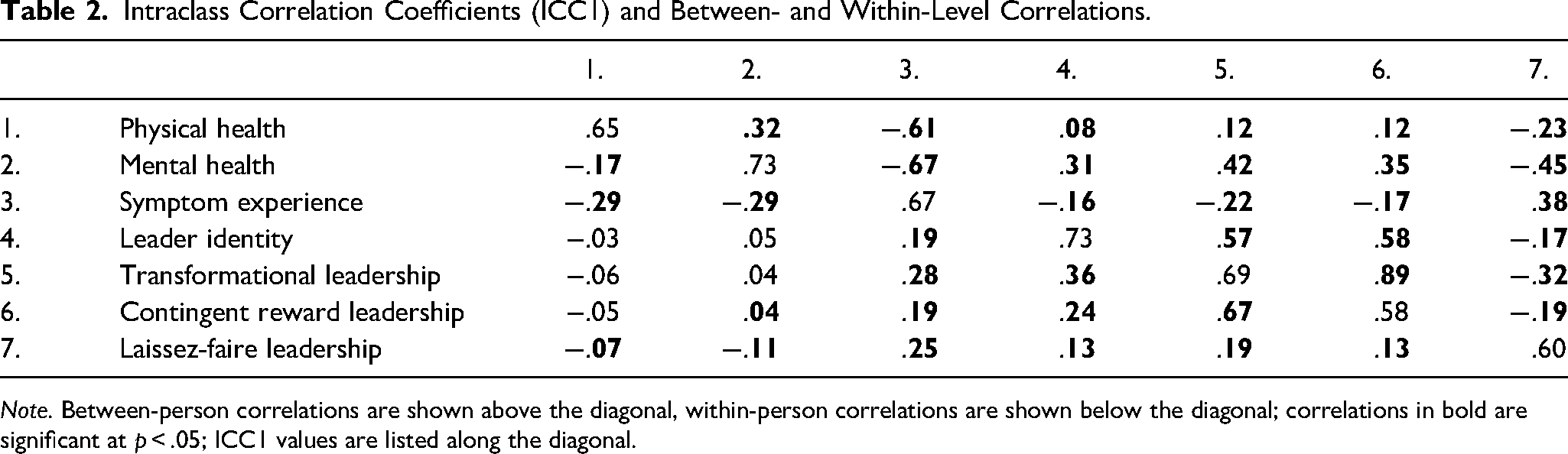
Note. Between-person correlations are shown above the diagonal, within-person correlations are shown below the diagonal; correlations in bold are significant at p < .05; ICC1 values are listed along the diagonal.
Analyses of Factor Structure and Measurement Invariance
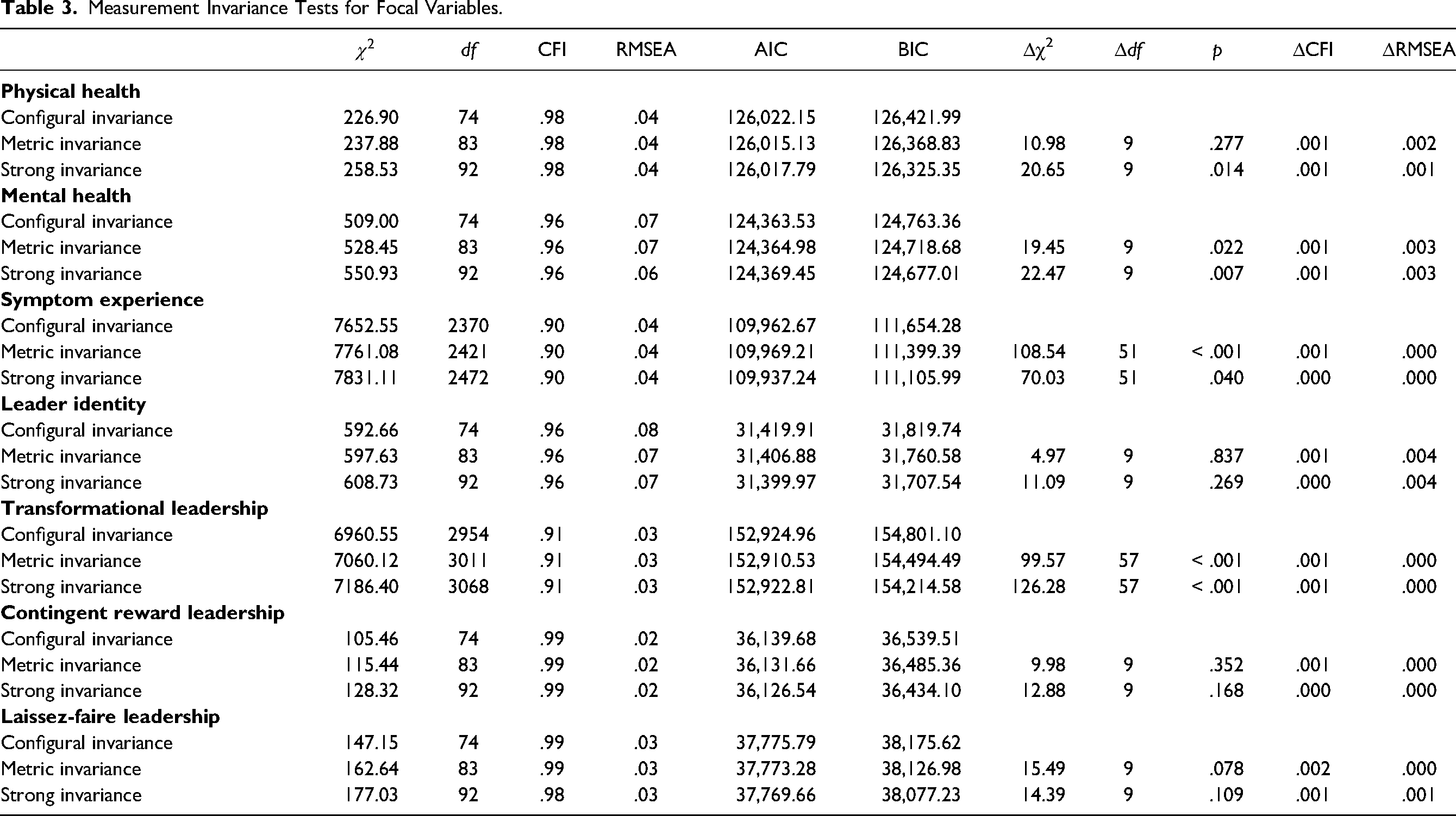
We conducted CFA based on T1 data to inspect the factor structure of our study variables and determine discriminant validity. Detailed CFA results can be found in the online supplemental materials. For longitudinal measurement invariance analyses, we fit three measurement models (i.e., configural, metric, and strong) across the four measurement points, following recommendations by Vandenberg and Lance (2000). The differences in relative fit indices between the configural, the metric, and the strong invariance model, respectively, were below common cut-offs (Cheung & Rensvold, 2002), indicating that strong measurement invariance upheld for all study variables. Table 3 presents detailed results of our measurement invariance tests.
Measurement Invariance Tests for Focal Variables.
Hypothesis Testing
We constrained the autoregressive and cross-lagged effects to be equal over time, as the time intervals between the measurement waves were one month each, and we expected no structural changes in the relations. The constrained model fit the data well (
Summary of Relevant Between-Person Parameter Estimates.
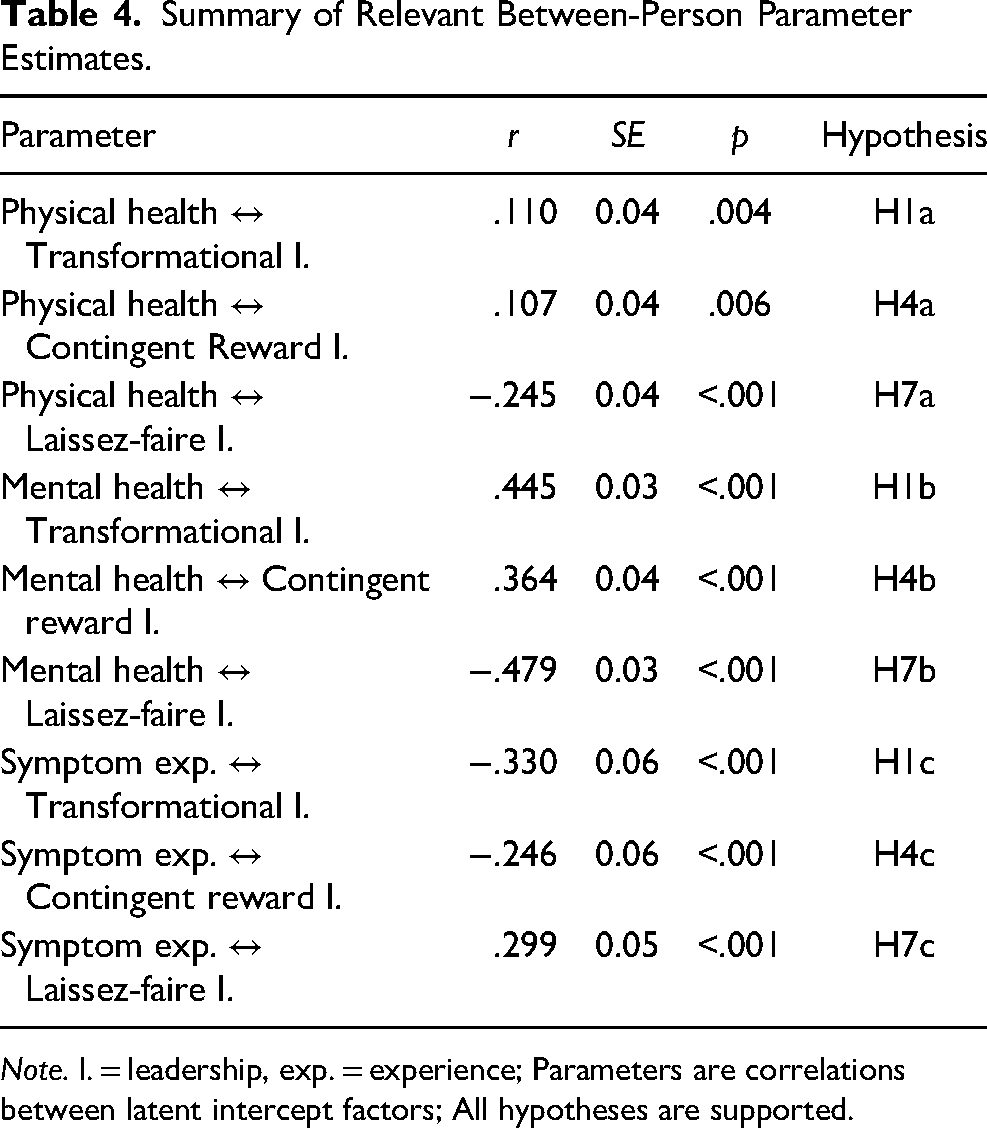
Note. l. = leadership, exp. = experience; Parameters are correlations between latent intercept factors; All hypotheses are supported.
Summary of Relevant Within-Person Parameter Estimates.
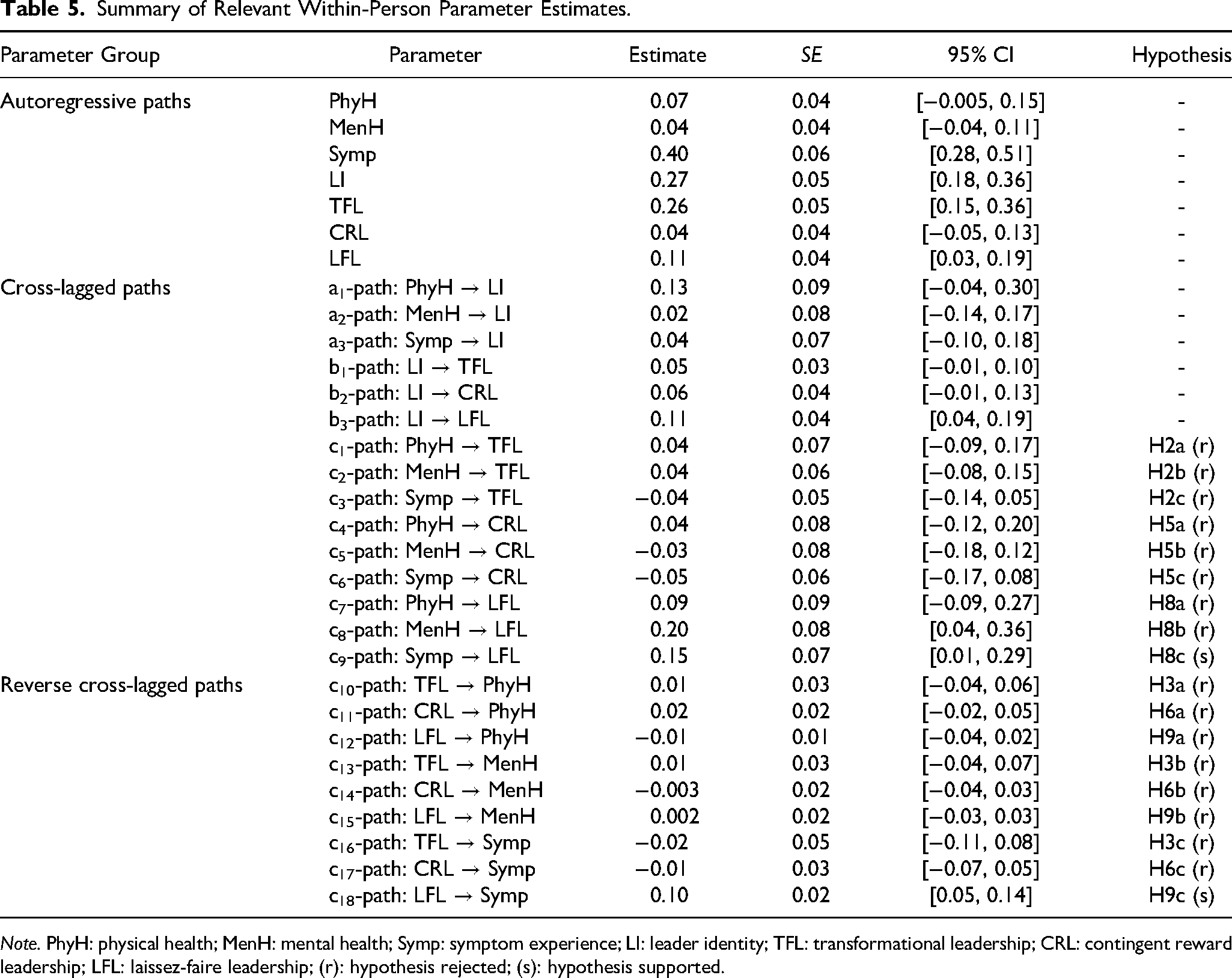
Note. PhyH: physical health; MenH: mental health; Symp: symptom experience; LI: leader identity; TFL: transformational leadership; CRL: contingent reward leadership; LFL: laissez-faire leadership; (r): hypothesis rejected; (s): hypothesis supported.
Hypotheses 1a-c predicted relations between health measures and transformational leadership at the between-person level of analysis. As hypothesized, transformational leadership was positively associated with physical health (rxy = .110, p = .004) and mental health (rxy = .445, p < .001) and negatively associated with symptom experience (rxy = −.330, p < .001). The within-person relations between health and subsequent transformational leadership (H2a-c), as well as the reversed effects (H3a-c) were not significant.
Hypotheses 4a-c predicted relations between health and contingent reward leadership at the between-person level of analysis. As hypothesized, contingent reward leadership was positively associated with physical health (rxy = .107, p = .006) and mental health (rxy = .364, p < .001), and negatively associated with symptom experience (rxy = −.246, p < .001). The within-person relations between health and subsequent contingent reward leadership (H5a-c), as well as the reversed effects (H6a-c) were not significant.
Hypotheses 7a-c predicted relations between health and laissez-faire leadership at the between-person level of analysis. As hypothesized, laissez-faire leadership was negatively associated with physical health (rxy = −.245, p < .001) and mental health (rxy = −.479, p < .001), and positively associated with symptom experience (rxy = .299, p < .001). Hypotheses 8a-c proposed within-person relations between health and subsequent laissez-faire leadership, and Hypotheses 9a-c pertained to the reversed cross-lagged relations. Contrary to Hypothesis 8b, we observed a positive relation between mental health and subsequent laissez-faire leadership (Β = .198, p = .016). Supporting Hypotheses 8c and 9c, we found positive relations between symptom experience and subsequent laissez-faire leadership (Β = .150, p = .036), as well as between laissez-faire leadership and subsequent symptom experience (Β = .097, p < .001).
Additionally, we postulated mediation effects between health and transformational (H10a-c), contingent reward (H11a-c), and laissez-faire (H12a-c) leadership via leader identity at the within-person level of analysis. None of the indirect effects via leader identity were significant, thus Hypotheses 10–12 were not supported (see Table 6 for a detailed overview of coefficients).
Summary of Within-Person Mediation Parameter Estimates.
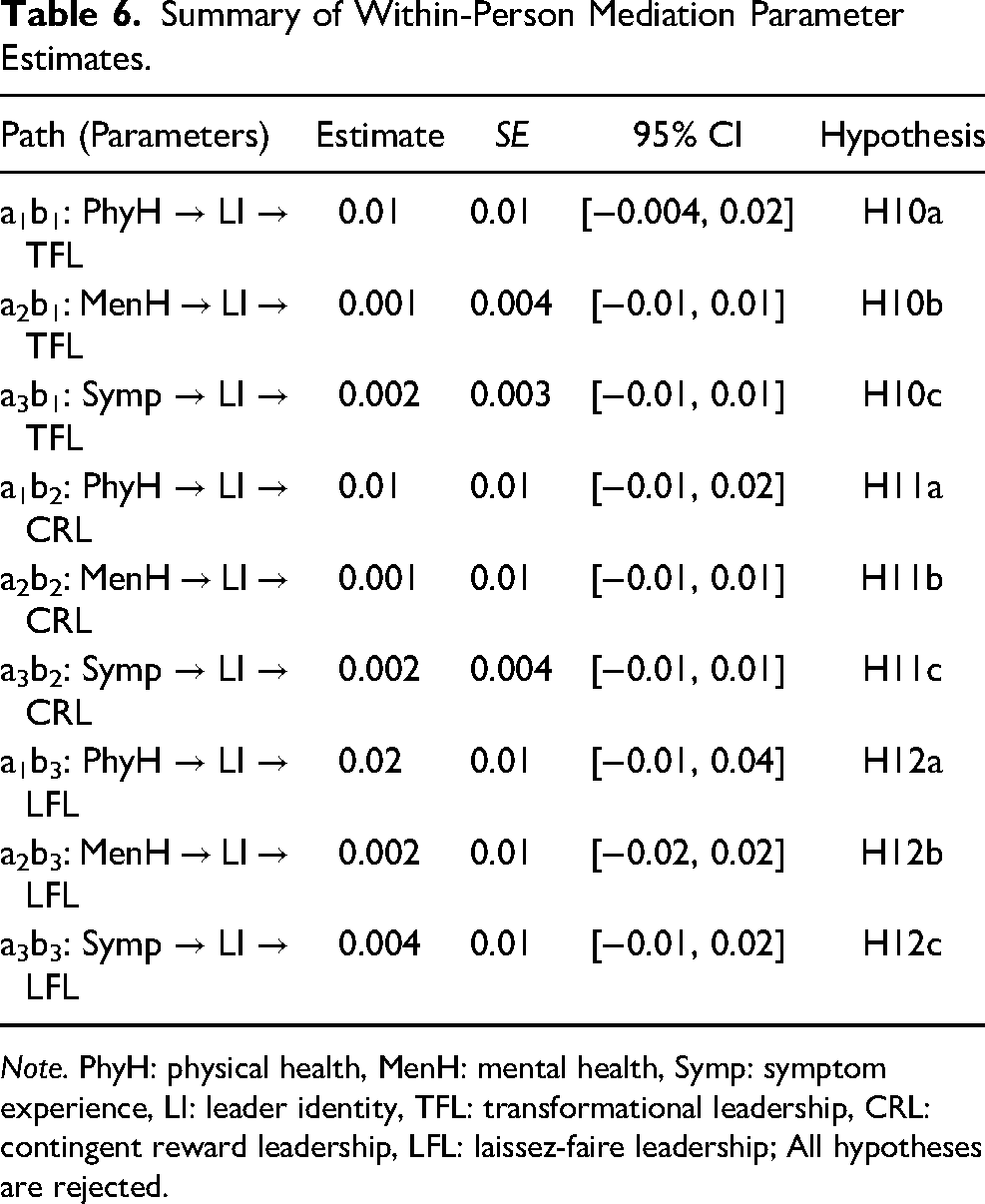
Note. PhyH: physical health, MenH: mental health, Symp: symptom experience, LI: leader identity, TFL: transformational leadership, CRL: contingent reward leadership, LFL: laissez-faire leadership; All hypotheses are rejected.
Supplemental Analysis
Research suggests small differences in the behavior of male and female leaders, such that female leaders show slightly more transformational leadership than male leaders (e.g., Eagly et al., 2003). Moreover, there are small differences in terms of perceived effectiveness, such that male leaders perceive themselves as more effective than female leaders (e.g., Paustian-Underdahl et al., 2014). Therefore, we conducted an additional analysis, in which we included sex as a time-invariant predictor of the random intercepts in the RI-CLPM. This model assumes that the effects of sex are time-invariant, affecting the observed variables indirectly through the random intercepts (Mulder & Hamaker, 2021). The results indicated baseline level differences for female and male leaders in the substantitve variables; nevertheless, all between- and within-person relations remained unchanged. Complete results are available in our online supplemental materials.
Discussion
The aim of this study was to provide insights into stable between-person and dynamic within-person relations between different forms of leader health and leadership behavior. By distinguishing between relations at the between-person and within-person levels of analysis, we contribute to a more nuanced understanding of the temporal processes involved in the relations between leader health and leadership behavior. At the between-person level of analysis, higher levels of leader health were related to more transformational and contingent reward leadership and less laissez-faire leadership. This is consistent with previous research on the between-person relations between better leader health and desirable leadership behavior (Kaluza et al., 2020).
At the within-person level, the assumed relations between leader health and leadership behavior were only partially supported. We found no evidence for within-person relations between leader health and both transformational and contingent reward leadership over time. Additionally, we found no evidence for indirect relations between leader health and leadership behavior via leader identity. However, symptom experience was positively related to next-month laissez-faire leadership, and vice versa. This finding extends cross-sectional research that found positive relations between leader stress and impaired well-being and destructive leadership behaviors (Harms et al., 2017; Kaluza et al., 2020). Specifically, the finding suggests that when leaders experience higher levels of somatic health symptoms than usual, they engage in more laissez-faire leadership in the next month, and vice versa. This reciprocal effect over time is in line with COR theory, which suggests that resource loss can trigger negative spirals, wherein resource loss begets further resource loss (Hobfoll et al., 2018). The fact that we found these within-person relations only for negative concepts (i.e., symptom experience and laissez-faire leadership), but not for positive concepts (e.g., leader health, contingent reward, and transformational leadership) is consistent with the proposition of COR theory that resource loss is more salient than resource gain (Hobfoll, 1989).
Additionally, the timeframe of one month considered in our study might explain why we found evidence for the existence of within-person loss spirals, but not for gain spirals. Research indicates that negative events and experiences tend to have longer lasting effects on individuals, because they elicit stronger reactions on a broad range of personal outcomes, such as feelings of uncertainty and perceived lack of control over the environment (Baumeister et al., 2001). Declines in health may lead to persistent feelings of uncertainty and anxiety about one's ability to fulfill leadership responsibilities, as health problems can result in losing a leadership position (Keloharju et al., 2023). In contrast, people generally adapt more quickly to positive events (Baumeister et al., 2001). As such, the positive within-person effects between leader health and constructive leadership behaviors could manifest over relatively short timeframes, but may diminish by the following month. This reasoning is consistent with daily diary research indicating that daily fluctuations in motivation and affect are associated with daily leadership behaviors (Lanaj et al., 2016; Lanaj et al., 2023).
Interestingly, we found that improved mental health was positively related to subsequent laissez-faire leadership at the within-person level. This finding challenges the principles of COR theory, which suggest that the availability of resources (i.e., leader health) facilitates resource investments to gain additional resources (Hobfoll, 2001) and not passive behaviors, such as laissez-faire leadership, which may result in resource loss. One potential explanation for this unexpected relation is moral licensing (Klotz & Bolino, 2013). Engaging in positive behaviors can grant leaders moral credit, which they may use to justify morally questionable behaviors without compromising their positive self-perception (Lin et al., 2016). Positive within-person shifts in mental health may signal to leaders that they have effectively fulfilled their leadership responsibilities. As a result, leaders may consider it justified to adopt laissez-faire leadership in the short term. Additionally, improvements in mental health might also reflect that things are going well, and leaders may feel that they can reduce their engagement (i.e., adopt laissez-faire leadership) without causing harm.
Alternatively, changes in one's personal life circumstances or other factors in the nonwork domain might influence leader health (e.g., Oc & Chintakananda, 2025) and leadership behavior (e.g., Dionisi & Barling, 2019). For example, reductions in personal stressors in the nonwork domain, such as resolving family issues, may improve leaders’ mental health. As a result, leaders might focus more on maintaining the improved conditions in their personal life, which could lead to reduced attention towards their leadership responsibilities at work, potentially contributing to higher levels of laissez-faire leadership over time. However, the negative relation between mental health and laissez-faire leadership observed at the between-person level of analysis (i.e., leaders with higher compared to those with lower levels of mental health were less likely to engage in laissez-faire leadership) might suggest that the positive within-person effects may only manifest over relatively short timeframes.
Theoretical and Practical Implications
The current study sheds light on temporal dynamics among leader health and leadership behavior. Specifically, we addressed calls for more research on dynamic processes of health and leadership, as they can unfold over shorter and longer timeframes (e.g., Inceoglu et al., 2021; Ployhart & Vandenberg, 2010). Leader health, symptom experience, and leadership behavior exhibited considerable within-person variability across one-month timespans. These monthly experiences capture dynamics that go beyond daily and weekly relations (e.g., Lanaj et al., 2021; Lanaj et al., 2023; Lin et al., 2019), indicating that leader resources and behavior fluctuate over longer time periods. As suggested by COR theory, the mutual reinforcement between symptom experience and laissez-faire leadership (i.e., increases in somatic symptoms and laissez-faire leadership) may suggest an accumulation of resource loss over time, which makes it difficult to break this adverse cycle.
Furthermore, the findings contribute to research on leader identity. Research suggests that leader identity evolves over longer periods of time (DeRue & Ashford, 2010; Hammond et al., 2017) and exhibits daily fluctuations that influence daily leadership behaviors (Lanaj et al., 2021; Lanaj et al., 2023). The relatively low within-person variability in leader identity found in our study suggests that monthly assessments may reflect more stable, longer-term evaluations rather than dynamic, shorter-term activations of leader identity. The impact of leader identity on work experiences and behaviors may primarily manifest through short-term (e.g., daily) activations (e.g., Lanaj et al., 2023), whereas monthly leader identity may require significant events (e.g., job changes) to change noticeably (Miscenko et al., 2017; Nieberle et al., 2024). Therefore, we recommend that research and practical measures on leader identity distinguish more clearly between the processes of forming and activating leader identity.
Considering practical implications, the findings suggest that leaders and organizations should prioritize leader health in leader development efforts. Healthier leaders are not only more likely to engage in transformational and contingent reward leadership compared to less healthy leaders, but they are probably less susceptible to experiencing within-person fluctuations in symptoms and loss spirals with laissez-faire leadership. Laissez-faire leadership may have an initial appeal to leaders because such behaviors require minimal personal resources. However, laissez-faire leadership can have detrimental effects on followers (e.g., Klasmeier et al., 2022) and, as our findings illustrate, on leaders themselves by deteriorating their health. When experiencing health issues, leaders should consider the potential long-term consequences of engaging in laissez-faire leadership behavior to prevent that laissez-faire leadership exacerbates their health problems over time. Organizations should provide leaders with additional support during times of health declines, as managing limitations and threats to their role execution can be challenging without assistance. As a preventive measure, organizations can implement targeted programs for leaders to develop their skills and identity (Miscenko et al., 2017). These programs should focus on helping leaders maintain their ability to meet role expectations and developing a functional view on their leader identity, which can support their effectiveness and health in the long-term.
Limitations and Future Research
Despite its strengths (e.g., multiple indicators of health and leadership, longitudinal design, and large sample of leaders), this study also has several limitations that should be addressed in future research. First, we collected self-reports of leader health, leader identity, and leadership behavior, which may be subject to response bias, as participants might present themselves in a more favorable light (Podsakoff et al., 2024). However, health and identity are internal states, which involve subjective experiences that are not directly observable by others (Arnold et al., 2017; Miscenko et al., 2017). Moreover, leadership encompasses multiple situations. Followers may only observe fragments of leadership behavior, and their perceptions can be biased by their overall evaluation of the leader (Hansbrough et al., 2015). Nonetheless, future studies should compare reports of leaders and followers to provide insights into which health fluctuations in leaders are noticeable and relevant for others.
Second, the timing of data collection may have influenced the relations. The study was conducted between August and November 2022, during the ongoing COVID-19 pandemic. Even though shocks to leadership behavior occurred only at the first lockdown in 2020 (Garretsen et al., 2024) and the general preference for healthy leaders remained the same during COVID-19 (Laustsen & Olsen, 2022), it is possible that we observed increased variability in some variables (Zacher & Rudolph, 2022). For example, leaders may have been sensitized to health-related topics and experienced more health fluctuations due to the anticipated winter wave of COVID-19 infections. However, it is unlikely that these conditions led to fundamental changes in the relations between leader health and leadership behavior, as many of our findings were consistent with previous research.
Additionally, the monthly time lags may have influenced the within-person results, as within-person variability and relations can differ substantially across different timeframes (Dalal et al., 2020). The retrospective evaluations of health, leader identity, and leadership behavior in the previous month may have averaged out some dynamics, potentially reducing the within-person variability and effects compared to shorter time intervals (e.g., Lanaj et al., 2023; Poethke et al., 2022). Also, the generally acceptable, but partly low within-person reliability coefficients observed in our study are noteworthy. Although standards for within-person reliability tend to be lower compared to between-person reliability (e.g., Yang et al., 2022), the low within-person reliabilities for some variables (physical and mental health and contingent reward and laissez-faire leadership) may have limited our ability to detect effects at the within-person level of analysis. Future studies should consider and compare different timeframes. Shorter time lags (e.g., weekly measurements) could reduce retrospective bias and capture more immediate links between leader health, leader identity, and leadership behavior (Dormann & Griffin, 2015). Longer time intervals may provide insights into trajectories of leader health and leader identity over time and their relations with indicators of effective leadership (e.g., follower attitudes and performance) beyond specific leadership behaviors.
Third, several correlations among the study variables are noteworthy. Specifically, transformational and contingent reward leadership were highly correlated at the between-person level of analysis (r = .89), indicating conceptual overlap between them. This is consistent with theoretical arguments that contingent reward leadership forms the foundation for cooperating with followers and motivating their task performance, potentially enabling the positive impact of transformational leadership (Judge & Piccolo, 2004; Wang et al., 2011). By including both constructs together in the analysis, we accounted for their shared variance. Additionally, the lower within-person correlation (r = .67) suggests that, despite their overlap, each construct also has distinct characteristics and relations with other variables.
Furthermore, we found a negative within-person correlation between physical and mental health (r = −.17) and a positive association at the between-person level (r = .32). This pattern is common in research using the SF-12v2 (e.g., Huo et al., 2018; Kleine et al., 2023). It is possible that declines in one health domain may shift the individual focus to more positive aspects of the other domain as a coping mechanism. Future research may use different measures and specific health scales to replicate our findings and identify the most important health dimensions for leaders.
Finally, future studies could examine how personal characteristics, and contextual factors interact with leader health in shaping leadership behavior. For instance, career aspirations and additional roles (e.g., middle management responsibilities) may conflict with leader obligations (Anglin et al., 2022), thereby exacerbating potential adverse effects between health problems and leadership behavior. Conversely, external resources, such as support, autonomy, and role clarity, may allow leaders to manage health problems more effectively, likely decreasing the extent to which leader health influences leadership behavior. Additionally, future research could examine the role of broader cultural factors or societal norms in which leadership is embedded (Oc & Chintakananda, 2025), as these factors may moderate the relations between leader health and leadership. This may occur because cultural differences exist in perceptions of what constitutes an effective leader (e.g., Lord et al., 2020). It would be interesting to understand whether good health is universally attributed to leaders or whether its relative importance compared to other characteristics differs across cultures. Overall, considering more complex resource configurations and contextual factors might also help identify explanatory mechanisms for the relations between leader health and leadership behavior.
Conclusion
Drawing from COR theory, this study examined relations between leader health and leadership behavior at the between- and within-person level of analyses. Additionally, we complemented the resource-based perspective of COR theory with propositions of role theory to explore leader identity as potential mediator of the within-person relations between leader health and leadership behavior. Based on four-wave longitudinal data collected among leaders in Germany, we found that leaders with higher levels of health were more likely to engage in transformational and contingent reward leadership and less likely to engage in laissez-faire leadership compared to leaders with lower levels of health. At the within-person level, we found only partial support for the assumed dynamics. Consistent with the notion of resource loss spirals, we found that when leaders experienced higher levels of somatic symptoms than usual, they subsequently engaged in more laissez-faire leadership, and vice versa. Overall, the findings advance the understanding of the temporal processes involved in leader health and leadership behavior and hopefully encourage future research to consider the dynamic within-person relations among these constructs in greater depth.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection for this research was funded by the German Federal Ministry of Labor and Social Affairs, the European Social Fund, and adjuvant through the Federal State of Saxony represented by the Saxon State Ministry of Economy, Labor, and Transportation.
Ethical Approval and Informed Consent Statements
In accordance with national regulations by the German Science Foundation, obtaining ethical approval from an ethics committee was not required for this study. Participation in the study was voluntary, with informed written consent obtained from participants. Data were collected and processed anonymously.