
Abstract
Background
Postural instability is a common observation after concussions, with balance assessments playing a crucial role in clinical evaluations. Widely used post-concussion balance tests focus primarily on static and dynamic balance, excluding the critical aspect of reactive balance.
Objectives
This study investigated the acute and longitudinal effects of concussion on reactive balance in collegiate athletes.
Methods
Concussed and healthy matched controls NCAA division I athletes were assessed at pre-season baseline and 4 post-concussion timepoints: acute, pre-return-to-play (RTP), post-RTP, and 6 months post-concussion. The instrumented-modified Push and Release test measured reactive balance during single- and dual-task conditions. Longitudinal effects of concussions on time to stability and step latency metrics were investigated applying Generalized Estimating Equations.
Results
Acutely after concussion, athletes demonstrated impaired reactive balance, indicated by longer times to stability, in dual-task conditions (P = .004). These acute impairments were transient and recovered over time. Exploratory analyses revealed that athletes who sustained their first lifetime concussion exhibited both acute (P = .037) and longitudinal (P = .004 at post-RTP) impairments in single- and dual-task compared to controls with no lifetime concussion.
Conclusions
This comprehensive evaluation provides insights into the multifaceted nature of post-concussion impairments and emphasizes the importance of considering cognitive demand and history of concussions in assessing athletes’ balance.
Introduction
Postural instability is frequently observed after concussion, 1 highlighting the pivotal role of balance tests in clinical evaluations. A comprehensive understanding of balance includes an individuals’ ability to stand, move, react, and engage with their surroundings.2,3 These factors manifest within 3 domains of balance: static balance, dynamic balance, and reactive balance. 4 However, post-concussion balance assessments focus on static and/or dynamic balance and offer little to no information about reactive balance. 3 Reactive balance, which encompasses postural responses to unpredictable disturbances to restore stability, 5 is particularly important for adapting to complex environments. 6 Given its association with prospective musculoskeletal injuries in athletes, 7 there is a need to understand the acute and longitudinal effects of concussions on reactive balance.
Reactive balance relies on interactions among spinal circuits, the brainstem, and the cerebral cortex 8 to coordinate responses to sudden unexpected alterations in the base of support or center of mass kinematics. In contrast to static and dynamic balance tasks that rely mainly on the integration of sensory inputs and motor responses through cortico-cerebellar-basal ganglia circuits to regulate a continuous postural or cyclic stepping (ie, walking) task,8,9 reactive balance is initiated faster than voluntary movement by short-latency activations at the spinal cord and brainstem level, and leaves little time for iterative corrections.4,10 Additionally, reactive balance responses can be primed in advance of the perturbation based on adaptation and triggered (ie, executed) promptly upon a loss of balance. 11 This priming involves cognitive resources, 10 although metrics of reactive balance are independent from computerized cognitive tests, clinical measures of reaction time, and metrics of static and dynamic balance commonly used in concussion evaluations. 12 Consequently, reactive balance is distinct dimension that remains independent of these conventional clinical metrics.
Limited prior work on reactive balance post-concussion has investigated effects of chronic concussion (ie, mild traumatic brain injury). 4 Pan et al 13 provided preliminary evidence that individuals experiencing persistent symptoms after concussion exhibit impaired reactive balance in response to a waist-pull perturbation. However, these deficits were evident only among people with ongoing symptoms of disequilibrium at various chronicity, spanning from 7 months to 7 years; asymptomatic individuals with a history of concussion did not display reactive balance impairments. The heterogeneous time since injury complicates our understanding of reactive balance post-concussion, including the acute and time-varying recovery of reactive balance.
Therefore, the purpose of this study was to assess the acute and longitudinal effects of concussion on reactive balance. We hypothesized that (H1a) athletes with acute concussion will take longer to regain balance during reactive balance tasks and (H1b) will display larger deficits in reactive balance during dual-tasks compared to healthy controls; (H2) athletes with a recent concussion will improve reactive balance throughout the assessments, but will still demonstrate persistent longitudinal deficits compared to the controls.
Materials and Methods
Participants
The study recruited NCAA Division I student-athletes currently enrolled at the University of Utah aged between 18 and 30 years. All eligible subjects were included, irrespective of their sex, gender, race/ethnicity, cultural background, or socioeconomic status. Exclusion criteria disqualified individuals that had a concussion within the past year prior to their enrollment, lower extremity surgeries within the previous 2 years, planned surgeries that would affect their ability to participate in their sport, or a documented history of vestibular or somatosensory pathology. All participants provided written informed consent in accordance with a protocol approved by the Institutional Review Board.
All concussions were diagnosed by a team physician following the latest consensus statement on concussion in sport 14 and reported to the study team by the team’s athletic trainer(s). Concussions were included regardless of the mechanism of injury or the specific context in which they occurred. The team’s athletic trainer recommended control subjects among the concussion subject’s teammates, matched by sex, age, playing position, and skill level (in order of decreasing priority). Skill level was determined by athletes’ competitive experience and depth chart position (eg, starter, minutes played, and race time), ensuring concussed and control participants were closely matched in athletic performance and training exposure. Matched controls were required to meet the same exclusion criteria as the concussed athletes, including: no concussion within the past year, no lower extremity surgeries in the past 2 years or planned surgeries, and no history of vestibular or somatosensory pathology. Additionally, controls were required to be uninjured and fully cleared for participation without any restrictions at the time of enrollment. Demographic data (age, sex, race, ethnicity, height, weight, and body mass index), athletic activities (eg, sport), lower extremity injury history, and self-reported lifetime concussion history were collected before completing any balance assessment.
Participants completed testing up to 5 times: at the start of intercollegiate competition at the University of Utah, typically as a freshman or upon arriving on campus as a transfer (Baseline); within 72 hours after a concussion (Acute); within 72 hours of beginning the return-to-play (RTP) protocol (Asymptomatic/Pre-RTP); within 72 hours of being cleared for unrestricted return to competition (Post-RTP); and 6 months after the initial injury (6 months). The RTP protocol followed the guidelines set by the Berlin Consensus Statement on Concussion in Sport. 14 Control participants were tested on the same schedule as their matched concussion. Notably, not every participant was present at each of the scheduled assessment timepoints due to scheduling conflicts and referral delays. Baseline assessments were conducted during summer-fall 2019, 2021, and 2022, while concussions and matched controls evaluations and follow-ups spanning from fall 2019 through fall 2023. Due to coronavirus disease 2019 (COVID-19) restrictions, 6-month follow-up visits could not be completed for athletes with concussions prior to March 2020. Our enrollment goal was 40 participants per group at each timepoint based on a previously published power analysis. 15
Instrumented Balance Assessments and Measured Outcomes
All procedures were part of a pre-registered protocol. 15 Testing was conducted in an athletic training room setting. Athletes completed all tasks in shoes; if athletes did not wear shoes to testing (eg, they wore sandals), testing was completed in socks or barefoot.
Participants wore 5 inertial measurement units (Opals v2; APDM Inc., Portland, OR) throughout the balance assessments. Sensors, sampling at 128 Hz, were located on the dorsum of the athlete’s left and right feet, on the anterior shank, the lumbar region of the spine (~L3/L4), and the mid-point of the sternum.
Reactive balance was assessed with the instrumented-modified Push and Release16-18 (I-mP&R). Participants performed 4 directions (forward, backward, left, and right) in both a single-task condition and a dual-task condition, for a total of 8 trials.15,16 Each participant was randomized to complete the single- or dual-task condition first. The direction order was constant for all timepoints. The dual-tasks included serial subtraction by 3’s, reciting the alphabet by every other letter, FAS verbal fluency test, 19 and categories (animals, fruit). Cognitive task performance was not recorded.
Raw kinematic data were processed through custom algorithms in MATLAB (r2023b; MathWorks, Natick, MA, USA). The primary outcome from the I-mP&R 16 was time to stability, defined as the time from release of support (t0), to stabilization. The secondary outcome was step latency, and tertiary exploratory outcomes included normalized step length, and time to first contact 15 (see Supplemental S1 for calculation details). To maximize reliability, summary metrics of the I-mP&R across all 4 directions were used. These summary metrics were the median time to stability, maximum step latency, median time to first contact, and median step length. 16
Statistical Analysis
Statistical analysis was performed with RStudio (2023.12.0 Build 369; Rstudio Team, 2020, Boston, MA, USA). Following the pre-registered procedure, 15 unadjusted comparisons were conducted using 2 sample t-tests with Bonferroni adjustments (5 timepoints; significance level = 0.05/5) to determine differences between concussed and control subjects at each timepoint. Such results are presented in the supplement (Supplemental S2).
Considering the non-uniform attendance of participants, the primary analysis implemented Generalized Estimating Equations (GEEs), which account for random missing data, 20 to evaluate the acute and longitudinal effects of concussion on reactive balance. GEEs were defined for time to stability and latency. Fixed effects variables were the assessment timepoint (Baseline, Acute, Pre-RTP, Post-RTP, and 6 months), group (concussion and control), and task (single-task and dual-task), as well as their 2-and 3-way interactions. Retaining significant interactions at the 0.10 level, the final GEE model included 2-way group interactions with assessment (group × assessment timepoint) and task (group × task). All models were also adjusted for covariates of age, sex, height, type of sport (contact or non-contact), and footwear worn during the testing (shoes, barefoot, and socks). 21 Post hoc pair-wise contrasts compared concussion and control groups at each timepoint when adjusting for covariates.
Following visual inspection of the results, an exploratory post-hoc analysis stratified participants by concussion history to explore potential differences in how lifetime concussion history affected the acute and longitudinal response to a new concussion (ie, the enrollment concussion). GEE models with equivalent fixed effects variables (assessment timepoint, group, and task), 2-way interactions (group × assessment timepoint and group × task), and covariates (age, sex, height, type of sport, and footwear) were defined for athletes enrolled into the concussion and control groups, stratified by their lifetime history of concussion before enrollment (or the concussion event that lead to enrollment).
To further investigate potential mechanisms underlying differences in our primary outcomes, the relationship between primary and secondary I-mP&R metrics of time to stability and step latency were evaluated using linear regression models and the coefficient of determination, R2, for single- and dual-task, in concussed and control groups. A.05 significance level was used for all GEE models and exploratory analyses.
Results
Overall, 91 athletes were enrolled (47 concussed athletes and 44 healthy teammate controls). Not every subject could be present at all timepoints, with comparable missing data between concussed athletes and matched controls (Table 1). High rates of lost to follow up at the 6 months timepoint were attributable to COVID-19 pandemic. Groups were overall similar in distribution of sex, age, height, mass, and participation in contact sports. Across timepoints, more than half of the athletes enrolled in the concussion group (59.6%) had a history of previous concussions defined as at least 1 lifetime concussion in addition to their enrollment concussion, and 45.5% control subjects had history of previous concussions prior to enrollment.
Demographics and Characteristics of the Population Involved.
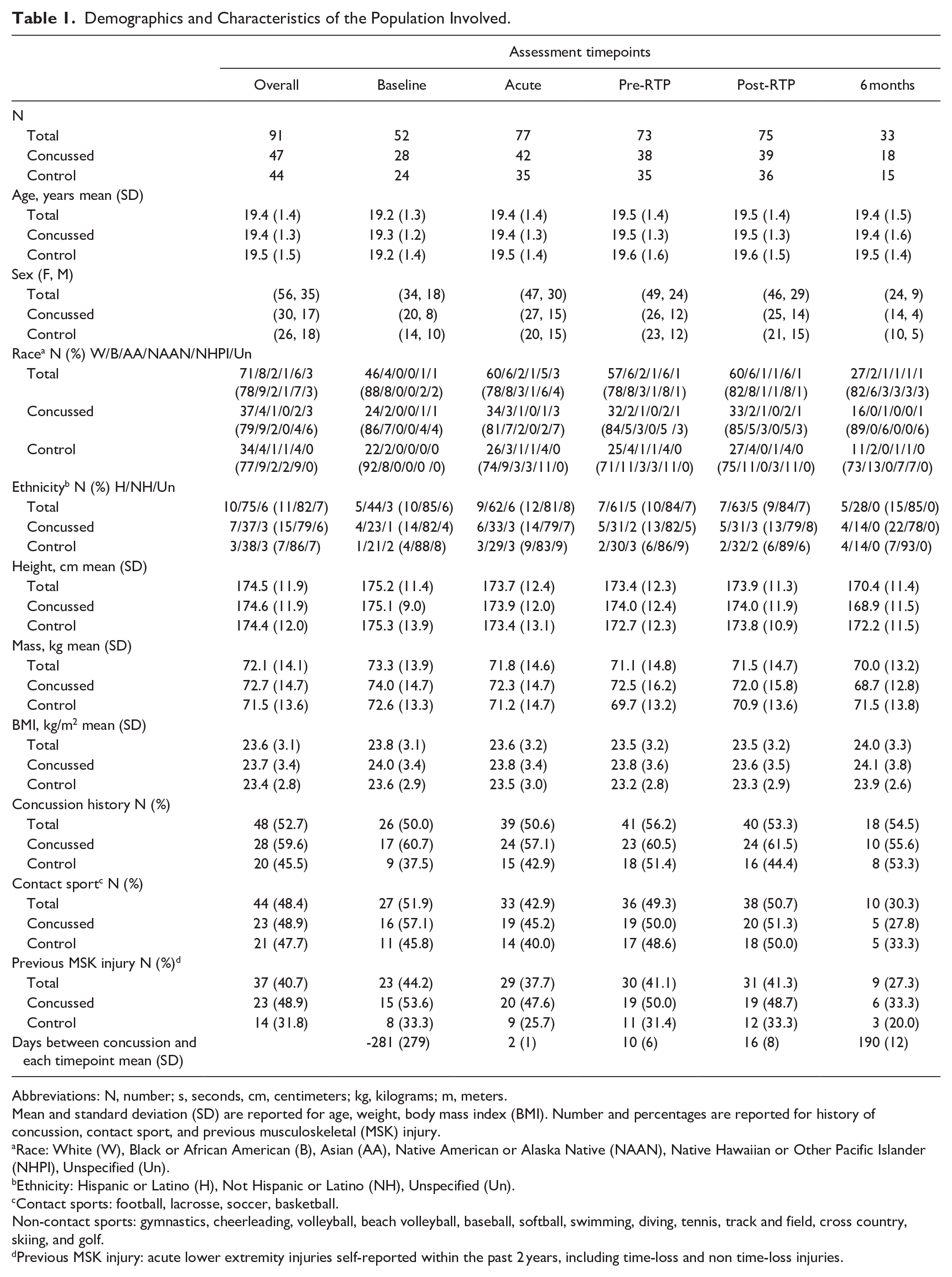
Abbreviations: N, number; s, seconds, cm, centimeters; kg, kilograms; m, meters.
Mean and standard deviation (SD) are reported for age, weight, body mass index (BMI). Number and percentages are reported for history of concussion, contact sport, and previous musculoskeletal (MSK) injury.
Race: White (W), Black or African American (B), Asian (AA), Native American or Alaska Native (NAAN), Native Hawaiian or Other Pacific Islander (NHPI), Unspecified (Un).
Ethnicity: Hispanic or Latino (H), Not Hispanic or Latino (NH), Unspecified (Un).
Contact sports: football, lacrosse, soccer, basketball.
Non-contact sports: gymnastics, cheerleading, volleyball, beach volleyball, baseball, softball, swimming, diving, tennis, track and field, cross country, skiing, and golf.
Previous MSK injury: acute lower extremity injuries self-reported within the past 2 years, including time-loss and non time-loss injuries.
To enhance clarity and streamline the discussion, results discussed refer solely to GEE models, emphasis is placed on primary and secondary outcomes of time to stability and step latency. Summary statistics of these I-mP&R reactive balance outcomes are reported in Table 2. Two sample t-tests with Bonferroni adjustments and Cohen’s d effect size with 95% confidence are reported in the Supplemental Material, as well as GEE results for time to first foot contact and step length (Table S2).
I-mP&R Reactive Balance Outcomes of Time to Stability and Step Latency.
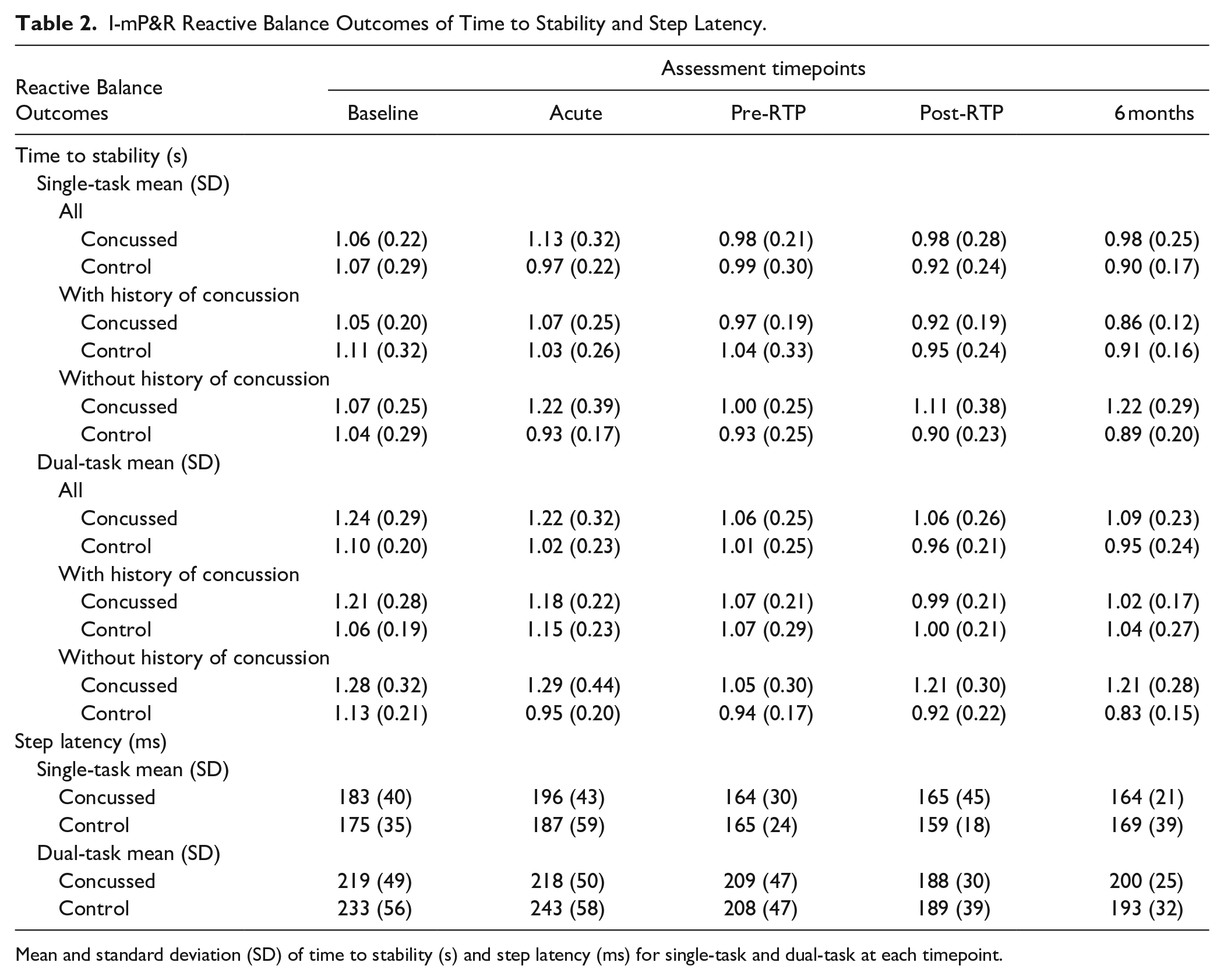
Mean and standard deviation (SD) of time to stability (s) and step latency (ms) for single-task and dual-task at each timepoint.
Time to Stability
Athletes with a recent concussion had longer time to stability than healthy controls (Figure 1). When adjusting for covariates using the GEE framework (Supplemental Table S3), a main effect of task (P = .012) and a group × task interaction (P = .013) indicated both groups exhibited longer time to stability (ie, worse reactive balance) in the dual-task condition, with the concussion group exhibiting greater increases in time to stability across tasks (Figure 1). Pair-wise contrasts at each time indicated significant group differences at the Acute timepoint for dual-task time to stability (P = .004), where the concussion group exhibited longer time to stability compared to the control group. There were no other significant differences when adjusting for covariates for single-task (Baseline P = .940; Acute P = .051; Pre-RTP P = .643; Post-RTP P = .493; 6 months P = .401) or dual-task (Baseline P = .390; Pre-RTP P = .613; Post-RTP P = .097; 6 months P = .121).
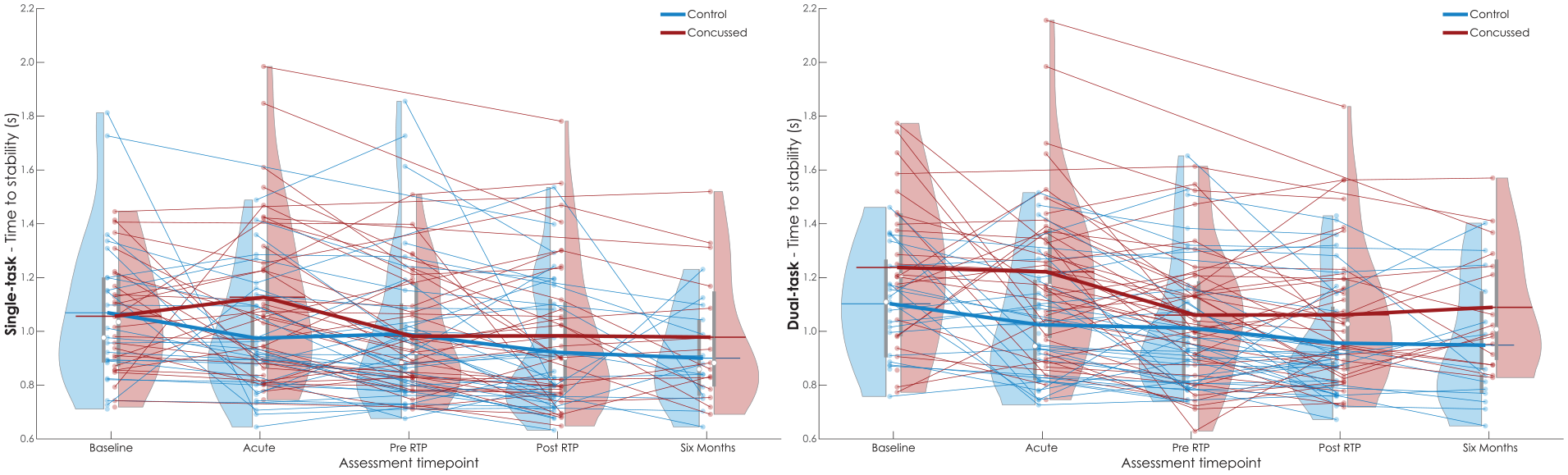
Time to stability (s) for single-task (left) and dual-task (right) I-mP&R at each assessment timepoint for concussed (red) and control (blue) subjects. Violin plot reports data distribution, mean (white circle), and interquartile range (gray box). Results of each subject relate with semi-transparent lines; thick lines link the averages of each distribution.
Stratifying by history of concussion (Figure 2) and adjusting for covariates in a GEE framework (Supplemental Table S4), athletes sustaining their first lifetime concussion (ie, athletes in the concussion group without a prior history of concussion before the enrollment concussion) exhibited longer times to stability single-task time to stability at the Post-RTP timepoint (P = .035), and longer dual-task times to stability at Acute (P = .037) and Post-RTP (P = .004) timepoints compared to athletes with no lifetime history of concussion enrolled in the study as controls (Figure 2). Notable, but non-significant effects were also observed at 6 months for both single-task (P = .073) and dual-task (P = .054). No differences were observed between the concussion and control athletes with a lifetime history of concussion before enrollment (all P > .414).
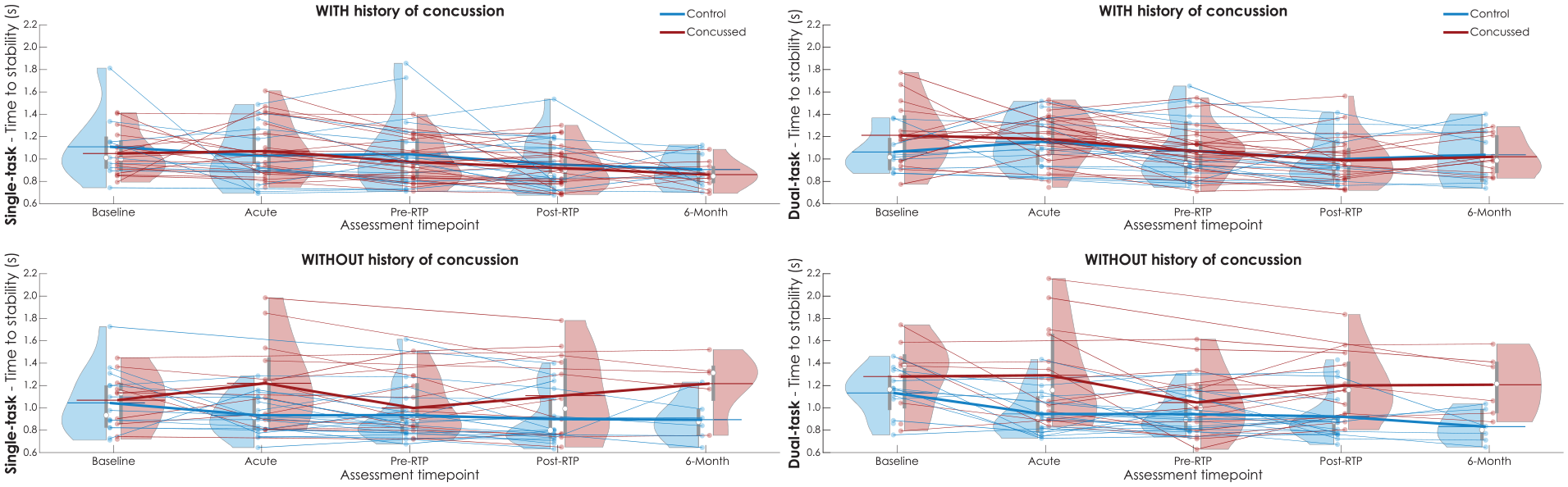
Time to stability (s) for single-task (left) and dual-task (right) I-mP&R stratified by history of concussion prior to enrollment, at each assessment timepoint for concussed (red) and control (blue) subjects. Violin plot reports data distribution, mean (white circle), and interquartile range (gray box). Results of each subject relate with semi-transparent lines; thick lines link the averages of each distribution.
Step Latency
No statistically significant group differences in latency were observed when adjusting for covariates in the GEE framework (Supplemental Table S3) for single-task (Supplemental Figure S1) or dual-task conditions (Supplemental Figure S2; P > .128 at all timepoints). A main effect of task was observed (P < .001), where latency was longer in dual-task conditions compared to single-task conditions, but there was no significant group × task interaction (P = .160).
Time to Stability Versus Step Latency
There was no significant relationship between time to stability and step latency in any group or condition at the Acute timepoint (Figure 3). Linear relationships ranged from R2 = .005 for controls during dual-task conditions to R2 = .091 for controls during single-task.
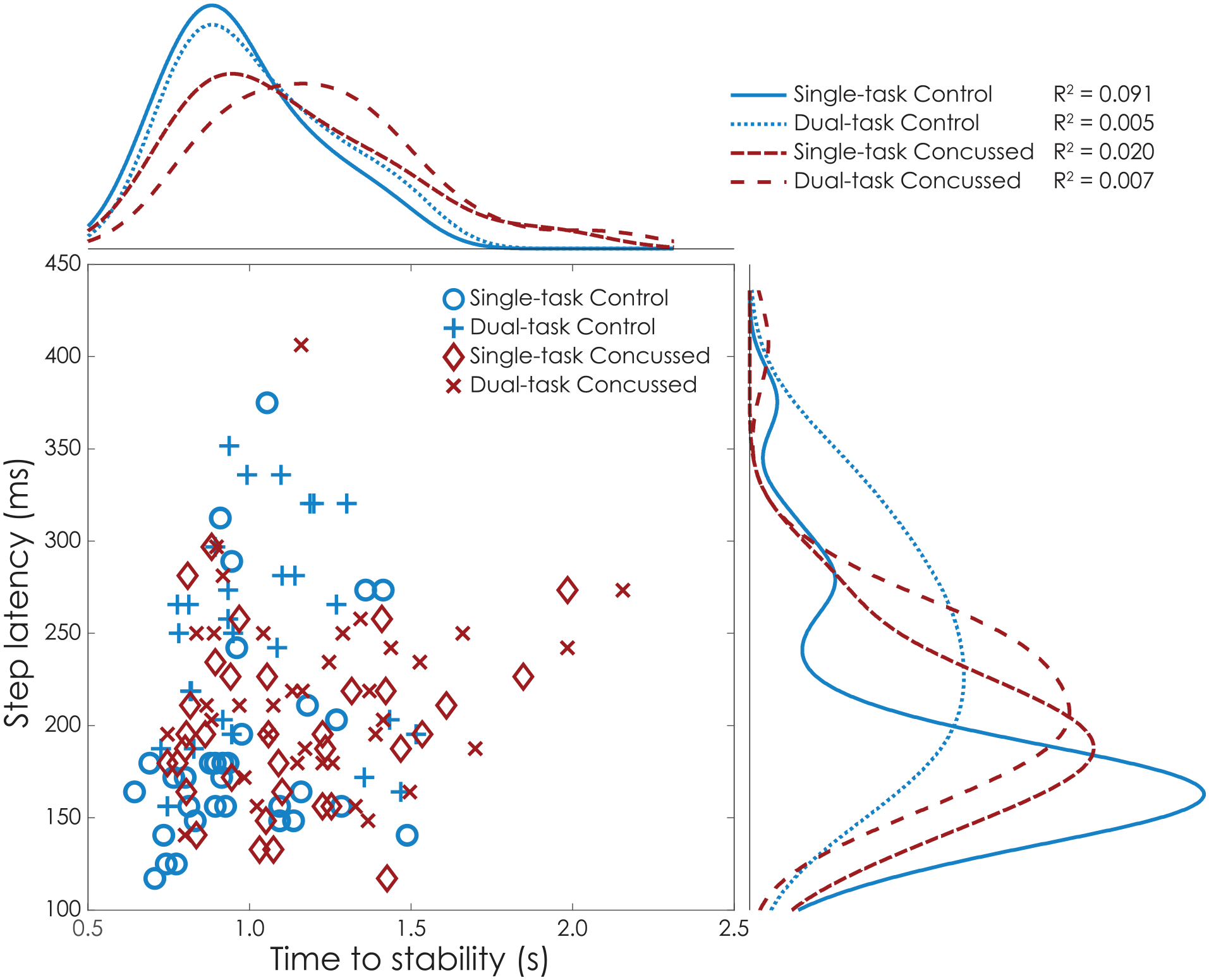
Scatter histogram of the relationship between time to stability (s) and step latency (ms) at acute timepoint, for single- and dual-task, for concussed (red) and control (blue) groups. Kernel density plots of the distributions are reported on the right and top of the graph for time to stability and latency, respectively. Overall latency does not associate with time to stability (R2 regression coefficients). The control group increased step latency (blue curves on the right) between single- and dual-task, with no effect on time to stability (blue curves on the top). The concussed group exibited faster response (step latency) than healty controls in dual-task (curves on the right), while also exhibiting longer time to stabilization (red curves on the top).
Discussion
This study explored the acute and longitudinal effects of concussion on reactive balance in collegiate athletes. Acutely after concussion (ie, <72 hours), athletes exhibited impaired reactive balance compared to normative values, 21 characterized by longer times to stability in dual-task conditions. We observed no group differences in time to stability at baseline, providing strong evidence that the slower time to stabilities at post-concussion timepoints were associated with the concussion injury. When further adjusting for demographic (age, sex, height, and sport type) and test-specific covariates (footwear), we still observed acute impairments in dual-task reactive balance. In contrast with studies of dual-task gait after concussion,22,23 reactive balance impairments resolved with the resolution of symptoms and were not detected in asymptomatic athletes. Athletes did not exhibit longitudinal group differences at assessments outside the Acute timepoint. However, we observed different effects of concussion on reactive balance based on one’s lifetime history of concussion; athletes who suffered their first lifetime concussion exhibited acute and longitudinal impairments in both single- and dual-task reactive balance compared to their peers with no lifetime concussion.
Dual-task performance differences between concussed and control athletes align with previous studies emphasizing the importance of attentional resources in managing cognitive and motor demands. 24 The link between cognitive processing and postural stability is challenged during dual-task scenarios, 10 where simultaneous engagement strains attentional capacity, affecting performance. 25 Dual-task paradigms have also proven to be more effective in challenging athletes, possibly explaining the differences that were observed exclusively in dual-task conditions rather than single-task situations. Dual-task impairments can also be clinically relevant to athlete health. Worsening dual-task gait is associated with musculoskeletal injuries in athletes returning after concussion, 26 and slower dual-task time to stability is associated with an increased risk of acute, lower extremity musculoskeletal injury in otherwise healthy athletes. 7 Specifically, a 250 ms increase in dual-task time to stability is associated with a 36% increase in acute musculoskeletal injury risk. The between-group differences observed at the acute timepoint (Acute difference = 0.20), and in our exploratory analysis between concussed and control athletes without a prior history of concussion (Post-RTP difference = 0.29 s; 6 months difference = 0.38 s) approach or exceed these clinically-meaningful effects. Nonetheless, the longitudinal changes in reactive balance fall below prior work on minimal detectable change, 21 and the lack of significant longitudinal differences in reactive balance metrics between concussed and control group contrasts with post-concussion dual-task gait differences observed in asymptomatic athletes up to 2 months post-injury. 27 These different results suggest concussion may impact the different balance control mechanisms for static, dynamic, and reactive balance in unique ways.
The differences between groups at the acute timepoint were not solely due to a regression, relative to baseline, in reactive balance performance in the concussion group—deficits appeared to be driven by the concussion group getting slower and the control group getting faster relative to baseline. Such improvements in the control group across time may indicate learning and adaptation effects commonly observed in assessments of reactive balance.28,29 Considering the time from baseline to acute timepoints (mean 281 days), such improvements in controls may also reflect changes in motor function—including reactive balance—through balance, strength, and conditioning training integrated into collegiate programs. In contrast to controls, athletes with concussion did not exhibit improved performance relative to baseline until they were asymptomatic (Pre-RTP timepoint). These findings suggest concussions may have repercussions on postural adaptation and motor learning.30,31
While the mechanisms underlying the acute post-concussion deficits in reactive balance remain unclear, it is unlikely that reaction time is an underlying cause. Slower reaction times are well-documented after concussion using both computerized neurocognitive testing and clinical drop-stick tests. 32 Yet, these traditional measures of reaction time are not associated with postural reaction times12,21 (eg, step latency). We did not observe differences in step latency across groups at any timepoint, and there were negligible associations between step latency and time to stability. Further, a notable but non-significant interaction, was evident where athletes with acute concussion exhibited slower time to stability, yet faster step latencies, in the dual-task condition compared to their healthy teammates. Combined, such results across time and (lack of) associations with step latency suggest post-concussion reactive balance impairments may be associated with altered trans-cortical loops, rather than short- or medium-latency responses. Altered long-latency trans-cortical responses may be influenced by an inability to appropriately prime a stepping response before the release 33 or an inappropriate motor response, driven by altered sensory integration and state estimation, after a loss of balance.13,34 However, such conclusions remain speculative and further research is needed to uncover the mechanisms underlying concussion-related reactive balance impairments.
Stratifying time to stability by concussion history indicated that acute reactive balance impairments may be influenced by one’s lifetime concussion history. Athletes without a history of concussion showed better performance acutely and, for dual-task, at Post-RTP and 6 months. While comparisons across the 4 groups were omitted due to insufficient statistical power, descriptive comparisons revealed that athletes in the control group, who did not experience any lifetime concussions, exhibited the fastest time to stability amongst all groups. Combined with the lack of differences between concussion and control groups with a history of concussion, these results encourage future research on potential chronic effects of the first lifetime concussion (ie, concussion history) on reactive balance.
The primary limitation of the presented study is the non-uniform attendance at each assessment, potentially introducing bias from fluctuating sample sizes. While the pre-registered protocol did not originally include baseline measurements, we opted to include such data in for the subset of participants for which it was available. Rather than excluding timepoints with missing data, we opted to include all data for each timepoint and treat missing data as missing without imputation. Further, the GEE model is advantageous for handling missing data, assuming completely at random missing data mechanism, allowing for a robust analysis of longitudinal observations. 20 It is possible that individuals exhibited different prioritization between cognitive and motor tasks during the dual-task conditions. Prior work has indicated that attention is focused on the cognitive task before a perturbation, but attention shifts to prioritizing postural stabilization over the cognitive task once stability is compromised (ie, the onset of the perturbation/loss of balance).10,35 Capturing this task prioritization would have required neurophysiological recordings or continuous tracking tasks due to the short, discrete nature of the reactive balance response. While we opted to maintain clinically-feasible cognitive tasks and instrumentation, future work should consider neurophysiological responses to reactive balance under single- and dual-task conditions after concussion. Additionally, noisy assessment environments and inter-administrator variability may have affected the results. 36 However, these reflect the settings for clinical concussion assessments, and a previous investigation reported moderate inter-administrator reliability and high validity of the I-mP&R. 16
This study highlights the acute impact of concussion on reactive balance in collegiate athletes, particularly in dual-task conditions. Such impairments recovered with the resolution of symptoms, with no deficits for most asymptomatic athletes compared to matched controls. However, the effects of concussion on reactive balance may differ based on lifetime concussion history. These effects of lifetime concussion history, as well as the effects of persisting symptoms after concussion, should be explored further. Future research should also consider directly investigating the effects of concussion on the ability to prime (ie, prepare) a motor response and the ability to execute said motor response. The identified long-term deficits and the importance of history of concussion in reactive balance, particularly in dual-task scenarios, suggest reactive balance may complement other clinical assessments, including static balance and dynamic gait assessments, in the acute management of concussion.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683241309569 – Supplemental material for Acute and Longitudinal Effects of Concussion on Reactive Balance in Collegiate Athletes
Supplemental material, sj-docx-1-nnr-10.1177_15459683241309569 for Acute and Longitudinal Effects of Concussion on Reactive Balance in Collegiate Athletes by Cecilia Monoli, Amanda J. Morris, Regan Crofts, Nora F. Fino, Tessa L. Petersell, Trevor Jameson, Leland E. Dibble and Peter C. Fino in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions of Benjamin Cassidy, Ryan Pelo, Nicholas Kreter, Sarah Hill, Brody Roemmich, Christina Geisler, Jun Son, Cameron Jensen, Corinne Mayfield, and the University of Utah Athletic Training Staff.
Author Contributions
Cecilia Monoli: Formal analysis; Software; Validation; Visualization; Writing—original draft; Writing—review & editing. Amanda Morris: Investigation; Software; Validation; Writing—review & editing. Regan Crofts: Data curation; Investigation; Writing—review & editing. Nora F. Fino: Formal analysis; Writing—review & editing. Tessa L. Petersell: Data curation; Writing—review & editing. Trevor Jameson: Resources; Writing—review & editing. Leland E. Dibble: Conceptualization; Funding acquisition; Methodology; Resources; Supervision; Writing—review & editing. Peter C. Fino: Conceptualization; Funding acquisition; Methodology; Project administration; Resources; Supervision; Writing—original draft; Writing—review & editing.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported with support from the Pac-12 Conference’s Student-Athlete Health and Well-Being Initiative (PI: Fino, Dibble), Grants: #5-04 Pac-12-Utah-Fino-19-01 and #9-01 Pac-12-Utah-Fino-23-01. Additional funding support was provided by the Eunice Kennedy Shiver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number K12HD073945, and the University of Utah Study Design and Biostatistics Center, with funding in part from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1TR002538 (formerly 5UL1TR001067-05, 8UL1TR000105, and UL1RR025764). The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the Pac-12 Conference, or its members, or of the National Institute of Health.
Ethical Approval and Informed Consent
The study was reviewed and approved by University of Utah IRB (IRB_00116431). All participants underwent written informed consent in accordance with a protocol approved by the Institutional Review Board.
Patient and Public Involvement Statement
Patients or the public were not involved in the design, conduct, reporting, or dissemination plans.
Equity Diversity and Inclusion Statement
All eligible subjects were included, irrespective of their sex, gender, race/ethnicity, cultural background, or socioeconomic status.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.