
Abstract
Background
Women have a higher risk of stroke and related disability than men but are underrepresented in stroke clinical trials. Identifying modifiable recruitment and enrollment barriers for women can improve study generalizability, statistical power, and resource utilization.
Objective
In a post-stroke neuromodulation study, we determined the impact of sex on the occurrence of exclusion criteria and compared the sex distribution of screened and enrolled individuals with a broader stroke-affected population.
Methods
A total of 335 individuals with chronic stroke were screened for a study examining how neuromodulation and high-intensity treadmill training affect walking speed and corticomotor excitability. Demographics and exclusions were retrospectively gathered as a secondary dataset. Exclusion criteria consisted of 6 categories (not target population, unable to do treadmill protocol, unable to do non-invasive brain stimulation, insufficient ankle motion and disinterest, and cognitive impairment). Incidence of each exclusion criterion was compared between women and men. The sex distribution was compared to a dataset from Chicago primary stroke centers.
Results
A total of 81 individuals were enrolled and 254 were not. The percentage of women excluded was significantly greater than that of men (P = .04). No individual exclusion criterion or categories excluded women more frequently than men. Screened and enrolled individuals had a lower proportion of women and younger age than a representative stroke population (P < .001).
Conclusions
We identified exclusion criteria (ie, headaches, cognitive scores, and age) that are modifiable barriers to enrollment of women in this post-stroke neuromodulation study. Addressing underrepresentation of women in stroke research is pivotal for enhancing generalizability, achieving statistical power, and optimizing resources.
Introduction
Stroke is a leading cause of death and disability in adults with an estimated global incidence of 11.7 million and prevalence of 89.1 million people. 1 This number is expected to rise in the coming years. 2 Chronic disability from stroke leads to lower levels of physical activity and reduced quality of life3,4 and is associated with secondary diseases and disorders, including depression, obesity, and diabetes.5,6 Notably, women have a higher lifetime risk of stroke and are more likely to suffer stroke-related disability than men.7,8
Given that poor walking recovery is a major contributor to disability,9,10 one of the primary goals of stroke motor rehabilitation is to restore functional walking to reduce and mitigate the consequences of chronic disability. Despite intensive rehabilitation efforts, walking impairment and disability persist. 9 This has driven the search for new therapies to improve or enhance walking rehabilitation. One promising emerging therapy is to enhance walking interventions with non-invasive neuromodulation, including transcranial direct current stimulation (tDCS).11,12 Although there exists favorable evidence regarding the potential benefits of tDCS,11,12 several factors have limited insights into the effectiveness and generalizability of this and other interventions. Many studies have had limited sample sizes, underscoring the need for expansive clinical trials to confirm efficacy of neuromodulation for improving post stroke walking.13,14 Also, in line with historical trends, 15 women have been underrepresented in stroke research, including clinical trials, where women typically represent ≤40% of samples.16,17
In the development of new large-scale clinical trials, it is important to evaluate how existing recruitment and enrollment practices can be modified to yield study populations that are more generalizable to the broader population, particularly with regards to sex. Recognizing and mitigating obstacles that impede the enrollment of participants in clinical trials could improve power to detect effects and reduce the overall time, effort, and resources needed to complete these studies. Furthermore, ensuring the proper representation of women in stroke studies not only enhances the overall generalizability of study findings but also addresses the long-standing issue of under-enrollment of women in randomized controlled trials. 15 Importantly, studies involving neuromodulatory strategies like tDCS and neurophysiological measurements with transcranial magnetic stimulation (TMS) have additional constraints, considerations, and eligibility criteria to ensure safety that may affect the inclusion of women disproportionately.
The impact of eligibility criteria on women in post-stroke neuromodulation studies, particularly involving walking and TMS, has been rarely reported.13,14,18,19 This is an important area of continued research.16,17 Hence, our primary objective is to investigate enrollment of women in a post-stroke neuromodulation (ie, tDCS) study in 2 ways (1) to determine whether sex (female vs male) has an impact on the occurrence of each barrier to enrollment (exclusion criterion) and determine if these effects differ by sex; and (2) to compare the sex distribution of individuals screened and enrolled in our study with that of a broader stroke-affected population.
Methods
Data for this study were retrospectively gathered as a secondary dataset from a randomized clinical trial (ClinicalTrials.gov: NCT03492229) that examined the effects of tDCS priming and ankle motor tracking on walking speed and corticomotor excitability in adults with chronic stroke. 20 In brief, this study involved high intensity speed-based treadmill training, with some experimental groups receiving tDCS and/or ankle motor training (neuromodulatory paradigm) prior to training. Outcome measures included walking speed and corticomotor excitability measured via TMS. Recruitment for this study occurred from 2014 to 2018. This study was approved by the institutional review board at the University of Illinois Chicago and conformed to ethical standards. All enrolled individuals provided written informed consent.
Adults aged 40 to 80 years who had sustained a first-ever monohemispheric stroke ≥6 months prior and were not participating in other physical therapy or exercise programs were recruited in this study. Subjects were recruited through advertisements posted at UIC. Advertisements were also placed around the metropolitan Chicago area. Additionally, individuals were recruited by physician referral from the Department of Neurology at UIC and from an existing participant database in our lab. Exclusion criteria for the study, divided into 6 broad categories, included: (1) not meeting target population: age <40 or >80 years, no residual gait deficits, brainstem or cerebellar stroke, history of 0 or >1 strokes, and participation in another exercise study or program. Age exclusions were done to avoid the impact of development or advanced age on study outcomes.21,22 Residual gait deficits were required to permit detection of improvements in walking outcomes. Individuals with brainstem or cerebellar stroke and with multiple strokes were excluded because of the potential for these to yield bilateral impairments. (2) Unable to do the treadmill protocol: unable to walk ≥5 minutes without assistance, severe osteoporosis, uncontrolled cardiorespiratory or metabolic diseases, too slow or too fast gait speed, uncontrolled anti-spasticity medications, and miscellaneous treadmill exclusions including joint pain and safety concerns (aphasia, balance problems, and incompatible with harness.). These exclusions were used to ensure safe and full participation in the training program. (3) Unable to do TMS: use of a pacemaker, metal implants in the head or face, unexplained or recurring headaches, history of seizures, medications that alter seizure threshold, skull abnormalities or fractures, and concussion with the prior year. These exclusion criteria were used to ensure safe application of TMS to determine our corticomotor excitability outcome measure. (4) <5° active ankle dorsiflexion: From prior work, we have determined that at least 5° active ankle dorsiflexion is necessary to perform the ankle motor tracking task. (5) Uninterested. (6) Mini-Mental State Examination (MMSE) score <21: This exclusion criterion was used to ensure understanding of and compliance with study procedures.
Potential participants were screened over the phone to determine initial eligibility (inclusion/exclusion criteria not requiring in-person interaction), availability, and interest in study participation. Sex (female or male) was recorded as self-reported by the potential participant. Participants who passed the initial phone screening, provided informed consent and were screened in-person for a final eligibility determination Reasons for participant exclusion during phone and/or in-person screening were recorded for each potential participant.
In the retrospective analysis presented in this paper, we reviewed phone and in-person screening forms, and recorded the incidence of each exclusion criterion for participants who were not enrolled in the trial. Exclusion incidence was separated by sex (female or male). Additionally, the sex composition of our screened population, enrolled population, and a representative stroke sample were compared. Our representative stroke sample consists of participants of the Chicago Health and Aging Project who were admitted for stroke to 15 Chicago primary stroke centers (PSCs) between January 1, 2010 and March 31, 2015.23,24 These individuals were residents of 4 Chicago neighborhoods and aged ≥65 years. 24 Data for this Chicago PSC population were obtained from a publicly available longitudinal population-based study. 23
Statistical Analysis
Descriptive statistics were used to create the demographics table which displays the incidence of each exclusion criterion for women and men. To test the primary aim of this paper, we compared the incidence of each exclusion criterion between sexes using Fisher’s exact test. To test the secondary aim of this paper, we compared the sex composition of the screened individuals, enrolled participants, and the representative stroke sample using chi-square analysis. We also compared ages between these groups using independent samples t-tests. IBM SPSS Statistics (Version 27) was used for statistical analyses. P < .05 was considered significant.
Results
Of the 335 individuals screened for the study 81 were enrolled and 254 were not enrolled. As previously mentioned, the exclusion criteria fall into 6 categories (Table 1, bold). When we examined the incidence of overall exclusion by sex, we found that the percentage of women who were excluded was significantly greater than the percentage of men who were excluded (P = .04; Table 1). When examining individual criteria, we found that no criterion excluded a significantly higher proportion of women than men, but history of seizures (P = .02) and having <5° of active dorsiflexion (P = .01) excluded a significantly lower proportion of women than men.
Incidence and Percentage of Exclusion Criteria by Sex.
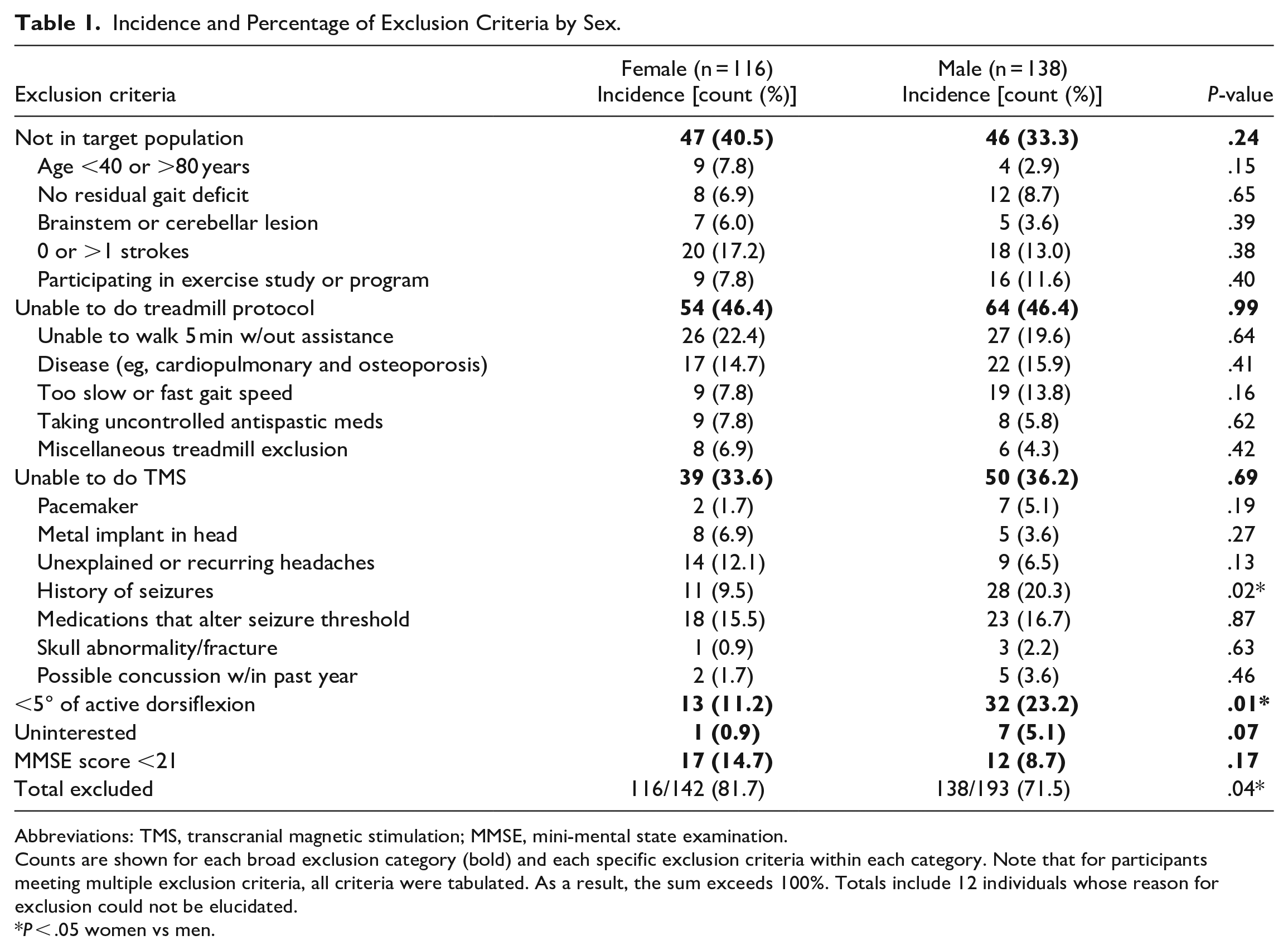
Abbreviations: TMS, transcranial magnetic stimulation; MMSE, mini-mental state examination.
Counts are shown for each broad exclusion category (bold) and each specific exclusion criteria within each category. Note that for participants meeting multiple exclusion criteria, all criteria were tabulated. As a result, the sum exceeds 100%. Totals include 12 individuals whose reason for exclusion could not be elucidated.
P < .05 women vs men.
We compared our enrolled and screened populations to each other, and to a representative sample of individuals with stroke (Chicago PSC stroke population; Table 2). The proportion of women in the enrolled and screened samples did not differ (χ2[1, 406] = 2.0, P = .16) but were significantly lower than the Chicago PSC stroke population, (χ2 [1, 10395] = 12.5, P < .001 and χ2 [1, 10 649] = 11.5, P < .001, respectively). The average age of the enrolled and screened samples did not differ (t[414] = 0, P > .99) but both were significantly lower than the Chicago PSC stroke population (t[10,393] = 5.5, P < .001 and t[10,640] = 11.0, P < .001, respectively. The racial composition of our enrolled participants did not differ from Chicago PSC stroke population (χ2 [2, 1268] = 4.3, P = .12).
Demographics of Enrolled Participant, Screened Individuals, and the Chicago PSC Stroke Population.
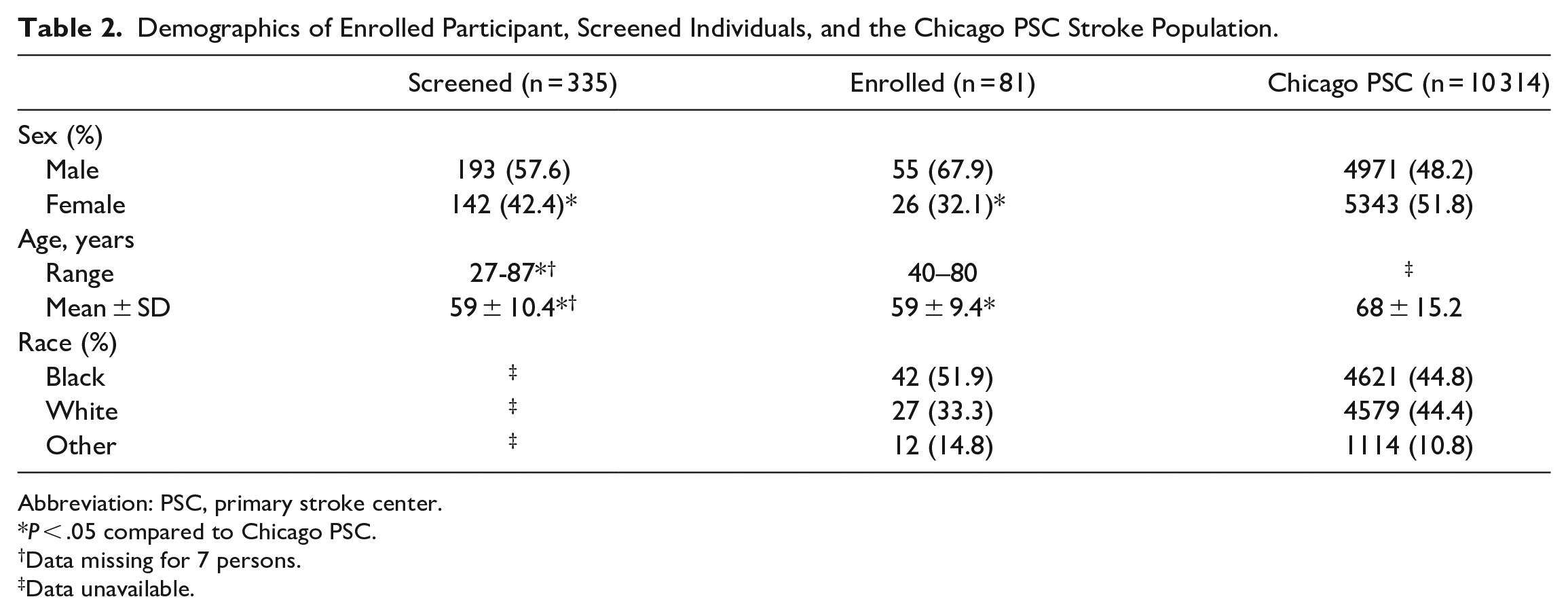
Abbreviation: PSC, primary stroke center.
P < .05 compared to Chicago PSC.
Data missing for 7 persons.
Data unavailable.
Discussion
The goals of this study were to determine whether sex influences the incidence of barriers to enrollment in a post-stroke neuromodulation and walking study, and to compare the sex composition of our study population to a larger stroke-affected population. Our analyses revealed that a significantly higher proportion of women were excluded than men overall, and there were several factors that may have disproportionately excluded women versus men. When comparing our screened and enrolled populations to the Chicago PSC stroke population, we identified that our participants encompassed a smaller proportion of women.
The noticeably lesser enrollment and recruitment of women in comparison to men underscores a dual challenge in recruitment of women: first, an inadequate number of women are included in the screening process relative to the stroke population; and second, among the women who undergo screening, a substantial number are subsequently excluded. This is concerning for several reasons. Historically, there has been an ongoing challenge in achieving equitable representation of women in clinical trials, 15 a phenomenon that is also true for stroke studies.16,17 The underrepresentation of women in stroke-related clinical trials is particularly noteworthy given that women bear a higher lifetime risk of stroke, both within the United States and globally. 7 Women are also more likely to die and suffer disability from stroke than males.7,8
While our data did not reveal any specific criteria that led to the exclusion of women at a significantly higher rate than men, certain factors warrant attention due to their sex-specific implications. For instance, women have a higher susceptibility to migraines and severe headaches.25,26 Given this disparity, it might be prudent to exercise scrutiny when evaluating individuals who report experiencing headaches, particularly given that in our study women were excluded at a 5% higher rate than men for headaches (although not a significant difference, P = .13). History of headache was included to mitigate the risk of TMS-induced headache, but reported instances of headaches during TMS are rare. 27 When they do occur, they are mild and transient. 27 Considering the potential to enhance recruitment among women, it could prove advantageous to reconsider the exclusion criterion related to headache history for future studies. One approach might involve either eliminating headache history as a basis for exclusion or refining the criterion to exclusively exclude individuals with severe headaches. This shift in approach could contribute to a more inclusive participant pool and alleviate sex-specific biases.
Another exclusion criterion of interest pertained to the MMSE score below 21. Women present lower MMSE scores than men of the same education level28,29 and that women tend to experience a more rapid decline in cognition with advancing age when compared to men. 30 Additionally, the MMSE was designed to assess cognitive impairment, which does not necessarily satisfy our goal of ensuring that participants are able to understand and comply with study procedures. In the current study, women were excluded at a 6% higher rate than men for MMSE scores (although not a significant difference, P = .17). Taking all this into account, reevaluating MMSE scores as an exclusion criterion could be beneficial, ensuring that any potential biases related to sex or age are mitigated. This could promote a more inclusive participant group. However, adjustments to cognitive criteria should be approached with extreme caution, considering individual safety concerns, particularly when dealing with fall-related aspects.
Exclusion rates for men were notably higher based on a history of seizure and having less than 5° of active dorsiflexion. History of seizure was included as exclusion criteria to ensure safe application of TMS, as seizure is the most serious risk of TMS, especially for those with a seizure history. Having at least 5° of active dorsiflexion was a study-specific criteria related to ability to complete ankle motor tracking. Previous studies have shown that healthy women demonstrate higher ankle range of motion than males,31,32 and that there is a higher prevalence of seizure disorders and epilepsy among men than women. 33 This suggests that significant differences in the history of seizures and active dorsiflexion in men over women could be explained by baseline differences.
Beyond the considerations of modifying inclusion criteria on an individual basis, as elaborated in the preceding section, it is imperative to scrutinize recruitment methods with the aim of enhancing participation of women. The average age of our subjects and that of those screened were significantly lower than the Chicago PSC stroke sample. Considering that 29.95% of strokes occur in individuals over the age of 80, 34 it is likely our age cap of 80 years led to the exclusion of a significant number of older participants. To improve age representativeness and possibly enhance recruitment of women—given that women tend to experience their first-ever acute strokes at a later age than men—it might be advantageous to increase or even remove the age cap, as has been recommended previously.16,17,35 However, this potential benefit must be weighed against the fact that excitability of the cerebral cortex declines and responsiveness to tDCS is delayed with advanced age.21,22 One should also keep in mind that falls are of even greater concern while walking for older stroke survivors. 35
This study has some limitations. Our interpretation of the generalizability of results involves our reliance on the Chicago PSC Stroke population data for comparison. This population only included individuals diagnosed with ischemic stroke who received tissue plasminogen activator in the emergency department, thus excluding individuals with hemorrhagic stroke as well as individuals who did not receive this treatment. Furthermore, the Chicago PSC Stroke population data used in this study only included individuals ≥65 years of age and with no prior stroke. Although, the demographics of this group are similar to other stroke populations of Chicago,36,37 they may not be fully representative of stroke survivors requiring gait rehabilitation. Additionally, while the demographics of this population may be representative of stroke incidence between January 1, 2010 and March 31, 2015, it may not represent Chicago stroke prevalence as well. However, it is worth noting that, despite the potential limitations of the Chicago PSC Stroke population data, the sex and age distributions of this data was consistent with data from the National Emergency Department Sample, which does not have the same limitations.38,39 Lastly, caution should be applied when generalizing our study results. Our protocol required specific inclusion criteria pertaining to neuromodulation and high intensity walking in a chronic stroke setting. Some exclusion criteria may exhibit varying prevalence in an acute or subacute setting. Additionally, studies regarding hand training or balance training, for example, may have different criteria with varying implications for modifying recruitment.
Conclusions/Implications
There was a notable disproportion in exclusion of women compared to men in this post-stroke neuromodulation study. While our enrolled population’s racial composition aligned with another larger Chicago Stroke Study Population, our screened and enrolled groups exhibited a younger average age and included fewer women than this population. Addressing the sex discrepancy in exclusion rates is pivotal not only for enhancing the inclusivity of the study but also for addressing the historical sex disparities in clinical trial participation, particularly in the realm of stroke research. Additionally, certain exclusion criteria, such as headache history, cognitive cut-off scores, and the designated age range, may warrant investigation for potential recruitment enhancements.
Footnotes
Acknowledgements
We thank all research personnel from the Brain Plasticity Lab that helped with recruitment and screening for the clinical trial from which this dataset was collected.
Author Contributions
Twinkle Mehta: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Validation; Writing—original draft; Writing—review & editing. Brice Cleland: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Supervision; Validation; Writing—review & editing. Sangeetha Madhavan: Conceptualization; Data curation; Funding acquisition; Investigation; Methodology; Project administration; Resources; Supervision; Writing—review & editing.
Data Availability Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Institutes of Health (SM) [R01HD075777]. Study sponsors had no role in study design, data collection, data analysis, data interpretation, writing the manuscript, or the decision to submit this manuscript for publication.