
Abstract
Background. Decreased automaticity is common among individuals with neurodegenerative disease and is often assessed using dual-task (DT) paradigms. However, the best methods for assessing performance changes related to DT demands remain inconclusive.
Objective. To investigate the reliability and validity of a novel battery of DT measures (DT Effect—Battery (DTE-B)) encompassing three domains: task-specific interference, task prioritization, and automaticity.
Methods. Data for this retrospective cross-sectional study included 125 participants with Parkinson’s disease (PD), 127 participants with Alzheimer’s disease (AD), and 84 healthy older adults. Reliability analyses were conducted using a subset of each population. DTE-B measures were calculated from single and DT performance on the Timed Up and Go test and a serial subtraction task. Construct validity was evaluated via associations within the DTE-B and with theoretically supported measures as well as known-groups validity analyses.
Results. Good to excellent reliability was found for DTE-B measures of task interference (motor and cognitive DT effects) (ICCs≥.658) and automaticity (combined DT effect (cDTE)) (ICCs≥.938). Evidence for convergent validity was found with associations within the hypothesized constructs. Known-groups validity analyses revealed differences in the DTE-B among the healthy group and PD and AD groups (ps≤.001), excepting task prioritization (ps≥.061).
Conclusions. This study provides evidence to support the DTE-B as a reliable measure of multiple constructs pertinent to DT performance. The cDTE demonstrated evidence to support its validity as a measure of automaticity. Further investigation of the utility of the DTE-B in both PD and AD, as well as other populations, is warranted.
Keywords
Introduction
A decrease in automaticity—performance of task without attention directed to task execution—is common among individuals with neurodegenerative disease.1,2 It is a key deficit in Parkinson’s disease (PD) and is a crucial target of retraining and rehabilitation for individuals with PD. 3 In PD, automaticity is more impaired among those with freezing of gait and cognitive impairment.4-6 In Alzheimer’s disease (AD), deficits in automaticity progress with disease severity.7-9 Automaticity is compromised in individuals with mild cognitive impairment relative to healthy individuals 9 and individuals with mild cognitive impairment with impaired automaticity progress to dementia more rapidly than those with comparatively intact automaticity.10,11
Automaticity is assessed by dual-task (DT) paradigms wherein a primary task (often a motor task) and a secondary task (often a cognitive task) are done concurrently 1 ; however, there is no consensus on the best methods or measures for assessing DT performance. 12 Yang et al 12 observed that there were many different methods for assessing the DT effect or the relative change in performance resulting from conducting a DT. DT assessment is performed by quantifying the change in primary task performance or the change in secondary task performance while completing the combined task.12-14 One of the most accepted measures for assessing task-specific DT interference is calculating the motor or cognitive DT effect, which relates DT performance to single-task (ST) performance. While this method is valuable in assessing individual task components related to DT performance, a measure assessing DT interference that quantifies the combined interference of the motor and the cognitive tasks may be a more holistic measure of DT effect and may provide a more accurate picture of automaticity.15-17 Task prioritization (ie, whether the motor or cognitive task is prioritized during DT) is most often determined by the manner of instruction for performing the DT. Recently, there have been efforts made to categorize and quantify task prioritization.13,14,18
Few studies investigating DT performance in PD or AD have included measures that individually assess change in performance of both the primary and secondary tasks that comprise the DT (motor DT effect [mDTE] and cognitive DT effect [cogDTE]). Fewer still have utilized a measure of task prioritization. To our knowledge, only one study has previously utilized a robust measure of combined interference in these populations. 15 The inclusion of measures of motor, cognitive, and combined effects of DT interference, as well as task prioritization, may help to elucidate subtle motor and cognitive deficits related to automaticity, particularly in individuals with neurodegenerative disease. 19 Additionally, utilization of a series of measures allows for assessment of other important aspects of DT performance including between task discrepancies and task prioritization and for putting them in context of each other. This method could prove useful for assessing disability, disease progression, and response to treatment. 20
The purpose of this study was to investigate the reliability and validity of a novel combination of DT measures herein referred to as the DT effect battery (DTE-B) among individuals PD, AD, and healthy older adults. The DTE-B includes several DT measures falling into three related domains: 1) Task-specific interference or effects (mDTE and cogDTE); 2) Task prioritization (task prioritization category and modified attention allocation index (mAAI)); and 3) Automaticity (combined DTE [cDTE]—a novel measure of combined motor and cognitive DT interference). The first aim of this study was to investigate the test–retest reliability of the DTE-B. The second aim was to investigate the construct validity (encompassing convergent validity, divergent validity, and known-groups validity) of the DTE-B. We hypothesized that evidence for the validity of the cDTE would be demonstrated through moderate to strong associations with measures of other DT metrics and more automatic tasks, as well as weak to no relationship with tasks with relatively high attentional demands (eg, high task complexity involving many sensory, motor, and cognitive functions). We anticipated that known-groups validity analyses would provide further evidence for the validity of the DTE-B. While AD and PD have differing pathophysiology and presentation, they have many commonalities including that they are both progressive neurodegenerative diseases, they are protein-misfolding disease, have prominent neuroinflammatory mechanisms, and lead to both cognitive and motor impairments.21,22 The main phenotypic difference is that PD has more prominent early motor features with later cognitive impairment while AD has more prominent early cognitive features. 23 The cDTE considers cognitive performance with equal weight to motor performance, such that a relatively similar decline in either will result in a similar outcome for cDTE. Thus, we hypothesized that while automaticity (cDTE) would be least impacted in the healthy older adult group, both the PD and AD groups would be more impacted, though not different between groups. However, since PD has more prominent motor impairment than cognitive impairment, and AD is characterized by more prominent cognitive impairment than motor impairment, we predicted that these disease features would influence task-specific interference (mDTE and cogDTE). Specifically, we anticipated that they would be different between these two groups with the AD group showing greater cogDTE and less mDTE than the PD group. We hypothesized that mAAI would differ between groups, with the PD group prioritizing cognitive performance (less decline in cognitive performance than motor performance under DT conditions), the AD group prioritizing motor performance (less decline in motor performance than cognitive performance under DT conditions), and the healthy older group demonstrating no clear prioritization strategy.
Methods
Design
A retrospective cross-sectional analysis of data collected from Cleveland Clinic Lou Ruvo Center for Brain Health (CCLRCBH) clinical medical records (PD and AD) and research (healthy older adults) data sets was conducted. 24 The work was approved by the Cleveland Clinic Institutional Review Board, number 16-101, and informed consent was waived. Demographic data, DT performance, PD symptoms, cognition and depression, balance and falls, and gait measures in healthy older adults and individuals with PD and AD were captured. Participants that completed repeat DT measurement at least 7 days but no more than 28 days apart (mean 8.9±3.7) were included in the reliability analyses. For Aim 1, test–retest reliability of the DTE-B was investigated in a subset of 105 participants made up of individuals from the PD (n=37), AD (n=34), and healthy (n=34) groups. For Aim 2, we explored the construct validity of the DTE-B by comparing its components to measures of other constructs (PD symptoms [PD group only], cognition and depression, balance and falls, and gait). Convergent validity was assessed by comparing the DTE-B with measures of the same or similar constructs, and divergent validity was evaluated by comparing the DTE-B to dissimilar constructs, including depression (Patient Health Questionnaire-9; PHQ-9) and non-motor symptoms of PD (Movement Disorder Society-Unified Parkinson’s Disease Rating Scale; MDS-UPDRS part I). Known groups’ validity was assessed by comparing DTE-B performance between AD, PD, and healthy groups.
Participants
Parkinson’s Disease and Alzheimer’s Disease Cohorts
All patients with an initial physical therapy evaluation at CCLRCBH from July 2017 to June 2019 were identified from medical records. Clinical diagnosis of PD or AD was completed by a neurologist using contemporary diagnostic criteria.25-27 Patients were included in either the AD or PD cohort based on their clinical diagnosis. The AD cohort included individuals ranging in symptomatic presentation from moderate dementia to mild cognitive impairment due to AD. Inclusion criterion for this study was a referral to physical therapy for primary treatment of PD or AD and completion of the dual task assessment (described below). All participants included in the analyses had a standardized physical therapy assessment conducted by one of four licensed physical therapists at one outpatient facility. All physical therapists underwent annual training for systematic collection and assessment of the outcome measures used in this study. Patients were excluded if they were referred to physical therapy for treatment of any condition that was not a result of PD or AD, including vestibular dysfunction, significant osteoarthritis, or lower extremity injury (fractures, strains, and sprains) or surgery. Data from 252 records were extracted—125 individuals with PD, and 127 individuals with AD (Figure 1). Study data sources flow diagram.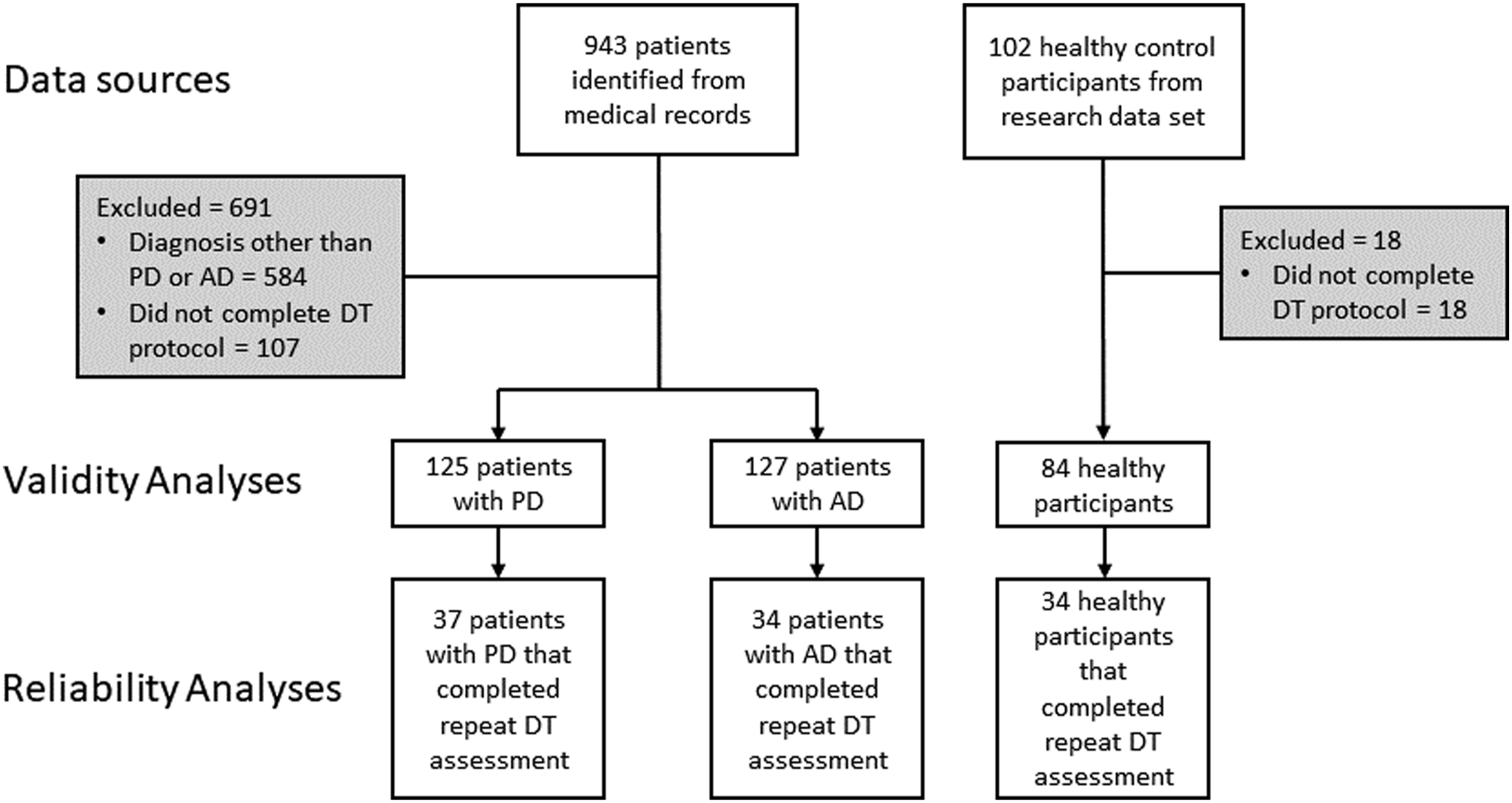
Healthy Older Adult Cohort
This cohort consisted of individuals aged 55–85 who were neurologically healthy and community-dwelling. Individuals were excluded from this group if they had significant orthopedic conditions that affected their gait or if they had any evidence of cognitive impairment (Montreal Cognitive Assessment (MoCA) < 26).
Descriptive statistics and P-values for between-group differences (Quade’s ANCOVA or Chi square test as appropriate) for the PD, AD, and healthy groups. Benjamini–Hochberg correction applied to control for family wise error. Significant group main effect P-values after correction are marked in red.
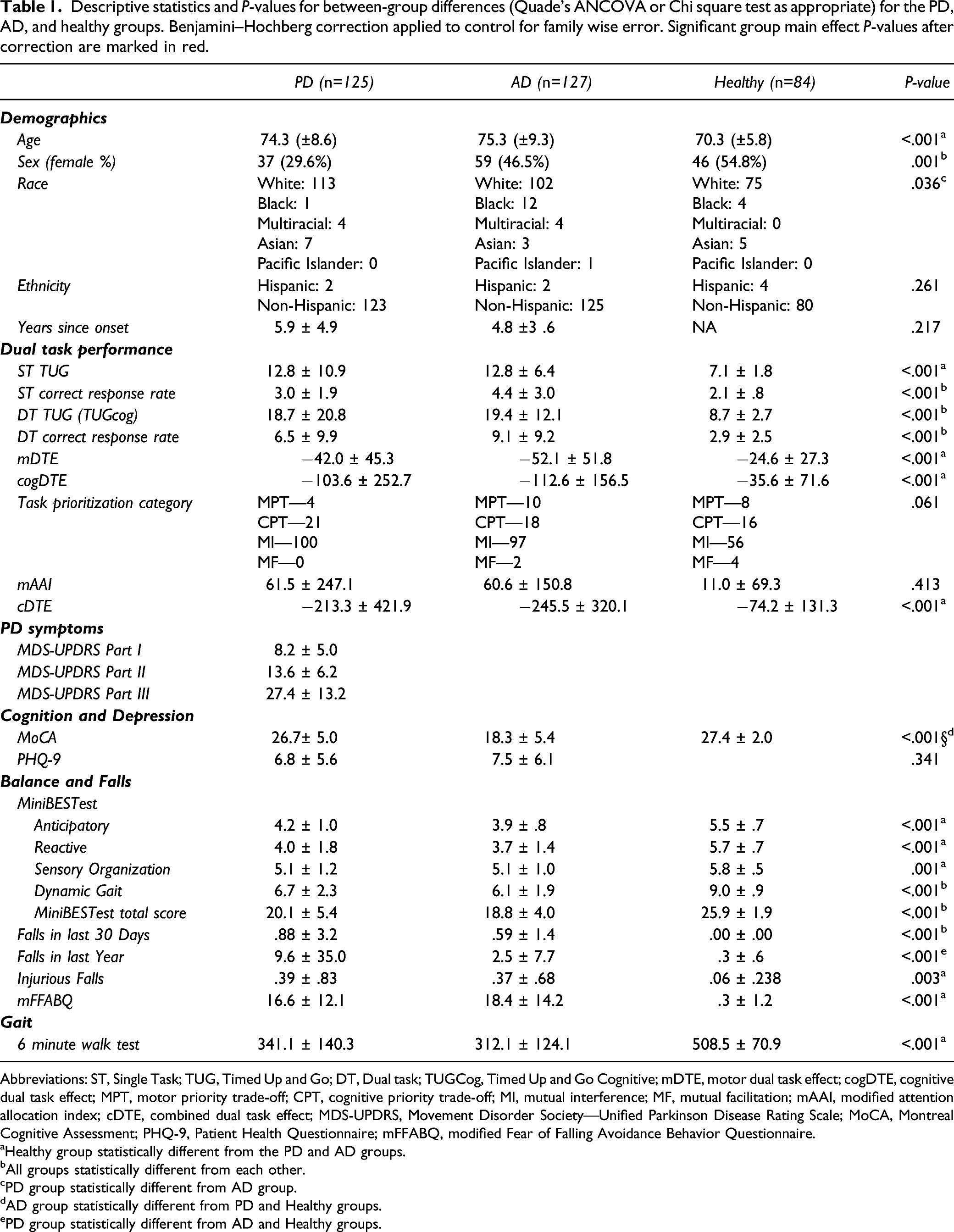
Abbreviations: ST, Single Task; TUG, Timed Up and Go; DT, Dual task; TUGCog, Timed Up and Go Cognitive; mDTE, motor dual task effect; cogDTE, cognitive dual task effect; MPT, motor priority trade-off; CPT, cognitive priority trade-off; MI, mutual interference; MF, mutual facilitation; mAAI, modified attention allocation index; cDTE, combined dual task effect; MDS-UPDRS, Movement Disorder Society—Unified Parkinson Disease Rating Scale; MoCA, Montreal Cognitive Assessment; PHQ-9, Patient Health Questionnaire; mFFABQ, modified Fear of Falling Avoidance Behavior Questionnaire.
aHealthy group statistically different from the PD and AD groups.
bAll groups statistically different from each other.
cPD group statistically different from AD group.
dAD group statistically different from PD and Healthy groups.
ePD group statistically different from AD and Healthy groups.
Measures
DTE-B
The DTE-B includes measures of task-specific interference (mDTE and cogDTE), task prioritization (task prioritization category and mAAI), and automaticity (cDTE) which can be derived from performance of a single DT assessment (Figure 2). Times for the following measures were extracted from physical therapy records: Timed Up and Go (TUG) and TUG-Cognitive (TUGcog). The TUG exhibits good test–retest (ICCs>.80) reliability in individuals with PD and AD.28-31 The TUGcog has excellent test–retest reliability (ICC=.94) for community-dwelling older adults.
32
ST cognitive performance during serial subtraction by three was captured by recording the number of correct responses during 20 seconds and the inverse correct response rate calculated as time in seconds divided by number of correct responses.33-35 DT cognitive performance was obtained during the TUGcog using the same method beginning from a different number between 80 and 100 and the inverse correct response rate calculated as the time to complete the TUGcog divided by the number of correct responses during the TUGcog. The resultant ST and DT correct response rates were entered into the DTE equations. The serial subtraction task was selected as it is the most common clinically utilized dual task paradigm and one of the most commonly studied. Instructions for the DT were designed to encourage neutral prioritization between the two tasks (“Walk as quickly as you can safely while completing the subtraction task as quickly as you can accurately”). These variables were then used to calculate mDTE and cogDTE using the equation
14
Dual task effect battery.
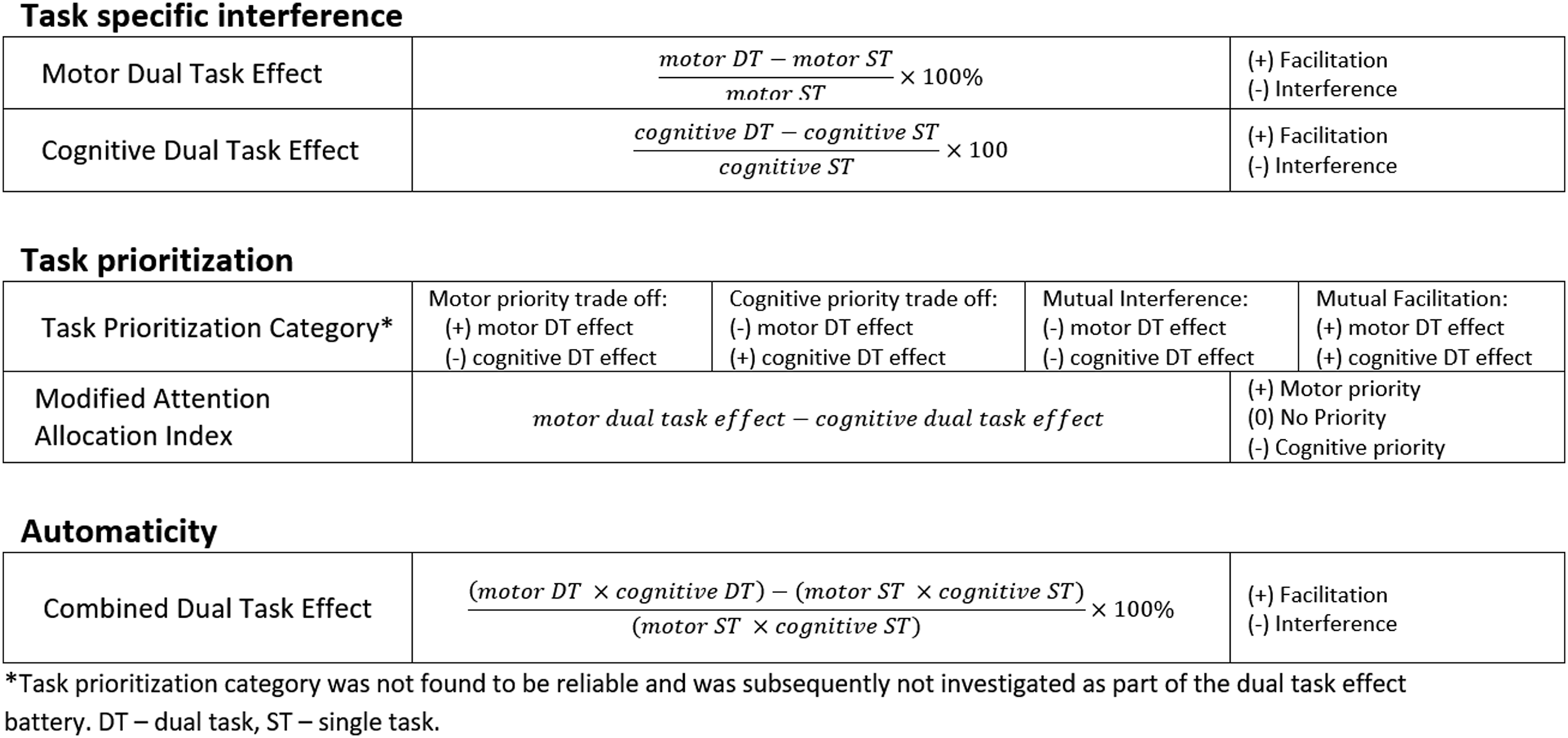
The cDTE equation was designed based on the DTE equation and expanded to assess the combined interference of both mDTE and cDTE (Supplemental Material 1). The cDTE was calculated using the following equation
For both the DT effect equations in this study, higher values indicate poorer performance, so a negative sign was inserted into the formula to be consistent with the established operational definition of DT effects13,14

This approach creates the convention that all negative DT effect values are indicative of performance that deteriorated under DT conditions compared to ST conditions (DT cost). A positive DT effect value is indicative of a relative improvement on performance under DT conditions (DT facilitation).13,14 While mDTE and cogDTE are measures of task-specific interference, it is proposed that cDTE is a measure that quantifies automaticity while performing a DT.
In addition to the measures of DT effect, task prioritization category (based on the criteria established by Plummer et al)
13
and mAAI were utilized to assess task prioritization during DT performance. Task prioritization category was determined by plotting the mDTE against the cogDTE with each quadrant representative of one of the following categories: mutual interference (decline in motor and cognitive performance), cognitive priority trade-off (improved or unchanged cognitive performance accompanied by decline in motor performance), motor priority trade-off (improved or unchanged motor performance accompanied by decline in cognitive performance), and mutual facilitation (improved motor and cognitive performance).
13
mAAI was calculated utilizing mDTE and cogDTE values to assess for trade-offs within the task as follows14,18
Positive values represent a shift in attention toward the motor task, whereas negative values indicate a shift in attention toward the cognitive task.
PD Symptoms
The MDS-UPDRDS parts I–III are a standardized measure of the impact of PD on non-motor symptoms, activities of daily living, and disease-specific motor skills, respectively. The MDS-UPDRS parts I–III were used to characterize PD symptoms. 36 The MDS-UPDRS was administered by a trained movement disorders neurologist.
Cognition and Depression
Cognition was measured using the MoCA, which was designed to differentiate normal cognition, mild cognitive impairment, and dementia due to AD. It has excellent test–retest reliability (correlation coefficient = .92), 37 with good internal consistency (Cronbach’s alpha = .83). Additionally, it has evidence for its validity in early PD. 38 The PHQ-9 was used to measure depression in the PD and AD groups and excellent reliability (Cronbach’s alpha = 089). 39 The MoCA was administered by a trained PD/AD nurse or neurologist.
Balance and Falls
Scores from the Mini Balance Evaluation Systems Test (MiniBESTest) were included to describe balance performance. The MiniBESTest measures anticipatory postural control, reactive balance, sensory orientation, and dynamic gait and exhibits excellent inter-rater reliability (ICC = .98). 40 Falls in the last 30 days, falls in the last year, and fall-related injuries in the last year were extracted. Lastly, scores for the modified fear of falling avoidance behavior questionnaire were extracted. The modified fear of falling avoidance behavior questionnaire is a self-report questionnaire that quantifies avoidance behavior due to fear falling. There is evidence for the reliability of the modified fear of falling avoidance behavior questionnaire among individuals with PD and other neurologic conditions (ICC=.812). 41 These measures were all administered by a trained physical therapist.
Gait
Scores from the Six-Minute Walk Test (6MWT) were included.42,43 The 6MWT has excellent test–retest reliability (ICC = .95–.96) for individuals with PD. 30 It has excellent test–retest (ICC = .982–.987), inter-rater (ICC = .97–.99), and intrarater reliability (ICC = .76–.9) for individuals with AD.28,44 The 6MWT was administered by a trained physical therapist.
Sample Size Estimation
Sample size was estimated using effect size and standard deviation for cDTE obtained from pilot data using PASS 20.0.3 (NCSS, LLC. Kaysville, Utah, USA, www.ncss.com/software/pass) for both aims. For the reliability analysis (Aim 1), confidence intervals for interclass correction module was utilized. The estimate revealed that a sample of 34 participants, who were each measured twice, would produce a two-sided 95% confidence interval with a width of .200 when the estimated interclass correlation is .850 utilizing a two-way random-effects ANOVA model (ICC 3,2). For construct validity (Aim 2), a sample of 84 achieves 80% power to detect a difference of .3 between the null hypothesis correlation and the alternative hypothesis correlation using a two-sided hypothesis test with a significance level set at α=.05.
Data Analysis
All analyses were conducted using SPSS 24.0 (IBM SPSS Statistics for Windows, Armonk, NY: IBM Corp) with α = .05. Descriptive statistics and between-group comparisons were conducted using chi square for nominal data and nonparametric (Quade’s) ANCOVA, due to lack of homogeneity of variance between groups and to include age as a covariate. Statistical corrections for multiple comparisons were completed using Benjamini–Hochberg corrections.
For Aim 1 (test–retest reliability and minimal detectable change [MDC]), a subset of participants from each group (PD (n=37), AD (n=34), and healthy (n=34)) completed DT assessment twice. These data were analyzed using the ICC model 3 for continuous data and Cohen’s kappa for categorical data (task prioritization category). ICC conventions were defined as poor (<.4), fair (.4 to .59), good (.6 to .74), and excellent (.75 to 1.00).
45
Kappa values were interpreted according to the following criteria: poor (<.00), slight (.00 to .20), fair (.21 to .40), moderate (.41 to .60), substantial (.61 to .80), and almost perfect (.81 to 1.00).
46
To determine the MDC, standard error of measurement (SEM) was calculated using the ICC test–retest reliability statistic, where SD=standard deviation and rxx= ICC test–retest reliability statistic
Once the SEM was determined, the minimal detectable change at a 95% confidence level (MDC95) for cDTE was calculated by multiplying the SEM by 1.96 (representing 95% of the area under the curve of a normal distribution) and 1.41 (the square root of 2 to control for possible error associated with calculating the coefficient from 2 time points)
For Aim 2 (construct validity), convergent validity, divergent validity, and known-groups analyses were completed. In this study, we compared the DTE-B to four domains of outcomes (PD symptoms, cognition and depression, balance and falls, and gait) using correlational statistics (Pearson product moment correlations or Spearman’s rho). We anticipated evidence for convergent relationship between cDTE and measures in the DTE-B, and more automatic tasks that require comparatively less attentional resources, such as steady-state gait 47 (6MWT) and balance reactions 48 (MiniBESTest reactive balance subscale). Conversely, we anticipate that tasks demanding a moderate or greater degree of attentional resources such as anticipatory balance control 49 (MiniBESTest anticipatory balance subscale), activities of daily living 50 (MDS-UPDRS part II), and disease-specific motor skills1,51 (MDS-UPDRS part III) will correlate more strongly with either task-specific interference measures (mDTE and cogDTE) or mAAI, a measure of attention allocation. We anticipated that tasks that require high levels of attentional resource allocation such as falls and modified Fear of Falling Avoidance Behavior Questionnaire would be more closely related to mAAI specifically.52,53 Conversely, we expected divergent validity, for cDTE specifically, to be demonstrated by minimal to no relationship between cDTE and the MDS-UPDRS part I and PHQ-9, and relationships with measures that require attentional resources that are weaker than their counterparts in the task interference domain (mDTE and/or cogDTE) and task prioritization domain (mAAI) as described above.
The groups for the known-groups validity analysis were created based on neurologic diagnosis as follows: PD group (more motor impairment than cognitive impairment), AD group (more cognitive impairment than motor impairment), and a healthy older adult group (no impairment). Due to the age differences between groups, non-parametric (Quade’s) ANCOVA was conducted comparing performance on DTE-B measures (mDTE, cogDTE, mAAI, and cDTE) across groups entering age as a covariate.
Results
There were several between-group differences on the outcomes of interest. These are presented in Table 1.
[Aim 1 (Reliability Analysis)
Test–retest reliability (ICC(3,2) with 95% confidence interval) and minimal detectable change (MDC95) for the motor dual task effect, cognitive dual task effect, modified attention allocation index, and combined dual task effect for each groups (PD, AD, and healthy). Test–retest reliability (Cohen’s κ with 95% confidence interval) for task prioritization category for each group.
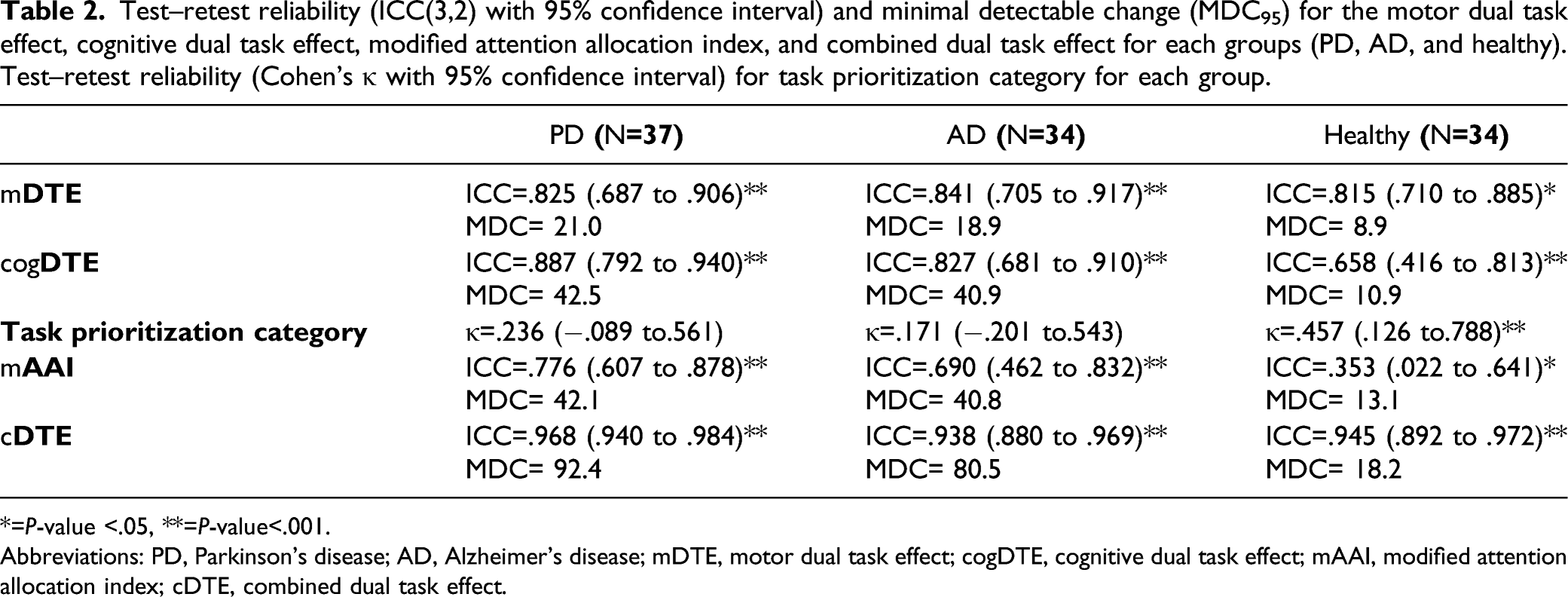
*=P-value <.05, **=P-value<.001.
Abbreviations: PD, Parkinson’s disease; AD, Alzheimer’s disease; mDTE, motor dual task effect; cogDTE, cognitive dual task effect; mAAI, modified attention allocation index; cDTE, combined dual task effect.
Aim 2 (Convergent Validity Analysis)
Pearson product moment correlation coefficient or Spearman’s rho for mDTE, cogDTE, mAAI, and cDTE on hypothesized measures that require attentional control (task-specific interference and task prioritization), hypothesized measures that require automaticity, and measures hypothesized to have no relationship with DTE-B among the PD, AD, and healthy groups. Benjamini–Hochberg corrections were applied to control for family wise error. Significant P-values after correction are marked in red.
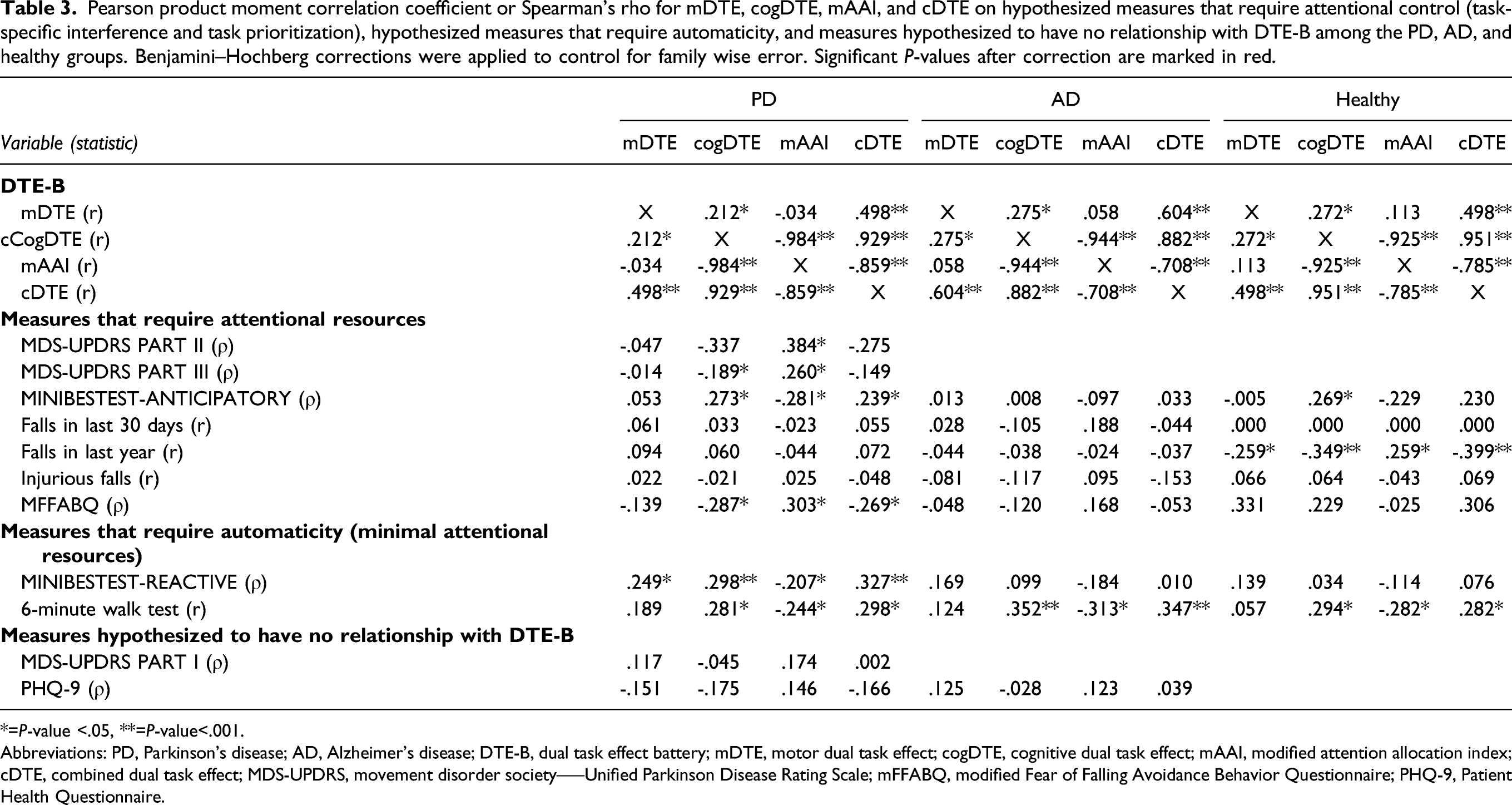
*=P-value <.05, **=P-value<.001.
Abbreviations: PD, Parkinson’s disease; AD, Alzheimer’s disease; DTE-B, dual task effect battery; mDTE, motor dual task effect; cogDTE, cognitive dual task effect; mAAI, modified attention allocation index; cDTE, combined dual task effect; MDS-UPDRS, movement disorder society–—Unified Parkinson Disease Rating Scale; mFFABQ, modified Fear of Falling Avoidance Behavior Questionnaire; PHQ-9, Patient Health Questionnaire.
Aim 2 (Divergent Validity Analysis)
The details of the results can be found in Table 3. No DTE-B measures were associated with MDS-UPDRS part I or with PHQ-9. In observing relative strengths of relationships between DTE-B and other outcomes based on hypothesized relationships, measures of task-specific interference or task prioritization domains, which rely on attentional resources, were more strongly associated with MiniBESTest anticipatory balance subscale (PD), MDS-UPDRS part II (PD), MDS-UPDRS part III (PD), and modified fear of falling avoidance behavior questionnaire (PD) than cDTE. cDTE, in the automaticity domain, was found to be more strongly related to miniBESTest reactive balance subscale (PD), 6MWT (PD), and falls in the last year (healthy). Additionally, cDTE was found to have minimal relationships among hypothesized outcomes related to task-specific interference and task prioritization (PD, AD, and Healthy).
[Aim 2 (Known-Groups Validity Analysis)
The known-groups validity analyses revealed significant between group differences for mDTE, cogDTE, and cDTE (ps<.001), while showing no difference on mAAI (P=.245) (Figure 3). Scheffe post hoc tests revealed that both the PD and AD groups differed from the healthy group (ps≤.033) but not from each other on all DTE-B measures (ps≥.295). Means and standard errors of the motor dual task effect (mDTE), cognitive dual task effect (cogDTE), modified attention allocation index (mAAI), and combined dual task effect (cDTE) among Parkinson’s disease (PD), Alzheimer’s disease (AD), and healthy groups. Statistically significant difference between groups on Scheffe post hoc tests indicates with brackets and the P-value reported.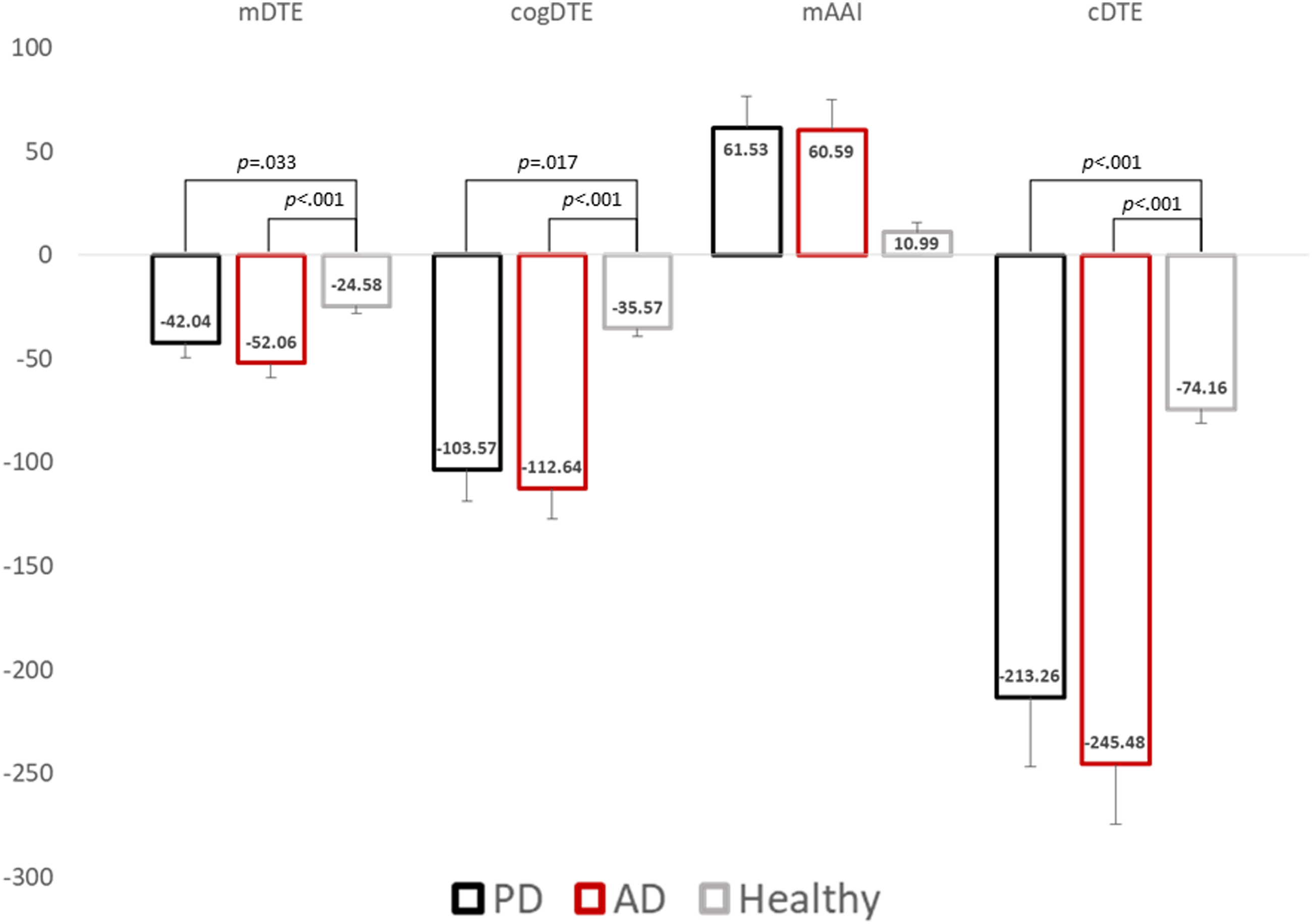
Discussion
Reliability
This study demonstrated that measures of task-specific interference (mDTE and cogDTE) and automaticity (cDTE) exhibit excellent test–retest reliability. Of these measures, the cDTE exhibited the highest level of reliability in each group. This is consistent with our hypothesis that cDTE is a measure of a comparatively more stable construct, automaticity. Compared to the other measures of DT performance, which can be highly influenced or biased by allocation of attention, cDTE incorporates measurement of both tasks reducing the influence of attention allocation. As task prioritization is greatly influenced by volitional attention allocation, it was unsurprising that task prioritization category and mAAI were found to be the least reliable of the DTE-B. This was particularly true of mAAI in the healthy group and is likely a result of this group having no distinct deficit in either cognition or motor control for which they need to actively compensate. This allows their task prioritization strategy to be more fluid than individuals with cognitive or motor deficits. MDCs found in this study were substantially smaller than those reported by Venema et al. 54 These differences may be primarily attributable to smaller ICC values found by Venema et al., which may be due to insufficient power due to an inadequate sample. In summary, this study provides evidence for the reliability of the DTE-B with good to excellent reliability for measures of task-specific interference and automaticity, while measures of task prioritization demonstrated poor to good reliability.
Convergent and Divergent Validity
In investigating the construct validity of the DTE-B, and following our hypothesis, there were moderate to strong relationships with cDTE and mDTE, cogDTE, and mAAI in all groups. This is not surprising as these measures share many common elements and variables in their formulation; however, it does indicate the highly related nature of these measures of task-specific interference, task prioritization, and automaticity, as they relate to DT performance. Among individuals with PD, there were moderate relationships identified between cDTE and measures of gait and reactive balance, such that poorer automaticity was related to poorer gait and reactive balance. These outcomes were anticipated to rely on automaticity, thus providing evidence for the validity of the cDTE as a measure of automaticity. Among the other variables in the DTE-B (mDTE, cogDTE, and mAAI), cDTE was most strongly associated with mDTE, cogDTE, and mAAI. Additionally, the pattern observed in the PD group was partially replicated in the AD and healthy groups, with both groups showing moderate associations between cDTE and the 6MWT, indicating that individuals with greater impairments in automaticity ambulated less distance. Overall, there is substantial evidence for cDTE as a measure of automaticity in the PD group, while in the AD and healthy groups this is less conclusive and would benefit from further investigation.
In contrast to cDTE which was hypothesized to be related to automatic functions, we anticipated that measures of task-specific interference and task prioritization would be more related to tasks requiring attentional resources. The findings in the PD group support this hypothesis while the findings in the AD and healthy groups are less conclusive. Within the healthy group, this may be attributable to floor (falls, modified fear of falling avoidance behavior questionnaire) or ceiling effects (miniBESTest anticipatory balance subscale) and minimal variability on the outcomes in these domains limiting the possibility for relationships to be identified statistically. Within the AD group, it is possible that cognitive impairments may have resulted in inaccurate reporting of falls and recognition of fear of falling avoidance behavior. Conversely, we may accept that there is no relationship between these variables in the AD and healthy groups; however, prior research has shown relationship between falls and mDTE in healthy older adults 55 and those with cognitive impairment. 56 Further research investigating DTE-B measures relationship to psychological variables is warranted to further support the proposed domains.
Additionally, this study provides evidence supporting the divergent validity of the DTE-B through a lack of association seen between it and dissimilar constructs (ie, DTE-B and MDS UDPRS I and PHQ 9). The pattern of associations in the PD group was clearly delineated and in line with the a priori hypotheses and supports the distinct but relatedness of the domains proposed in the DTE-B. The pattern of findings in the AD group is less clear; however, they are somewhat consistent with finding previously reported among individuals with cognitive impairment, 15 indicating that cognitive-specific interference (cogDTE) may play a leading role in driving DT-related performance in those with AD. We found mDTE was not strongly related to gait, balance, and falls, but cogDTE was, highlighting the importance of considering multiple outcomes when evaluating DT performance. In summary, the findings of this study support the DTE-B as a measure of the multiple DT dimensions. This provides opportunities for future work that extends knowledge of DT mechanisms and applications to multiple DT-related domains.
Known-Groups Validity
In the known-groups validity analyses, consistent with our hypothesis, we found that DT performance was uniformly better in the healthy group compared to the PD and AD groups. In contrast to our hypothesis, we found no difference in the presentation of DT performance among the PD and AD groups on task-specific interference, which we anticipated would be influenced by the difference in phenotypic disease features, with AD having more prominent cognitive involvement and PD more prominent motor involvement. This appears to be primarily driven by task prioritization during DT, which was motor prioritized in both groups; this may be a strategy that prioritizes safety over cognition during a functional task. 57 These results are supported by the literature showing that both individuals with PD and AD tend to self-prioritize motor activities over cognitive activities during DT.58,59 One possible explanation for our results is that task prioritization may be more a function of the task involved.57,60-62 This can occur when the attributes of one task are inherently more salient, novel, or challenging. In the case of the DT paradigm utilized in this study, it is possible that the motor task (TUG) was more salient than the cognitive task. Conversely, it is also possible that the cognitive task (serial subtraction) was more challenging or novel than the motor task. Either situation could result in an increased likelihood for individuals to utilize a motor prioritization strategy. Alternatively, this lack of difference may be due to the instructional language used, which encouraged neutral prioritization. 63 Our results show that DT performance may be different between healthy and neurodegenerative populations; however, the patterns of DT performance may not be related to disease pathology. Future research should utilize multiple DT paradigms across participants with different diseases to assess how task and individual characteristics influence task prioritization.
Dual-Task Performance and Falls
In contrast to previous findings, this study found little association between DT performance and falls. Among all groups, only the healthy older adult group was found to have an association between falls and cogDTE and cDTE. This finding is consistent with previous research indicating the relationship between DT performance and falls in the healthy older adult population. 64 Surprisingly, in the PD and AD groups, no relationship between DT performance and falls was identified. While this finding diverges from much of the literature, Heinzel et al. also found that mDTE and cogDTE of a cognitive-motor DT which consisted of serial subtraction and walking, similar to this study, were not associated with future falls in PD. 65 However, in the PD group there was a relationship between DT performance and modified fear of falling avoidance behavior questionnaire, indicating that when DT performance was poorer, individuals had more avoidance behavior related to fear of falling. This may support the hypothesis that poor DT performance is related to falls; however, a sufficiently large portion of participants in the PD group may have recognized this risk and adapted by avoiding risky behaviors, thereby reducing their falls. This would most likely occur in the PD group given the higher fall history and greater need to avoid risky behaviors. 66
Interpretation of the DTE-B
The DTE-B is a tool that can be utilized by clinicians and researchers to characterize DT performance, and can provide clinicians information for better informed decision making. As the DTE-B includes measures of task-specific interference, task prioritization, and automaticity, it allows for interpretation of results relating to these domains and their interactions. Generally speaking, poorer cDTE is indicative of a decreased capacity for automaticity which is not able to be sufficiently compensated for by attentional strategies. Changes in cDTE consequently indicate changes in this capacity. mAAI, on the other hand, is a measure of task prioritization, which is more flexible, and can be interpreted as appropriate or maladaptive in the context of the individual and the task. For example, if an individual with a history of falls demonstrates poor motor DT performance during a walking or balance paradigm and mAAI indicates significant cognitive prioritization, then this individual is likely demonstrating a maladaptive task prioritization strategy, whereas an individual with MCI without fall history or other risks may be demonstrating an appropriate accommodative task prioritization strategy.
Limitations
This study utilized data collected during routine physical therapy practice for the PD and AD participants, and as such, it is possible that these samples represent unique subpopulations with uncertain generalizability. Additionally, while this study did utilize consistent instructional language encouraging neutral task prioritization, it is possible that the instructional language influenced task performance, resulting in changes in attentional resource allocation from usual performance. It is also possible that the DT paradigm utilized in this study may not be most representative of daily life activities that require dual-tasking and, thus, our results may not be generalizable to these DT activities. As such, different DT paradigms with differing task components may have resulted in different results. As the mechanisms for all aspects of DT performance are not fully understood in especially in the context of PD and AD. Thus, the analyses between the PD and AD groups should be interpreted cautiously. Research regarding DT mechanisms is warranted. The cognition of the PD group in this study was largely within normal limits; subsequently, our results may not be generalizable to individuals with PD-dementia. Additionally, the falls data collected was retrospective in nature and subject to several potential biases and our results regarding falls should be interpreted cautiously. This study utilized a retrospective design and as such some variables that may be related to the DTE-B were not able to be included. Participants in this study were included based on clinical diagnosis, which could occur at different stages of disease between individuals with AD and PD. It is possible that while our sample appears to have similar disease duration in the AD and PD group, it is possible that disease severity could be different.
Conclusion
This study provides evidence of the reliability of the DTE-B, novel tool that may improve the consistency of measurement and reporting of DT-related performance and abilities. The DTE-B may improve the characterization of multiple domains within DT performance, specifically attention allocation and automaticity, which are underutilized both clinically and in research. The novel measure of combined interference, cDTE, demonstrated adequate evidence to support its validity as a possible measure of automaticity, as shown in analyses of convergent, divergent, and known-groups validity. Further investigation of the utility of the DTE-B is warranted.
Supplemental Material
sj-pdf-1-nnr-10.1177_15459683221088864 – Supplemental Material for A Novel Way of Measuring Dual-Task Interference: The Reliability and Construct Validity of the Dual-Task Effect Battery in Neurodegenerative Disease
Supplemental Material, sj-pdf-1-nnr-10.1177_15459683221088864 for A Novel Way of Measuring Dual-Task Interference: The Reliability and Construct Validity of the Dual-Task Effect Battery in Neurodegenerative Disease by Jason K. Longhurst, John V. Rider, Jeffrey L. Cummings, Samantha E. John, Brach Poston, Elissa C. Held Bradford and Merrill R. Landers in Neurorehabilitation and Neural Repair
Supplemental Material
sj-pdf-2-nnr-10.1177_15459683221088864 – Supplemental Material for A Novel Way of Measuring Dual-Task Interference: The Reliability and Construct Validity of the Dual-Task Effect Battery in Neurodegenerative Disease
Supplemental Material, sj-pdf-2-nnr-10.1177_15459683221088864 for A Novel Way of Measuring Dual-Task Interference: The Reliability and Construct Validity of the Dual-Task Effect Battery in Neurodegenerative Disease by Jason K. Longhurst, John V. Rider, Jeffrey L. Cummings, Samantha E. John, Brach Poston, Elissa C. Held Bradford and Merrill R. Landers in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the parent study from which the healthy older adult cohort was obtained was funded by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health:#P20GM109025.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.