
Abstract
Background. Embedding mirror therapy within a virtual reality (VR) system may have a superior effect on motor remediation for chronic stroke patients. Objective. The objective is to investigate the differences in the effects of using conventional occupational therapy (COT), mirror therapy (MT), and VR-based MT (VR-MT) training on the sensorimotor function of the upper limb in chronic stroke patients. Methods. This was a single-blinded randomized controlled trial. A total of 54 participants, including chronic stroke patients, were randomized into a COT, MT, or VR-MT group. In addition to 20-minute sessions of task-specific training, patients received programs of 30 minutes of VR-MT, 30 minutes of MT, and 30 minutes of COT, respectively, in the VR-MT, MT, and COT groups twice a week for 9 weeks. The Fugl-Meyer motor assessment for the upper extremities (FM-UE; primary outcome), Semmes-Weinstein monofilament, motor activity log, modified Ashworth scale, and the box and block test were recorded at pre-treatment, post-intervention, and 12-week follow-up. Results. Fifty-two participants completed the study. There was no statistically significant group-by-time interaction effects on the FM-UE score (generalized estimating equations, (GEE), P = .075). Meanwhile, there were statistically significant group-by-time interaction effects on the wrist sub-score of the FM-UE (GEE, P = .012) and the result of box and block test (GEE, P = .044). Conclusions. VR-MT seemed to have potential effects on restoring the upper extremity motor function for chronic stroke patients. However, further confirmatory studies are warranted for the rather weak evidence of adding VR to MT on improving primary outcome of this study. Clinical trial registration: NCT03329417.
Keywords
Introduction
Mild to severe motor impairment of the upper extremity is a major consequence following stroke, 1 which contributes to dependence in activities of daily living. 2 Thus, regaining the motor function of the affected upper extremities is a best-practice recommendation for neurological rehabilitation. 3
Neuroscientific evidence has revealed that the neuroplasticity that rehabilitation induces has strong implications for compensating for the loss of function of the affected brain region. 4 Enrichment in exercise and enrichment in sensory input are the chief principles for improving neuroplasticity, which facilitates motor recovery for stroke patients. 5 Mirror therapy (MT) is a kind of rehabilitation strategy wherein patients can experience the illusion of the affected hand’s movement by observing the unaffected hand’s reflection in a mirror placed on a sagittal plane between the hands. 6 For the heavy involvement of the visuomotor imagery process, MT leads to improved physical impairment through yielding activations in the motor-associated network of the brain. 7 Different from high-intensity motor practice, MT is a priming technique for brain activation used to re-establish the motor function of the affected limb by enriching the visual and proprioceptive inputs. 8 The beneficial effects of mirror visual feedback from MT on motor recovery could contribute to the reduction of imbalance in the motor cortex activity between the ipsilesional and contralesional hemispheres after stroke. 9 Recently, MT has been recommended to restore the sensorimotor function of chronic stroke patients as evidenced by a systematic review. 10
Arm-hand movement training in virtual reality (VR) is an effective strategy for promoting the functional motor recovery of stroke patients as VR provides a training environment involving intensive visual, auditory, and haptic feedback from computerized technology.11,12 The mirror visual illusion that emerges through VR systems strengthens multisensory integration, or the effect of visual signals interacting with bilateral proprioceptive signals. 13 Recent research revealed that the add-on effects of VR to MT empowered rehabilitation outcomes 14 for the engagement of a contralesional action observation network. 15 Through the visualization of the mirrored movements of the non-paretic limb 16 with a computer-generated scenario, VR-based MT (VR-MT) demonstrated its feasibility in interventions for patients with functional neurological disorder 17 and stroke. 18 However, little evidence is available regarding the use of VR-MT for a limited number of recruited patients, an inadequate research design, and low-intensity training.
The latest Cochrane review of interventions for improving upper limb function following stroke recommended using mirror therapy as a routine practice. 19 However, asymmetry in the sitting posture during the conducting of MT using a traditional mirror box will cause problems with movement learning and control. 20 VR technology provides beneficial effects on the management of motor symptoms for delivering highly immersive environments for motor learning. 21 The rationale for using VR-based mirror therapy for facilitating upper limb recovery following stroke includes multisensory neuroplasticity, 22 increasing the range and difficulty of the involved training programs, 23 and eliciting a stronger sense of ownership of the affected limb. 24 Thus, in this study, we proposed that embedding the mirror therapy within a VR system may have a superior effect on motor remediation. However, a recent scoping review literature found that the research on mirror therapy combined with VR technology is of low quality. 25 The present study investigated the differences in the effects of using COT, MT, and VR-MT training on the sensorimotor function of the upper limb in chronic stroke patients. We hypothesized that VR-MT may reduce impairment and enhance activity participation more than traditional MT and COT do for chronic stroke survivors.
Methods
This study used a 3-condition pragmatic randomized controlled trial design with pre-treatment, post-intervention, and 12-week follow-up assessments. The 3 conditions were COT, MT, and VR-MT. Each condition received a total occupational therapy care session of 50 minutes comprising 20 minutes of usual care (including therapist-facilitated task-specific training) and 30 minutes of the study condition, which was provided twice a week for 9 weeks. Two evaluators were blinded to the participant’s condition.
Participants: Patients were recruited from the department of physical medicine and rehabilitation at a medical center in South Taiwan between October 2017 and April 2020. The inclusion criteria for stroke patients were as follows: (1) chronic stroke patient with unilateral cerebral infarction or hemorrhage, and whose disease duration was more than 6 months following stroke, (2) an FM-UE score ranging from 23 to 60, corresponding to poor to notable arm-hand capacity, and (3) a mini-mental state examination (MMSE) score not lower than 24. The exclusion criteria were: CT showing multiple cerebral infarctions or hemorrhage; not being able to have a VR experience due to visual problems; severe hemi-neglect; and global aphasia leading to difficulty with following written or spoken multi-step instructions.
Demographic and baseline clinical characteristics of study participants.
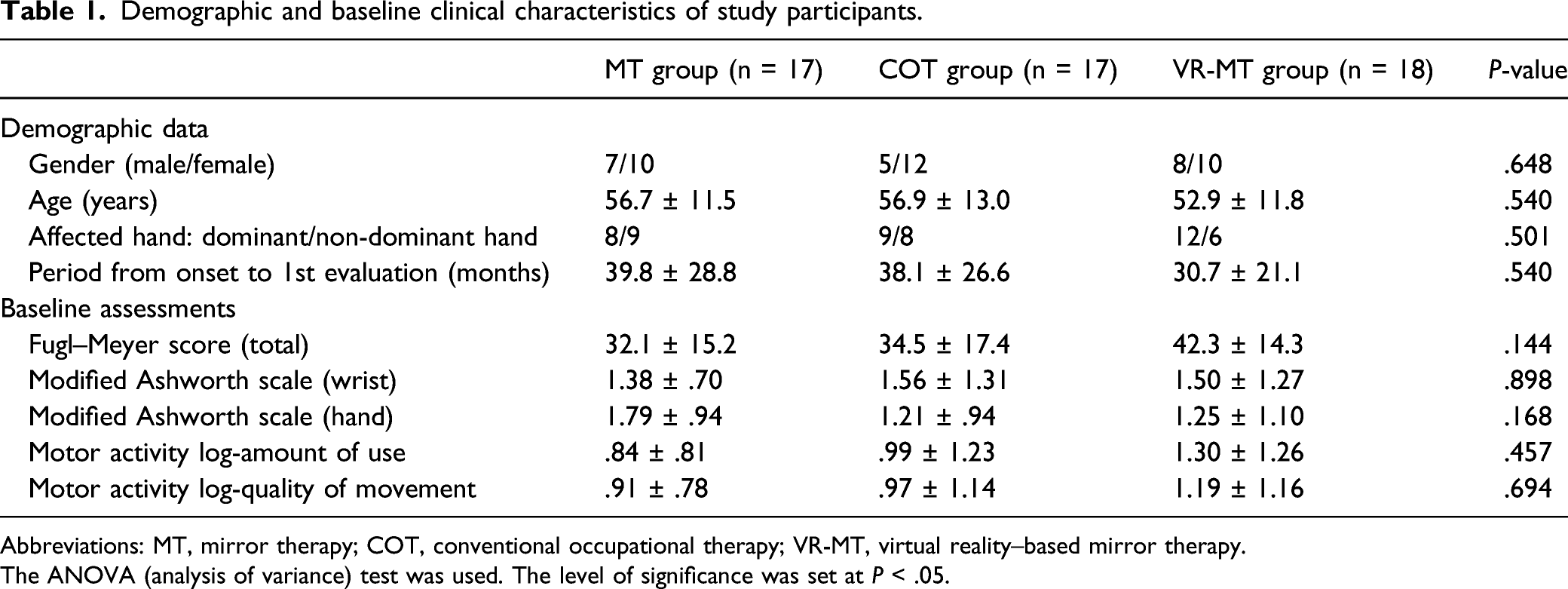
Abbreviations: MT, mirror therapy; COT, conventional occupational therapy; VR-MT, virtual reality–based mirror therapy.
The ANOVA (analysis of variance) test was used. The level of significance was set at P < .05.
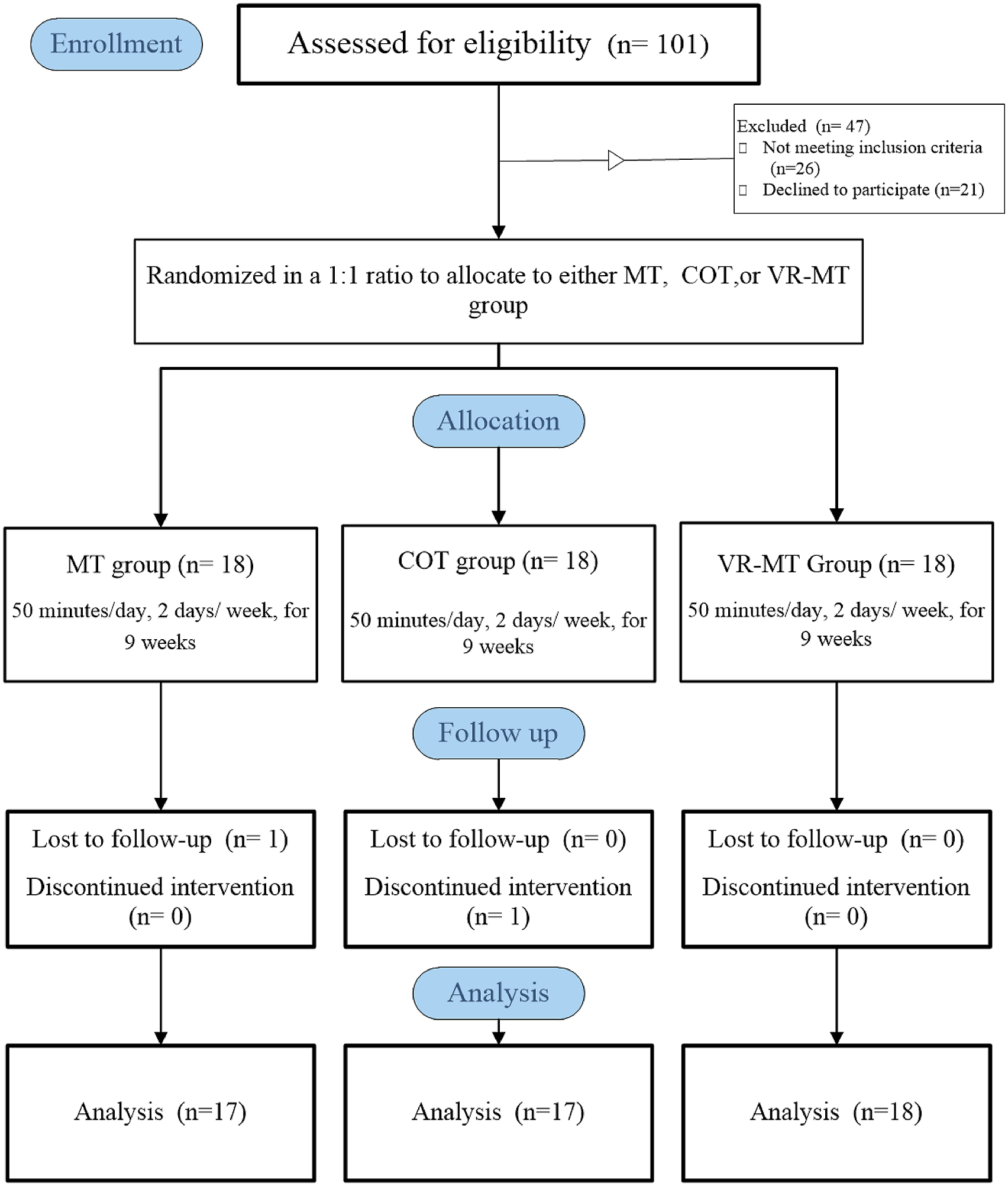
Flow chart of the enrollment of patients and completion of the study.
VR-MT system
26
: A personal computer–based desktop VR-MT system (Figure 2) was developed for providing immersive mirror visual feedback. The system contained a personal computer (operating system: Windows® 10; central processing unit: Intel i5-4590 equivalent or greater; Compatible HDMI 1.3 video output), a Leap Motion Controller (LMC) with 3 infrared light-emitting diode lights, 2 monochromatic infrared camera sensors as real-time motion capture devices for the hands, and an Oculus Rift as the VR headset. The Unity cross-platform game engine was used as the VR-MT system software. The VR mirror visual feedback was generated with the following procedures: (1) The LMC captures the joints’ coordinates in the unaffected hand; (2) the mirror hand position was calculated to obtain the joints’ coordinates in the affected hand; and (3) the joints’ coordinates in both hands were successfully generated and then displayed on the VR headset (Oculus Rift). (A) Schematic representation of virtual-reality based mirror therapy system; (B) an overview of the actual VR environment.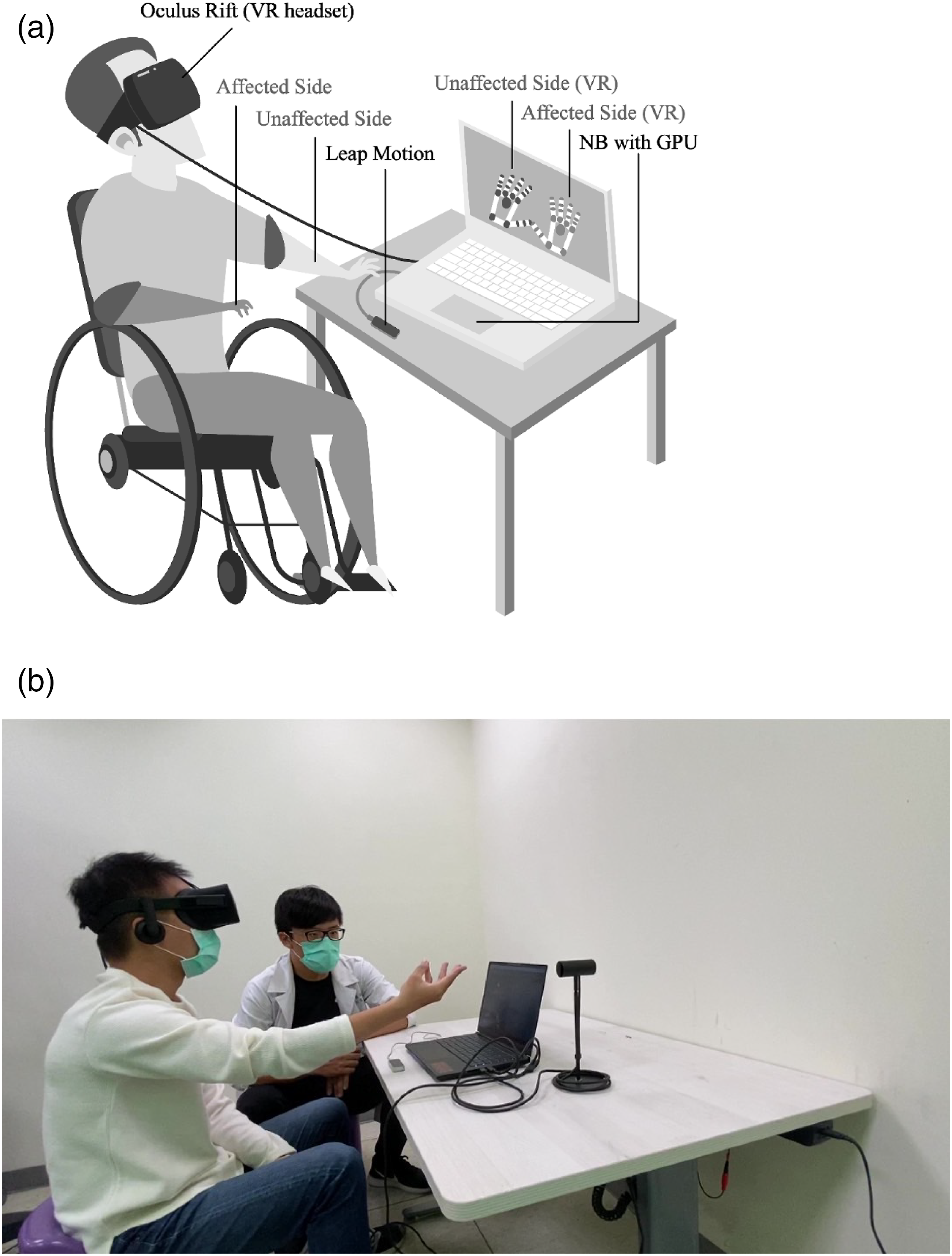
Interventions
MT, VR-MT, and COT exercises
Outcome Measurement
Demographic and Clinical Data Collection
The demographic data included age, sex, the side of the affected hand, and the time interval after stroke onset, and baseline evaluations were recorded (Table 1).
Primary Outcome Measure
Fugl-Meyer motor assessment for upper extremity (FM-UE): FM-UE is a quantitative measure for upper limb motor recovery after stroke with responsiveness to change. 28 The 33 items constituting the FM-UE were each scored on a 3-point ordinal scale: 2 points for being performed entirely, 1 point for being performed partially, and 0 points for no action being performed. This was a 66-point scale developed with 4 sub-scores: 36 for the shoulder/arm, 10 for the wrist, 14 for the hand, and 6 for the coordination subsection in the upper extremity. With respect to construct validity, a high correlation between the functional level and the total and the hand sub-scores of the FM-UE has been found in the stroke patients. 29 The minimal detectable change (MDC) is 5.2 points for the total score 30 and 1.64 for the sum of wrist and hand sub-scores 31 of the FM-UE for chronic stroke patients.
Secondary Outcome Measure
Motor activity log(MAL): The instrument consists of a semi-structured interview for examining how much (amount of use, AOU) and how well (quality of movement, QOM) the subject uses his or her affected arm. Both the AOU and the QOM are rated on a 6-point ordinal scale ranging from 0 to 5, with a higher score indicating better hand use in real-life situations. The MDC of the AOU and the QOM of the MAL is .56–1.06 for chronic stroke patients. 32
Box and block test (BBT): This is an efficient test for measuring a deficit in manual dexterity for stroke patients. The MDC for the BBT is 5.5 blocks/minute for stroke patients. 33 A higher score is indicative of better gross manual dexterity.
Semmes-Weinstein monofilament (SWM) test: The SWM test, a set of 20 nylon monofilaments, is used to determine the touch-pressure threshold of the hands with both intra- and inter-rater reliability for stroke patients. 34 When the sensory evaluation was conducted, monofilaments were applied to the affected thumb and exerted a constant force onto the skin for 1–1.5 seconds. An SWM was labeled with a numerical marking, a log to the base 10 of the force in tenths of milligrams. If the patient detected 2 out of 3 stimuli, this filament number was recorded. 35 A higher SWM test score represented poor sensation.
Modified Ashworth scale (MAS): This is reliable and frequently used in clinics for assessing upper extremity spasticity. The MAS scores are scored between 0 and 4, with higher scores indicating a greater severity of spasticity. 36
Ethics Statement
The research protocol received approval from the National Cheng Kung University Hospital Institutional Review Board (A-ER-105-213). Prior to participation, the participants signed a consent form listing the study’s aims and related procedures.
Adverse Effects Study Report Protocol
An adverse event in the study was defined as an affected upper limb injury, dizziness, and visual disturbance attributable to the intervention, which required a visit to a hospital. Participants were informed about the small increased risk during the informed consent process.
Statistical Analysis
SPSS 20.0 for Windows (Statistical Package for Social Sciences Inc. Chicago, IL, USA) was used for performing statistical analysis. Considering the effects obtained regarding the ability to improve the motor function of the paretic hands of stroke survivors who have undergone VR-based mirror therapy, an estimate of the sample size was made with an effect size of .45 (η 2 = .17), a 2-tailed alpha of .05, and a power of .80 on the FM-UE outcome of a previous study on mirror therapy for upper limb function in stroke patients. 37 It was determined that at least 17 patients should be recruited in each of the training groups to verify this study’s results. Assuming a dropout rate of 5%, we planned to enroll 54 patients in this study. Descriptive statistics were used to describe the means and standard deviations of the demographic data and all of the outcome measures. The normality of the data distribution was examined using the Shapiro-Wilk test. The analysis of variance (ANOVA) test was used to compare the disease characteristics and the clinical data of the patients at baseline depending on the distribution. To account for autocorrelation in repeated measurements on the same participant, the generalized estimating equations (GEE) method with unstructured variance-covariance matrix adjusted by baseline pre-treatment score was used to identify different intervention effect for improving upper limb function over time, with the intervention protocols (MT, COT, and VR-MT) serving as the factors. The main effects of time, group, and the group-by-time interaction were evaluated. The baseline pre-treatment score was used as a covariate considering that patients with better pre-treatment scores were likely to have better treatment responsiveness compared with those with worse pre-treatment scores. The GEE method was also used to examine within-group differences across results at the different time points of the baseline, post-intervention, and follow-up. The statistical significance level was set at P < .05.
Results
Fifty-four chronic stroke patients with mild to severe motor impairment were recruited in the MT, TOT, and VR-MT groups with mean ages of 56.0 ± 11.5, 56.0 ± 13.2, and 52.9 ± 11.8 years old, respectively. During the study, 2 patients (1 in the MT group and 1 in the COT group) dropped out for dwelling place changing and medical worsening. (Figure 1). The training effects were analyzed based on 52 participants who completed the study. Table 1 summarizes the characteristics of age, disease duration, and the severity of the affected upper extremities of the 52 patients. No across-group differences exist on any measure at baseline; however, the difference between baseline FM-UE scores for VRMT and MT group and for VRMT and COT group was greater than the MDC of FM-UE. In addition, the study had no reported adverse effects.
Descriptive and inferential statistics for the results of FM-UE, MAL, MAS, SWM, and BBT.
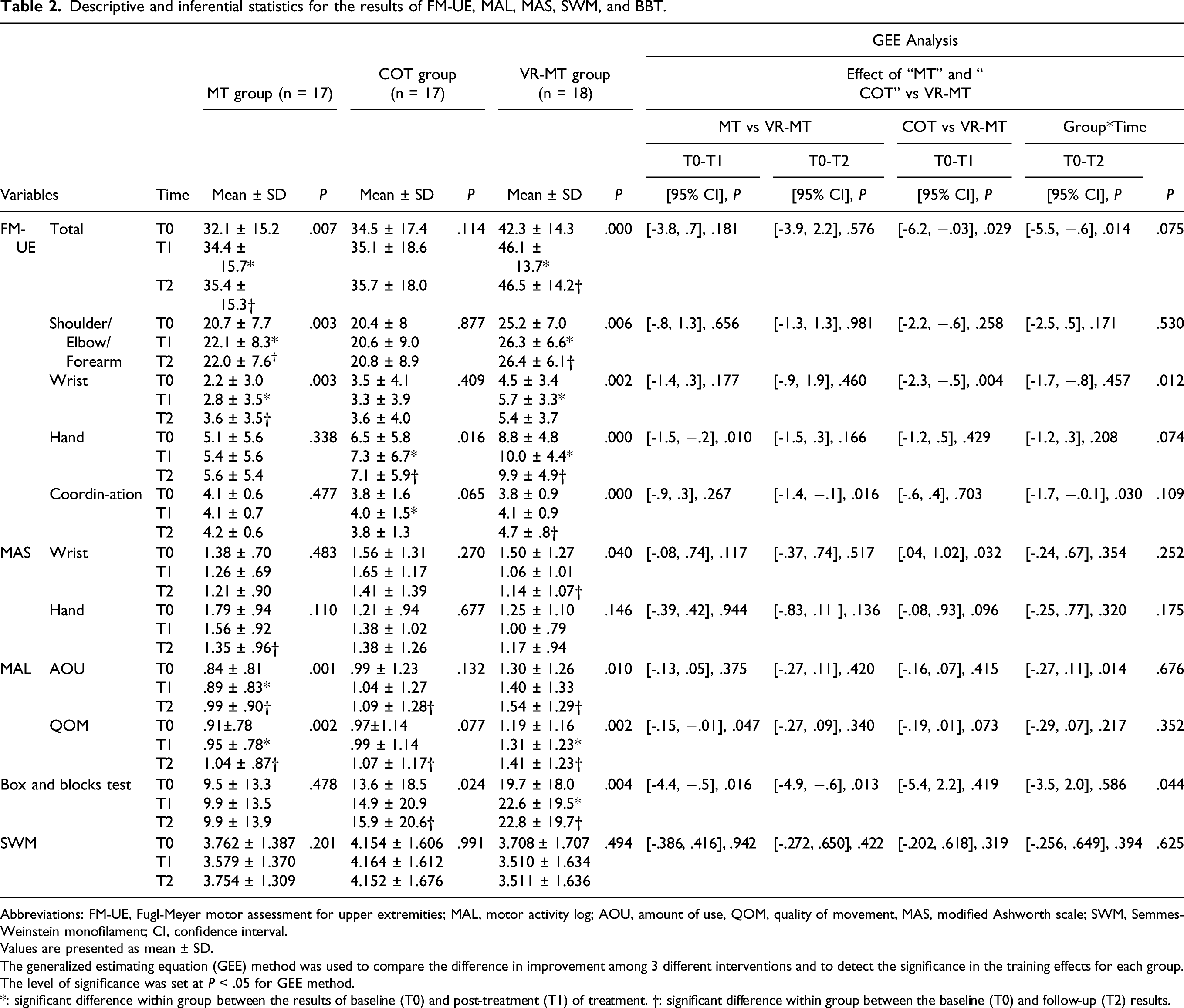
Abbreviations: FM-UE, Fugl-Meyer motor assessment for upper extremities; MAL, motor activity log; AOU, amount of use, QOM, quality of movement, MAS, modified Ashworth scale; SWM, Semmes-Weinstein monofilament; CI, confidence interval.
Values are presented as mean ± SD.
The generalized estimating equation (GEE) method was used to compare the difference in improvement among 3 different interventions and to detect the significance in the training effects for each group.
The level of significance was set at P < .05 for GEE method.
*: significant difference within group between the results of baseline (T0) and post-treatment (T1) of treatment. †: significant difference within group between the baseline (T0) and follow-up (T2) results.
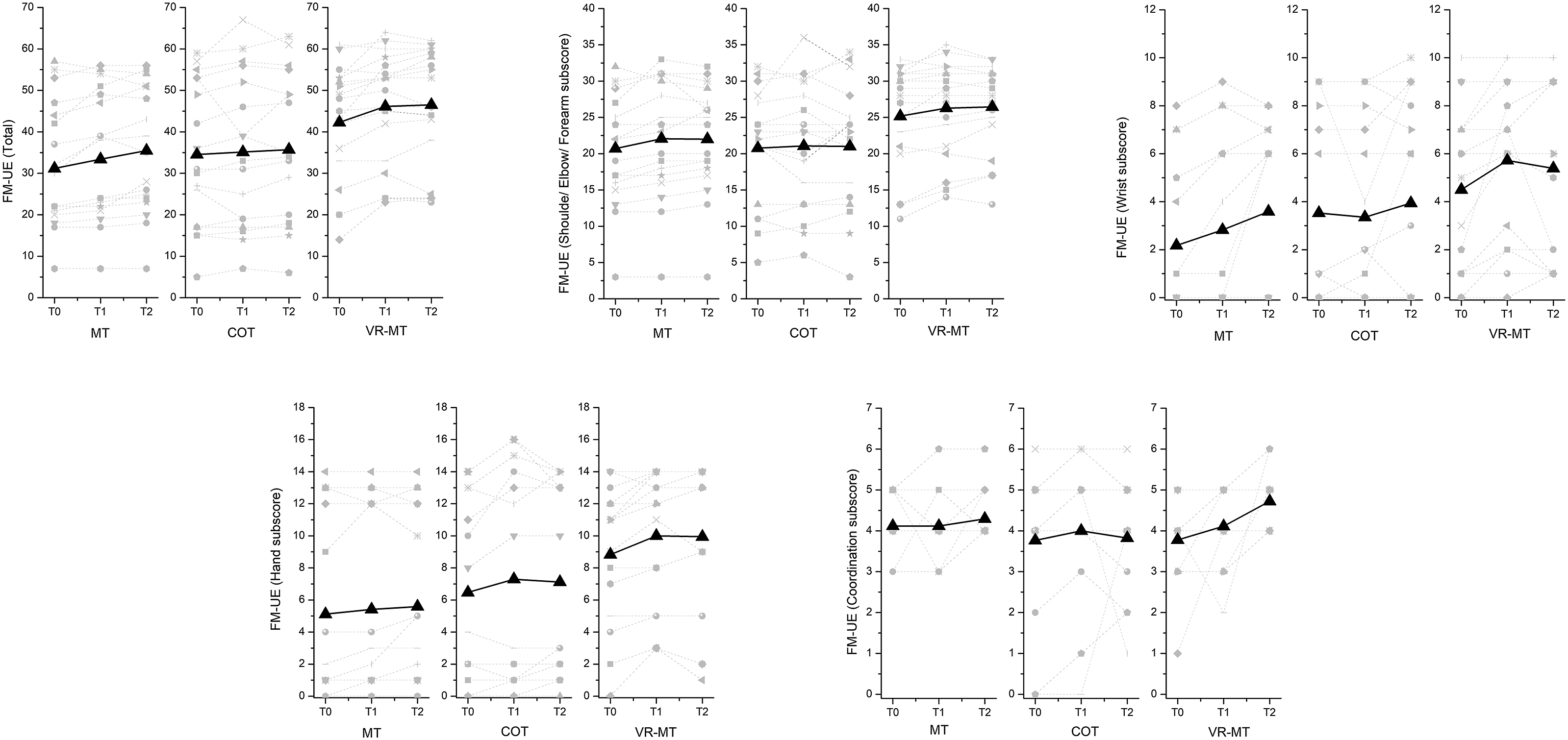
Individual (light gray color: dashed line) and mean (black color: solid line) score in the total and the sub-score of FM-UE of the participants for each time-point (T0: baseline, T1: post-treatment and T2: follow-up) and each treatment condition. Note: For some data points were with same values, lesser number of data points were found in the figure.
With regard to the motor function subsections, the group-by-time interaction effects on the wrist sub-score (GEE, P = .012) of FM-UE was with statistical significance. In particular, VR-MT has beneficial effects on wrist training (GEE, P = .004) compared with COT training. In addition, the better improvement in UE coordination for patients in the VR-MT group was compared with patients in COT (GEE, P = .030) and in MT (GEE, P = .016) group at follow-up evaluation. The FM-UE shoulder/arm and wrist sub-score showed significant within-group improvement in the VR-MT (GEE, P = .006 and GEE, P = .002, respectively, for the shoulder/arm and wrist sub-score) group and MT (GEE, P = .003 and GEE, P = .003, respectively, for the shoulder/arm and wrist sub-score) group but not in the COT (GEE, P = .877 and GEE, P = .409, respectively, for the shoulder/arm and wrist sub-score) group. In addition, in both the COT (GEE, P = .016) and VR-MT (GEE, P = .000) groups, a significant within-group increase was found in the mean values of the hand sub-score. For the patients in the VR-MT group, the mean change value of the sum of wrist and hand sub-scores was 2.2 between the pre-treatment and post-intervention, and it was 2.0 between the pre-treatment and follow-up, which was greater than that of the MDC (1.64). Furthermore, the mean changes in the wrist component of the MAS scores in the VR-MT group, from pre-treatment to post-intervention, achieved a significant within-group difference (GEE, P = .013).
A statistically significant group-by-time interaction effect was found in the BBT result (GEE, P = .044). Compared to the MT group, VR-MT group bas better effect at post-intervention (GEE, P = .016) and follow-up (GEE, P = .013) evaluation. The within-group improvement of the BBT results was found in the VR-MT (GEE, P = .004) and COT group (GEE, P = .024). The effect of VR-MT and MT also had functional consequences for increasing the amount (GEE, P = .010 and GEE, P = .001, respectively, for VR-MT and MT) and quality (GEE, P = .002 and GEE, P = .002, respectively, for VR-MT and MT) in the usage of the affected arm. However, the change values were .24 for the AOU and .22 for the QOM in the VR-MT group for the follow-up, which was less than the MDC for the AOU and the QOM of the MAL.
Neither significant group-by-time interaction effects nor within-group differences in either of the 3 conditions (P > .05) were found for improving the touch-pressure sensibility assessed via the SWM test.
Discussion
This study examined the difference in the effects of MT, COT, and VR-MT in conjunction with 20 minutes of therapist-facilitated task-specific training aimed at motor, sensation, and task performance of the upper extremities of chronic stroke patients. The obtained findings in the current study suggest that the change in total score of FM-UE did not differ statistically with group-by-time interaction effects. Although the patients in the VR-MT and MT groups made statistically significant improvements in the FM-UE total scores following intervention, the training-induced gains in the FM-UE of each condition did not exceed the MDC. In addition, VR-MT enhanced more significant gains in the FM-UE wrist sub-score at post-intervention compared with the COT intervention and made better improvements in the FM-UE coordination sub-score between the pre-treatment and follow-up evaluations compared with the COT and MT interventions for chronic stroke patients. Moreover, there were group-by-time interaction effects on BBT; VR-MT showed more significant increases in the BBT compared with the MT intervention at post-intervention and follow-up evaluations. The results partially supported the hypothesis that VR-MT has better effects on enhancing the motor function of the affected upper limb in stroke participants.
A simple movement-based hand exercise through VR goggles was used in this experiment to study the effects of VR-MT on motor recovery. The obtained results showed a superior effect on improving the motor impairment of the affected wrist and coordination in chronic stroke patients. The VR technology and VR headset were used as mediums of action observation of bilateral hand movements, 38 which could be an add-on treatment to regular neuro-rehabilitation for stroke patients. A recent research study revealed that the new mirror therapy interface leads to motor improvements, 39 which supported the current study’s findings.
There were no statistically significant group-by-time differences in both the self-perceived amount and the quality of the use of the affected arm in the current study. However, the AOU and QOM of the affected upper limb assessed via the MAL improved significantly for patients who received either MT or VR-MT, in addition to motor function. As supported by a recent research study on a VR-based mirror therapy, bilateral cortical excitability modulation due to interhemispheric communication through mirror feedback during treatment was likely to decrease motor impairment as well as the functional use of the affected upper limb of chronic stroke patients in the MT or VR-MT group in the study. 40
Statistically significant improvement in the FM-UE hand sub-score was also found for participants in the VR-MT and COT groups. The results obtained for the VR-MT group were similar to those of the study of Hoermann and colleagues. 23 Hand capacity improvement was found following MT with augmented reflection technology on the stroke upper limb capacity scale. Bilateral priming effects with a strong ownership sense of the affected limb 41 could be benefits of improving motor function. COT programs involve facilitating daily task performance through the mixture of skill training and task performance, which is a powerful technique for driving a change in hand performance. 42
Another aspect to highlight is the statistically significant group-by-time interaction effects on the BBT result. The BBT improved with statistical significance for patients receiving VR-MT in the current study, which was different from the finding of a previous VR-MT research study. 18 In the previous study, a relatively severely impaired population was recruited, which might have reduced VR-MT’s capacity for remediating motor impairments. The VR image of the non-paretic upper limb was suppressed in the previous study, which might have also weakened MT’s effect on balancing cortical activation between hemispheres, as numerous studies have supported the efficacy of MT with bilateral training.9,43
The rationale for improving sensory function following VR-MT receives support from a recent research study related to brain activation patterns for mirror therapy. 44 Stronger activation occurred in the primary sensorimotor cortex for VR-based mirror therapy than in the traditional mirror box condition. The synchronous multisensory perception, looking at the mirror hand presented in a VR scenario, increases activation in somatosensory areas more than seeing the hand in a mirror. 45 However, the touch-pressure sensibility of the affected hand did not reveal a significant change in the VR-MT group. It is worth noting that the effects of mirror therapy on sensation have rarely been discussed. 46 Only 1 randomized control trial found that mirror therapy improved temperature sense. 37 Tactile stimulation was not part of the treatment program, which contributed to reduced effects on tactile sensibility in the current study. Further research investigating the effects of adding haptics to MT or VR-MT on the sensory function of the affected hand for patients with stroke is needed.
The results of previous research demonstrated that mirror therapy using advanced technology, such as a camera, 47 augmented reflection, 23 and VR, 18 is a feasible strategy for improving upper extremity function safely. Overall, the evidence is minimal, as only low numbers of small-sized trials were available, and the study design quality was poor. The strength of the current study is that involved the larger sample size of 54 participants recruited and randomly allocated to the VR-MT, COT, and MT groups to examine the effects of VR-based mirror therapy on improving motor function and the performance of the affected upper limb in the current study. In addition, for the purpose of understanding the details in the change of the motor status of the upper extremity, the total scores and 4 subsection FM-UE scores were each examined and discussed in the current study, although the use of FM-UE sub-scores separately is not standard. However, some limitations of the study should be discussed. First, the trial was a single-center study and lacked long-term follow-up, thus limiting the generalizability of the study findings. Second, the relative small sample size led to a heterogeneous baseline FM-UE score in the 3 treatment conditions despite the fact that the study had a randomization control trial design. VR-MT group already had a big difference at baseline FM-UE score might have impacted the expected effect of VR-MT training. In addition to these limitations, the non-significant group-by-time interaction effects on primary outcome led the evidence for the effect of adding VR to MT seems to be rather weak. Future research studies on cortical activity due to VR-MT are needed to better understand the underlying neural mechanisms of VR-MT. In addition, task-oriented mirror therapy provided more superior effects on the upper extremity function; 48 thus, the effects of task-based VR-MT on the upper limb motor function of stroke patients should be investigated in future work.
Conclusions
This study suggested that VR-MT has potential treatment effects on restoring motor skills and the function of the affected upper extremity in chronic stroke patients. Motor remediating in a mirror therapy task with immersive virtual feedback may help to foster bilateral prime brain activation with the multisensory integration of visual and bilateral proprioceptive signals, thus triggering better motor learning effects.
Footnotes
Acknowledgments
The authors are grateful to Dr. Sheng-Hsiang Lin and Ms Wan-Ni Chen for providing the statistical consulting services from the Biostatistics Consulting Center, Clinical Medicine Research Center, National Cheng Kung University Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work received support from the ministry of science and technology (MOST), Taiwan. [Grant number: 106-2314-B-006-049-MY2].