
Abstract
Background and Purpose. Individuals with stroke often present symptoms of multiple domains, such as weakness of the affected upper extremity (UE) and unilateral spatial neglect (USN), which are both associated with poor functional outcome. The aims of this systematic review were to search and review studies that investigated (1) the relationship between USN and affected UE sensorimotor recovery poststroke and (2) the effectiveness of sensorimotor interventions to improve the affected UE in patients with USN. Methods. An electronic search of databases (MEDLINE, EMBASE, CINAHL and Cochrane CENTRAL) was conducted using a combination of the following terms: stroke, USN, and affected UE. Studies meeting the inclusion criteria were rated using a modified version of the Quality Index, and relevant data were extracted. Results. A total of 850 studies were identified, and 14 were included; 13 studies assessed correlations between USN and the affected UE capacity/recovery, and 1 study assessed an intervention to improve the UE of individuals with USN. An association between presence of USN and UE capacity/recovery was found in most studies and USN did not interfere with recovery of the affected UE in the single experimental study. Conclusions. USN is associated with poor UE motor capacity and less UE recovery poststroke. Therefore, these impairments should be considered when planning rehabilitation and discharge. Because USN is a well-researched phenomenon, the lack of studies and insufficient evidence related to UE interventions in individuals with USN was unexpected. These interventions should be developed and researched to improve UE and overall functional outcome poststroke.
Keywords
Introduction
Stroke is a worldwide leading cause of long-term disability. 1 Possible consequences of stroke include motor and cognitive impairments, 2 with survivors often presenting with impairments of multiple domains, 3 leading to decreased independence in basic (BADL) and instrumental activities of daily living (IADL), dissatisfaction with life, and depression.4,5
Upper extremity (UE) sensorimotor impairments on the contralateral side to the brain lesion are very common poststroke and include weakness (paresis) to paralysis, inability to isolate movements, abnormal muscle tone, and changes in somatosensation.6,7 UE impairments were found to predict poor functional outcome8-10 and long-term decreased subjective well-being. 11 Therefore, improving the motor and functional ability of the affected UE is one of the main goals of stroke rehabilitation.12,13 The limited recovery and inability to use the affected UE in daily function poststroke has been widely reported.7,14 Furthermore, improvement in UE functional capacity does not guarantee a parallel improvement in UE actual daily use,15,16 suggesting that there are different factors affecting the complex process of UE recovery. Many studies have aimed to identify the factors that can predict UE functional recovery but have focused mainly on motor factors, such as initial motor impairment and spasticity,9,17 and only a few studies have focused on cognitive impairments, such as the presence of unilateral spatial neglect (USN).
USN is the failure to respond to stimuli presented on the contralesional side and occurs in 25% to 48% of individuals with stroke.18,19 The USN phenomenon has been widely researched, and its presence was found to be related to lower levels of independence in BADL and IADL,20,21 greater risk of falls, 22 longer lengths of hospital stay, and overall poorer functional outcome compared with individuals without USN.23,24 Interventions aimed at improving USN have been developed, implemented, and researched extensively.25,26 However, because USN may directly or indirectly affect UE motor recovery, such as by patients not paying attention to the affected UE during function or during therapeutic sessions, failure to fully implement motor learning techniques, interventions should not only focus on improving USN, but also focus on improving the affected UE when USN is present.
Indeed, some studies have investigated the association between cognitive impairments and UE motor recovery. For example, a previous review 27 addressed spatial cognition and motor recovery after stroke. USN was identified as a key element that may impede UE motor and functional recovery and that should be taken into account during rehabilitation. In another systematic review and meta-analysis, 28 authors found associations between attention and executive function deficits and UE motor recovery and suggested that these impairments should be taken into consideration when planning treatment. Because this review excluded studies that included patients with USN, the associations with USN are unknown. In another systematic review, 29 the impact of USN on goal-directed arm movements was researched, and USN was found to be related to impairments in tasks that required perceptual, memory-guided, or delayed actions. This systematic review, however, included only studies with movements performed with the less-affected (stronger) UE. Although some conclusions may be cautiously drawn from these reviews, it remains unclear how USN affects sensorimotor recovery of the UE and if current interventions are as effective in patients with USN compared with patients without USN.
The aims of this systematic review were to search and review studies that investigated (1) the relationship between USN and motor or functional recovery of the affected UE after stroke and (2) the effectiveness of sensorimotor interventions to improve the affected UE in patients with and without USN. The focus of this systematic review is on UE recovery and not daily function—that is, achieving independence in daily activities.
Methods
This systematic review was registered in PROSPERO (CRD42018096456) and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) statement. An electronic search of several databases, including MEDLINE, EMBASE, CINAHL, and Cochrane CENTRAL, was conducted in February 2018. A combination of the following terms was searched: cerebral vascular accident, unilateral spatial neglect (USN), and affected upper extremity (UE). Exact terms and synonyms were determined based on a broad literature review, previous studies, and clinical experience (see Supplementary Appendix for the complete MEDLINE search strategy). There were no restrictions on year of publication. Further studies were identified by searching the reference lists of relevant studies.
After removing duplicates, titles and abstracts were screened by one author, according to the following inclusion criteria: (1) participants were adults poststroke; (2) study design was observational or experimental; (3) outcome measures included at least 1 measure for USN and 1 measure for UE sensorimotor capacity or function; (4) full text was available in English. Case studies were excluded as well as studies that included participants with other neurological disorders—for example, traumatic brain injury, Parkinson’s disease. If the intervention provided was aimed at improving USN symptoms (and not the UE), these studies were also excluded, unless UE outcome measures postintervention were also provided.
The full text of relevant articles was retrieved and further reviewed by the authors and research assistants. Quality assessment of studies was done using a modified version of the Quality Index checklist, 30 which also includes questions from the Quality Assessment Scale by Crombie and Harvey. 31 This version has been previously used in other systematic reviews to assess the quality of observational studies.29,32 Each article was rated on a 20-item scale, scoring between 0 and 20, when a higher score indicates higher quality (0-9, poor; 10-14, fair; 15-20, good quality). Studies were rated by 2 independent raters, and disagreements were discussed and clarified. If not, a third rater assessed the study.
Data extraction included the following: study design, description of the study population and timing of assessments, outcome measures used to assess USN and UE motor impairment or function, type of intervention used in experimental studies, and relevant findings. The main findings regarding each study were identified, and a narrative synthesis of the results was conducted.
Results
A total of 850 studies were identified, 34 full texts were assessed for eligibility, and a total of 14 studies were included in this systematic review (see Figure 1, the PRISMA chart). A total of 13 studies14,23,33-43 included testing of correlations between USN and the affected UE capacity or recovery; of these, 11 studies14,23,33-41 were observational studies, and 2 studies42,43 were a secondary analysis of an experimental design. Only 1 of the 14 included studies specifically researched the effect of an UE intervention provided to participants with USN. 44 The aims, design, and methods used for the various studies were heterogeneous. In addition, a diversity was seen in the assessment tools used to assess USN and in the outcome measures to assess the affected UE.
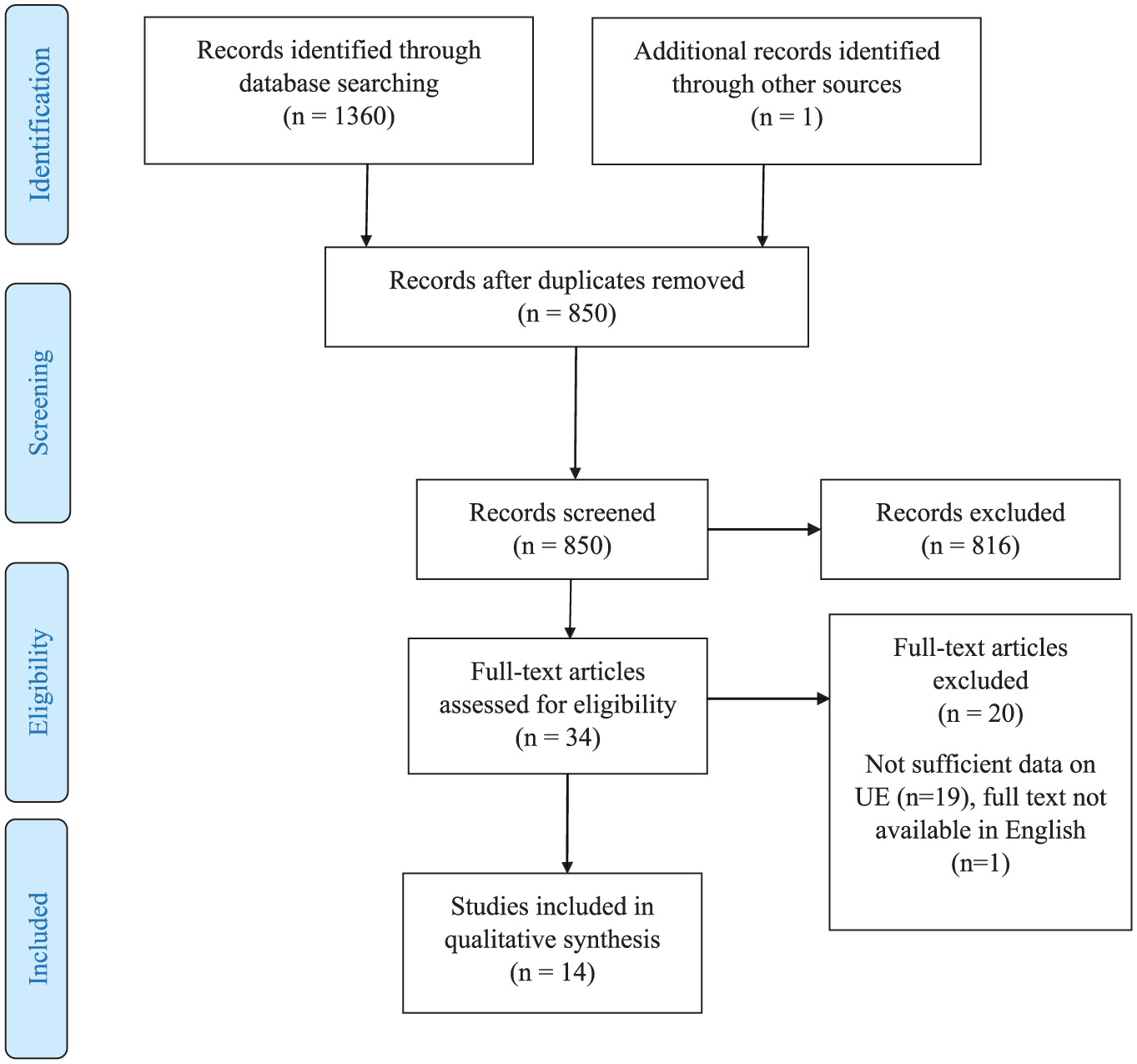
PRISMA chart.
Characteristics of Included Studies
Table 1 presents the design, population, USN and UE assessment tools used, timing of assessments, and quality of the 14 studies. All studies included adults poststroke; 2 studies included participants with only right hemisphere damage,23,41 and 1 study 40 included only participants without voluntary finger extension during the first 2 weeks after stroke. Nine studies were longitudinal (8 prospective14,23,36-41 and 1 retrospective 35 ), with the first assessment conducted between 1 and 6 weeks poststroke and final assessment conducted between 3 months to 1 year poststroke. Two studies were cross-sectional, with a single assessment, performed between 2 and 4 weeks poststroke 33 and 6 months poststroke. 34 Two additional studies were experimental42,43 and included USN in a secondary analysis as a possible factor affecting UE outcome following the intervention. Only 1 study that assessed the effectiveness of an UE intervention for individuals with USN was found. 44 This pilot study included a single group of 20 individuals with USN at the chronic stage poststroke and assessed UE improvement following 6-week repetitive task-specific training (3 sessions/wk) using a repeated-measure design. All studies were rated as fair to good quality according to the modified Quality Index.
Description and Quality of Included Studies.
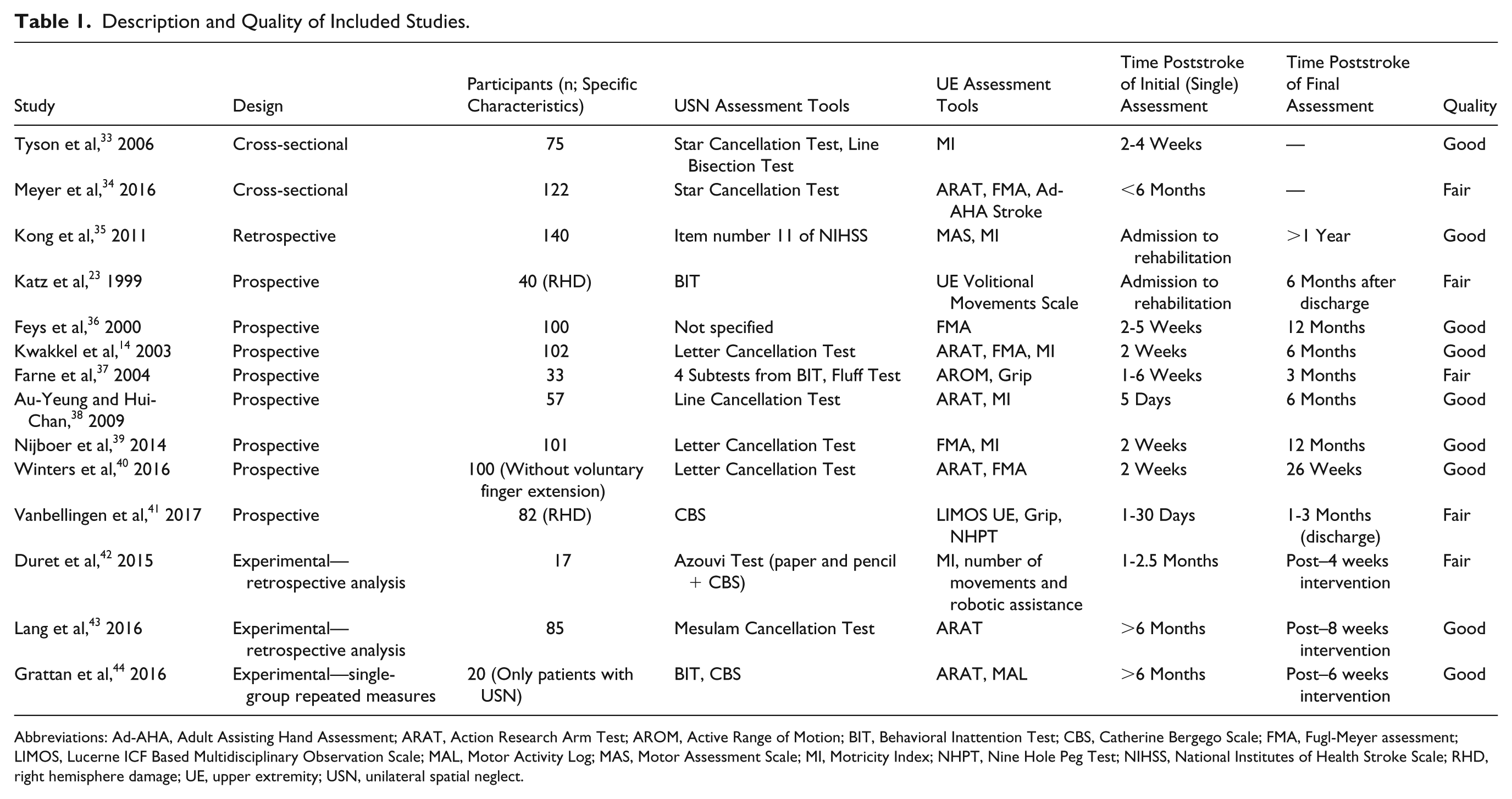
Abbreviations: Ad-AHA, Adult Assisting Hand Assessment; ARAT, Action Research Arm Test; AROM, Active Range of Motion; BIT, Behavioral Inattention Test; CBS, Catherine Bergego Scale; FMA, Fugl-Meyer assessment; LIMOS, Lucerne ICF Based Multidisciplinary Observation Scale; MAL, Motor Activity Log; MAS, Motor Assessment Scale; MI, Motricity Index; NHPT, Nine Hole Peg Test; NIHSS, National Institutes of Health Stroke Scale; RHD, right hemisphere damage; UE, upper extremity; USN, unilateral spatial neglect.
Assessment tools for USN included mainly paper and pencil tests, such as the Star Cancellation Test, Letter Cancellation Test, Line Bisection Test, and partial or complete admission of the Behavioral Inattention Test, as was seen in 11 of 14 studies.* The Catherine Bergego Scale, an observation of the participant’s function, was used in 3 studies41,42,44 to assess USN, relevant items from the National Institutes of Health Stroke Scale were used in another study, 35 and 1 study 36 did not specify the tool used but defined USN as being present or not present. Some studies used only 1 assessment to determine presence of USN, whereas in other studies 2 or more tests were used. Outcome measures to assess the affected UE included screening tools (Motricity Index14,33,35,38,39,42), tools for assessing motor impairment (Fugl-Meyer Motor Assessment14,34,36,39,40), or tools for assessing UE functional capacity (Action Research Arm Test14,34,38,40,43,44). One study 34 used the Adult Assisting Hand Assessment Stroke, which is an observational tool used to assess the affected UE use while performing a bilateral functional task. Another study 41 used a modified version of the Lucerne ICF based Multidisciplinary Observation Scale to assess UE use in ADLs. One experimental study 42 also used the number of repetitions of movements performed during a robot-assisted session as an UE outcome measure.
Findings of Included Studies
Table 2 presents the general findings of the 13 observational studies and specifically, whether an association exists between USN and UE capacity or recovery. A total of 10 observational studies14,23,33-37,39-41 reported that the presence of USN was associated with poor motor UE capacity or function. Of these, the 2 cross-sectional studies found a significant association between the presence of USN and poor motor scores both at 2 to 4 weeks 33 and at 6 months 34 poststroke, and the longitudinal studies14,23,35-37,39-41 found USN to be a significant predictor of poor motor capacity of the affected UE. One study, which included repeated assessments of USN and UE motor impairments over 52 weeks, found the association between these impairments to be the most pronounced during the first 10 weeks poststroke. 39
Findings of Included Studies.
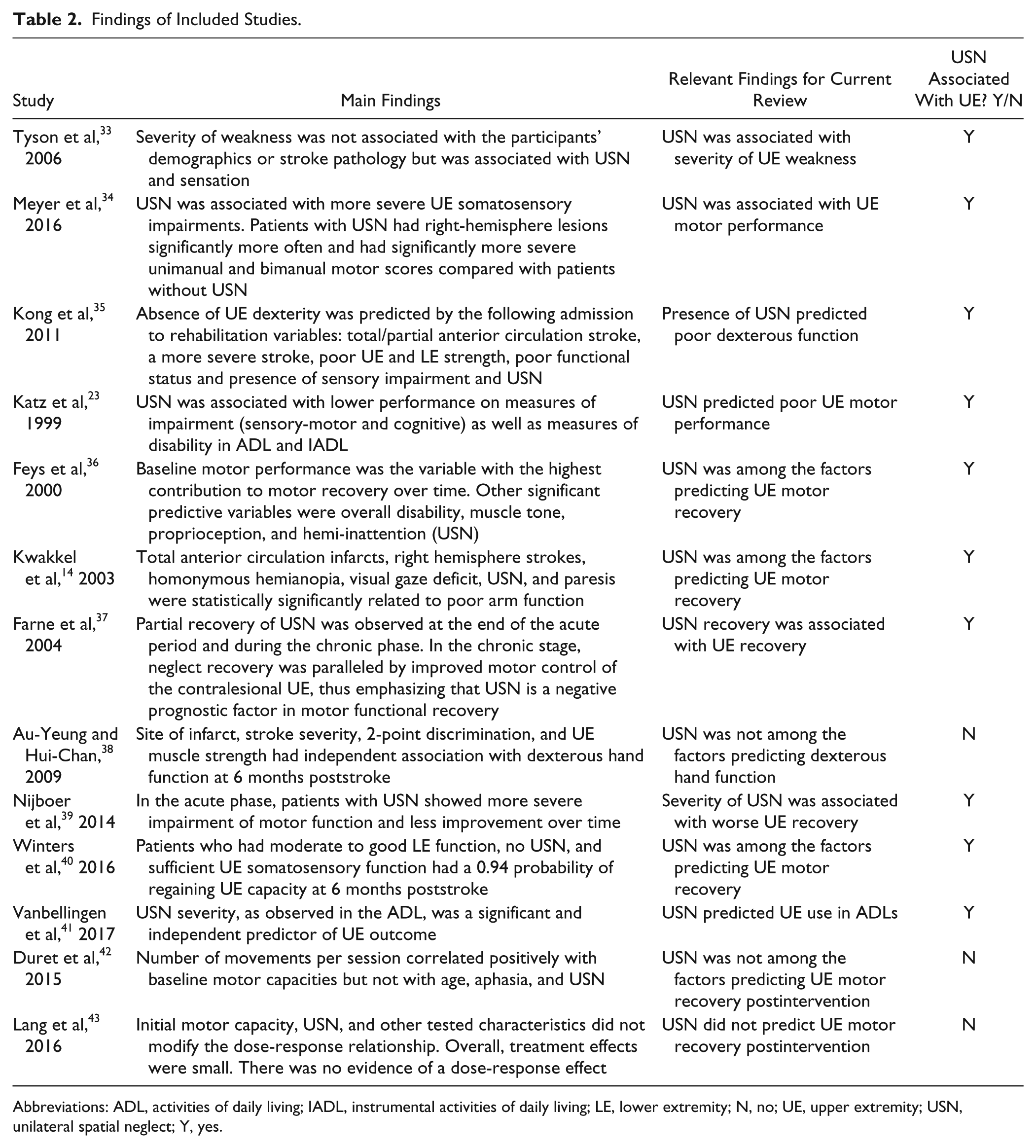
Abbreviations: ADL, activities of daily living; IADL, instrumental activities of daily living; LE, lower extremity; N, no; UE, upper extremity; USN, unilateral spatial neglect; Y, yes.
Three studies did not find an association between USN and UE variables.38,42,43 One prospective study 38 did not find USN to be a predictor of dexterous hand function at 6 months poststroke. Correlations were also not found between the presence of USN to UE improvement following UE treatment as assessed in a secondary analysis in the following 2 experimental studies. USN, as assessed at baseline prior to a 4-week combined robot-assisted practice (4 sessions/wk) in addition to conventional occupational therapy (4-5 sessions/wk) for improving the affected UE poststroke, was not found to be associated with UE motor performance postintervention. 42 The presence of USN was also not found to affect the dose-response relationship of participants with chronic stroke who participated in a 4-arm randomized controlled trial assessing task-specific intervention (4 sessions/wk during 6 weeks). 43
In the only experimental study 44 that was included in this review, participants with USN, who participated in the 6-week repetitive task-specific practice, reported satisfaction from the intervention, and significant but small improvements were seen for UE motor and functional measures.
Discussion
This systematic review aimed to address 2 clinically relevant questions faced by clinicians when treating patients following stroke and emphasizes the complexity of treating individuals who demonstrate a wide range of motor and cognitive symptoms. Initially, the aim was to investigate the relationship between the presence of USN and UE motor impairment or UE recovery in individuals with stroke.
This question has been previously addressed by others, who concluded that individuals with USN demonstrate worse functional outcome when compared with individuals without USN.20,24,27 A total of 10 of the 13 studies in this review also revealed that the presence of USN is associated with poor UE motor capacity, in the subacute as well as in the chronic stages poststroke. This information may help predict rehabilitation outcomes, and plan treatment and discharge and is, therefore, relevant for clinicians and decision makers to ensure that the interventions are effective and tailored for their patients. An association between USN and UE capacity was possibly not found in 3 of the 13 studies, because the focus was on the recovery of dexterous hand function, 38 which characterizes individuals with less motor impairment and more UE functional ability, and sufficient statistical power was lacking in the 2 experimental studies,42,43 which assessed the influence of USN as a secondary analysis following the intervention and included very few participants with USN in each group.
The evidence above emphasizes the disadvantage that individuals with USN have when considering the affected UE, having less UE recovery compared with individuals without USN. Therefore, it was surprising to find only 1 study 44 that specifically addressed the influence of USN on UE outcomes following intervention. In this study, only participants with USN were included; therefore, it is unknown how individuals without USN would respond to the intervention. In other words, the second aim of this systematic review, which has not previously been investigated, revealed a lack of research regarding the effectiveness of sensorimotor interventions to improve the affected UE in patients with USN.
Treating the UE of individuals with USN is very challenging because these individuals have difficulties focusing their attention on their affected UE during the therapeutic sessions, often cannot search or locate their hand, and experience difficulties watching their hand while it is moved (by the clinician). Because visual feedback is important for the practice and learning of movements, 45 especially in patients who have sensory deficits, this fact may impede their UE recovery. Furthermore, sustained attention, often impaired in individuals with USN, 46 has a critical role in the motor recovery process after stroke. 47 Therefore, interventions aimed at improving the affected UE of individuals with USN should be developed and implemented to practice visual scanning and UE movements to decrease these impairments and to increase overall function. Some studies have suggested providing treatment for USN while incorporating additional techniques involving the UE—for example, increasing patient’s attention to their affected UE while practicing passive or active-assisted movements,48,49 focusing on goal-directed movements toward stimuli presented on the affected side, 50 or using the task-specific approach using the affected UE. 51 Using USN interventions as an integral part of the sensorimotor treatment might also be beneficial, 27 such as seen in a study that used eye-patching to improve USN, which resulted in UE improvement as well. 52 Future research should assess the effectiveness of these combined interventions on the affected UE as well as improving USN.
Findings from the 3 experimental studies included in this review42-44 are also encouraging because they suggest that individuals with USN may benefit from UE interventions despite the initial disadvantage USN poses. Because very few participants with USN were included in the 2 studies42,43 and the third included only participants with USN, 44 further research is needed to shed light on the specific influence of USN on UE recovery.
The UE in the included studies was assessed utilizing different assessment tools, which assessed the UE motor capacity, such as the ability to produce isolated movements, range of motion, and strength. Because motor capacity is not necessarily parallel with function or daily use of the UE7,15 and may also be affected by USN, it is important to incorporate assessment tools that assess UE function.
USN is considered a very well-researched phenomenon. However, because the tools used to capture and characterize USN are limited, not functional, and vary between studies,49,53 the reported prevalence of USN following stroke is not precise.18,19 Most of the reviewed studies used 1 or 2 paper and pencil tests to assess the presence of USN; however, it is known that because different types of USN exist, using a test battery to assess USN is more sensitive than any single test alone. 54 Furthermore, studies reporting the prevalence of combined UE weakness with USN were not found, and therefore, this is unknown.
Not only is USN not the focus in many studies addressing UE assessment or treatment poststroke, very often, patients with USN are intentionally excluded from these studies. For example, the following randomized controlled trials that investigated the effectiveness of Constraint Induced Movement Therapy55,56 and robot-assisted therapy 57 to improve the affected UE excluded participants with USN. In other studies that do not define USN as an exclusion criterion, information regarding the presence or severity of USN is usually not provided. 12 This is perhaps understandable from a methodological point of view, to exclude confounding variables; however, it limits the generalization of the findings to individuals with USN. This isolation can obviously not be done when treating patients in the clinical field, who often present a variety of impairments in conjunction.
This systematic review included only studies published in English; therefore, a language bias might exist. Another limitation is the fact that the types and severity of USN were not taken in to consideration, and it is possible that different types of USN may require different treatment approaches. 53 Most of the included studies did not specify the type and location of the brain lesion. Because a few previous studies showed that right versus left USN differ in some characteristics, it is possible that the association with UE impairments might vary as well. Because the focus was on USN, findings cannot generalize to other common cognitive impairments, such as anosognosia for hemiplegia, apraxia, or aphasia, that can also appear in conjunction and affect the recovery of the affected UE poststroke.
In conclusion, USN is associated with poor UE motor capacity and less UE recovery poststroke. Therefore, these impairments should be considered when planning rehabilitation and discharge. Because USN is a well-researched phenomenon, the lack of studies and insufficient evidence related to UE interventions in individuals with USN was unexpected. Specific interventions for this population should be developed and researched to improve UE and overall functional outcome poststroke. Overall, more research in the field of USN in conjunction with other impairments is warranted.
Supplemental Material
Supplementary_Appendix – Supplemental material for Is Unilateral Spatial Neglect Associated With Motor Recovery of the Affected Upper Extremity Poststroke? A Systematic Review
Supplemental material, Supplementary_Appendix for Is Unilateral Spatial Neglect Associated With Motor Recovery of the Affected Upper Extremity Poststroke? A Systematic Review by Noa Doron and Debbie Rand in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.