
Abstract
Background. Robots that physically assist movement are increasingly used in rehabilitation therapy after stroke, yet some studies suggest robotic assistance discourages effort and reduces motor learning. Objective. To determine the therapeutic effects of high and low levels of robotic assistance during finger training. Methods. We designed a protocol that varied the amount of robotic assistance while controlling the number, amplitude, and exerted effort of training movements. Participants (n = 30) with a chronic stroke and moderate hemiparesis (average Box and Blocks Test 32 ± 18 and upper extremity Fugl-Meyer score 46 ± 12) actively moved their index and middle fingers to targets to play a musical game similar to GuitarHero 3 h/wk for 3 weeks. The participants were randomized to receive high assistance (causing 82% success at hitting targets) or low assistance (55% success). Participants performed ~8000 movements during 9 training sessions. Results. Both groups improved significantly at the 1-month follow-up on functional and impairment-based motor outcomes, on depression scores, and on self-efficacy of hand function, with no difference between groups in the primary endpoint (change in Box and Blocks). High assistance boosted motivation, as well as secondary motor outcomes (Fugl-Meyer and Lateral Pinch Strength)—particularly for individuals with more severe finger motor deficits. Individuals with impaired finger proprioception at baseline benefited less from the training. Conclusions. Robot-assisted training can promote key psychological outcomes known to modulate motor learning and retention. Furthermore, the therapeutic effectiveness of robotic assistance appears to derive at least in part from proprioceptive stimulation, consistent with a Hebbian plasticity model.
Introduction
Stroke remains a leading cause of disability despite 20 years of multidisciplinary efforts to develop technologies that enhance rehabilitation. Although robotic devices allow patients to practice movement without direct therapist supervision1-3 and enhance recovery,4,5 the mechanisms of benefits, beyond increasing the dose of movement repetitions, remain unclear.6-8 Understanding these mechanisms is essential for improving this approach.
Robotic therapy typically mimics one strategy used by rehabilitation therapists—active movement assistance,9-11 which seems justifiably based in motivational or neuroplasticity theories. Success is known to encourage motivation, self-efficacy, and willingness to practice.12-14 Active assistance increases success, and therefore presumably activates these positive learning features. Alternately, active assistance might promote Hebbian plasticity by increasing the amount of proprioceptive input in a way that is time-correlated with attempted motor activity. 15
Evidence supporting the motivational and Hebbian hypotheses is sparse.8,16 Motivation, measured with end-of-training surveys, is generally higher for robotic compared with conventional training (eg, Housman et al 1 ). However, this may be due the video gaming environment, 17 the quantitative feedback, or the novelty of robotics technology, rather than the active assistance. 18 Another confounding factor is that robotic assistance typically increases the number of movements that can be completed in a given amount of time. 2 Because most studies control therapy dose in terms of the duration, robotic therapy may be more effective because patients attempt more movements, although the mechanisms of dose-response effects in movement rehabilitation are still under study.19-22
The few studies that have matched the number of unassisted and robotic training movements are equivocal. An early pilot study used the ARM Guide to assist chronic stroke patients in reaching and found no differential benefit compared to a matched amount of unassisted reaching practice. 23 Another study used the HWARD hand robot to assist grasping and found that the group that received assistance on all training trials recovered more hand movement, compared to a group that received assistance on only half a matched number of trials. 24 A recent study of finger training found better long-term retention of functional gains with assistance compared with no assistance. 25 In the largest clinical trial of robotic therapy for the upper extremity, a novel therapist-supervised therapy was designed as a control, in an attempt to match the number of training movements to the robotic therapy. The 2 therapies produced comparable outcomes, which compared favorably with standard of care.2,21 This was particularly true for younger participants and participants with more recent strokes, although the effectiveness of intensive therapy diminished with time. 21
Related to these findings, robotically assisting in movement sometimes causes the trainee to reduce their effort or “slack.” 26 Energy expenditure in the early version of the Lokomat gait robot was lower than during manually assisted stepping among subjects with spinal cord injury, suggesting participants “rode along” with the robot. 27 Slacking has also been observed for the upper extremity during robotic training, 26 and appears to be a neural adaptation mechanism that aids in effort minimization. 28 Reduced patient effort during robotic therapy has been shown to reduce benefit.29,30
In the present study, we sought to determine the therapeutic effects of high and low levels of robotic assistance during finger movement training. By carefully designing the movement task and robotic assistance, we ensured that participants in both groups attempted a comparable number of practice movements while playing the same video game with the same robot. Additional assurance that efforts would be comparable across groups comes from a pilot study in which we found that this task, game, and form of assistance caused participants to exert similar physical effort regardless of the assistance level (ie, this system caused minimal slacking). 31 Furthermore, we quantified motivation and self-efficacy at multiple time points throughout training to better assess the psychological effects of assistance. Finally, we quantified finger proprioception at multiple time points using a novel robotic measure, 32 hypothesizing that any benefit from Hebbian-like plasticity mechanisms would require intact proprioception.
Methods
Study Design and Participants
We used the FINGER robotic exoskeleton31,33 (Figure 1) to provide 2 levels of assistance to participants with stroke-related finger movement impairments while they played a musical computer game in the style of Guitar Hero. We randomized participants into high and low assistance groups and then dynamically adjusted the amount of robotic assistance each week to drive participants toward 85% and 50% success rates, respectively. Initially, we intended to run a third group in which participants would have undergone the same treatment as the other 2 but without any robot assistance. However, we chose to omit this group after realizing during our pilot testing 31 that participants in the unassisted group would not be able to match the dose of practice of the participants in the other 2 groups. Removing this group also allowed us to increase the number of participants in the other 2 groups to 15 each. The 30 participants who completed the study (Figure 1A) met the following criteria: (1) history of unilateral stroke at least 6 months prior, (2) age between 18 and 80 years, and (3) able to score at least 3 blocks on the Box and Blocks Test 34 (BBT). Sample size was determined by power analyses 35 (see Supplemental Material). All trials were performed at University of California Irvine, and all participants provided informed consent according to a protocol approved by the local institutional review board. The study was listed on ClinicalTrials.gov (NCT02048826). The trial ceased after all 30 participants completed the program.
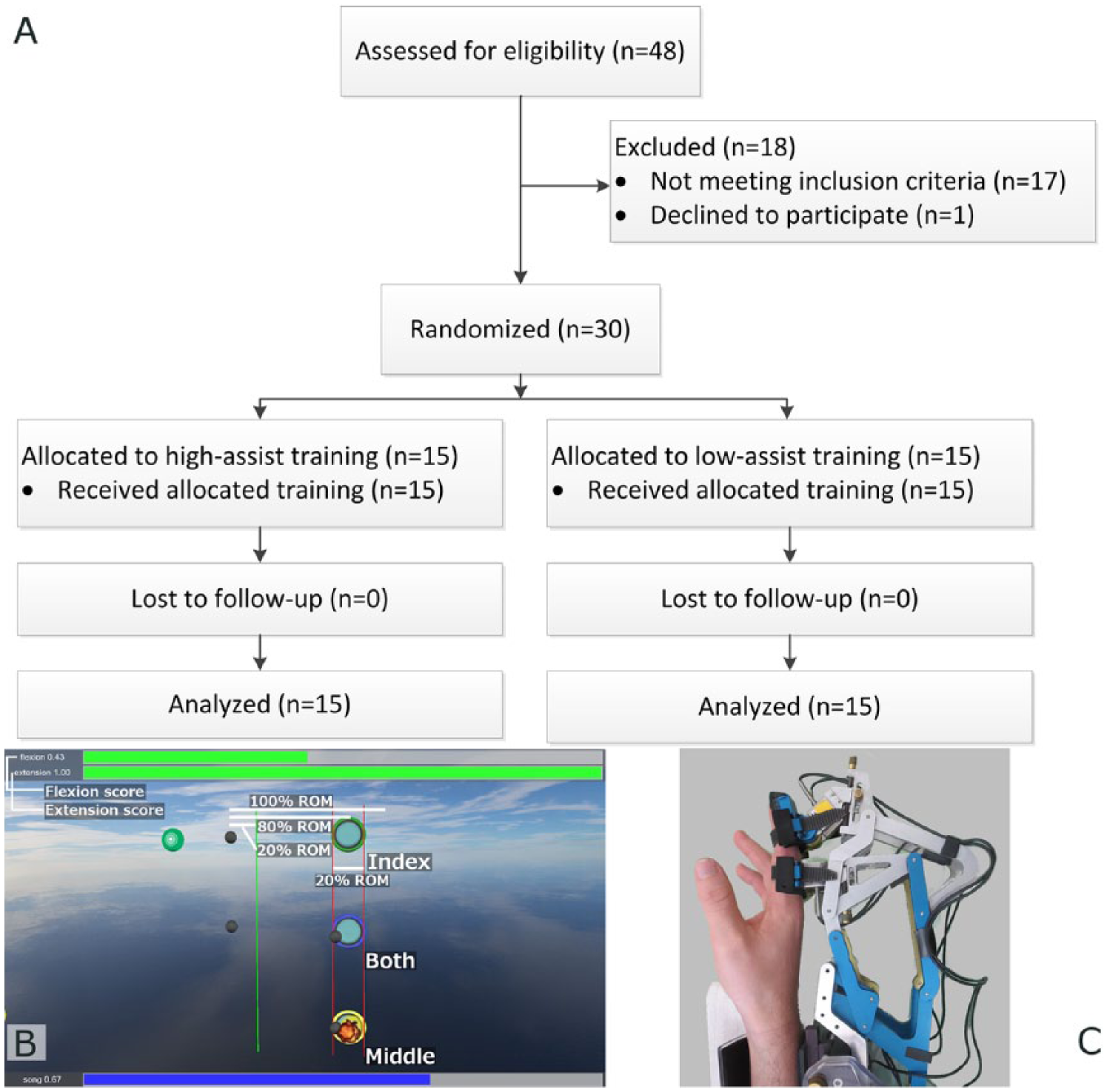
Experiment overview. (A) CONSORT (Consolidated Standards of Reporting Trials) flow diagram. (B) Annotated screenshot of the computer game used for this experiment. As popular music played, colored circles denoting “notes” flowed from left to right at the top (green), middle (blue), or bottom (yellow) of the screen toward like-colored targets. Targets were placed at 80% of full flexion. Smaller grey circles showed the position of the index and middle fingers. Participants had to start behind the green line and flex the correct finger(s) so as to stop inside of the targets just as the notes reached them. A score for each finger was displayed at the top of the screen, based on percentage of notes hit, calculated as moving average. Screenshot is for training the left hand; the screen and note directions were flipped when training the right hand (C) The FINGER robot used to provide participants with assistance as they played the computer game. Mechanisms attached to the index and middle fingers assisted in a naturalistic finger curling motion.
We randomized participants into the high- and low-assist groups using a block allocation procedure with blocks defined by age and BBT score (see Supplemental Material). Participants were enrolled and assigned to groups by the same physical therapist. A second, blinded, experienced evaluator (a licensed occupational therapist) assessed participants using a set of clinical outcome measures, with the primary outcome being the change in BBT from baseline to 1 month posttherapy (see Supplemental Material for a complete description of outcome measures). Since interventions differed only in the level of assistance provided by the robot, it was not difficult to preserve the blindness of the evaluator or participants, resulting in a double-blind design. To ensure that the participants were at a stable baseline at the time of enrollment, participants returned one week after their preliminary evaluation to repeat the BBT. Two weeks after their first baseline evaluation participants began movement training in the FINGER robot for three 1-hour sessions per week for 3 weeks. Finally, the participants repeated the initial set of outcome measure twice: once at the end of therapy (EOT), and then again at the 1-month follow-up (1 Mo FU).
The robotic training procedure is described in detail in the Supplemental Material. Briefly, during each training session, participants played 5 songs (see Supplemental Table S1) 2 times each, for a total of 1065 possible movements per session. Participants were instructed to try to hit note objects by moving either the index and/or middle finger(s) (as specified by note color) so as to stop inside of a target just as the scrolling musical note passed through it (Figure 1). As participants played the game, the FINGER robot provided assistive forces that guided the fingers along a physiological spatiotemporal trajectory that intercepted the musical note at the target. However, the robot only provided these forces if the participants initiated the movements themselves as determined using force sensors mounted between the fingers and robot mechanisms (threshold = 6 N). Assistive forces guiding participants toward their desired trajectories were applied using a compliant position controller, the gains of which were adapted on a weekly basis to maintain success rates at the target level. 31 Once per week the participants also played one song without assistance to quantify their ability to move their fingers without assistance.
We measured finger proprioception at baseline using a novel procedure that we recently found to be sensitive to changes in proprioception with aging. 32 FINGER slowly moved the index and middle fingers past each other while blocking any visual feedback, participants indicated the moment of crossing, and the angular distance to the actual crossing event was defined as the error (see Supplemental Material for more details).
Data Analysis
We tested the significance of time, group (high assistance vs low assistance), and the time × group interaction on all the outcomes using linear mixed-effect (LME) models. The model allowed random intercepts for each participant to account for the fact that the participants spanned a wide range of impairment levels. We did not correct for multiple comparisons across outcome measures. The Supplemental Material provides more model details, as well as the methods we used to analyze motivation and self-efficacy scores.
Results
There were no significant differences between the high- and low-assistance groups at baseline (Table 1). The BBT score showed no significant change between the 2 baseline evaluations (t test, P = .89), confirming a stable baseline. The average number of movements attempted by the high and low assistance groups over the 3 weeks of study therapy was not significantly different (7994 ± 1101 vs 7930 ± 723, t test, P = .86, Figure 2A). The average success rates for the high- and low-assistance groups were 81.6% ± 7.2% and 55.1% ± 6.9% (t test, P < .001, see Figure 2B), as planned. On the once a week song without robotic assistance, success rates were about 20% for both groups (Figure 2C).
Demographic Data and Key Baseline Clinical Outcomes.
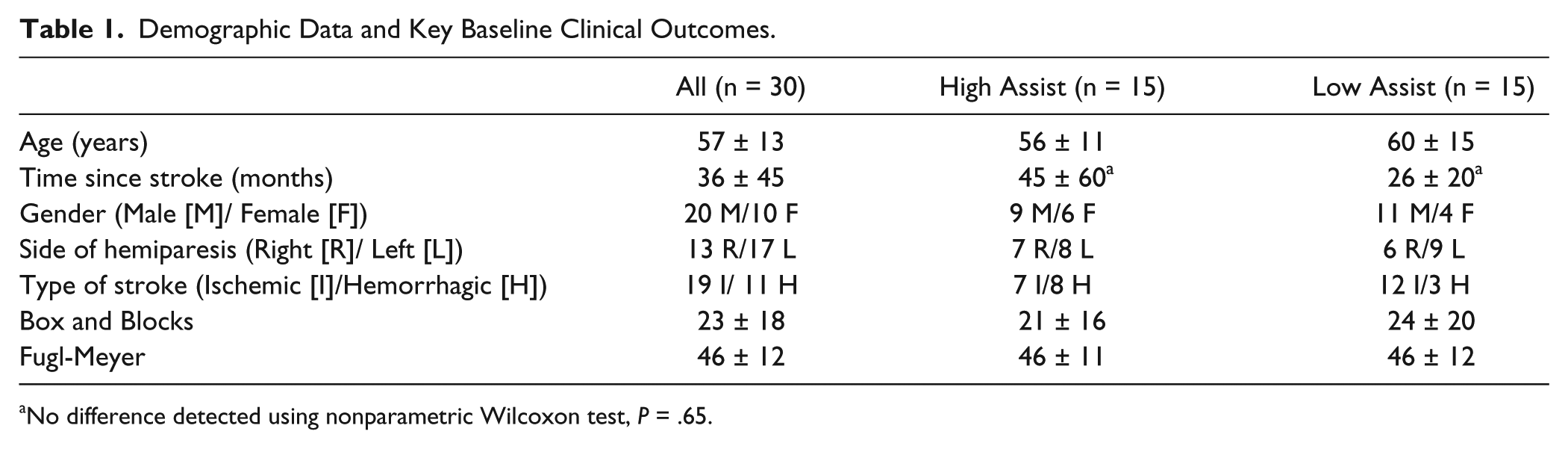
No difference detected using nonparametric Wilcoxon test, P = .65.
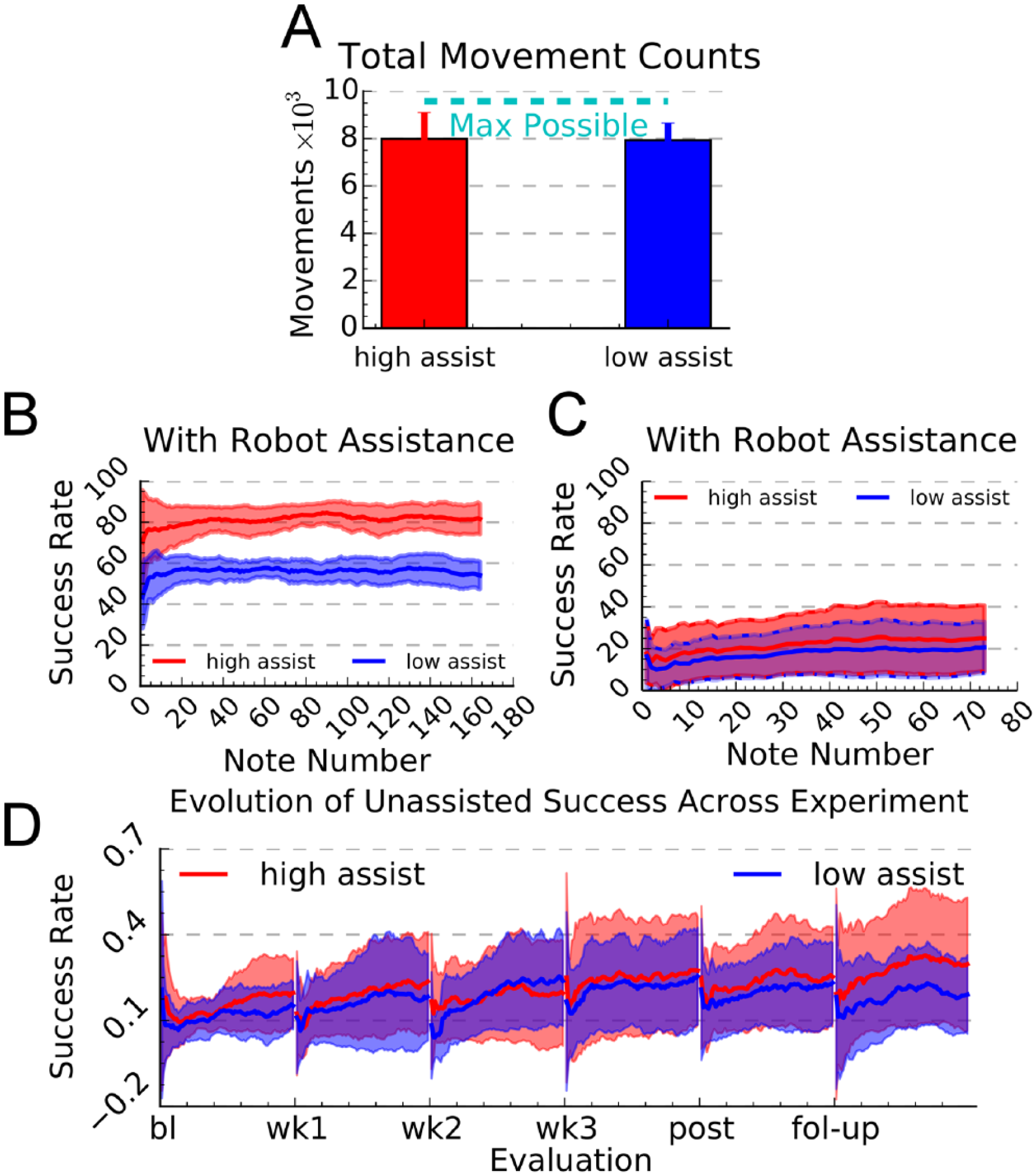
Quantified aspects of the robot-assisted training. (A) Mean number of practice movements across 3 weeks of training for participants in the high- and low-assistance groups. The dashed line shows the number of possible practice movements, calculated as the number of notes that the computer game presented to the participants. (B) Mean success rate in hitting notes for a song presented in the first training session with the robot adaptively assisting movement. The algorithm quickly adapted the amount of assistance during the song to achieve the target levels of success for the high- and low-assistance groups. (C) Mean success rates for a different song, part of the once per week assessment during which the robot did not assist in movement. In each panel, error bars and shaded regions denote ±1 SD. (D) Evolution of unassisted success rate across 6 evaluation sessions (baseline, week 1, week 2, week 3, end of therapy [EOT], and 1-month follow-up (1 Mo FU), demonstrating motor learning of the computer game task. Participants played one song without assistance during evaluations. Participants improved performance of the song as they played it, then retained some of that improvement the next training session, associated with a net improvement in performance. Shaded regions show ±1 SD.
Changes in Movement Ability
The primary outcome measure (BBT) and all the other outcome measures (except for the Nine Hole Peg Test and the National Institutes of Health [NIH] Stroke Scale) improved significantly over time (Table 2, Figure 3A and B). There was no effect of group for any outcome measure. However, group effects became significant when examined as a function of time for the Fugl-Meyer test, LME F(1/58) = 3.95, P = .05, and the Lateral Pinch Strength Test, LME F(1/58) = 6.11, P = .0164.
Change in Clinical Outcome Measures. a
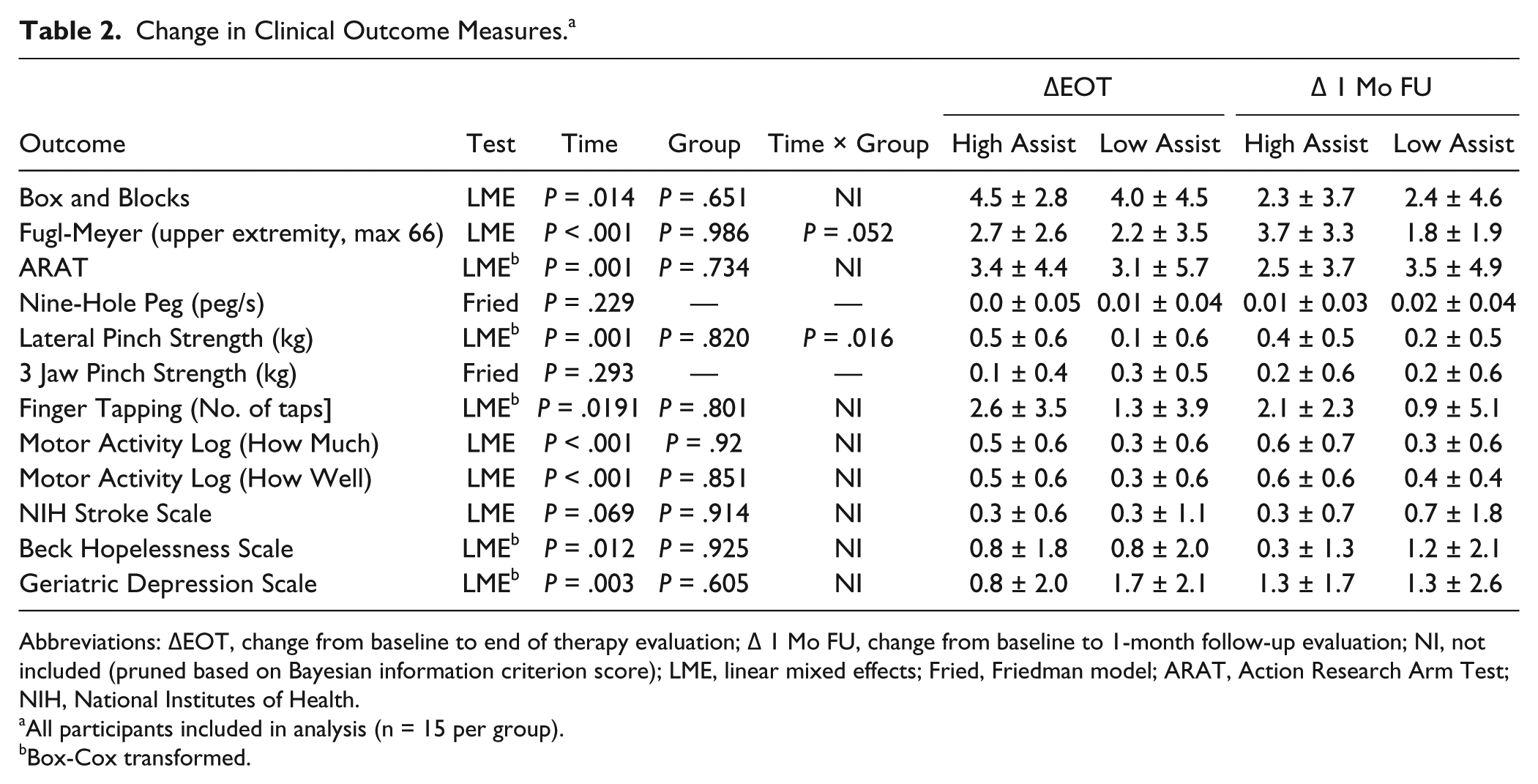
Abbreviations: ΔEOT, change from baseline to end of therapy evaluation; Δ 1 Mo FU, change from baseline to 1-month follow-up evaluation; NI, not included (pruned based on Bayesian information criterion score); LME, linear mixed effects; Fried, Friedman model; ARAT, Action Research Arm Test; NIH, National Institutes of Health.
All participants included in analysis (n = 15 per group).
Box-Cox transformed.
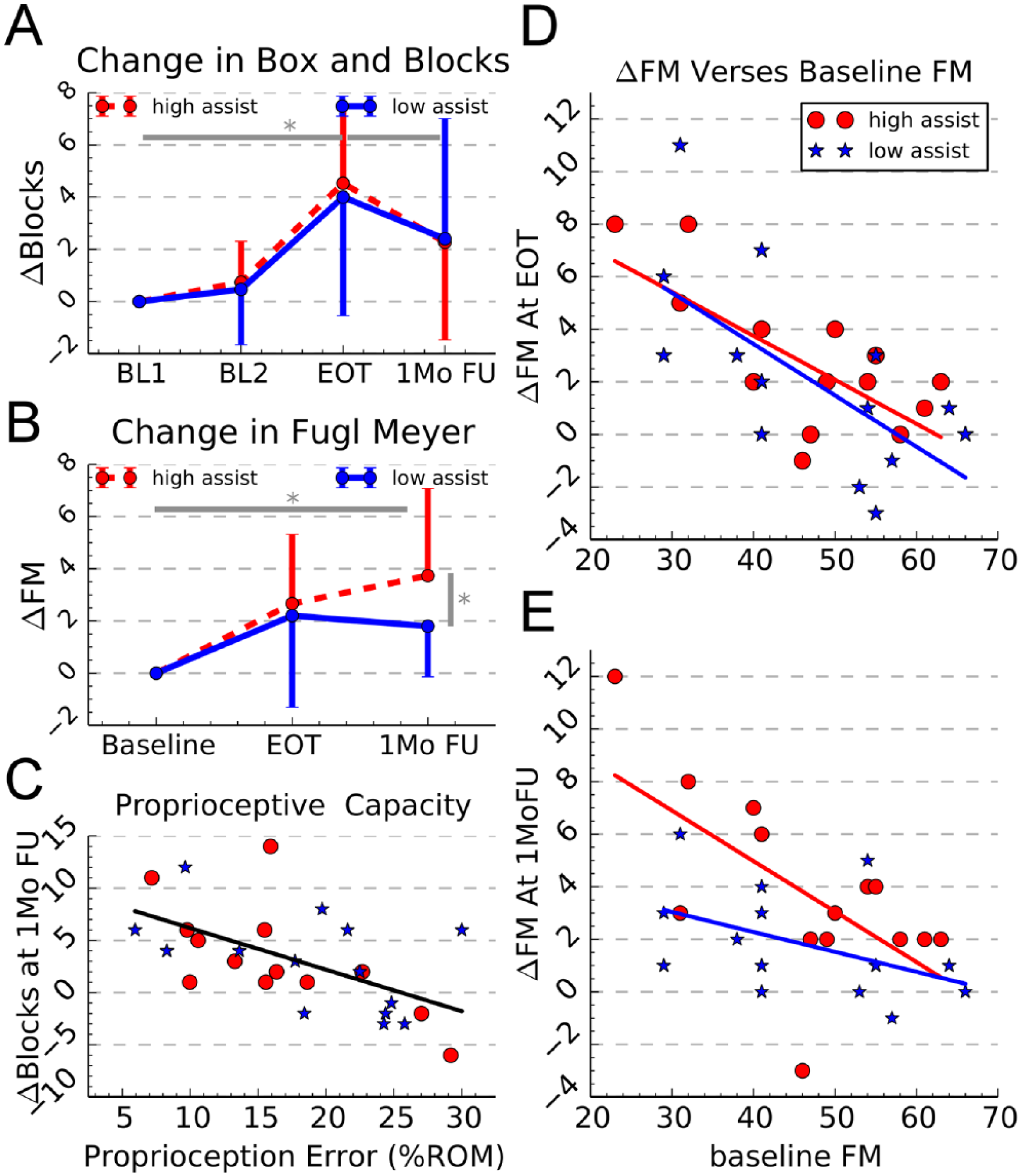
Clinical outcomes and covariates. (A) Change in Box and Blocks score measured from baseline to end of therapy evaluation and to the 1-month follow-up evaluation. *Denotes significant difference, P < .05. (B) Change in the upper extremity Fugl-Meyer score. Error bars in A and B show ±1 SD. (C) Change in Box and Blocks score at the 1-month follow-up as function of proprioception error measured at baseline. (D) Change in Fugl-Meyer score, measured from baseline to the end of therapy, versus baseline Fugl-Meyer score. (E) Change in Fugl-Meyer score, measured from baseline to the 1-month follow-up, versus baseline Fugl-Meyer score.
The participants’ ability to hit notes without robotic assistance, measured during the same song each week, improved over time (t test, P < .001), with a nonsignificant trend toward more improvement for the high-assistance group (Figure 2D, P = .23).
Changes in Psychological Outcomes
Motivation was significantly higher for participants in the high-assistance group (Figure 4A) LME group effect, F(1/218) = 56.26, P < .001. Motivation also increased significantly over time irrespective of group (Figure 4A) LME F(1/218) = 4.93, P = .027. Of the individual subscales of the Intrinsic Motivation Inventory (IMI), only the effort subscale showed a significant difference between groups (Figure 4B, see also Supplemental Table 3). Participants in the high-assistance group felt that they were exerting more effort despite the fact that they received more robotic assistance. The value, interest, and effort subscales all increased significantly over the course of the experiment (Supplemental Table 3). Perceived competence was the only IMI subscale with which baseline BBT score was significantly related, with participants with lower BBT scores expressing lower perceived competence, LME F(1/23) = 4.63, P = .04.
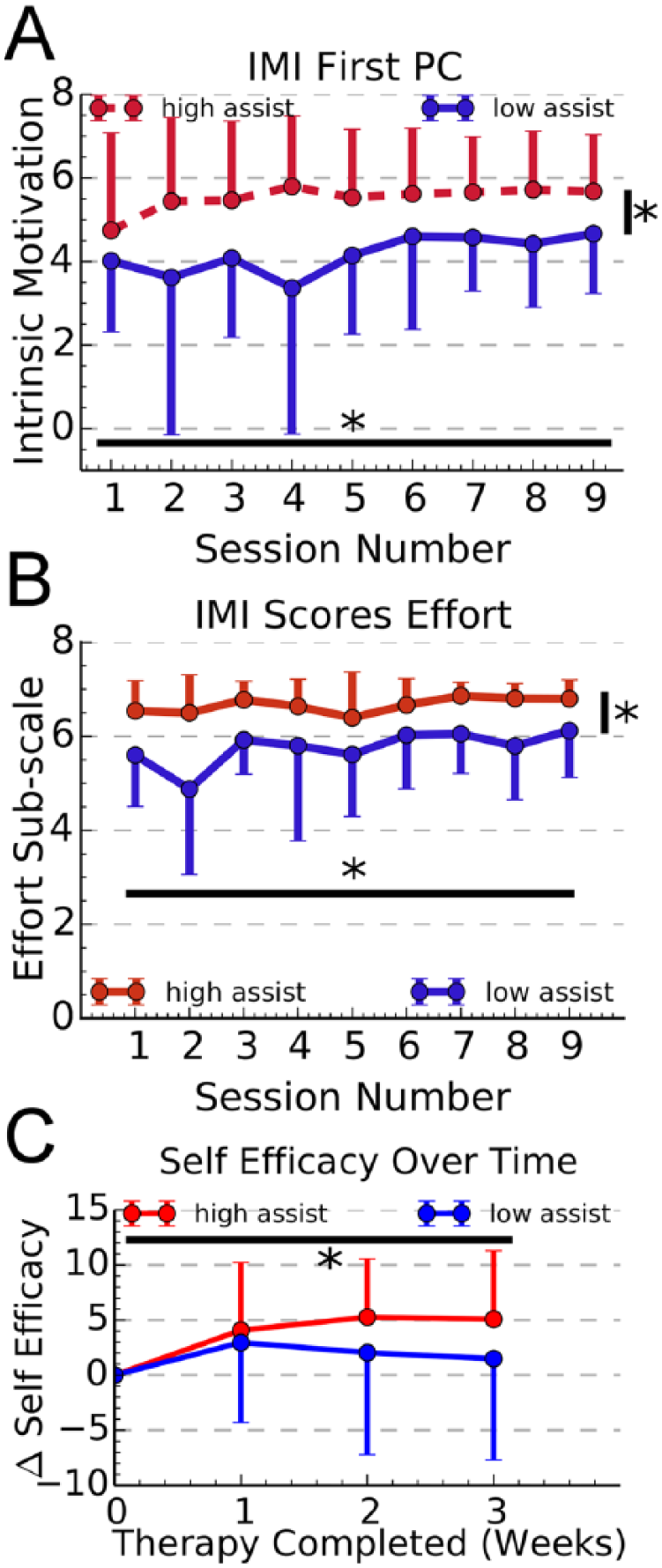
Motivation and self-efficacy across training. (A) The weighting of the first principal component of the Intrinsic Motivation Inventory (IMI), across the 9 training sessions. Individuals in the high-assist group reported significantly higher motivation (P < .001) (B) The effort subscale of the IMI across the nine training sessions; the high-assist group reported significantly higher effort (P < .002). (C) Change in self-efficacy across the 3 weeks of training. Self-efficacy was quantified by asking participants to estimate the probability of various scores in the Box and Blocks tests. The value on the y-axis is the number of additional blocks the participants estimated they could lift and place, with 50% confidence. Self-efficacy improved across training (P < .04), but the improvement was not different between groups. Error bars show ±1 SD.
At the end of each week of training we measured the participant’s self-efficacy with regard to the BBT to be administered that week. The number of blocks the participants estimated they could move increased significantly with respect to time, LME F(1/73) = 6.3, P = .014, but there was not a significant time × group interaction, LME F(1/73) = 0.302, P = .58.
The scores on the Beck Hopelessness Scale and the Geriatric Depression Scale improved significantly at both the EOT and 1 Mo FU (Table 2). There was not a significant difference between groups or a time × group interaction for these scales.
On average, participants in both groups reported achieving 3 new tasks and performing 3 existing day-to-day tasks better by the end of training. They also rated the training highly. See Supplemental Material for more details on subjective outcome results.
Predictive Value of Baseline Motor Impairment and Proprioception
Baseline Fugl-Meyer score was a significant predictor of the change in Fugl-Meyer, with individuals with lower baseline scores benefitting more from the training (linear regression P < .001 posttherapy and P = .002 at follow-up). At the EOT assessment neither the intercept nor the slope of the line relating baseline FM to delta FM were significantly different between groups (Figure 3D). However, at the 1-month follow-up assessment, the intercept of the high-assistance group was significantly higher (Figure 3E), LME F(1/26) = 5.17, P = .03, and the difference in slopes trended toward significance, LME F(1/26) = 2.39, P = .13. Thus, more severely impaired participants benefitted more from the higher assistance level. This finding held when we removed the individuals with the highest baseline FM scores, to check for a possible ceiling effect (see Supplemental Material).
Baseline finger proprioceptive ability predicted the change in BBT score at the 1-month follow-up, with better proprioceptive ability predicting a larger increase in BBT score at the follow-up (Figure 3C, P = .002, R2 = 0.335). It did not predict any of the other clinical outcomes. Participants with the most impaired finger proprioception at baseline tended not to improve their BBT score (Figure 3C).
Finger proprioception did not vary significantly over the course of the experiment, LME F(1/54) = 0.42, P = .52. Proprioceptive error at the baseline evaluation was strongly correlated with proprioceptive error at EOT (linear regression, R2 = 0.63, P < .001) and moderately correlated at the follow-up (R2 = 0.41, P < .001). Proprioception at baseline did not influence improvement in the high-assistance group more than in the low-assistance group (see Supplemental Material).
Discussion
The goal of this study was to determine the dose-matched effects of high and low levels of robotic assistance on finger movement recovery after chronic stroke; motivation was a secondary input. Both groups improved on clinical and robotic measures of movement, as well as psychological assessments of motivation, self-efficacy, and depression. The high-assist group improved more than the low-assist group on the Fugl-Meyer test and the lateral pinch strength test. The high-assist group also reported significantly greater motivation and effort throughout training. Participants with more severe motor impairment and better finger proprioception benefited more from the robotic training, regardless of assistance level. We first highlight several unique ways we controlled the robotic training in this study, then discuss implications for hand recovery mechanisms after stroke.
Unique Features of the Robotic Approach in This Study
Understanding the effects of robotic assistance on motor recovery has been challenging because robotic assistance usually helps participants make more movements, increasing the dose of movement training, which may in some cases improve recovery. Here, both groups made an almost identical total number of movements (~8000).
Some studies have suggested robotic assistance discourages effort and reduces motor learning. Here, we provided a form of assistance and a video game that caused minimal amounts of slacking. 31 Participants had to create an initiatory force to receive assistance, and the compliant assistance allowed errors (eg, the high-assistance group missed 1/6 notes). The video game was modeled after one of the most engaging and popular video games in history. Given these features, the positive benefits of greater robotic assistance found in this study need not contradict studies that have demonstrated that effort and errors benefit recovery.7,29,36,37 It is possible to design robotic training environments that promote effort and allow errors while still assisting trainees (refer Hogan et al 7 ).
Another unique feature of this study is the degree to which we quantified psychological aspects of the training. We measured motivation at each training session, instead of just following completion of training, finding that it was consistently higher for participants receiving high assistance. We also quantified self-efficacy for the first time to our knowledge in a robot-assisted therapy study, finding that it increased across training. Clinical scores of depression also improved. Taken together, these findings indicate that robot-assisted training can promote key psychological outcomes known to modulate motor learning and retention.
Most previous studies of robotic movement training have focused on arm movement or gait. We studied individuated finger movement because the fingers have a large cortical representation, in part due to a high density of tactile and proprioceptive sensors. 38 If Hebbian plasticity plays a role in robotic movement training, we speculated its role would be in evidence for finger training. As a consequence of this focus, compensation, such as by leaning with the trunk for arm movement, was impossible during the training. We can state unequivocally that significant motor learning occurred for the effector trained, as evidenced by improved success rates for the song during which robot assistance was not provided.
In summary, when interpreting the present study’s results, the term robot-assisted training should be understood to refer to training that requires participant effort, prevents slacking, allows error and variability, is highly motivating, produces quantifiable psychological and motor learning benefits, and is applied to highly sensate, individuated finger movement.
Does Robot-Assisted Training Facilitate Hebbian Plasticity?
A long-standing if somewhat implicit and not-well studied premise of robot-assisted therapy is that it might facilitate Hebbian plasticity by enhancing proprioceptive input. Previously we found that playing a similar musical game isometrically was less effective than when finger movement as allowed 35 . Here we found in carefully controlled conditions that high assistance robotic training was modestly more effective at reducing upper extremity impairment on a secondary endpoint, the Fugl-Meyer score. High assistance allowed participants to better complete the requested movements, and thus this result supports the Hebbian premise.
In addition, we hypothesized that any benefit from Hebbian learning stimulated by robotic assistance would require intact proprioception. Consistent with this hypothesis, the integrity of finger proprioception at baseline, assessed robotically, predicted the ability of the participants to benefit from the training, assessed with the BBT. In further support, the same set of participants underwent fMRI at study start, wearing a plastic exoskeleton similar to FINGER and playing a similar musical computer game with the fingers. Hemispheric asymmetry of activation in somatosensory cortex also predicted change in BBT score, again suggesting a need for normative proprioceptive processing to benefit from robotic training. 39 These findings are some of the first well-controlled data to support the Hebbian hypothesis for robot-assisted training, the other being from the study of the HWARD hand robot, in which the group that received assistance on all training trials (vs half) recovered more ability to move the hand. 24
Nevertheless, we are still cautious in concluding that Hebbian-like processes dominate robot-assisted training effects. First, the measured benefits of the higher level of assistance were small, only about 2 Fugl-Meyer points, and did not transfer to other measures, including the primary endpoint BBT score. In addition, although proprioception impairment correlated with the primary endpoint, it did not correlate with the other outcome measures. Furthermore, participants in the high-assistance group judged the robotic training as significantly more motivating, which may have played a role, as discussed next.
The Role of Motivation in Robot-Assisted Training
Motivation is widely considered to be an important facilitator of motor recovery.40-42 Motivation modulates motor learning, and, in particular, long-term motor retention, in part through dopaminergic systems.14,43 Here, we demonstrated that increasing the level of robotic assistance increased motivation, even after we controlled for the motivational value of the game (since both groups played the same game).
Indeed, without assistance, practicing with impaired limbs can seem futile, 18 and over time this sense of futility might contribute to cessation of use of the limb. 44 In the current study, game success rates were only 20% without assistance, a discouragingly low value. The success enabled by the robot might have reduced sense of futility and encouraged spontaneous use of the impaired limb outside of the laboratory, consistent with a trend in the Motor Activity Log being higher for the high-assistance group. We note also that the differential increase in the Fugl-Meyer score for the high-assistance group was seen mainly in the period following cessation of formal training, at the one-month follow-up, suggesting this group may have continued spontaneous self-training of their limbs. Other studies of robot-assisted therapy report enhanced carry-over during the follow-up phase for the robot-trained group,1,2,25 a phenomenon also demonstrated for rewarded motor training and attributed to dopaminergic function. 14
We conclude robot assistance can enhance motivation, which, in turn, may promote spontaneous use of the impaired limb and/or improve motor retention, important topics for future research. However, motivation does not appear to completely explain the enhancing effect of assistance, as it does not account for the role of preserved proprioceptive function, an observation strongly predicted by the Hebbian hypothesis.
Why Was Robot Assistance Better for More Impaired Participants?
A final interesting finding was that high-assistance training was more effective for participants with more severe motor impairments. This finding is mirrored by studies from our laboratory of motor skill learning by unimpaired participants in which training with robotic assistance provided a greater benefit to initially less skilled participants.45-47 One possible explanation relates to what is known as the Challenge Point Hypothesis,48,49 which proposes that participants will benefit most from practice at difficulty levels that allow them to extract actionable information. Practice with lower levels of assistance may have led to more opaque and unusable failures. Another possibility is that motivational effects discussed above were stronger for participants who were initially more impaired. A third possibility is that the more severely impaired individuals did not use their impaired limbs in daily life at study onset,44,50,51 thus having more of a reserve for motor learning, even with greater neural damage.
Limitations
One limitation of this study is that the population included a relatively high percentage of hemorrhagic stroke survivors, which could be a confounding factor. Another caveat for interpreting the within-group changes in outcomes is that the two measurements used to establish a stable baseline were only one week apart. Also, as mentioned above, the benefits of the higher level of assistance for impairment reduction were small and only evident in secondary endpoints, that is, Fugl-Meyer and Lateral Pinch Grip scores. The protocol was not designed to maximize transference of these benefits to hand function, such as by combining robotic and task-specific training. 52 We analyzed motivation, but separating motivation from attention is difficult, and either the low or high success groups could have exhibited reduced attention (because of the higher level of robotic help, or the increased failure rate, respectively), which could have affected the results. Future studies should parse out the effects of attention.
Implications
Counter to expectations from some robot-assisted therapy literature, we found that the higher level of robotic assistance was beneficial, particularly for people with more severe hand impairment and intact proprioception. The finding that higher rates of success are desirable is consistent with the 70% to 90% target scoring range selected for adaptive assistance by a widely used arm training robot “to avoid discouraging patients who could not yet move well without boring patients who could”7,10; similar findings for the hand and arm may suggest generalizable principles. Enforcing higher rates of success than those studied here, or providing forms of assistance that do not require engagement, still may encourage passivity and slacking, limiting benefits.26,29,30,53
The result that a relatively high level of assistance is beneficial stands in contrast to a recent study that found that augmenting errors had a more positive therapeutic effect after stroke than free movement. 54 It is likely the case that different forms of robotic training simultaneously activate different networks of motor learning processes, including error-based, use-dependent, and reinforcement learning networks, which rely on Hebbian-like and other plasticity mechanisms, and can be modulated by dose, effort, and motivation. We postulate that these networks sometimes respond in opposing ways, with their individual response strengths dependent on the specific features of the robotic training paradigm being applied and the neural resources available to support them. An important goal for helping individuals with a stroke is then to determine how to best select at baseline the type of training that will optimally blend the network responses to create a net positive therapeutic response. This study suggests that individuals with more severe levels of hand impairment (but still some hand function—ie, a BBT score of at least 3), and intact finger proprioception, benefit most from high levels of robotic assistance (as much as an 8-block gain in BBT and 8-point gain in Fugl-Meyer—see Figure 3). On the other hand, people with severely impaired finger proprioception at baseline may be better served by trying to retrain proprioceptive function before robot-assisted training, a relatively unexplored area, or by protocols that boost proprioceptive activity before training, as suggested by some prior work. 55
Footnotes
Acknowledgements
We would like to thank Skylar Hanson and Ariel Ortiz for their assistance through the trial.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Reinkensmeyer has a patent Method and apparatus for automating arm and grasping movement training for rehabilitation of patients with motor impairment, with royalties paid to U.C. Irvine. Dr. Cramer reports personal fees from Dart Neuroscience, GlaxoSmithKline, MicroTransponder, Roche, RAND Corp, outside the submitted work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by NIH-R01HD062744 from the National Center for Medical Rehabilitation Research at the National Institute of Child Health and Human Development, and the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1 TR000153. Dr Cramer is supported by K24–HD074722.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.