
Abstract
Background. Antipsychotic drugs (APDs) are used to manage traumatic brain injury (TBI)–induced behavioral disturbances, such as agitation and aggression. However, APDs exhibiting D2 receptor antagonism impede cognitive recovery after experimental TBI. Hence, empirical evaluation of APDs with different mechanistic actions is warranted. Aripiprazole (ARIP) is a D2 and 5-hydroxytryptamine1A (5-HT1A) receptor agonist; pharmacotherapies with these properties enhance cognition after TBI. Objective. To test the hypothesis that ARIP would increase behavioral performance and decrease histopathology after TBI. Methods. Adult male rats were subjected to either a controlled cortical impact (CCI) or sham injury and then randomly assigned to ARIP (0.1 or 1.0 mg/kg) or VEH (1.0 mL/kg, saline vehicle) groups. Treatments began 24 hours after surgery and were administered once daily for 19 days. Motor (beam-balance/beam-walk) and cognitive (Morris water maze) performance was assessed on postoperative days 1 to 5 and 14 to 19, respectively, followed by quantification of hippocampal CA1,3 neuron survival and cortical lesion volume. Results. Beam-balance was significantly improved in the CCI + ARIP (1.0 mg/kg) group versus CCI + ARIP (0.1 mg/kg) and CCI + VEH (P < .05). Spatial learning and memory retention were significantly improved in the CCI + ARIP (0.1 mg/kg) group versus the CCI + ARIP (1.0 mg/kg) and CCI + VEH groups (P < .05). Both doses of ARIP reduced lesion size and CA3 cell loss versus VEH (P < .05). Importantly, neither dose of ARIP impeded functional recovery as previously reported with other APDs. Conclusion. These findings support the hypothesis and endorse ARIP as a safer APD for alleviating behavioral disturbances after TBI.
Keywords
Introduction
Traumatic brain injury (TBI) affects an estimated 1.5 to 2 million individuals in the United States each year, which results in 52 000 deaths and 120 000 cases of long-term neurological disabilities.1-5 In addition to the mortality and morbidity caused by TBI, the cost of medical and rehabilitative care combined with the loss of productivity due to the inability to return to the work force in a timely manner, or at all, imposes a significant financial burden, which is estimated to be approximately $76.5 billion per year. 5 Clearly, TBI is a significant public health care concern.
In addition to the debilitating motor and cognitive deficits,6-9 TBI also induces salient neuropsychiatric complications. 10 In the acute recovery phase after TBI, agitation (eg, nonpurposeful verbal and/or physical behavior) and aggression can interfere with receipt of care or with engagement in important rehabilitation activities.11-13 Furthermore, these neuropsychiatric complications can put the TBI survivors and others at risk of physical harm through either nonspecific agitation or overt aggression. These complications are not rare. Recent studies report that 24% to 96% of patients surviving TBI exhibit agitated behavior in the acute recovery phase14-17 whereas 11% of TBI survivors demonstrate aggressive behavior. 18 Agitation and aggression may occur in the context of a post-TBI manic or psychotic state. Overall, the impact of agitated behavior on the rehabilitation process is significant. 19
The goals of psychopharmacotherapy in the post-TBI phase are 2-fold: First, they are used to manage symptoms and behaviors that otherwise would prevent the TBI survivor from receiving appropriate postinjury care and engaging in important and necessary rehabilitation. Second, they are used to control aggression when it is felt that the risk of injury to self or others is significant. Research into appropriate pharmacological interventions for agitation and aggression in TBI is lacking. 10 Hence, given the absence of randomized clinical trials, pharmacological treatment options are typically “borrowed” from other diagnostic entities with similar symptomatic presentations and applied to TBI survivors without a full understanding of the specific risks and benefits unique to TBI. 20 Antipsychotic drugs (APDs) are frequently used in the context of attenuating agitation and aggression during the recovery phase.21-25
Despite the advantages of APDs after TBI, there are also significant drawbacks that may not be fully appreciated in the clinical setting because of the paucity of data. Specifically, the few studies to date investigating the effects of APDs after experimental TBI show that they impair recovery and in some instances exacerbate TBI-induced behavioral deficits. Feeney and colleagues 26 demonstrated that a single administration of haloperidol (HAL), a dopamine2 (D2) receptor antagonist, provided after TBI in adult rodents delayed motor recovery. Moreover, administration of HAL after the rats were deemed recovered, as indicated by normal traversal of a beam, led to a reinstatement of the deficits. 26 Similar findings were reported by Goldstein and Bullman 27 and Kline et al. 28 Moreover, a short-and-consistent exposure paradigm (ie, once daily administration for 19 days) of HAL and risperidone (RISP) impeded recovery as demonstrated by the APD-treated rats performing significantly worse than vehicle controls.29,30 A more recent study by Phelps et al 31 has elaborated further on the findings from the chronic administration studies29,30 by showing that the deleterious effects on cognition persist for up to 3 months. Deleterious effects of HAL on cognition after TBI were also reported by Wilson and colleagues. 32
Given that often a patients’ best chance of regaining function after TBI is by spontaneous recovery, it is critical that the use of APDs (eg, HAL and RISP) that inhibit this process is minimized and that alternative treatments are evaluated for potential efficacy. One likely candidate is the atypical antipsychotic aripiprazole (ARIP), which exerts partial agonist activity at D2 and 5-hydroxytryptamine1A (5-HT1A) receptors33-35 and has been shown to be effective in the treatment of cognitive deficits associated with schizophrenia. 36 Additionally, ARIP has been shown to selectively increase dopamine levels in the hippocampus and prefrontal cortex, 37 an effect that may improve learning as both of these structures are critically involved in cognitive function. Moreover, D2 receptor agonists such as methylphenidate and bromocriptine and 5-HT1A receptor agonists, such as 8-OH-DPAT, repinotan HCl, and buspirone have been shown to confer significant cognitive benefits in preclinical models of TBI.38-44 Because of its lack of D2 receptor antagonism and partial agonist activity at 5-HT1A and D2 receptors, the aim of the current study was to test the hypothesis that ARIP would not negatively affect recovery after TBI, but instead would enhance behavioral performance and decrease histopathology.
Materials and Methods
Animals
Forty adult male Sprague-Dawley rats (Harlan, Indianapolis, IN, USA) were housed in standard steel-wire mesh cages and maintained in a temperature (21°C ± 1°C) and light (12:12 hour light:dark cycle with lights on at 7:00
Surgery
Rats weighing 300 to 325 g on the day of surgery underwent surgical anesthesia, which was induced and maintained with inspired concentrations of 4% and 2% isoflurane, respectively, in a 2:1 ratio of N2O:O2. Following endotracheal intubation the rats were secured in a stereotaxic frame and ventilated mechanically. Core body temperature was maintained at 37°C ± 0.5°C with a heating blanket. Utilizing aseptic procedures, a midline scalp incision was made, the skin and fascia were reflected to expose the skull, and a craniectomy (6-mm in diameter) was made in the right hemisphere (encompassing bregma–lambda and between the sagittal suture–coronal ridge) with a handheld trephine. Subsequently, the impacting rod was extended and the impact tip (6 mm, flat) was centered and lowered until it touched the dura mater, then the rod was retracted and the impact tip was advanced 2.8 mm farther to produce a brain injury of moderate severity (2.8 mm tissue deformation at 4 m/s). Immediately after the controlled cortical impact (CCI), anesthesia was discontinued, the incision was closed, and then the rats were extubated and assessed for acute neurological outcome. Sham rats underwent similar surgical procedures, but were not subjected to the impact.
Acute Neurological Evaluation
Following termination of anesthesia, hind limb reflexive ability was assessed by gently squeezing the rats’ paw every 5 seconds and recording the time to elicit a withdrawal response. Return of the righting reflex was determined as the time required for a rat to turn from the supine to prone position. These natural reflexive responses are sensitive indicators of injury severity and anesthetic effects.7-9,38-41
Drug Administration
Following surgery, the rats were randomly assigned to the following 5 groups: CCI + ARIP (0.1 mg/kg; n = 10), CCI + ARIP (1.0 mg/kg; n = 10), CCI + vehicle (VEH; 1.0 mL/kg; n = 10), Sham + ARIP (1.0 mg/kg; n = 5) or Sham + VEH (1.0 mL/kg; n = 5). ARIP (Toronto Research Chemicals, Toronto, Ontario, Canada), was prepared daily by dissolving in 1:1 dimethyl sulfoxide:saline, which also served as the VEH. The doses of ARIP were chosen because they were reported to increase dopamine release in the hippocampus and prefrontal cortex. 37 Treatments began 24 hours after CCI or sham surgery and were provided intraperitoneally once daily (after the daily behavioral assessments to circumvent sedative effects that may confound the results) for 19 days.
Motor Performance: Beam-Balance and Beam-Walk
Motor function was evaluated using well-validated beam tasks.28-31 Briefly, the beam-balance task consisted of placing the rat on an elevated (90 cm) narrow (1.5 cm) wooden beam and recording the duration it remains on it for a maximum of 60 seconds. The beam-walk task, which is a modified version of that originally devised by Feeney and colleagues 9 consisted of recording the time to traverse an elevated (90 cm) narrow wooden beam (2.5 wide, 100 cm long) and enter a darkened goal box at the opposite end to escape bright light and high decibel white noise. All rats were trained to perform the tasks without errors prior to surgical manipulations. A baseline performance assessment was taken on the day of surgery. Testing consisted of providing three trials (60 seconds allotted time with a 30 seconds intertrial interval) per day on each task and took place on postoperative days 1 to 5. The average daily scores for each subject were used in the statistical analyses.
Cognitive Function: Acquisition of Spatial Learning (Time to Platform)
A Morris water maze (MWM) task that is sensitive to TBI-induced cognitive dysfunction and subsequent recovery6-9,38-41 was used to compare acquisition of spatial learning. The maze consisted of a plastic pool (180 cm diameter; 60 cm height) filled with water (26°C ± 1°C) to a depth of 28 cm and was situated in a room with salient and permanent visual cues. The platform was a clear Plexiglas stand (10 cm diameter, 26 cm high) that was positioned 26 cm from the maze wall in the southwest quadrant of the maze and held constant throughout the study. Acquisition of spatial learning began on postoperative day 14 and consisted of providing a block of 4 daily trials (120 seconds maximum, 4 minutes intertrial interval) for 5 consecutive days (days 14-18 postsurgery) to locate the platform when it was submerged 2 cm below the water surface (ie, invisible to the rat). For each daily block of trials, the rats were placed in the pool facing the wall at each of the 4 possible start locations (north, south, east, and west) in a randomized manner. Each trial lasted until the rat climbed onto the platform or until 120 seconds had elapsed, whichever occurred first. All rats were required to remain on the platform for 30 seconds before being placed in a heated incubator between trials (4-minute intertrial interval).
Cognitive Function: Memory Retention
Memory retention was assessed on postoperative day 19 (ie, 1 day after the final acquisition training session). During this test, the platform was removed from the pool and the rats were placed in the maze from the location point most distal to the quadrant where the platform was previously situated (ie, “target quadrant”) and allowed to freely explore the pool for 30 seconds. The percent time spent in the target quadrant was used in the statistical analysis. The behavior data were obtained using a spontaneous motor activity recording and tracking (SMART) system, which in addition to determining time to the platform, also calculated swim speed.
Histology: Quantification of Hippocampal Cell Survival
Following the last behavioral assessment (ie, postoperative day 19), the rats were anesthetized with pentobarbital (50 mg/kg intraperitoneal) and then perfused transcardially with 200 mL 0.1 M phosphate buffered saline (pH 7.4) followed by 300 mL 4% paraformaldehyde. The brains were extracted, postfixed in the perfusate for 1 week, dehydrated with alcohols, and embedded in paraffin. Coronal sections (7-µm thick) were cut at 1-mm intervals through the lesion on a microtome and mounted on microscope slides. After drying at room temperature, the sections were deparaffinized in xylenes, rehydrated, and stained with Cresyl violet. An observer blinded to experimental conditions analyzed tissue underlying the area of contusion (3.5 mm posterior to bregma) from rats in each group for determination of treatment efficacy on selectively vulnerable hippocampal CA1,3 neurons. To reduce counting errors associated with false positive identification of dying neurons, the total number of CA1,3 morphologically intact neurons were counted using a Nikon Eclipse E600 microscope with a 40× objective. The data are presented as the percent of total neurons in the ipsilateral (injured) CA1,3 regions relative to the contralateral (uninjured) hippocampus and provide an estimate of surviving neurons as previously reported.39,41,44,45
Histology: Quantification of Cortical Lesion Volume
Cortical lesion volumes (mm3) were assessed by an observer blinded to experimental conditions using a Nikon Eclipse 90i microscope. The area of the lesion (mm2) was first calculated by outlining the inferred area of missing cortical tissue for each section (typically 5-7) and then by summing the lesions obtained, as previously reported.39,41,44,45
Data Analyses
Statistical analyses were performed on data collected by observers blinded to treatment conditions using StatView 5.0.1 software. The motor and cognitive data were analyzed by repeated-measures analysis of variance (ANOVA). The acute neurological data, probe trials, swim speed, and histological findings were analyzed by one-factor ANOVAs. When the ANOVA revealed significant effects, the Newman-Keuls post hoc test was used to determine specific group differences. The results are expressed as the mean ± standard error of the mean (SEM) and are considered significant when P values are ≤.05.
Results
Two rats (1 from each the CCI + ARIP [0.1 mg/kg] and CCI + VEH groups) were excluded from the study because of an inability to locate the visible platform, which may be indicative of visual acuity deficits that could confound the spatial learning data. Hence, statistical analyses are based on 38 rats. No significant differences were observed among the sham groups, regardless of treatment in any of the assessments and thus the data were pooled and analyzed as 1 group (denoted as “SHAM”).
Acute Neurological Evaluation
No significant differences were observed among the TBI groups in time to recover the hind limb withdrawal reflex in response to a brief paw pinch (left range = 181.9 ± 4.2 to 189.7 ± 4.1 seconds, P > .05; right range = 177.9 ± 4.0 to 186.8 ± 4.0 seconds, P > .05) or for return of righting ability (range 310.0 ± 20.2 to 346.3 ± 16.9 seconds, P > .05) following the cessation of anesthesia. The absence of significant differences among the groups suggests an equivalent level of injury and anesthesia.
Motor Performance
Beam-Balance
Prior to surgery (baseline) all groups balanced on the beam for the full 60 seconds on each of 3 trials (Figure 1). After surgery, the overall ANOVA revealed significant Group (F3,34 = 5.607, P = .0031) and Day (F5,170 = 25.586, P < .0001) differences, as well as a significant Group × Day interaction (F15,170 = 3.907, P < .0001). The post hoc test showed that all CCI groups balanced significantly less than the SHAM group (P < .05). Moreover, the CCI + ARIP (1.0 mg/kg) group performed better than the CCI + VEH group (P < .05), but did not differ from the CCI + ARIP (0.1 mg/kg) group (P > .05).
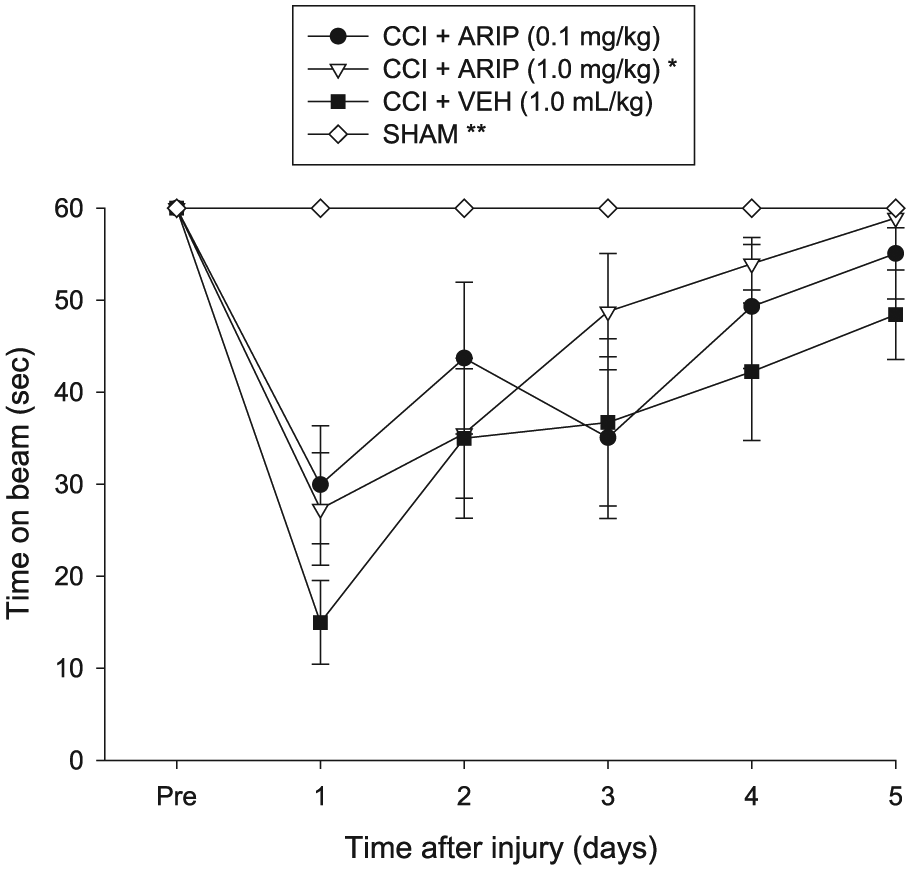
Mean (± SEM) time (seconds) maintaining balance on an elevated narrow beam before and after traumatic brain injury (TBI) or sham injury. There was no significant difference between the sham groups and thus they were pooled (SHAM). *P < .05 versus CCI + VEH. **P < .05 versus all CCI groups. There was no difference between the CCI + ARIP (0.1 mg/kg) and CCI + ARIP (1.0 mg/kg) groups (P > .05). ARIP, aripiprazole; CCI, controlled cortical impact; VEH, saline vehicle.
Beam-Walk
No differences were revealed among the groups in beam-walk ability prior to surgery as all rats traversed the beam in less than 4 seconds (Figure 2). Postsurgical repeated-measures ANOVA showed significant Group (F3,34 = 28.657, P < .0001) and Day (F5,170 = 93.474, P < .0001) differences, as well as a significant Group × Day interaction (F15,170 = 27.858, P < .0001). All CCI groups were impaired relative to the SHAM group (P < .0001), but did not differ from one another, regardless of treatment (Ps > .05).
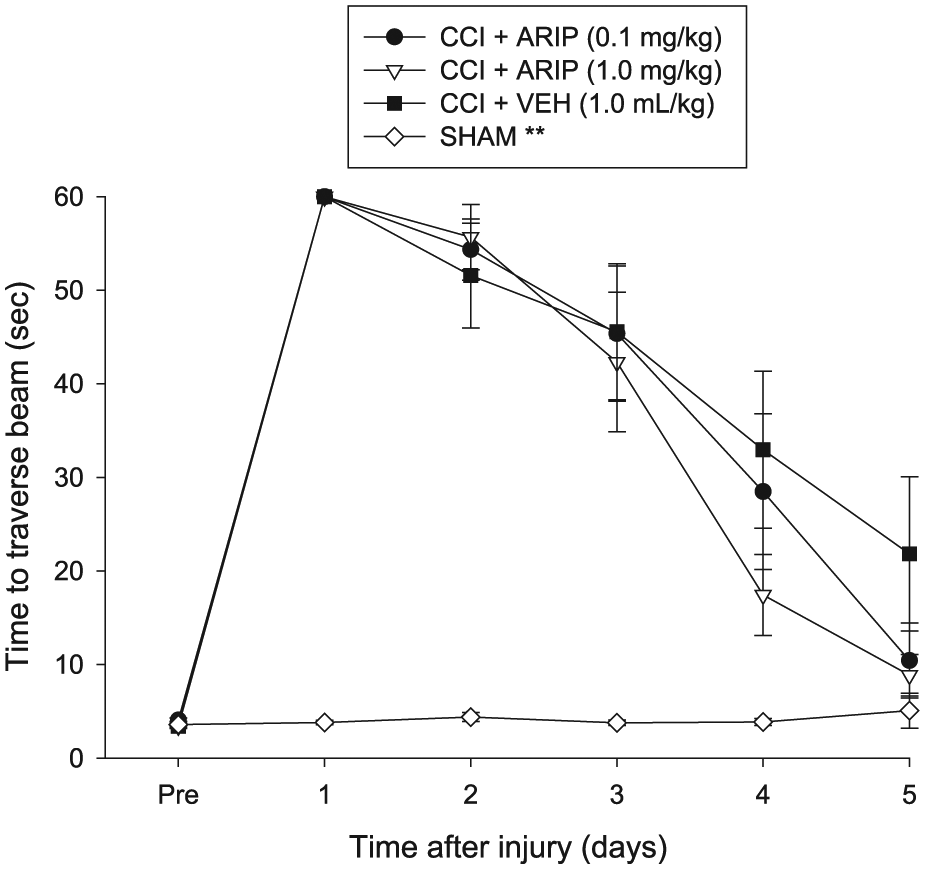
Mean (± SEM) time (seconds) to traverse an elevated narrow beam after traumatic brain injury (TBI) or sham injury. There was no significant difference between the sham groups and thus they were pooled (SHAM). No statistically significant differences were observed among the controlled cortical impact (CCI) groups, regardless of treatment. **P < .05 versus all CCI groups.
Cognitive Function: Acquisition of Spatial Learning (Time to Platform)
Repeated-measures ANOVA of the MWM data for postoperative days 14 to 18 revealed significant Group (F3,34 = 11.465, P < .0001) and Day (F4,136 = 11.297, P < .0001) differences, but no Group × Day interaction (F12,136 = 1.108, P = .358). The post hoc analysis revealed significant differences among the groups. First, as depicted in Figure 3, all CCI groups were significantly impaired versus SHAM controls (P < .05). Second, the CCI + ARIP (0.1 mg/kg) group was able to locate the escape platform quicker than the CCI + ARIP (1.0 mg/kg) and CCI + VEH groups (Ps < .05). Third, there was no difference between the CCI + ARIP (1.0 mg/kg) and CCI + VEH groups (P > .05).
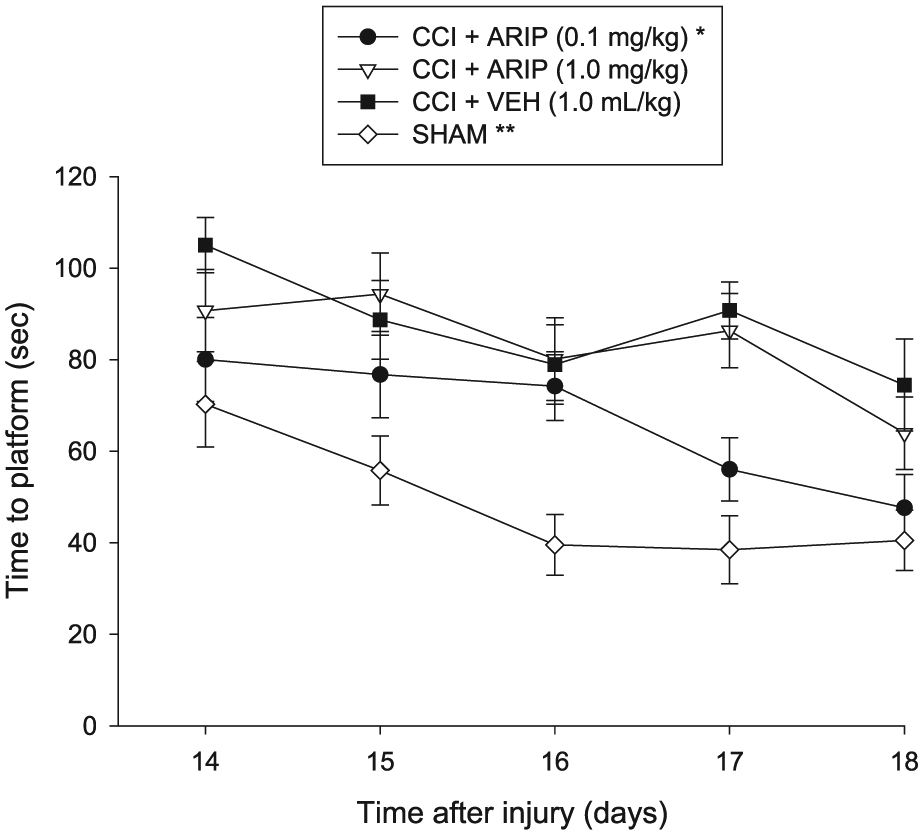
Mean (± SEM) time (seconds) to locate a hidden platform in the Morris water maze. There was no significant difference between the sham groups and thus they were pooled (SHAM). *P ≤ .0033 versus CCI + ARIP (1.0 mg/kg) and CCI + VEH. **P < .05 versus all CCI groups. No significant difference was revealed between the CCI + ARIP (1.0 mg/kg) and CCI + VEH groups (P > .05). ARIP, aripiprazole; CCI, controlled cortical impact; VEH, saline vehicle.
Cognitive Function: Acquisition of Spatial Learning (Distance to Platform)
Analysis of swim distance (i.e., pathlength) to locate the escape platform revealed significant Group (F3,34 = 14.570, P < .0001) and Day (F4,136 = 12.864, P < .0001) differences. All CCI groups were significantly impaired versus SHAM controls (P < .05). The distances required to locate the platform became increasingly shorter over time for the CCI + ARIP (0.1 mg/kg) group versus the CCI + VEH group (P < .05; Figure 4). The CCI + ARIP (1.0 mg/kg) group did not differ from the CCI + ARIP (0.1 mg/kg) or CCI + VEH groups (Ps > .05).
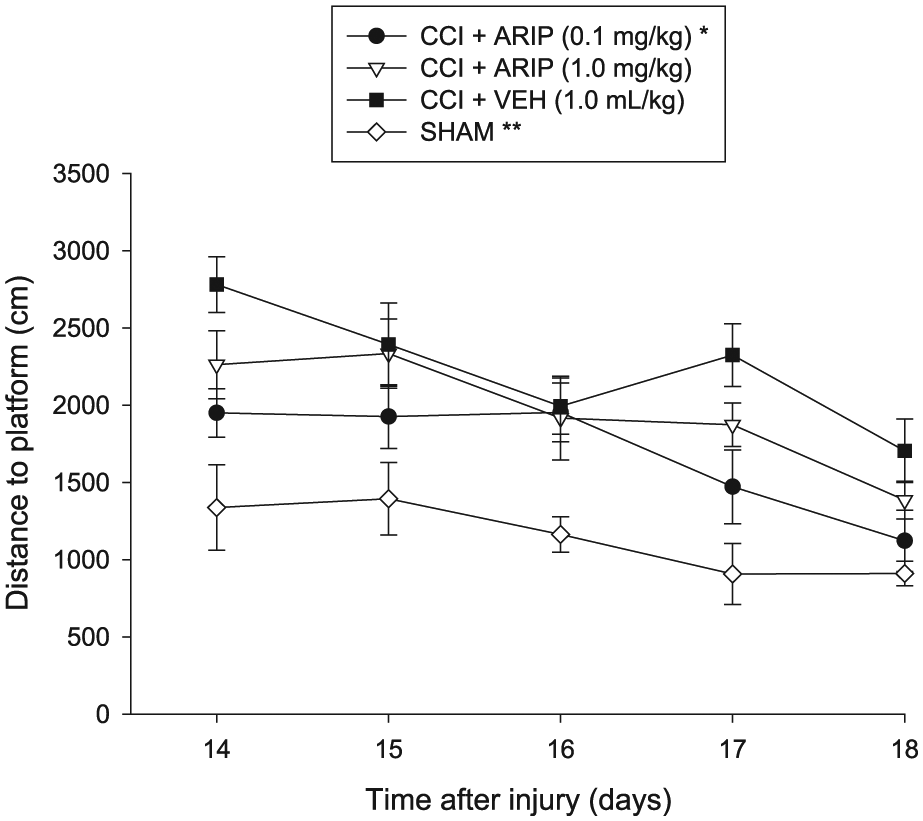
Mean (± SEM) path length (cm) during acquisition of spatial learning in the Morris water maze. There was no significant difference between the sham groups and thus they were pooled (SHAM). *P < .05 versus CCI + VEH. **P < .05 versus all CCI groups. No significant difference was revealed between the CCI + ARIP (1.0 mg/kg) and CCI + VEH groups (P > .05). ARIP, aripiprazole; CCI, controlled cortical impact; VEH, saline vehicle.
Cognitive Function: Swim Speed and Probe Trial
No significant differences in swim speed (range = 31.5 ± 0.8 to 33.8 ± 1.1 cm/s) were observed among the groups (P > .05). Analysis of the probe data did not reveal a significant difference between the SHAM and CCI + ARIP (0.1 mg/kg) groups (P > .05), but did show that both groups demonstrated significant memory retention as evidenced by a greater percentage of the 30 seconds allotted time spent in the target quadrant versus the CCI + VEH group (Ps < .05). The SHAM group also spent more time in the target quadrant than the CCI + ARIP (1.0 mg/kg) group (P < .05). Additionally, as depicted in Figure 5, the CCI + ARIP (1.0 mg/kg) group did not differ from the CCI + VEH (P > .05) or the CCI + ARIP (0.1 mg/kg) group (P > .05).
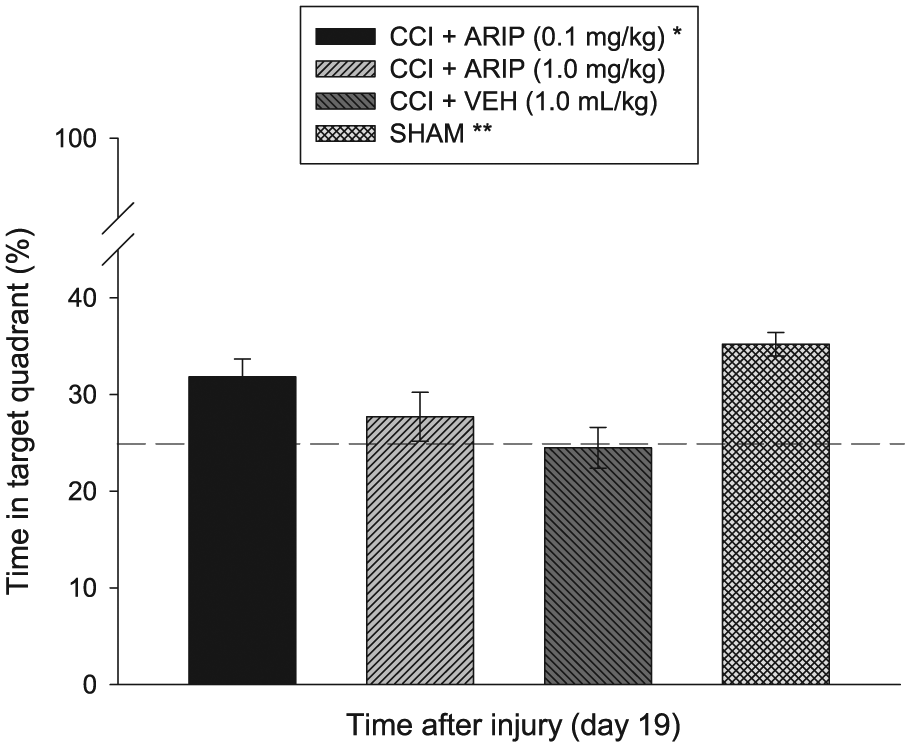
Mean (± SEM) percentage of time spent in the target quadrant (ie, where platform was previously located) following a single probe trial 19 days after traumatic brain injury (TBI) or sham injury. *P < .05 versus CCI + VEH. **P < .05 versus CCI + VEH and CCI + ARIP (1.0 mg/kg) groups, respectively. No other group comparisons were significant. The dotted line represents performance at the chance level (25%). ARIP, aripiprazole; CCI, controlled cortical impact; VEH, saline vehicle.
Histology: Quantification of Hippocampal Neurons
Controlled cortical impact produced significant reductions in normal appearing (ie, morphologically intact) CA1 and CA3 neurons in the hippocampus ipsilateral to the impact. The analyses revealed that all CCI groups differed from the SHAM control group for both CA1 and CA3 neurons (P < .0001). While there was no statistical difference among the CCI groups, regardless of treatment, in the percentage of normal appearing CA1 neurons (P > .05; Table 1), there was a significant group difference in CA3 neurons (P < .05). Specifically, as depicted in Table 1, ARIP conferred neuroprotection as revealed by greater CA3 morphologically intact cells in both the 0.1 mg/kg and 1.0 mg/kg groups versus the VEH controls (Ps < .05).
Effects of Aripiprazole (ARIP) or Vehicle (VEH) on Histopathology After Traumatic Brain Injury (TBI). a
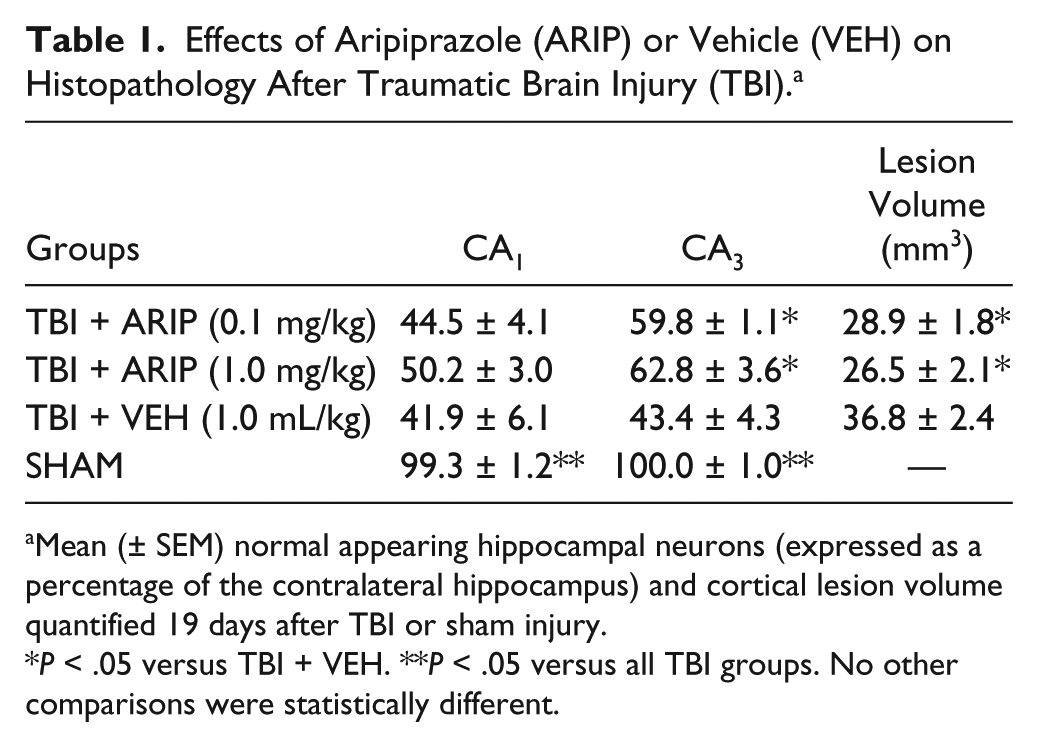
Mean (± SEM) normal appearing hippocampal neurons (expressed as a percentage of the contralateral hippocampus) and cortical lesion volume quantified 19 days after TBI or sham injury.
P < .05 versus TBI + VEH. **P < .05 versus all TBI groups. No other comparisons were statistically different.
Histology: Cortical Lesion Volume
Analysis of the cortical lesion volume data showed a significant Group effect (F2,12 = 6.428, P = .012). Subsequently, the post hoc test revealed that the lesion sizes in the CCI + ARIP (0.1 mg/kg) and CCI + ARIP (1.0 mg/kg) groups were significantly smaller than that observed in the CCI + VEH group (Ps < .05; Table 1). No differences were revealed between the ARIP-treated groups (P > .05).
Discussion
Antipsychotic drugs with D2 receptor antagonist properties have been reported to impair functional recovery in preclinical models of TBI.26-32 Despite these undesirable findings, these APDs are still frequently used to control agitation, and to a lesser extent aggression, after clinical TBI; their use can be a detriment to the TBI patients’ recovery. Hence, evaluating APDs with different pharmacological profiles is warranted. As such, the aim of the current study was to evaluate the effect of ARIP on motor, cognitive, and histological outcome after brain trauma produced by the well-established CCI injury model.28-31,38,39,46
ARIP is an atypical APD that unlike the classic HAL has no D2 antagonist effects, but rather exerts D2 and 5-HT1A receptor agonism.33-35 The hypothesis was that ARIP, which lacks D2 receptor antagonistic properties, would not negatively impact the prescribed endpoints, but rather might actually confer benefits as several studies have shown that pharmacotherapies exerting D2 and 5-HT1A receptor agonism enhance neurobehavioral and histological outcome in preclinical models of TBI.38-42 The rationale was that if the hypothesis was supported, then perhaps ARIP could be considered as a safer alternative for managing TBI-induced behavioral deficits.
Two salient findings were revealed that support the hypothesis. First, and foremost, ARIP did not negatively affect recovery after TBI regardless of dose. This finding is in marked contrast to HAL and RISP, which impair the recovery process after CCI injury whether provided before or after daily behavioral assessments.28-30 Moreover, the deleterious effects of HAL and RISP are still present 3 months after drug withdrawal indicating a long-term abatement of recovery. 31 Second, ARIP facilitated motor recovery on the beam balance agility task and enhanced spatial learning and memory in the MWM. Moreover, hippocampal CA3 neuronal loss and cortical lesion volume were reduced in both ARIP-treated groups vs. vehicle controls. The histological benefits observed with ARIP have not been seen with other APDs after TBI, and may be mediated by its neurotransmitter receptor properties, namely D2 and 5-HT1A receptor agonism.
Clinically, ARIP has also been shown in healthy subjects to enhance cognition as demonstrated by increased reaction times to a correct response in a working memory task relative to HAL and placebo controls. 47 A greater effect of ARIP on patients processing speed was also observed in patients with schizophrenia. Specifically, ARIP was superior to RISP on emotional working memory and working memory. 48 Cognitive skills have also been shown to improve with ARIP in adolescents and young adults with schizophrenia. 49 Moreover, a synergistic effect was observed in motor speed and cognition following a combination of rehabilitation and ARIP in subjects diagnosed with schizophrenia or schizoaffective disorder. 50 The findings suggest that combining treatments can be more effective than individual therapies. Indeed, work from Kline et al 41 has shown an added protective effect on choline acetyltransferase (ChAT) cells after TBI when 8-OH-DPAT is combined with environmental enrichment (EE), a preclinical model of neurorehabilitation. Recently, in a pediatric model of TBI, Monaco and colleagues 51 showed an additive effect on cognitive performance when combining buspirone and EE.
A possible mechanism for the ARIP-induced benefits on motor, cognitive, and histological outcome may include its actions as a 5-HT1A receptor agonist. As alluded to earlier, 5-HT1A receptor agonists have been shown to confer neuroprotection and functional recovery after TBI. The benefits are seen whether 8-OH-DPAT is provided acutely or chronically after CCI injury.40,42 Moreover, buspirone also confers significant cognitive and histological protection after TBI.44,51 5-HT1A receptor agonists impart multiple physiological actions, but one intimately tied to cognition is cholinergic interaction. It is understood that the neurotransmitter acetylcholine is involved in learning and memory.52,53 Moreover, significant decreases in ChAT expression are observed after CCI injury 41 and after the administration of HAL and RISP. 54 Treatment with 8-OH-DPAT after a CCI injury attenuated the TBI-induced loss of medial septal ChAT cells and improved MWM performance. 41 As a 5-HT1A receptor agonist ARIP may produce similar effects and thus protection of cholinergic integrity may be a possible mechanism for the findings.
An additional or alternate mechanism mediating the benefits conferred by ARIP may be via the dopaminergic system. The D2 receptor agonist bromocriptine (BRO) promotes cognitive recovery and also reduces TBI-initiated malondialdehyde, in multiple brain regions.38,39 BRO has been reported to attenuate HAL-induced neuronal toxicity, perhaps by attenuating mitochondrial dysfunction and production of hydroxyl free radicals. 55 This is relevant due to the fact that oxidative stress is one of numerous pathophysiological effects induced by TBI that contributes to cognitive dysfunction. 39 Because ARIP is a partial D2 receptor agonist, this may be yet another potential explanation for the observed benefits in the current study. However, before definitive statements on potential mechanisms can be made, follow-up studies evaluating the effects of ARIP on ChAT cell protection and/or attenuation of oxidative stress after TBI are required.
In conclusion, our data show that ARIP did not yield deleterious effects on motor or cognitive function after experimental TBI, which is unlike that consistently observed with HAL and RISP.28-32 Furthermore, the lower dose of ARIP facilitated the acquisition of spatial learning relative to the vehicle-treated group and did not differ from sham controls. This narrow dose response is similar to what has been reported with other 5-HT1A receptor agonists.40-42,44,51 Overall, the findings support the hypothesis and present ARIP as a safer APD for alleviating behavioral disturbances after TBI. Moreover, ARIP may have further rehabilitative potential by improving cognitive recovery in TBI patients. To expand further on this promising avenue, future studies should investigate the benefits of ARIP in combination with EE, a preclinical model of neurorehabilitation.56,57
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by National Institutes of Health grants NS084967, NS060005, HD069620, and HD069620-S1 (AEK).