
Abstract
Background. Alzheimer’s disease (AD) is a highly prevalent neurodegenerative disorder. Rate of decline and functional restoration in AD greatly depend on the capacity for neural plasticity within residual neural tissues; this is at least partially influenced by polymorphisms in genes that determine neural plasticity, including Apolipoprotein E4 (ApoE4) and synaptosomal-associated protein of 25 kDa (SNAP-25). Objective. We investigated whether correlations could be detected between polymorphisms of ApoE4 and SNAP-25 and the outcome of a multidimensional rehabilitative approach, based on cognitive stimulation, behavioral, and functional therapy (multidimensional stimulation therapy [MST]). Methods. Fifty-eight individuals with mild-to-moderate AD underwent MST for 10 weeks. Neuro-psychological functional and behavioral evaluations were performed blindly by a neuropsychologist at baseline and after 10 weeks of therapy using Mini-Mental State Examination (MMSE), Functional Living Skill Assessment (FLSA), and Neuropsychiatric Inventory (NPI) scales. Molecular genotyping of ApoE4 and SNAP-25 rs363050, rs363039, rs363043 was performed. Results were correlated with ΔMMSE, ΔNPI and ΔFLSA scores by multinomial logistic regression analysis. Results. Polymorphisms in both genes correlated with the outcome of MST for MMSE and NPI scores. Thus, higher overall MMSE scores after rehabilitation were detected in ApoE4 negative compared to ApoE4 positive patients, whereas the SNAP-25 rs363050(G) and rs363039(A) alleles correlated with significant improvements in behavioural parameters. Conclusions. Polymorphisms in genes known to modulate neural plasticity might predict the outcome of a multistructured rehabilitation protocol in patients with AD. These data, although needing confirmation on larger case studies, could help optimizing the clinical management of individuals with AD, for example defining a more intensive treatment in those subjects with a lower likelihood of success.
Introduction
Alzheimer’s disease (AD) is an adult-onset neurodegenerative disorder affecting more than 35 million persons worldwide. 1 The clinical phenotype of AD is characterized by dementia, an acquired syndrome consisting of progressive deterioration in global intellectual ability of such severity, that interferes with usual social and occupational performance. 2
While the spectrum of symptoms in AD includes impaired cognition, function, and behavior, the expression of these features varies across individuals. Thus, a wide range of variability does exist in the age at onset of symptoms, domains of cognition affected, extent of functional dependence, prevalence of behavioral symptoms, and rate of decline. 3 Genetic factors are associated with this variability, as disease progression and functional restoration greatly depend on the capacity for neural plasticity within residual neural tissues. 4 This is at least partially influenced by polymorphisms in genes known to orchestrate neural plasticity, including Apolipoprotein E4 (ApoE4) and synaptosomal-associated protein of 25 kDa (SNAP-25). Thus, cognitive decline is faster in patients who carry the ApoE4 (Apo E4+) allele 5 , and, on the other hand, recent results showed that ApoE4 status predicts the outcome of cognitive stimulation (CS) on visuospatial memory. 6 SNAP-25 is a vesicular SNARE protein that plays an important role in the release of neurotransmitters by interacting with voltage-gated calcium channels, 7 inhibiting their function, and reducing responsiveness to depolarization.8,9 SNAP-25 polymorphisms were shown to correlate with risk of developing AD. In particular, the intronic rs363050(A) and rs363043(T) alleles, as well as the rs363050/rs363043 A-T haplotype resulted significantly more frequent in persons with AD and were associated with pathological scores of categorical fluency and functional MRI (fMRI) parameters in AD. 10
As an effective pharmacological treatment for AD is still missing, the potential usefulness of non-pharmacological interventions in both preventing and slowing cognitive decline in AD 11 is actively investigated. A growing number of studies is evaluating the efficacy of CS in elderly subjects with cognitive impairment. 12 Results indicate that a single cycle of CS therapy is effective in improving the cognitive level of people with AD,13,14 and long-term administration of this therapy was shown to improve quality of life. 15 Overall results also suggest that occupational therapies as well as physical exercise can reduce psychobehavioral disturbances in patients with dementia and can increase their interaction with the environment, enhance their quality of life, and reduce their negative attitudes.16,17
A multidimensional approach 18 based on CS as well as recreational/occupational and psychomotor/physical therapy was developed in our center. This approach, multidimensional stimulation therapy (MST),19-21 has been shown over the past 10 years not only to improve behavioral and cognitive disturbances but also to increase the activation of temporal areas in the right insular cortex and in the thalamus, as determined by fMRI. 22 However, few data are available on factors influencing the outcome of non-pharmacological therapies in people with AD.
Because genetic patterns have convincingly been shown to modulate the clinical severity of AD, 10 we investigated whether any correlations could be detected between ApoE4 positive/negative (Apo E4+/Apo E4-) and SNAP-25 polymorphisms and the outcome of rehabilitative treatment in patients with mild-to-moderate AD. In this work, we demonstrated that this is indeed the case, as specific associations were detected between both such polymorphisms and the degree of success of MST.
Methods
Patients
Fifty-eight patients (32 females/26 males, mean age 75.8 years; SD = 5.4 years) who underwent MST at the Neurology Departments of the Don Gnocchi Foundation were included in this study. All patients had a clinical diagnosis of probable or possible AD with associated mild cerebrovascular disease in mild to moderate stage of progression according to the NINCDS-ADRDA Work Group criteria. 23 All patients underwent complete medical and neurological evaluation, laboratory analysis, computed tomography scan or MRI, and other investigations when necessary (eg, electroencephalography, single-photon emission computed tomography scan, cerebrospinal fluid examination, etc) to exclude reversible causes of dementia. Blood count, urine analysis, blood chemistry screen, serum folate, B12 levels, and thyroid functions tests were evaluated prior to the enrollment; none of the patients enrolled suffered from malnutrition or vitamin deficiency syndromes. Patients were excluded if they had (a) severe aphasia (Token test score <20) 24 or severe auditory and/or visual loss, (b) overt severe behavioral disturbances that could hinder the MST session, and (c) recent (3 months before MST) introduction or dose modification of the following pharmacological treatments: cholinesterase inhibitor, memantine, antidepressant, or antipsychotic drugs. Low-dose benzodiazepines for insomnia were allowed during the study. All the Individuals enrolled in the study, and their relatives when appropriate, provided written informed consent according to a protocol approved by the local ethics committee of the Don C. Gnocchi Foundation before admission to the study.
Every patient was examined twice: at baseline and at the end of the 10-week treatment.
Rehabilitative Methods
The MST program involves 3 different actors: persons with Alzheimer (PWA), the dyad PWA-caregiver, and the caregiver himself or herself. Among the caregivers, 14 husbands, 17 wives, 7 sons, 11 daughters, and 1 sister of AD patients as well as 8 nurses were enrolled. In all, 47/58 caregivers were living with the patient.
People with AD performed 30 group rehabilitation sessions (2.5 hours a day, for 3 days a week, for a total of 10 weeks). In detail, the treatment involves 4 steps: (a) reality orientation activities and cognitive exercises (about 45 minutes), (b) physical activity (about 30 minutes), (c) occupational activities of daily living (about 30 minutes), and (d) recreational activities (about 45 minutes).
The treatment was administered by a psychologist and a rehabilitation therapist, both of whom were specialized in cognitive rehabilitation and trained in our center. All subjects performed further stimulation (45-minute walk and specific cognitive activities) at home with their caregiver. Every caregiver underwent two support interviews with a psychologist and attended an educational course.
For further details on the rehabilitation treatment efficiency see Baglio et al 22 and Farina. 25
Neuropsychological, Functional, and Behavioral Evaluation
Changes in cognitive, functional, and behavioral status were assessed by an experienced neuropsychologist blinded to the treatment status who used psychometric tests and scales. Mini-Mental State Examination (MMSE) was used as an index of change in cognitive functions, and, for the purpose of this work, MMSE raw scores were adjusted for age and educational level (conversion formulae are reported in Magni et al 26 ); only corrected scores were counted for correlation analysis. The Functional Living Skills Assessment (FLSA) 27 was used as a measure of functional performance; FLSA assesses performance in tasks of everyday life through direct observation of role-playing. Finally, behavioral disturbances were assessed with the Neuropsychiatric Inventory (NPI) scale. 28
ApoE4 Genotyping
Genomic DNA was isolated from peripheral blood mononuclear cells (PBMC) by phenol-chloroform extraction. Custom-designed taqman probes for the 112 and 158 codons were used. Primers and probes for the 112 codon are: 112 forward primer: 5′-GGG CGC GGA CAT GGA G-3′, 112 reverse primer: 3′–TCC TCG GTG CTC TGG CC-5′, 112 Arg Probe: 5′-CGT GCG CGG CCG-3′-FAM, 112 Cys Probe: 5′-ACG TGT GCG GCC GCC TG-3′-VIC. Primers and probes for the 158 codon are: 158 forward primer: 5′-TCC GCG ATG CCG ATG-3′, 158 reverse primer: 3′-GCT CGG CGC CCT CG-5′, 158 Arg probe: 5′-CCT GCA GAA GCG CCT GGC A-3′-FAM, 158 Cys probe: 5′-CCT GCA GAA GGG CCT GGG AGT-3′-VIC.
SNAP-25 Genotyping
SNPs rs363043, rs363039, rs363050, located into intron 1 of SNAP-25 gene were typed using the Taqman SNP Genotyping Assays (Applied Biosystems by Life Technologies, Foster City, CA, USA) on an ABI PRISM 7000 Sequence Detection System. For rs363039, rs363043, rs363050, respectively, the C_327976_10, C_2488346_10 C_329097_10. Human Pre-Designed Assays (Applied Biosystems by Life Technologies) were used.
Statistical Analysis
The Kolmogorov-Smirnov test was applied to verify normal distribution of numerical variable scores. All numerical scores, resulted normally distributed, and they were shown as mean and standard deviation (SD). Paired t-test was adopted to calculate variations in MMSE, NPI, and FLSA scores after MST. Linear regression analysis was performed between mean delta score of MMSE, NPI, FLSA evaluations after rehabilitative treatment and age, age of disease onset, disease duration, level of education and mean baseline score of each scale. Analysis of variance was performed to analyse gender association with MMSE, NPI, and FLSA delta scores. Chi-square analysis was used to exclude any deviation of SNPs genotype distribution from Hardy-Weinberg equilibrium. A multivariate logistic forward stepwise regression model was computed using Apo E4+ vs Apo E4- as response variables and difference between scores evaluated after rehabilitative treatment and at baseline (∆) of MMSE, NPI, and FLSA scales as explanatory variables. Moreover, this model was corrected by MMSE at baseline (MMSEb), NPIb, and FLSAb values, age of patients at the baseline, their level of education and gender. Similarly a multinomial, multivariate logistic regression analysis was performed evaluating each SNAP-25 polymorphic genotype as responsible variable and ∆MMSE, ∆NPI, and ∆FLSA as explanatory variables, together with MMSEb, NPIb, and FLSAb values, age of patients at the baseline, their level of education, gender, and Apo E4+ genotype, which were considered as covariates. Haplotype association analysis was performed using Plink software 29 by logistic regression analysis; haplotype probabilities of individual subjects were incorporated as covariates in the regression model, which estimate the beta value associated with ∆MMSE, ∆NPI, and ∆FLSA.
Results
Neuropsychological evaluations were performed at baseline and at the end of the 10 weeks treatment. Detailed data regarding MMSE, NPI, and FLSA evaluation at baseline (MMSEb, NPIb, FLSAb), and after MST treatment (MMSEf, NPIf, FLSAf), are presented in Table 1. A paired t-test analysis of MMSE, NPI, FLSA basal versus final scores was calculated; results indicated a statistically significant improvement for each of the scales that were evaluated (P = .003; P = .007, P = .01; df = 57, respectively) (Table 1). For further details please see Farina et al 21 and Baglio et al. 22 Differences between the results obtained at 10 weeks and at baseline are reported as delta scores (ΔMMSE, ΔNPI, ΔFLSA) (Table 1). Improvement are represented by ΔMMSE and ΔFLSA >0, whereas a behavioral improvement is described by ΔNPI <0. Results of correlation analyses between ΔMMSE, ΔNPI, and ΔFLSA values and demographic factors, calculated by linear regression analysis, considering the baseline value of each scale as covariate, are presented in Table 2.
Genotype Distribution of ApoE and SNAP-25 Polymorphisms in 58 AD Patients, MMSE, NPI, FLSA Evaluation Pre (b) and Post (f) MST.
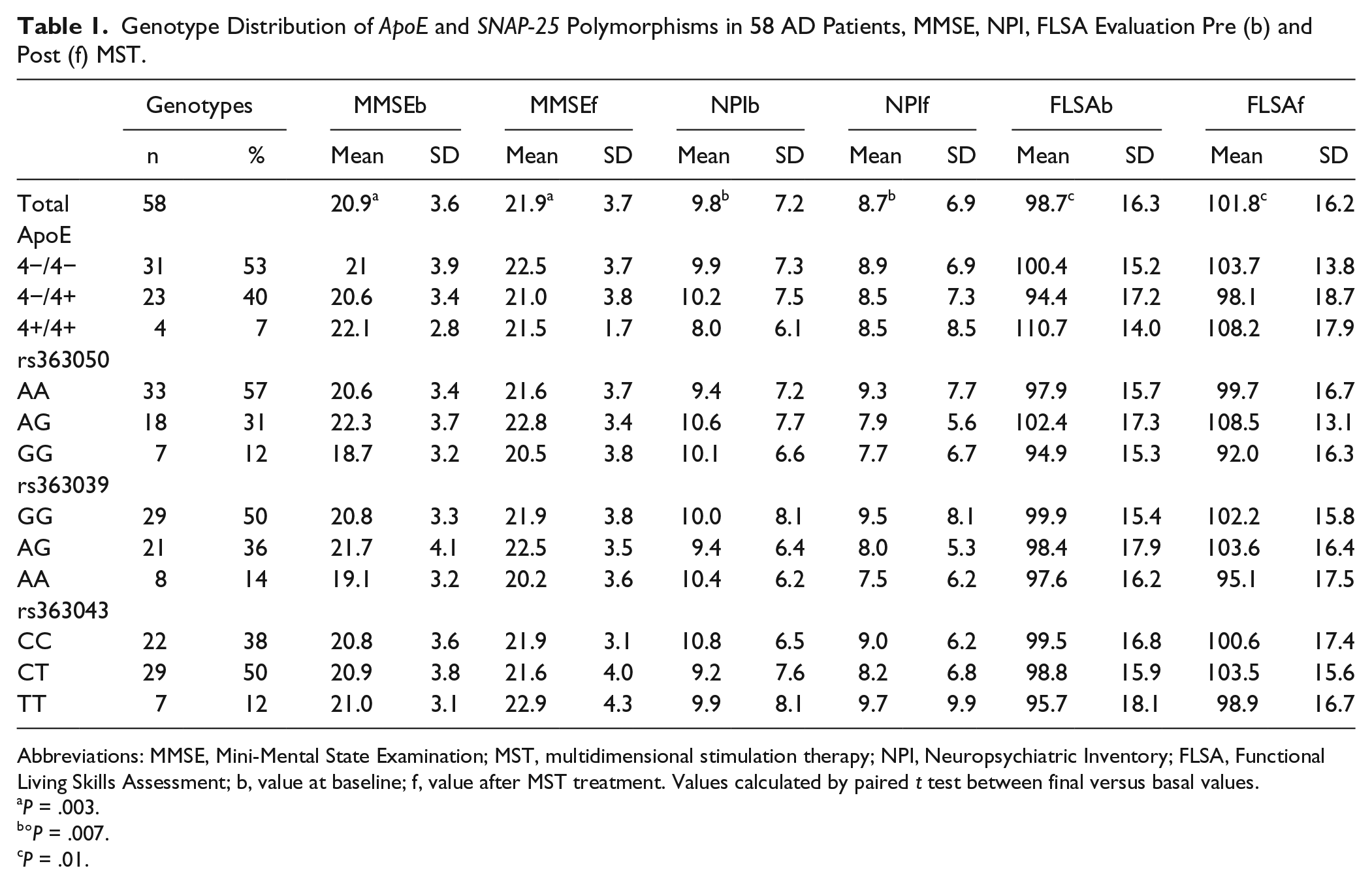
Abbreviations: MMSE, Mini-Mental State Examination; MST, multidimensional stimulation therapy; NPI, Neuropsychiatric Inventory; FLSA, Functional Living Skills Assessment; b, value at baseline; f, value after MST treatment. Values calculated by paired t test between final versus basal values.
P = .003.
°P = .007.
P = .01.
Linear Regression Analysis Between Mean Delta Score of MMSE, NPI, and FLSA Evaluations After Rehabilitative Treatment and Demographic Data of AD Patients.

Abbreviations: MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory; FLSA, Functional Living Skills Assessment; MMSEb, MMSE value at baseline; NPIb, NPI value at baseline; FLSAb, FLSA value at baseline; ∆, delta between final versus basal values.
Statistically significant P value (P value adjusted for baseline values).
A significant association between ∆MMSE values and gender (female vs male) (negative beta value of association to females: P = .02, β = −0.33) was found; this result indicates that a lower outcome at MMSE was observed in female compared with male AD patients. A borderline significant positive correlation between MMSE values and age at baseline was observed as well (P = .05, β = +0.25).
Results also showed NPI outcomes to be negatively associated with the level of education (P = .02, β = −0.31). In contrast, no correlations were found between cognitive and behavioral outcomes after treatment, disease duration, age at baseline, and age at onset.
ApoE Genotypes
Twenty-seven of the 58 patients carried the Apo E4 allele (Apo E4+): 4 were E4+/E4+ homozygote and 23 were E4+/E4− heterozygote (all were E4+/E3+). Among Apo E4−/E4− subjects: 4 carried the E2/E3 genotype and 27 were E3+/E3+. Genotype distribution and frequencies are reported in Table 1, ApoE genotype distribution resulted to be in Hardy-Weinberg equilibrium.
Multivariate logistic forward stepwise regression model was performed to calculate possible association between ApoE polymorphisms and ΔMMSE, ΔNPI, and ΔFLSA scores. Apo E4+ and Apo E4− allelic association with Δvalues for each scale was calculated after correction for baseline values, age, level of education and gender, which were considered as covariates. Results indicated the presence of a statistical association between ApoE polymorphism and ΔMMSE scores after treatment (P = .041). Therefore, a weak positive effect of the Apo E4− allele (odds ratio [OR] = 1.4; 95%CI = 1.0-1.9) on the outcome of MST was observed (ΔMMSE = 1.5 ± 2.4), whereas the Apo E4+ allele was correlated with lower MMSE scores after therapy (ΔMMSE = 0.1 ± 1.8). Graphical results are shown in Figure 1. We also compared individuals carrying Apo E4−/E4− versus those carrying E4+/E4− and E4+/E4+ in order to evaluate any gene dose effect. Notably, a negative response to treatment was observed in Apo E4+/E4+ homozygous subjects (ΔMMSE = −0.5 ± 1.9) (OR = 0.6), whereas an intermediate MMSE outcome was observed in subjects carrying at least one ApoE4 allele as heterozygote Apo E4+/E4− (ΔMMSE = 0.2 ± 1.8) (OR = 1.0). The best responses were detected in (E4−/E4−) homozygous carriers (ΔMMSE = 1.5 ± 2.4) (OR = 1.5), even if this trend did not reach statistical significance. Similarly, a better outcome of NPI scores after MST was present in Apo E4− carriers compared with in Apo E4+ (Figure 1 panel B). Finally no associations were observed between ApoE polymorphisms and ΔFLSA results (Figure 1 panel C).
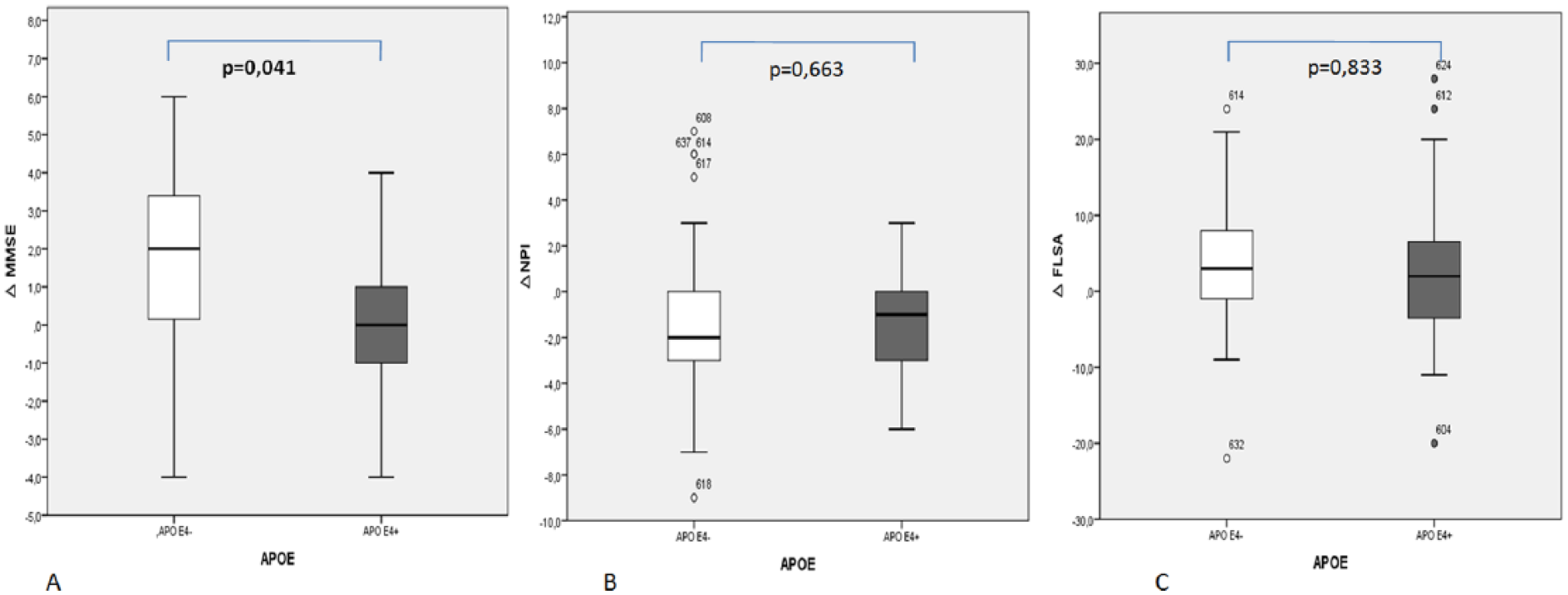
Box plot data and statistical association after multivariate logistic regression analysis of ApoE association to ΔMMSE (panel A), ΔNPI (panel B) and ΔFLSA (panel C). Apo E4+ vs Apo E4− was considered as dependent variable, baseline values MMSEb, NPIb, and FLSAb, age at baseline, level of education, and gender were computed as covariates. ° represents outliers cases. MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory; FLSA, Functional Living Skills Assessment.
SNAP-25 Genotypes
Frequency of distribution of the three analyzed SNAP-25 gene SNPs (rs363043(C/T), rs363039(G/A), rs363050(A/G)) is reported in Table 1, all the polymorphisms were in Hardy-Weinberg equilibrium. Moreover the SNAP-25 polymorphic genotype distribution was evaluated next by multinomial multivariate logistic regression analysis in relationship with ΔMMSE, ΔNPI, and ΔFLSA scores. SNAP-25 genotypes categories for each SNP were considered as the dependent variable and possible associations with the Δ values were calculated after correction for the baseline value, age, level of education, gender and ApoE genotype (E4− vs E4+), which were considered as covariates.
A statistically significant association was observed between ΔNPI values and the rs363050 and rs363039 SNAP-25 genotypes (Figure 2 panels B and E). In particular, subjects carrying the rs363050(G) as well as the rs363039(A) alleles were characterized by lower ΔNPI scores, which correspond to an improvement in behavioural functions after rehabilitative treatment. Notably, a significantly better outcome after treatment was observed in individuals carrying the minor rs363050 homozygote (GG) (ΔNPI = −2.4 ± 3.1) compared with those with the major homozygote (AA) genotype (ΔNPI = −0.9 ± 3.0) (P = .015, OR = 0.2, 95% CI = 0.03-0.7), and in those with the heterozygote (AG) (ΔNPI = −2.7 ± 2.9) compared with those with the homozygote (AA) genotype (P = .007, OR = 0.5, 95% CI = 0.3-0.8) (Figure 2 panel B). A lower OR value was observed in subjects carrying only the minor allele (A) as homozygous genotype (AA) (OR = 0.2) compared with those carrying both alleles (AG) as heterozygote (OR = 0.55), suggesting a higher impact if 2 minor alleles are carried. No statistically significant differences were nevertheless observed between (GG) and (AG) genotypes (P = .088) (Figure 2 panel B). A similar significantly better outcome was observed in subjects carrying the rs363039 minor homozygote (AA) (ΔNPI = −2.9 ± 3.1) compared with those with the major homozygote (GG) genotype (ΔNPI = −0.5 ± 3.2) (P = .019, OR = 0.09, 95% CI = 0.01-0.7) (Figure 2 panel E). Patients carrying the heterozygous genotype (AG) showed a better outcome (ΔNPI = −1.5 ± 2.9) than those homozygote for (GG) genotype (ΔNPI = −0.5 ± 3.2) though not statistically significant (P = .369, OR = 0.1, 95% CI = 0.9-1.1) (Figure 2 panel E). Also in this case a lower OR value was observed in patients carrying the minor allele as homozygote (AA) (OR = 0.09) than in those with the heterozygote genotype (AG) (OR = 0.1) (P = .025, OR = 0.1, 95%CI = 0.01-0.8), suggesting a possible dose effect association of these genotypes with the NPI outcome.
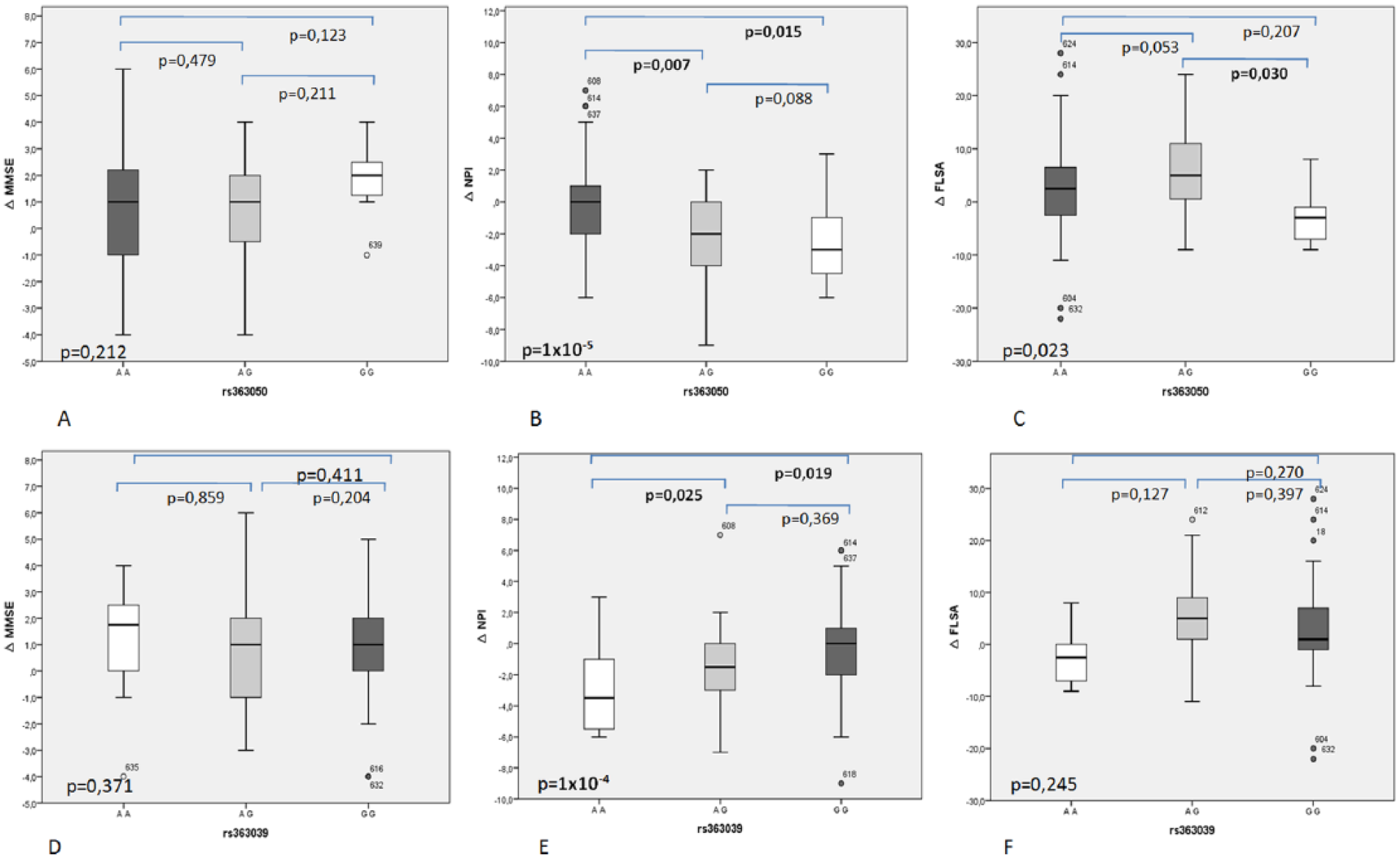
Box plot data and statistical association after multinomial multivariate regression logistic analysis between SNAP-25 rs363050 genotypes and ∆MMSE scores, (panel A) ∆NPI scores (panel B), ∆FLSA scores (panel C). Box plot data and statistical association after multinomial multivariate regression logistic analysis between SNAP-25 rs363039 genotypes and ∆MMSE scores, (panel D) ∆NPI scores (panel E), ∆FLSA scores (panel F). ° represents outliers. MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory; FLSA, Functional Living Skills Assessment.
Subjects carrying rs363050 (GG) and/or rs363039 (AA) genotypes showed higher MMSE scores after MST treatment though this association did not reach statistical significance after multinomial regression analysis (Figure 2 panels A and D, respectively). No associations were observed between SNAP-25 polymorphisms and ∆FLSA results. No association was observed between rs363043 and MMSE, NPI, or FLSA outcome.
ApoE and SNAP-25 Interaction
Possible epistatic interactions between ApoE and SNAP-25 polymorphisms on the outcome of the MST intervention were evaluated. Firstly patients were clustered for Apo E4+ and Apo E4− genotypes and the association of SNAP-25 polymorphisms with ∆NPI, ∆MMSE, and ∆FLSA scores was analyzed by multinomial multivariate regression analysis adopting the same covariates evaluated on the whole group of patients (baseline value, age, level of education, gender). No significant association were detected when either in the Apo E4+ or in the Apo E4− subjects were analyzed separately (data not shown). Patients were next stratified on the basis of different SNAP-25 genotypes in order to evaluate ApoE4 impact in groups belonging to diverse SNAP-25 genotypes. Also in this case no statistical association was noticed with MST outcome.
SNAP-25 Haplotype Analysis
The detection of a linkage disequilibrium between rs363050, rs363039, and rs363043 SNPs in intron 1 (Figure 3) led us to further analyze possible associations between this haplotype and MST outcomes. The frequencies of haplotype distribution are reported in Table 3 and show the presence of a significant association between SNAP-25 haplotypes and lower ΔNPI. In particular the rs363050(G)-rs363039(A)- rs363043(C)-(GAC) haplotype was statistically associated with a better outcome of treatment as measured by the NPI scale (P = .03, β = −1.27) (Table 3).
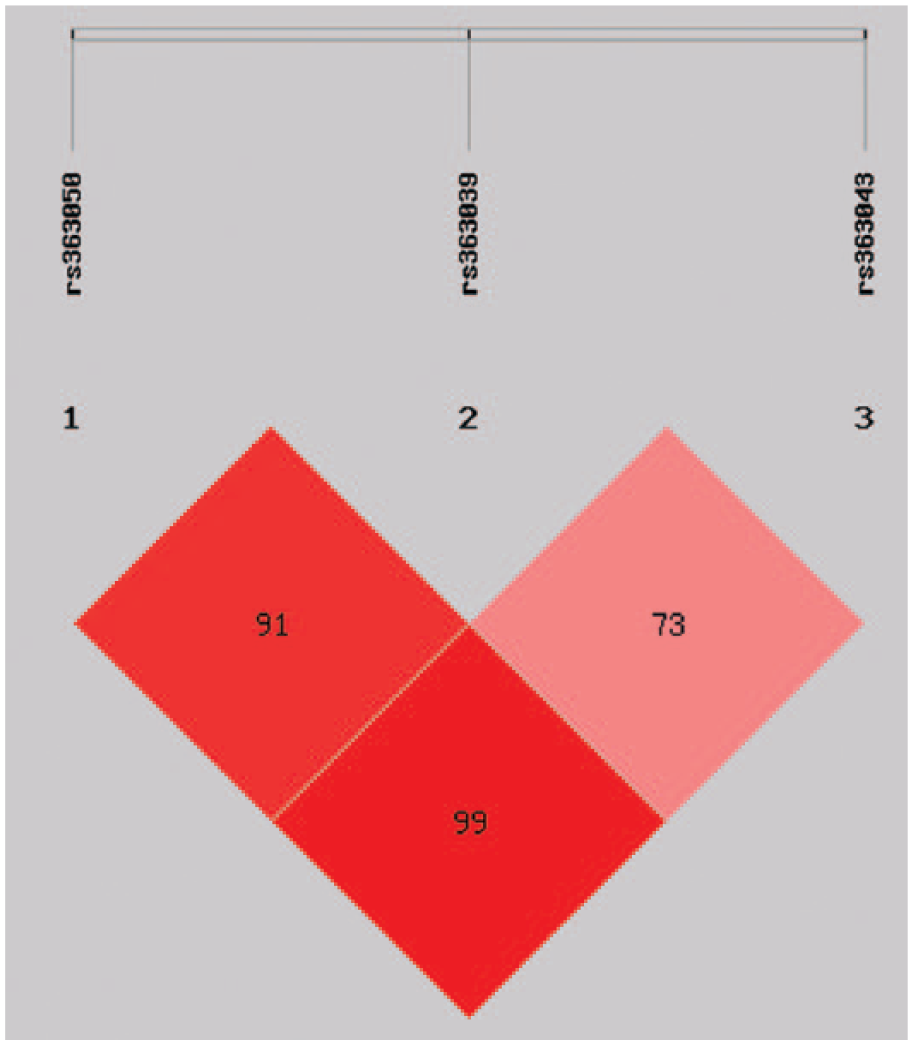
Linkage disequilibrium of SNAP-25 rs363050, rs363039, and rs363043 mapping in Intron 1.
Haplotype Association Between SNAP-25 rs363050, rs363039, rs363043, and ΔNPI Values.
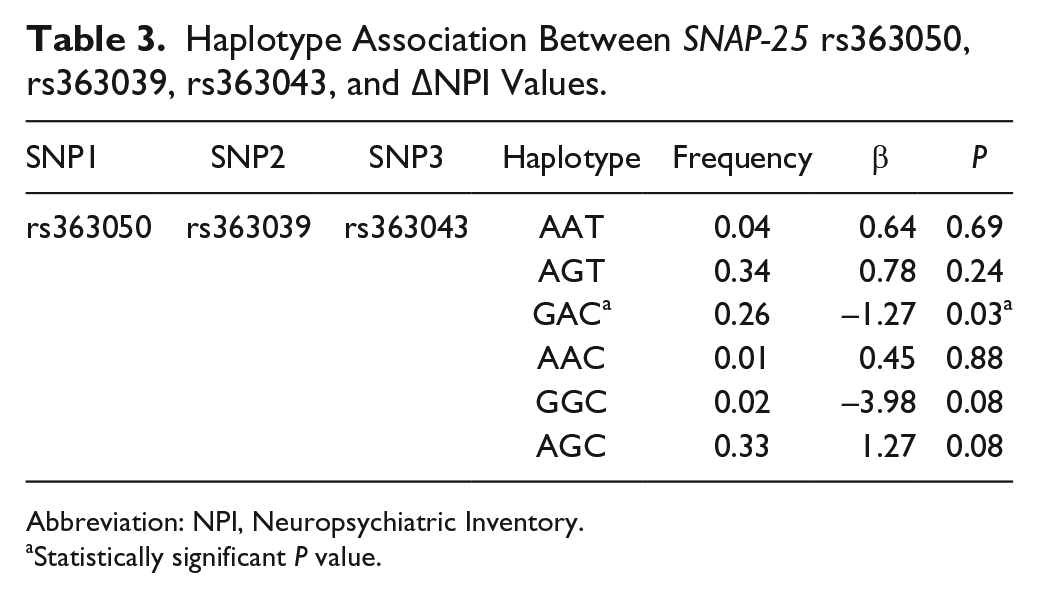
Abbreviation: NPI, Neuropsychiatric Inventory.
Statistically significant P value.
Discussion
Alzheimer’s disease is a highly prevalent neurodegenerative disorder with a complex and unclear pathogenesis; pharmacological therapies for AD are not yet available, and the efficacy of physical and occupational treatments is greatly variable amongst patients. Genetic factors play a role in the pathogenesis of AD. Thus, besides the presence of the E4 allele of Apolipoprotein E gene (ApoE4), the only known confirmed genetic risk factor for sporadic AD, single nucleotide polymorphisms in various genes, including interleukin-10, PIN-1,30,31 and SNAP-25, 10 have been shown to correlate with susceptibility to disease and to the rate of clinical progression. We explored whether the outcome of multidimensional stimulation, including CS, in AD could be associated as well with the genetic background of the patient, focusing on ApoE4 and SNAP-25 polymorphisms. Data herein suggest that this is indeed the case as significant associations were detected between such polymorphisms and the effect of rehabilitation.
In particular, we observed that the risk alleles Apo E4+ and SNAP-25 rs303050 (A) and rs363039 (G) were associated with a lower outcome after MST treatment for MMSE and NPI score, whereas no effect were observed at FLSA. Statistically significant MMSE scores after rehabilitation were detected in Apo E4− compared with Apo E4+ patients, though at a low level of significance, and the SNAP-25 rs363050(G), rs363039(A) alleles and rs363050(G)-rs363039(A)-rs363043(C)-(GAC) haplotype correlated with a significantly better outcome after MST as measured by the NPI scale. From a (still) purely speculative point of view it is interesting to observe that, whereas ApoE status is known to correlate with cognitive impairments, SNAP-25 polymorphisms have instead been associated with behavioral pathologies, such as those that characterize autistic spectrum disorders.
Among subjects carrying E4+ allele, those with the E4−/E4+ heterozygous genotype were characterized by an intermediate OR score of association with MMSE improvement after MST. Interestingly, OR score of association with MST-associated MMSE improvements were higher in E4−/E4+ individuals and lower in E4+/E4+ subjects, even if the overall number of analyzed individuals was too low to reach statistical significance. This observation, nevertheless, suggests a probable gene dose effect on the outcome of MST, even if this possibility will need to be validated in a larger case study. However this observation may be supported by recent pharmacogenetic studies evidencing that ApoE4 allele influences the therapeutic outcome in AD patients suggesting Apo E4+/E4+ homozygous carriers as the worst responder to conventional treatment of AD patients 32 and that different drugs may reduce the risk of AD development only in subjects who do not carry ApoE4 allele.33-35
Notably, our data are in agreement with recently published evidences indicating a poorer efficacy of Cognitive Stimulation on visuospatial memory performance measured using the Corsi test 6 in Apo E4+ patients. The ApoE4 status has been reported to influence cognitive functions, 36 possibly because ApoE gene produces a protein that plays an important role in neuronal plasticity and repair.37-39 Thus, the ApoE lipoprotein stimulates synapse development, 40 clearance of lipid debris, 41 and promotion of granule cell mossy fiber sprouting. 42 The effectiveness of these processes is reduced when the E4 allele directs ApoE production. Data in mouse model reinforce the idea that ApoE alleles are involved in AD. Thus, a more efficient degradation of ApoE4 in astrocytes in transgenic mice results in lower levels of ApoE in the brain and cerebrospinal fluid, suggesting that the reduced levels of total ApoE seen in ApoE4 carriers may directly contribute to disease progression. Apo E4+ is also less efficient than Apo E4− in transporting brain cholesterol. 43 Very recently, an increase of amyloid accumulation and allele frequency of ApoE4 was seen in mild traumatic brain injury patients with cognitive impairment,44,45 and a meta-analysis concluded that the ApoE4 allele may be associated with a poor prognosis in severe traumatic brain injury patients. 46 These evidences suggest that an ApoE4 cognitive phenotype could be associated with more inefficient mechanisms of neuronal repair and plasticity. It is therefore possible that people with AD carrying ApoE4 are less able to engage cognitive reserve mechanisms that could benefit from CS, with the result that carriers and non-carriers benefit differently from experiences that enhance cognition.
Several studies show that engaging in regular exercise could be useful in preventing AD, and suggest that the mechanisms through which this benefit occurs are influenced differently depending on ApoE allele status. Some authors reported an association between physical activity and reduced AD risk that is restricted to carriers of the ApoE4. 47 Conversely more recent studies 48 found that physical activity correlates with cognitive status in non-carriers of the ApoE4 allele, but not in ApoE4 carriers. Recently, it was reported that plasma Abeta(1-42/1-40) levels were lower in people undertaking higher levels of physical activity, yet this was only significant in non-ApoE4 subjects. 49 Further studies are needed to ascertain the optimum levels of activity needed for individuals of each genotype to obtain the greatest benefit to cognitive health.
Polymorphisms in the SNAP-25 gene, on the other hand, were mostly correlated with results at MST when behavioural improvement was measured. Thus, the SNAP-25 rs363050 (G) and rs363039(A) alleles, as well as the SNAP-25 rs363050(G)-rs363039(A)-rs363043(C)-(GAC) haplotype, which are in linkage disequilibrium, were statistically associated with lower NPI scores after treatment, that is, with a more relevant effect of this treatment of behavioral parameters. Finally, a more important NPI improvement was observed in those patients that were homozygotes for the SNAP-25 minor alleles rs363050(GG) and rs363039(AA) compared with those who were rs363050(AG) and rs363039(AG) heterozygtes, suggesting a gene dose effect of the minor allele in both polymorphisms. Also in this case, however, this will need to be confirmed in a larger case study. No relationships between SNAP-25 rs363043 and MST outcomes were observed.
The association of rs363043(C) allele within the haplotype rs363050(G)-rs363039(A)-rs363043(C)-(GAC) may be due to the linkage disequilibrium existing between these SNPs.
Subjects carrying rs363050 (GG) and/or rs363039 (AA) genotypes showed also a better outcome at MMSE evaluation after MST treatment, but this trend did not result statistically significant at the multinomial regression analysis. Probably the impact on cognitive performance of SNAP-25 polymorphism is not as high as the one of ApoE polymorphism.
SNAP-25 is a vesicular SNARE protein that plays an important role in the release of neurotransmitters via its interaction with voltage-gated calcium channels. SNAP-25 gene polymorphisms are suggested to associate with intelligence and were shown to be involved in a number of neurologic conditions, including bipolar and behavioral disorders as ADHD and autistic spectrum disorders. We have recently suggested a role for SNAP-25 polymorphism in the risk of developing AD in individuals with a diagnosis of mild cognitive impairment. In particular, we have shown that the complementary rs363050(A) allele is significantly more frequent in patients with AD and mild cognitive impairment and is associated with pathological scores of categorical fluency and functional MRI parameters in individuals with a diagnosis of AD dementia. 10
Previous studies suggested that synaptic loss correlates with the clinical manifestations of AD, while there is no relation between the number of accumulated parenchymal amyloid plaques and synaptic pathology.50,51 Other results showed that SNAP-25 expression negatively correlates with MMSE scores, as higher cerebrospinal fluid concentrations of SNAP-25 were seen in patients suffering from more severe cognitive decline. 52 Notably (a) an excess of SNAP-25 activity during adulthood is sufficient to mediate significant deficits in the memory formation process, (b) expression of SNAP-25 in the adult dorsal hippocampus results in the deregulation of memory consolidation machinery in this brain region, 53 and (c) overexpression of SNAP-25 in cultured hippocampal neurons associates with impaired synaptic transmission. 54 Altogether, these results suggest that increased SNAP-25 levels do impair synaptic maturation and/or neurotransmission. Notably, using luciferase reporter gene assays, we have analyzed the functional effect of rs363050 SNP on transcriptional activity and observed that the rs363050(A) allele associates with a significantly higher SNAP-25 expression compared to the rs363050(G) allele. 55 These data thus suggest that, in AD patients, the lower success of rehabilitation seen in the presence of the rs363050(A) allele, or of a SNAP-25 pattern in linkage disequilibrium with this allele, is the result of the higher SNAP-25 levels present in these patients.
A possible synergistic effect of SNAP-25 and ApoE polymorphisms on MST outcomes was finally evaluated, but no effects were revealed. This may be due to the fact that these genes act at different levels of neural plasticity. The promise of genomic medicine is to realize and to deliver a personalized approach to treatment of diseases that is targeted to individual genetic pattern. Analysis of the genetic background of persons with AD could become useful in guiding the clinicians to define which rehabilitative intervention might better fit each patient, for example defining a more intensive or different kind of therapy in those subjects with a lower opportunity of success. 4 The data presented here, suggesting that SNPs in ApoE and SNAP-25 correlate with the outcome of non-pharmacological treatment in AD, despite needing to be confirmed in large case studies, could help in the optimization of the clinical management of individuals with neurological conditions.
Nevertheless, given the low number of patients enrolled, the present study must be considered as a pilot research whose results will need to be confirmed and further investigated in large case studies.
Footnotes
Authors’ Note
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by 2014 Ricerca Corrente (Italian Ministry of Health and 5x1000, 2013).