
Abstract
Background. Tinnitus is a common untreatable condition that originates from central maladaptive plasticity initiated by peripheral injury. Repetitive transcranial magnetic stimulation (rTMS), direct cochlear low-level laser therapy (LLLT), and acupuncture were tried for tinnitus treatment, but the results of these methods were clinically unsatisfactory. Objective. This study aimed to test the combined effect of the 3 methods targeting both peripheral and central auditory areas as a new therapeutic strategy for tinnitus. Methods. For this, 30 patients were randomized to 3 equal groups receiving 3 different interventions: inhibitory rTMS to the left auditory cortex, LLLT (which includes a combination of direct cochlear LLLT and laser acupuncture) to the affected ear(s), and finally, a combination of rTMS and LLLT. The Tinnitus Handicap Inventory (THI) and Visual Analogue Scale (VAS) were assessed before, immediately after, and at 2 weeks and 4 weeks after 10 consecutive every-other-day sessions for each intervention type. Results. We found that combined stimulation was effective in tinnitus treatment. This effect remained for 4 weeks after the end of the treatment. However, each of rTMS and LLLT alone had no significant effect. Repeated-measures ANOVA showed a significant effect of Time and Time × Intervention interaction for THI and VAS scores. The post hoc t test for different time points per intervention revealed a significant difference between baseline and all postintervention measurements of both THI and VAS for the combination intervention. Conclusion. Combined central rTMS and peripheral LLLT is more beneficial as a new method for management of tinnitus rather than these two used separately.
Introduction
Tinnitus, an auditory phantom phenomenon of sound perception in the absence of external or internal source, 1 is a widely prevalent debilitating disease, with a worldwide prevalence of 10% to 15% in the adult population, 2 especially in elderly people, with a prevalence of 24% to 33%. 3 Tinnitus may have a severe impact on quality of life, with associated psychiatric disturbances, poor concentration, and sleep impairment. 4 In Egypt, the highest age-specific prevalence rate of tinnitus was recorded among individuals older than 60 years (around 18%), especially among urban inhabitants. 5
Tinnitus is thought to be caused by peripheral cochlear and/or auditory nerve injuries that induce central maladaptive plasticity in auditory brain areas.6,7 Moreover, functional magnetic resonance imaging studies demonstrate the involvement of several non-auditory brain areas, such as the anterior cingulate cortex, dorsal lateral prefrontal cortex, insula, supplementary motor area, orbitofrontal cortex, parahippocampus, posterior cingulate cortex, and the precuneus, in different aspects of tinnitus pathophysiology. 8
Many trials for tinnitus treatment have been published, including pharmacological and nonpharmacological approaches. Some trials with tricyclic antidepressants and benzodiazepines have shown minimal beneficial effects,9,10 but none of those drugs was approved by the Food and Drug Administration for tinnitus treatment.1,10 The difficulty of finding satisfactory pharmacotherapy for tinnitus has pushed researchers to test other nonpharmacological approaches, such as various neuromodulation methods. 11
Repetitive transcranial magnetic stimulation (rTMS) is a noninvasive brain stimulation technique based on the electromagnetic induction principle and can induce changes in the cortical excitability that outlasts the stimulation period itself. 12 Depending on the frequency, rTMS can induce long-term potentiation and long-term depression-like change of cortical excitability if applied at high (≥5 Hz) or low (≤1 Hz) frequency. 13
Many clinical trials have shown that low-frequency (1 Hz) rTMS to the left temporoparietal cortex is effective in the treatment of tinnitus.14,15 However, other trials have found it to be no more effective than placebo.16-19 Moreover, during the past decade, direct cochlear low-level laser therapy (LLLT) for the treatment of tinnitus has shown controversial success rates, because some authors have reported a significant reduction in tinnitus parameters.20-22 In other studies, this effect was supposed to be placebo induced.23-25
Acupuncture has been used for a long time to treat tinnitus. Neuroscience studies related the effects of acupuncture to neuronal stimulation, activation of endogenous opioid mechanisms, and neuropeptides that stimulate specific brain structures. 26 Laser acupuncture as an alternative to manual acupuncture has considerable practical relevance, because it permits the stimulation of acupoints in a precisely defined manner.27,28 The same contradictory results seen with direct cochlear LLLT apply to the effect of acupuncture on tinnitus suppression. 29 Two out of 7 trials showed a positive effect of acupuncture for the treatment of tinnitus. 29
In previous studies, both laser acupuncture and direct cochlear LLLT led to the activation of cortical areas that may play an important role in the development and consolidation of tinnitus in healthy individuals.27,28,30 Accordingly, adding laser acupuncture and direct cochlear LLLT to rTMS might help in controlling other brain regions implicated in tinnitus generation that cannot be accessed by rTMS alone.
To the best of our knowledge, a few studies have targeted both peripheral (cochlea and auditory nerve) and central areas implicated in tinnitus pathophysiology. 31 However, these studies did not combine laser acupuncture and direct cochlear LLLT with rTMS for the treatment of tinnitus. We hypothesized that the combination of peripheral LLLT treatment (combined laser acupuncture and direct cochlear LLLT) with central rTMS treatment may achieve better effects as a new therapeutic strategy for tinnitus.
Materials and Methods
A total of 30 chronic tinnitus patients participated in this study (Table 1). These patients were recruited from outpatient clinics of neurology and otolaryngology in Sohag University Hospital. All patients gave written informed consent for participation in the study. The study protocol was approved by the local ethics committee of Sohag University.
Patient Data. a
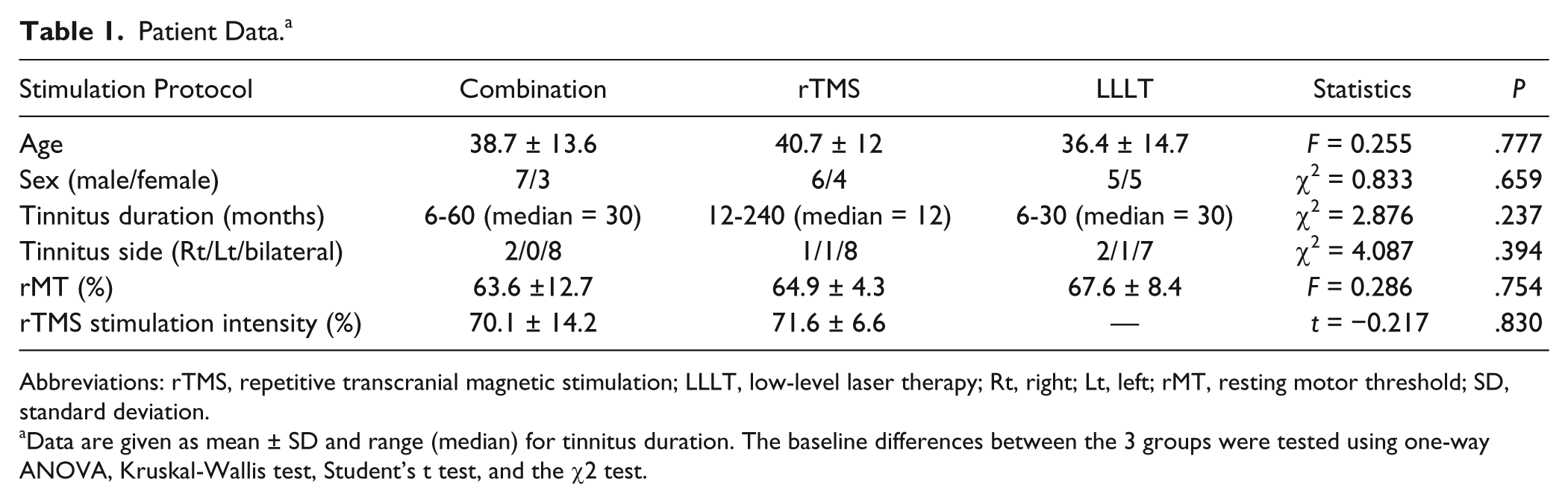
Abbreviations: rTMS, repetitive transcranial magnetic stimulation; LLLT, low-level laser therapy; Rt, right; Lt, left; rMT, resting motor threshold; SD, standard deviation.
Data are given as mean ± SD and range (median) for tinnitus duration. The baseline differences between the 3 groups were tested using one-way ANOVA, Kruskal-Wallis test, Student’s t test, and the χ2 test.
All patients were aged >18 years old, and all of them suffered from subjective unilateral or bilateral, nonpulsatile, chronic tinnitus (of at least 6 months’ duration) with normal neurological examination. Detailed medical history and examination, pure tone audiometry, otoscopy, and tinnitus scorings were performed for all patients by an otolaryngologist who was not directly involved in therapeutic interventions. Patients excluded from the study were those who complained of neurological diseases that increase the risk of seizures during rTMS treatment, including epilepsy, brain tumors, strokes, previous cranial surgeries, head trauma, and encephalitis, and patients who suffered from migraine or who were under current treatment with psychoactive drugs, including antidepressants, antiepileptics, neuroleptics, or who had implanted intracranial devices or cardiac pacemakers. Table 1 shows the various demographic and baseline data for the patients. Figure 1 shows an average audiogram of the patients in each group.
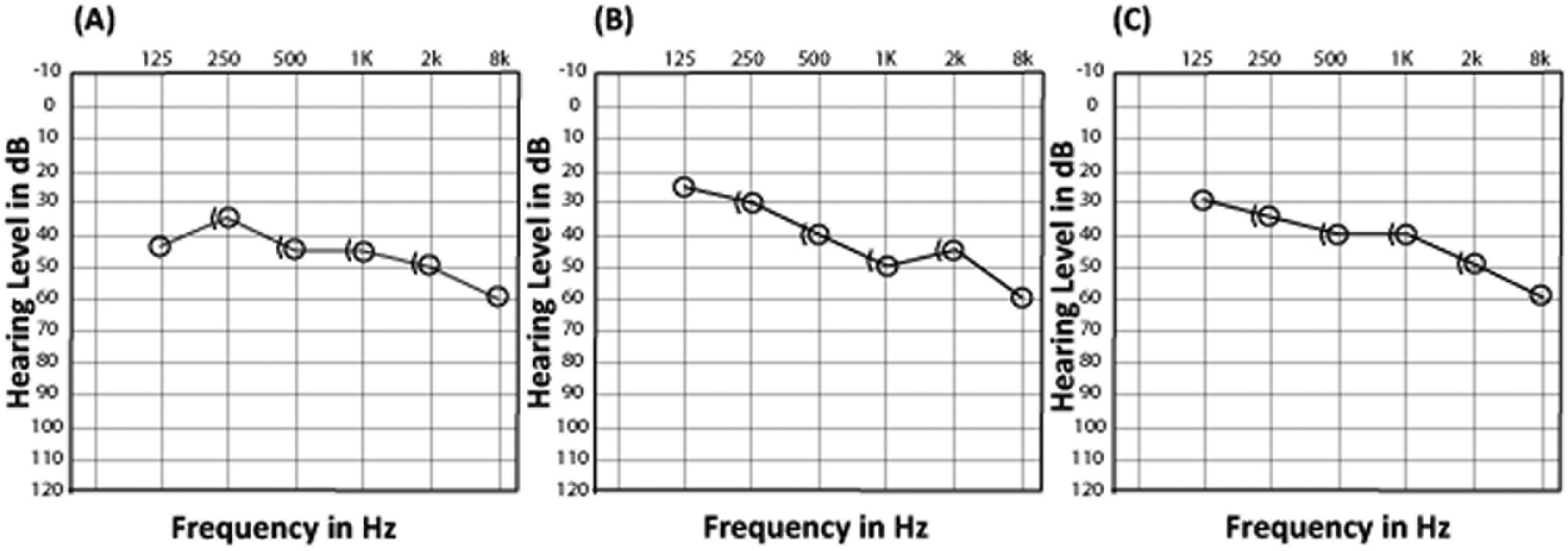
Mean audiogram levels for the affected ear (unilateral cases) and the more severe ear (bilateral cases) for the 3 groups of patients. A. Mean audiogram values for the combination intervention group. B. Mean audiogram values for the rTMS-only group. C. Mean audiogram values for the LLLT-only group.
Study Design
Patients were stratified into 3 groups using the blocked randomization method according to age and the Tinnitus Handicap Inventory (THI) scores. A block size of 6 was used, and SPSS version 16 was used to generate a random sequence of numbers. One group received combined rTMS and LLLT (n = 10), the second group received rTMS treatment alone (n = 10), and the third group received LLLT treatment alone (n = 10). The investigator who analyzed the outcome measures was blinded to the type of intervention. Moreover, the outcome measurements used in this study were self-reported scales. The patients in each group were blinded to the methods used in the other 2 groups (Figure 2).
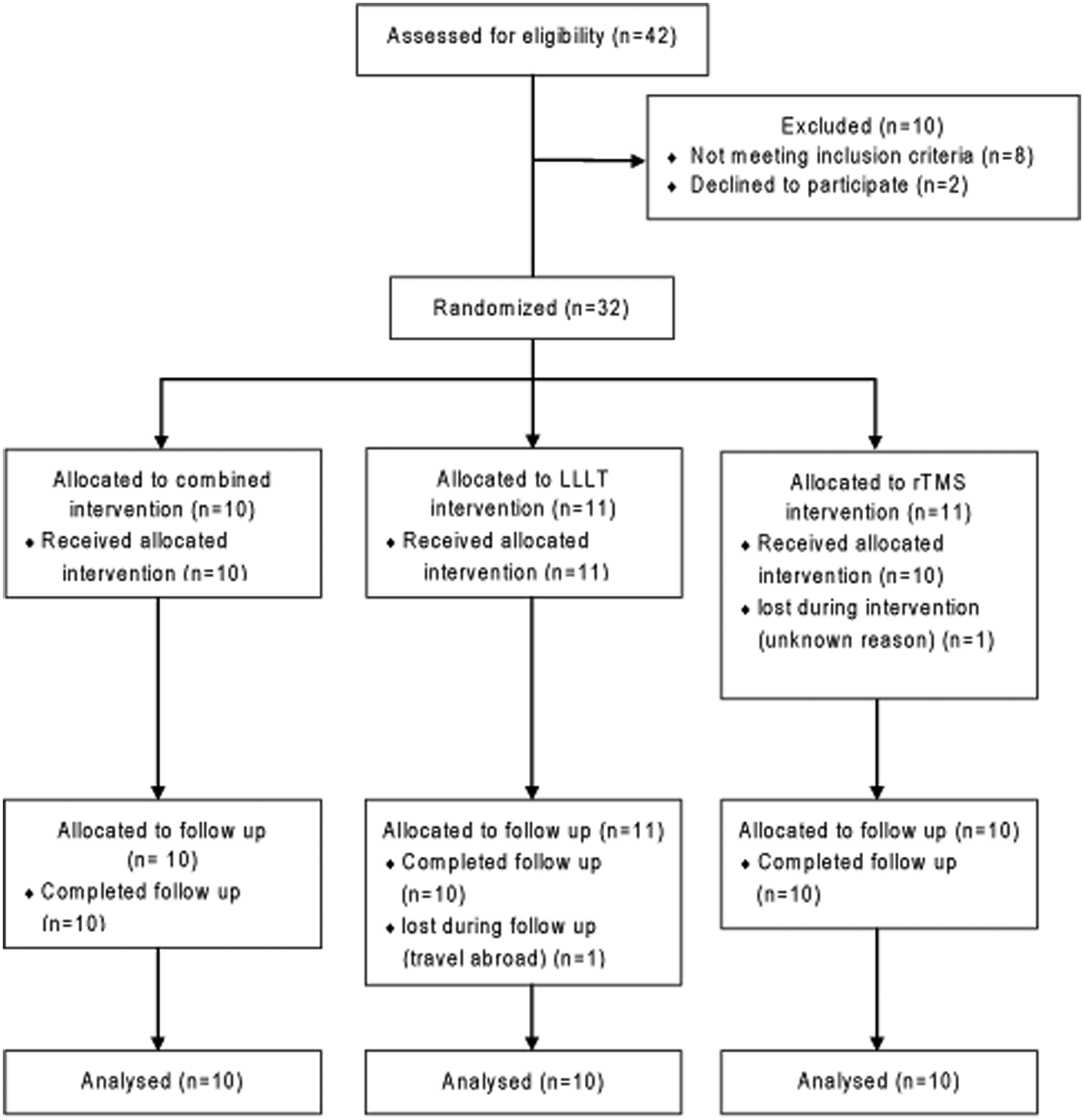
Patient flowchart.
An Arabic validated version of the THI, which consists of a 25-item questionnaire, and a Visual Analogue Scale (VAS) ranging from 0 to 100, where 0 means no tinnitus and 100 means the worst possible tinnitus-related discomfort, were taken as outcome measurements for the effect of various interventions. Both outcome measurements were taken before (baseline), immediately after (post-0), 2 weeks after (post-2), and 4 weeks after (post-4) the end of various interventions. The therapeutic interventions were applied as 10 treatment sessions every other day, excluding Fridays, for a period of 21 days.
Therapeutic Interventions
Three therapeutic interventions were used in this study. The first was the combined intervention composed of separate sequential rTMS and LLLT stimulations in the same treatment session. The next 2 were separate rTMS and LLLT interventions in which each patient received a single type of therapeutic stimulation per treatment session.
For rTMS, a figure-of-eight coil (9 cm for the outer diameter) connected to a Magstim Super Rapid stimulator (Magstim Co, Ltd) was used. Each participant was seated comfortably on an armchair, with the arms placed on the armrest and the hands facing upward. A surface electromyogram was recorded from the right abductor pollicis brevis on the right hand using pairs of silver electrodes. The optimal motor point for eliciting the best motor-evoked potential was established by a suprathreshold stimulus over the left primary motor cortex. The resting motor threshold was determined as the minimal stimulus intensity that induces a motor-evoked potential of at least 50 µV in the right abductor pollicis brevis in 5 out of 10 stimulations. 32
In each session, 2000 rTMS pulses of 110% resting motor threshold stimulus intensity and 1 Hz stimulation rate were given to the left temporoparietal cortex regardless of the handedness and tinnitus laterality. The coil was positioned over the left temporoparietal cortex by moving 2.5 cm upward from T3 on a line from T3 to Cz and then 1.5 cm posteriorly perpendicular to that line.33,34 The handle of the coil was directed upward and held with a mechanical arm. Accordingly, the induced current in the brain was directed approximately perpendicular to the location of the superior temporal gyrus. Although the location of the auditory cortices is highly variable, 35 the primary auditory cortex and much of the secondary auditory cortex are located in the superior temporal gyrus. 36 All patients used ear plugs for hearing protection during the intervention.
A Polaris 2 device (Astar Physiotechnology, Co) with a single diode probe was used to produce laser light (200 mW, 5 Hz, and 808 nm) for LLLT treatment. The laser light was applied to 5 locations: the external auditory meatus for direct cochlear LLLT and the following 4 acupuncture points that are related to hearing disorders: the highest point in the depression between the angle of the mandible and mastoid bone (S.J 17 Chinese map of acupuncture points), the temperomandibular joint when the mouth is slightly opened (S.I. 19), the depression in front of the supratargic notch (S.J. 21), and above the auricle (S.J. 20), for laser acupuncture. The external auditory meatus and first 2 acupuncture points (S.J. 17 and S.I. 19) were irradiated with a total energy of 40 J/cm2. This total energy was supplied as 10 sequential stimulations for each point. Each of these 10 stimulations gives energy of 4 J/cm2 and lasts 26 s, and the total duration of the 10 stimulations was 260 s for each point. Each of the last 2 points (S.J. 20 and S.J. 21) was irradiated with a total energy of a single shot of 4 J/cm2 for 26 s. The laser light frequency used for external auditory meatus and all acupuncture points was intentionally low (5 Hz, pulse width of 75%) because lower frequencies are absorbed better than higher ones at acupuncture points.
Statistical Analysis
Repeated-measures analysis of variance (ANOVA) was used for analysis of THI and VAS scores. Greenhouse-Geisser was used for adjustment of sphericity if needed. A two-tailed paired t test with Bonferroni correction was used for post hoc analysis. Demographic variables and baseline clinical characteristics between groups were compared using one-way ANOVA and Kruskal-Wallis, χ2, and Student’s t tests. The results were considered significant if P <.05. SPSS version 16 was used for statistical analyses. If not mentioned otherwise, data are given as mean ± standard error of the mean.
Results
Table 1 presents the demographic and baseline data of patients who participated in the study. There were no significant differences in the baseline characteristics of patients between the 3 groups of different interventions. All patients tolerated the 3 types of interventions without serious adverse effects. Most of the patients who received rTMS either alone or in combination with LLLT reported facial muscular twitches and mild headache at the site of coil position.
Tables 2 and 3 present the data for THI and VAS, respectively, for all groups. These data were found to be normally distributed based on the Shapiro-Wilk test. The baseline differences between groups regarding THI and VAS were insignificant (F = 0.019, P = .982, and F = 0.024, P = .976, respectively). For THI results, Figure 3 shows a 50% reduction of THI immediately after the end of the combined intervention. As shown in Table 2, the mean THI was 66.6 before the intervention and 33.3 after the intervention. Repeated-measures ANOVA with Time as the within-subject factor and Intervention as the between-subject factor revealed a significant main effect of Time (F = 26.415; P < .0001) and an insignificant main effect of Intervention (F = 2.677; P = .087). This effect of time (THI decreased with time) was dependent on the type of intervention because there was a significant Time × Intervention interaction (F = 5.441; P = .003). Post hoc t tests with Bonferroni correction of α error for each time point per intervention revealed significant differences between baseline and post-0 (P < .0001), between baseline and post-2 (P < .0001), and between baseline and post-4 (P = .004) for the combination intervention only (Figure 3). There was a clear tendency for improvement of THI because there was a reduction in the mean baseline THI by 10 and 6 points immediately after, by 12 and 8 points 2 weeks after, and finally, by 11 and 6 points 4 weeks after the end of the intervention for rTMS and LLLT, respectively (Table 2). According to earlier studies, 37 a THI score reduction of >10 points was considered a clinically effective “responder.” For combination, rTMS-only, and LLLT-only interventions, the percentages of responders were 80%, 20%, and 30%, respectively.
THI Values for the Different Interventions. a
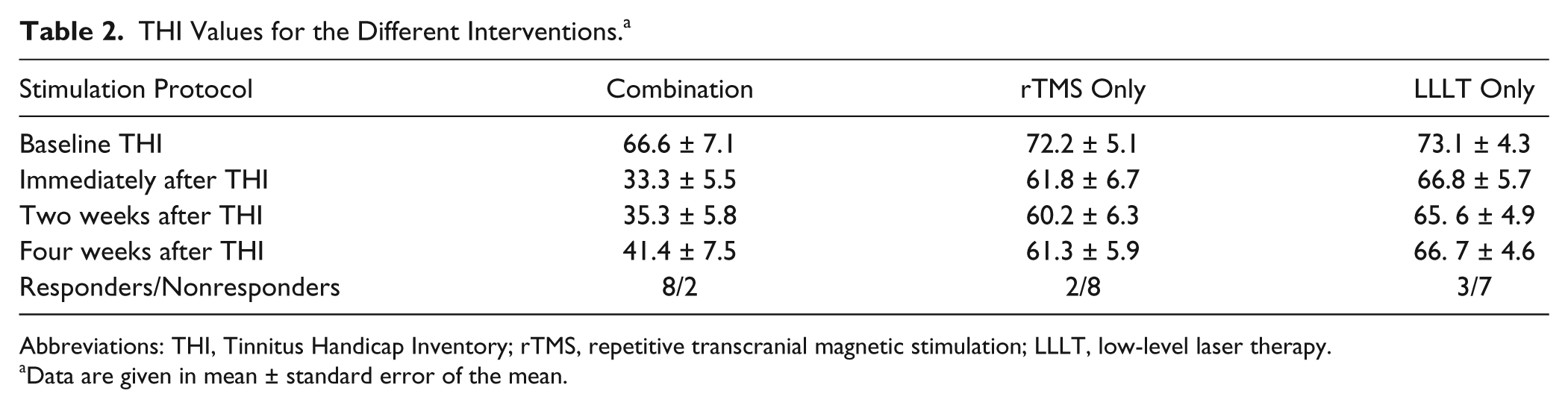
Abbreviations: THI, Tinnitus Handicap Inventory; rTMS, repetitive transcranial magnetic stimulation; LLLT, low-level laser therapy.
Data are given in mean ± standard error of the mean.
VAS Values for the Different Interventions. a
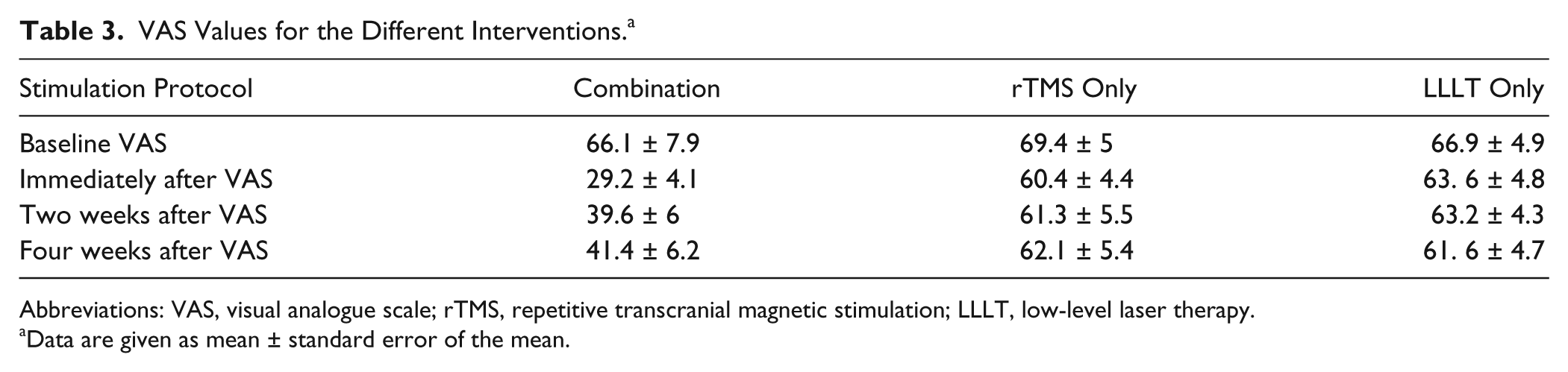
Abbreviations: VAS, visual analogue scale; rTMS, repetitive transcranial magnetic stimulation; LLLT, low-level laser therapy.
Data are given as mean ± standard error of the mean.
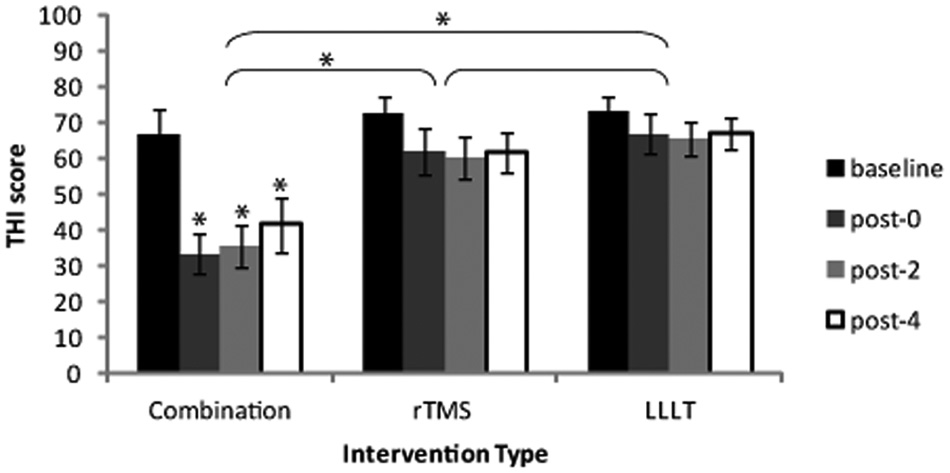
The THI for the various interventions showing a significant reduction in the THI values for the combination intervention group compared with the LLLT- and the rTMS-only groups. There is no significant difference between both the LLLT and the rTMS groups. The significant reduction in THI scores for the combination intervention group remained up to 4 weeks after the end of treatment (*P < .05).
For VAS results, Figure 4 shows a 56% reduction in the mean VAS score after the end of the combination intervention. As shown in Table 3, the mean VAS score was 66.1 before the intervention and 29.2 after the intervention. Repeated-measures ANOVA taking Time and Intervention as within- and between-subject factors, respectively, revealed a significant main effect of Time and Intervention (F = 26.48, P < .0001, and F = 4.982, P = .014, respectively). There was also a significant Time × Intervention interaction (F = 9.878, P < .0001). Post hoc t tests with Bonferroni correction of the α error for different time points per intervention revealed significant differences between baseline and post-0 (P < .0001), between baseline and post-2 (P = .002), and between baseline and post-4 (P = .009) for the combination intervention. For the LLLT intervention, post hoc testing revealed significant differences between baseline and post-0 and between baseline and post-4 (P = .024 and P = .023, respectively; Figure 4).
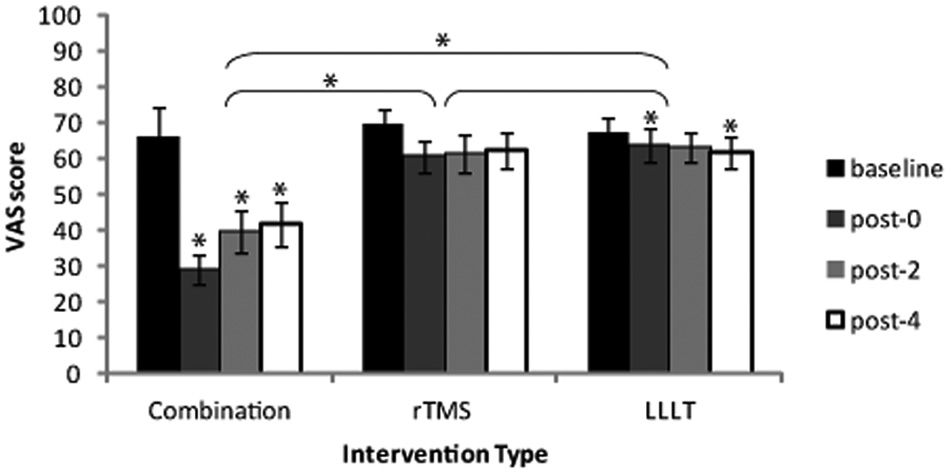
The VAS for the 3 interventions showing significant reduction of VAS values for the combination intervention group compared with the LLLT- and the rTMS-only groups. There is no significant difference between both the LLLT and the rTMS groups. The significant reduction in VAS scores for the combination intervention group remained up to 4 weeks after the end of treatment. There was significant change in the VAS score for the LLLT intervention group (*P < .05).
The significant effect of the combination intervention on THI was not related to tinnitus duration and severity. Regression analyses for the reduction in THI scores immediately after the intervention (post-0) and tinnitus duration and baseline THI as a measure of tinnitus severity were insignificant (β = 0.426, P = .208, and R2 = 0.089, and β = 0.625, P = .053, and R2 = 0.314, respectively). Although in our study THI reduction seems to increase in patients with high baseline THI, this change is not statistically significant. Moreover, there was no significant relation between change in THI scores and degree of hearing loss (F = 0.989, P = .418).
Discussion
To the best of our knowledge, this is the first study to combine peripheral LLLT and central rTMS stimulation for the treatment of chronic tinnitus. We found that a combination of both types of neural stimulations is a much more powerful noninvasive and safe method of treatment compared with the use of either stimulation alone.
Several imaging studies showed activation of multiple cortical and subcortical, auditory, and affective brain regions, including the temporoparietal cortex, during tinnitus perception.38,39 Tinnitus, which often results from an insult to the peripheral auditory system, is associated with changes in the structure and function of many brain regions. These regions include multiple levels of the auditory system as well as other parts of the limbic system involved in memory and emotions. Given the broad extent of brain regions affected, it is unlikely that a single drug or treatment modality can effectively reduce or eliminate tinnitus. A multidisciplinary approach for the management of tinnitus is clearly needed. 6
In tinnitus patients, damage to the hair cells or fibers of the auditory nerve produced by acoustic trauma or ototoxic drugs reduces the sensorineural cochlear input to central auditory centers. In turn, this increases the spontaneous firing rate and the synchrony of firing of the neurons in these central auditory centers in an attempt to compensate for this reduced input. These central auditory centers include cochlear nuclei, inferior colliculus, and primary and secondary auditory cortices.40,41 Moreover, intracortical inhibition is thought to be diminished in chronic tinnitus because of this peripheral deafferentation as a result of receptor damage.6,7,41,42 Tinnitus-related hyperactivity in central auditory centers seems to be linked to downregulation of cellular inhibitory activity. 43 A recent in vitro study confirmed that a downregulation of GABAergic inhibition is responsible for the development of hyperactivity in the dorsal cochlear nucleus in mice with behavioral evidence of tinnitus. 44
Inhibitory low-frequency rTMS, which is known to induce a long-term depression-like decrease in cortical excitability, 13 has been successfully used to interfere with the neural function in the temporoparietal cortical regions to transiently suppress tinnitus.45,46 Low-frequency (1 Hz) rTMS is known to induce intracortical inhibition in the motor cortex, as measured through paired pulse stimulation, especially in those with low baseline intracortical inhibition, as in tinnitus patients. 47 Moreover, 1-Hz rTMS increases the duration of the cortical silent period, which is another inhibitory cortical function. 47 Accordingly, low-frequency rTMS has often been used for the treatment of tinnitus.
This study is in agreement with previous studies that support the beneficial effect of low-frequency rTMS on the left temporoparietal cortex in symptomatic relief of tinnitus.15,33,46,48-54 However, after a careful analysis of the results from the previously mentioned studies, it seems that the clinical benefit of rTMS in the treatment of tinnitus, although statistically significant, is minimal, with small effect size and many nonresponding patients.15,37,49,50,55 Moreover, several studies have concluded that rTMS treatment is not more effective than placebo in the treatment of tinnitus.16-18 There could be several reasons for the lack of response in some patients and/or studies. Some neuroimaging studies have shown deeply situated loci of tinnitus-related cortical hyperactivity, which means that rTMS treatment may be unable to access the whole neural circuit involved in tinnitus pathophysiology. 50 Another reason may be the large between-subject variability in the response to rTMS as documented in the motor cortex. 56 Moreover, the tinnitus-related neural network varies in different patients and may be related to tinnitus duration. 57 Differences in treatment site, duration of stimulation, efficacy of and/or presence of sham stimulation, and patient selection may be additional factors that play a role in the variability of response among different studies. 15
This limited clinical response of rTMS in the treatment of tinnitus has pushed many researchers to augment the effect of rTMS by means of accurate targeting of tinnitus-related auditory cortical sites using functional imaging guided rTMS stimulation 54 and through various combined protocols of targeting auditory and nonauditory cortical sites. 37 Other trials to treat tinnitus by using a combined approach have been tried, such as combined counseling using hypnosis and muscle relaxation techniques and LLLT 58 ; EGb 761 (Ginkgo biloba extract EGb 761, Rökan, Tanakan, Tebonin), which is a standardized extract of Ginkgo biloba leaves and has antioxidant properties as a free radical scavenger combined with LLLT 20 ; tinnitus retraining therapy combined with cognitive behavioral therapy 59 ; tinnitus masking therapy combined with counseling 60 ; and finally, various drug combinations such as carbamazepine and flunarizine, and betahistine and flunarizine, 61 all with variable results. However, none of these noninvasive brain stimulation techniques to achieve better treatment effects target the peripheral areas (the cochlea and auditory nerve), which are thought to be the origin of the central maladaptive plasticity.
Many clinical trials have used direct cochlear LLLT for the treatment of tinnitus, with documented but controversial clinical benefits. Some trials have shown a significant effect in the treatment of tinnitus even if with small effect size in humans21,22,24,58 and in animals. 62 However, other studies deny any significant effect of direct cochlear LLLT for relief of tinnitus and explain the results of positive studies by a placebo effect.23,63,64 Other methods targeting the peripheral auditory pathway for treatment of tinnitus include acupuncture. The evidence for the effect of acupuncture treatment of tinnitus is mixed. 29 Some studies show a positive effect, 65 whereas others do not. 66 A significant effect of acupuncture for treatment of tinnitus was based on traditional Chinese medicine, and its benefit was not totally agreed on because there were some studies that showed an insignificant effect. 29 Accordingly, we combined both methods in one step by stimulation of external auditory meatus for cochlear irradiation and some other ear-disorder-related acupuncture points by LLLT (peripheral LLLT) as a trial for a more effective peripheral stimulation method for the treatment of tinnitus.
Imaging studies have shown that direct cochlear LLLT induces thalamo-limbic-fronto-parietal network activation. 30 This corresponds well to the tinnitus-related brain network. 8 Moreover, there are many clinical benefits of LLLT because it has been proved to be effective in wound healing, tissue repair, musculoskeletal complications, and pain control. LLLT increases cell proliferation and collagen synthesis, prevents neuronal degeneration, promotes improved neuronal function and repair, and enhances neural growth.21,67 These beneficial effects of LLLT may be related to its biophysiological rather than thermal effects because it was proved that LLLT is absorbed primarily by neuronal mitochondria, leading to the release of H+ ions that suppress the Na+ and K+ channels, which in turn leads to a reduction of aberrant nerve action potentials generated in tinnitus patients. 21 Another beneficial biophysiological effect of LLLT is its ability to increase ATP synthesis, increase release of growth factors, and increase blood supply and improvement of microcirculation in irradiated regions. 67 Accordingly, LLLT may have beneficial effects on the health of neural tissues by preventing neuronal degeneration, improving neuronal function and repair, and enhancing neural growth. 68 As one of the diseases that may be related to damage of inner ear neuronal tissues, tinnitus might be one of the target conditions for treatment using LLLT.
According to the theory of traditional Chinese medicine, acupuncture points can be stimulated (needle or electrical or laser stimulation) to treat a disease. 69 The rationale for using acupuncture is the principle that acupoint stimulation may elicit an electrical charge that triggers action potentials to rebalance neurophysiological systems. 29 In animal and human studies, acupoint stimulation led to neurohumoral changes and modification in neurotransmitters released in the central nervous system. Moreover, functional imaging studies have revealed that laser acupuncture can induce specific brain area activation that might have a role in mediating its beneficial effects.27,28,70 Moreover, acupuncture treatment rebalances the function of the olivocochlear nucleus. 71 Neuroscience studies reveal that the effect of acupuncture is not only related to neuronal stimulation but also to the activation of endogenous opioid mechanisms and neuropeptides that stimulate specific brain structures.72,73
The controversial effect of each of rTMS, direct cochlear LLLT, and acupuncture in the treatment of tinnitus might be related to the inability of each method alone to fully target the disordered central and peripheral parts of the auditory pathway. A possible explanation of the improved effect seen when combining the 2 approaches as proposed by our study might be the triple targeting effect: the proinhibitory effect of low-frequency rTMS stimulation targeting the malfunctioning auditory cortex, the direct cochlear LLLT targeting the disordered cochlea and central brain circuits involved in tinnitus, and finally the laser acupuncture targeting the olivocochlear nucleus brainstem and other cortical circuits related to tinnitus.
One of the limitations of our study is the small sample size, which makes the results prone to type II error, with exaggeration of the treatment effects, in addition to the lack of placebo groups. However, this study is considered to be a pilot study.
In conclusion, this combined approach may be a much better as well as a safe and easy option for treating tinnitus patients with probable multiple mechanisms of action. Other large-scale controlled clinical trials are needed to optimize this procedure and find a uniform protocol that can be generalized for use in tinnitus patients.
Footnotes
Acknowledgements
This research was accepted and won a travel award for the 36th annual meeting of the Japan Neuroscience Society that was held in June 2013 in Kyoto, Japan. We also thank Dr Tatsuya Mima, Associate Professor, Human Brain Research Center, Kyoto Graduate School of Medicine, Kyoto University, Japan, for his greatly valuable comments and advice regarding this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.