
Abstract
Background. The growing social emergency represented by Alzheimer’s disease (AD) and the lack of medical treatments able to modify the disease course have kindled the interest in nonpharmacological therapies. Objective. We introduced a novel nonpharmacological approach for people with AD (PWA) named Multidimensional Stimulation group Therapy (MST) to improve PWA condition in different disease domains: cognition, behavior, and motor functioning. Methods. Enrolling 60 PWA in a mild to moderate stage of the disease, we evaluated the efficacy of MST with a randomized-controlled study. Neuropsychological and neurobehavioral measures and functional magnetic resonance imaging (fMRI) data were considered as outcome measures. Results. The following significant intervention-related changes were observed: reduction in Neuropsychiatric Inventory scale score, improvement in language and memory subscales of Alzheimer’s Disease Assessment Scale–Cognitive subscale, and increased fMRI activations in temporal brain areas, right insular cortex, and thalamus. Conclusions. Cognitive-behavioral and fMRI results support the notion that MST has significant effects in improving PWA cognitive-behavioral status by restoring neural functioning.
Keywords
Introduction
Alzheimer’s disease (AD) is a neurodegenerative disorder affecting multiple clinical domains involving cognitive functioning, behavioral aspects, and functional-physical skills. 1 In the past 15 years, the growing social emergency represented by AD and the lack of medical treatments able to modify the disease course have kindled the interest in nonpharmacological therapies. This term, often used to describe the array of approaches and techniques proposed in the literature, spans several domains (cognitive-oriented therapies, physical medicine, etc). Another term used to indicate these kinds of approaches is psychosocial therapies, but this word seems to exclude the possibility that these therapies can modify brain function or structure. Hence, some authors have proposed modified versions such as biopsycosocial or psychobiosocial therapies.2,3 Functional magnetic resonance imaging (fMRI), due to its capacity to monitor neural circuits reorganization, has been recently introduced to evaluate the efficacy of these nonpharmacological treatments (see Cramer et al 4 for a review), also including treatments for amnestic mild cognitive impairment (MCI) 5 and AD. 6
Cognitive stimulation (CS) is probably the most widespread and well-studied technique in this field, but it is still a matter of debate whether this therapy is able to slow down the disease course. 7 The most defined form is cognitive stimulation therapy (CST), which incorporates the positive aspects of reality orientation therapy but avoids putting the person with dementia in stressful situations and implements stimulation in a respectful and person-centered manner. 8 In 2003, Spector and colleagues 9 showed that this approach was at least as effective as cholinesterase inhibitors to reduce cognitive decline. On the basis of this work, the 2006 NICE guidelines concluded that this intervention should be routinely proposed to people with mild to moderate dementia. 10 Recently, a maintenance protocol with CST was developed with a very precise procedure that involved not only professionals but also people with dementia and their caregivers. 11 It seems that CST was able to change some aspects of cognition, especially those related to language and memory, more than others.12,13 In a Cochrane review on CS, 14 the authors found a consistent benefit on cognitive function that persisted at follow-up 1 to 3 months after the end of the treatment. In secondary analyses with smaller total sample sizes, improvements were also observed on self-reported quality of life and well-being.
In the past years, further nonpharmacological therapy studies have allowed for firmer conclusions to be drawn on their efficacy. Occupational and recreational therapy, for example, can reduce psychobehavioral disturbances of people with dementia, increase their participation, improve their quality of life, reduce negative communication, extend the caregiver sense of competence, and reduce his/her burden.15,16 Moreover, exercise has been shown to improve the physical health and the well-being of people with dementia 17 and appeared to be beneficial in reducing behavioral and psychological symptoms of dementia (BPSD). 18 Interestingly, aerobic exercise training in adults seems to promote an improvement in spatial memory and to reverse age-related loss in volume by 1 to 2 years. 19 In Belgium and the Netherlands, psychomotor therapy has been well integrated into mental health care since 1965. 20
Based on this growth of evidence, some research groups have therefore decided to propose multidimensional protocols of treatment for people with AD (PWA), based on the hypothesis that this type of approach would be the most suitable to improve their condition in different disease domains: cognition, behavior, and motor functioning. This kind of therapy would be also the most appropriate for the unique profile of each person with AD, even when performed in small groups.21,22 In the past 13 years, our group has developed a multidimensional approach—Multidimensional Stimulation Therapy (MST). Our previous findings23-25 support the notion that this group activity program, based on cognitive stimulation, recreational-occupational activities, and physical-psychomotor exercises, can lead to an improvement in behavioral aspects for PWA.
In this article, we describe a randomized single-blind trial aimed to clarify the efficacy of an MST program in outpatients affected by AD in mild to moderate stages of the disease. We also included fMRI as a surrogate marker of treatment efficacy.
Methods
Participants
Sixty participants were consecutively recruited from the Don Gnocchi Foundation Memory Clinic.
Outpatients eligibility criteria were the following: (a) diagnosis of probable AD according to NINCDS-ADRDA criteria 1 ; (b) evidence of AD pathophysiological processes detected with structural MRI as a biomarker of neural injury 1 ; (c) mild to moderate stage of AD (Mini-Mental State Examination (MMSE) score of 15-24 [see Magni et al 26 ] and Clinical Dementia Rating scale score of 1-2 [see Hughes et al 27 ]); (d) age range 65 to 85 years and school attendance range 5 to 17 years; (e) right handedness as assessed by the Edinburgh inventory. 28 PWA were excluded if they had (a) severe aphasia (Token test score < 20 [see Spinnler and Tognoni 29 ]) or severe auditory and/or visual loss; (b) overt severe behavioral disturbances that could hinder the MST session; and (c) recent (3 months before the MST) introduction or dose modification of the following pharmacological treatments: cholinesterase inhibitor, memantine, antidepressant, or antipsychotic drugs. Low-dose benzodiazepines for insomnia were allowed during the study.
Each patient had a caregiver who supervised treatment compliance.
Demographic, neuropsychological, and anatomical details are shown in Table 1.
Baseline Demographics, Neuropsychological, and Anatomical Characteristics.
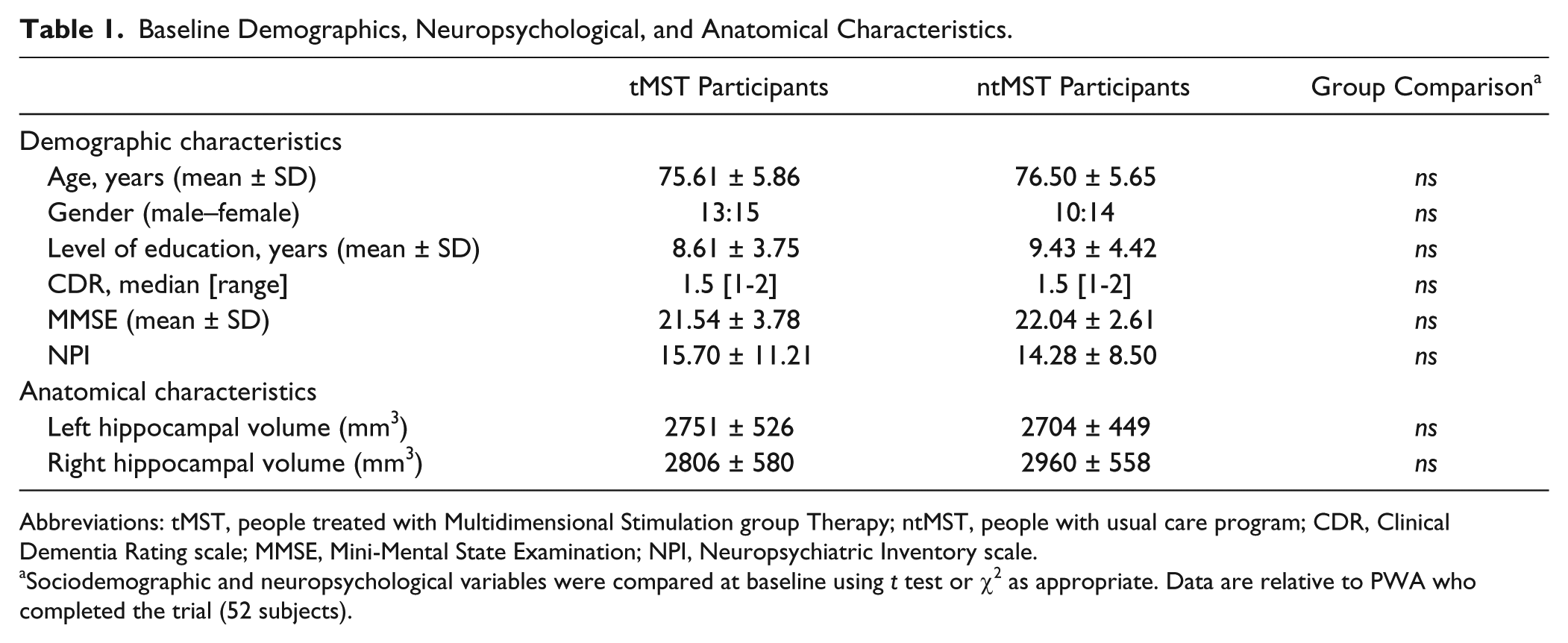
Abbreviations: tMST, people treated with Multidimensional Stimulation group Therapy; ntMST, people with usual care program; CDR, Clinical Dementia Rating scale; MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory scale.
Sociodemographic and neuropsychological variables were compared at baseline using t test or χ2 as appropriate. Data are relative to PWA who completed the trial (52 subjects).
According to a previous multicenter controlled study, 25 sample size calculation was performed considering an effect size of 1.7 and a standard deviation of 2.8 of primary outcomes differences between groups. Under the assumption of normal distribution of the scores and considering an α level of .05, a sample size of 30 subjects resulted in a power greater than 70% and was thus believed to be adequate for this trial.
Moreover, 22 healthy controls (HC) who were age-matched and sex-matched to the PWA (73.2 ± 5.1 years; 8 males/14 females; MMSE score >28) were also included in the fMRI analysis for the description of the typical activation pattern and for the definition of regions of interest to be used for the analyses on PWA data.
The study was approved by the Ethics Committee of Don Gnocchi Foundation, and informed written consent was obtained from all the included subjects and their caregivers (or a legally acceptable representative if applicable and if different from the caregiver) before study initiation.
The trial was registered at www.clinicaltrials.gov (NCT01893398).
Randomization and Masking
The target population was stratified by gender and randomly assigned (1:1 ratio) to MST (tMST) or a usual care program (no stimulation treatment, ntMST) in a single-blind parallel-group study. Randomization was conducted by an independent operator, who was not involved in assessment and treatment using a computer algorithm (http://graphpad.com). Participants and their caregivers were instructed not to discuss the nature of their therapy with the research assistants who did the assessments. Outcome measures were collected by researchers blinded to group allocation.
Intervention
The MST program involved 3 levels of treatment. The first level was focused on PWA, the second level involved the caregiver, whereas the third one included the dyad PWA–caregiver.
Level 1—PWA
The PWA performed 30 rehabilitation sessions (2.5 hours a day, 3 days a week) in a room with a kitchen area, table and chairs, and materials necessary to carry out recreational–occupational activities. MST was administered by a psychologist and a rehabilitation therapist, both specialized in cognitive rehabilitation. Tight interaction between participants and therapists was an essential feature of our program: as previously noted, 30 an attractive environment or the mere presence of the staff is insufficient to evoke in PWA the exercise of their full functional capacities. The treatment involved 4 steps: (a) Reality Orientation activities and cognitive exercises (about 45-minute); (b) physical activity (about 30-minute); (c) occupational activities of daily living (about 30-minute); (d) recreational activities (about 45- minute).
Level 2—Caregiver
All caregivers of PWA had a single support interview with a psychologist at the beginning and at the end of the training. In these moments, family caregivers could freely express their psychological sufferance and their practical difficulties. Caregivers also followed a standardized short group educational program with a rehabilitation therapist. The program touched on several points: AD clinical picture, pathogenetic mechanism, pharmacological therapy and recent advances in research, coping with behavioral problems, as well as legal and social aspects. The second level was offered (a) to collect data about past preferences and personality of the PWA in order to integrate this information into the rehabilitation program; (b) to offer psychological support to the caregiver; and (c) to promote the detection of practical coping solutions. Moreover, during psychoeducational meetings, caregivers were trained by the therapist in order to continue the treatment at home (see Level 3).
Level 3—Dyad PWA and Caregiver
All subjects performed further stimulation at home: aerobic physical activity and specific but simple cognitive activities every day. Level 3 was introduced to improve in the amount and intensity of the MST treatment and to favor a positive PWA–caregiver interaction at home (eg, strategies of practical coping solutions).
Procedures
As shown in timeline (Figure 1), assessments were done in both groups at baseline (T_0) and after 10 weeks (T_1). Only in the tMST group a follow-up evaluation was collected after 22 weeks, because the ntMST group was treated with MST for ethical purposes in accordance with the recommendations of the local ethics committee.
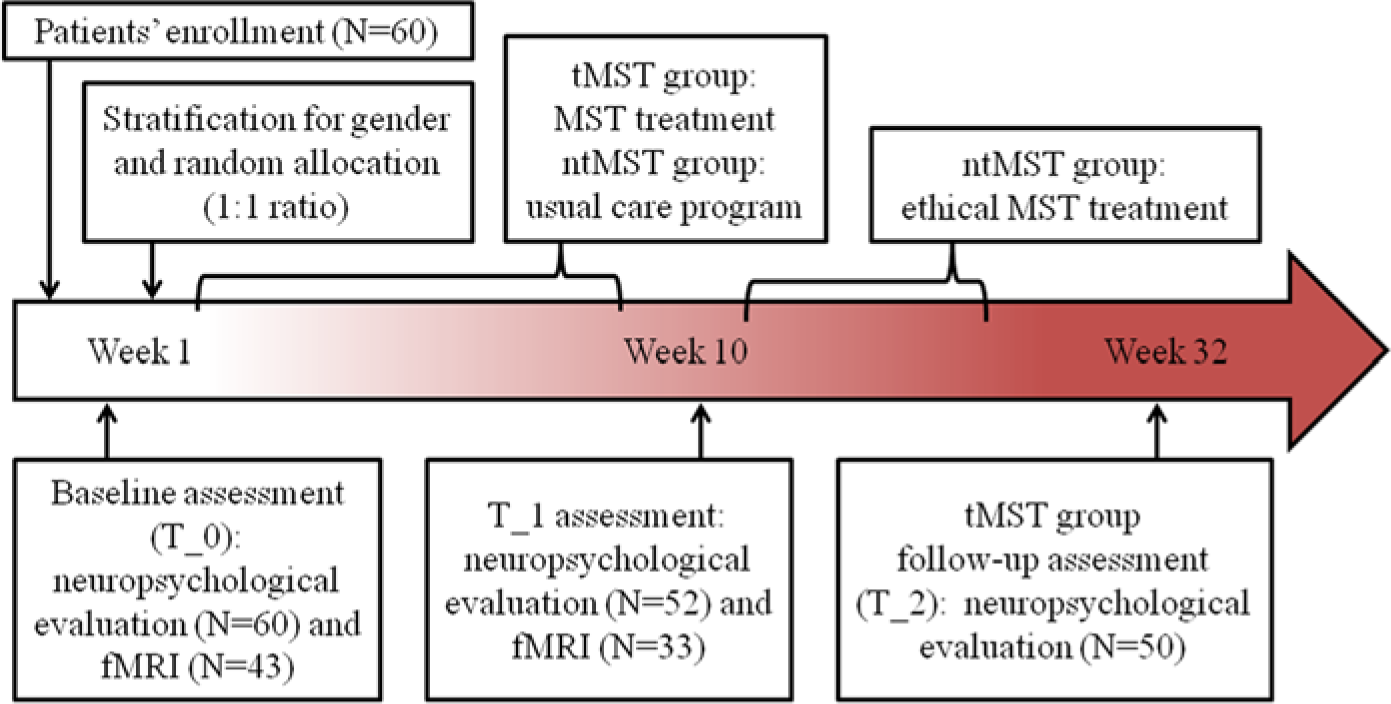
Timeline of the trial. Timing and duration of the various procedures used in the trial.
The tools used as primary outcome measures in this trial were the following: (a) Alzheimer’s Disease Assessment Scale–Cognitive subscale (ADAS-cog 31 ); (b) the Functional Living Skills Assessment Scale (FLSA 32 ); (c) the Neuropsychiatric Inventory scale (NPI 33 ); and (d) quality of life measures (Short Form 36 health survey questionnaire—SF-36 34 ). Changes in cognitive (ADAS-cog), functional (FLSA), behavioral (NPI) status, and in physical well-being (SF-36) were assessed by an experienced neuropsychologist blinded to the treatment.
Finally, we used fMRI with a language task (paced-overt verbal fluency task 35 ) to detect possible changes (T1 vs T0) in brain activation patterns in PWA as a surrogate biomarker of MST efficacy.
MRI Acquisition Protocol
MRI scans were obtained using a 1.5-Tesla scanner (Magnetom Avanto, Siemens). The protocol included the following: (a) a structural MRI study with T1, T2, and FLAIR weighted images to exclude subjects with pathological brain abnormality; (b) fMRI echo planar images with blood oxygenation level dependent (BOLD) contrast; and (c) a morphological T1-weighted MPRAGE sequence, used as reference for fMRI analysis and for the calculation of structural measures (hippocampal volumes) with FSL (FMRIB’s Software Library; www.fmrib.ox.ac.uk/fsl).
fMRI Stimuli/Design
We adopted the verbal fluency paradigm described by Basho and colleagues 35 to test language function. This fMRI task was chosen because it allows an appropriate response monitoring and a tight control over and reduced individual variability of task performance, making it suitable for the application in patients with cognitive deficits. The functional sequence included 6 experimental blocks alternated with 6 control blocks (30 seconds for block) for a total duration of 6 minutes (see Supplemental Methods for details, available online at http://nnr.sagepub.com/content/by/supplemental-data).
Before the fMRI session, all participants completed a practice session, which included different stimuli from those presented in the scanner. For stimuli presentation and overt responses collection, we used an MRI-compatible visual and sound system (VisuaStim Digital system from Resonance Technology Inc), while the use of E-Prime software 2.0 (http://www.pstnet.com) ensured exact timing of prompts.
Statistical Analysis
Statistical analysis on primary outcome measures was performed using SAS software package 9.2. Sociodemographic, clinical, and neuropsychological variables were compared at baseline using t test or χ2 test as appropriate.
The primary outcome measures in this study were changes in neuropsychological test and scale scores from baseline. We modeled these changes at 10 weeks. Only in the tMST group there were changes also evaluated at 22 weeks. To account for variable skewness, nonparametric analysis and variables normalization using Blom’s transformation were performed. Mann–Whitney nonparametric comparison of score differences was performed to identify statistically significant results. When variables resulted in a statistically significant difference, the analysis was confirmed using the analysis of covariance of normalized scores. Score differences were described using mean and standard deviation of retro-transformed Blom’s variables. Categorical variables were described by percentages. The least square differences and R2 model fitting were reported in Table 2. An α value of .05 was considered statistically significant, and all comparisons were 2-tailed. Finally, score modifications at 22 weeks in the tMST group were evaluated by means of regression analysis over time considering previous values at baseline and 10 weeks.
Analysis of Covariance Results for All Test/Scales and Statistically Significant Subscales of ADAS-Cog.
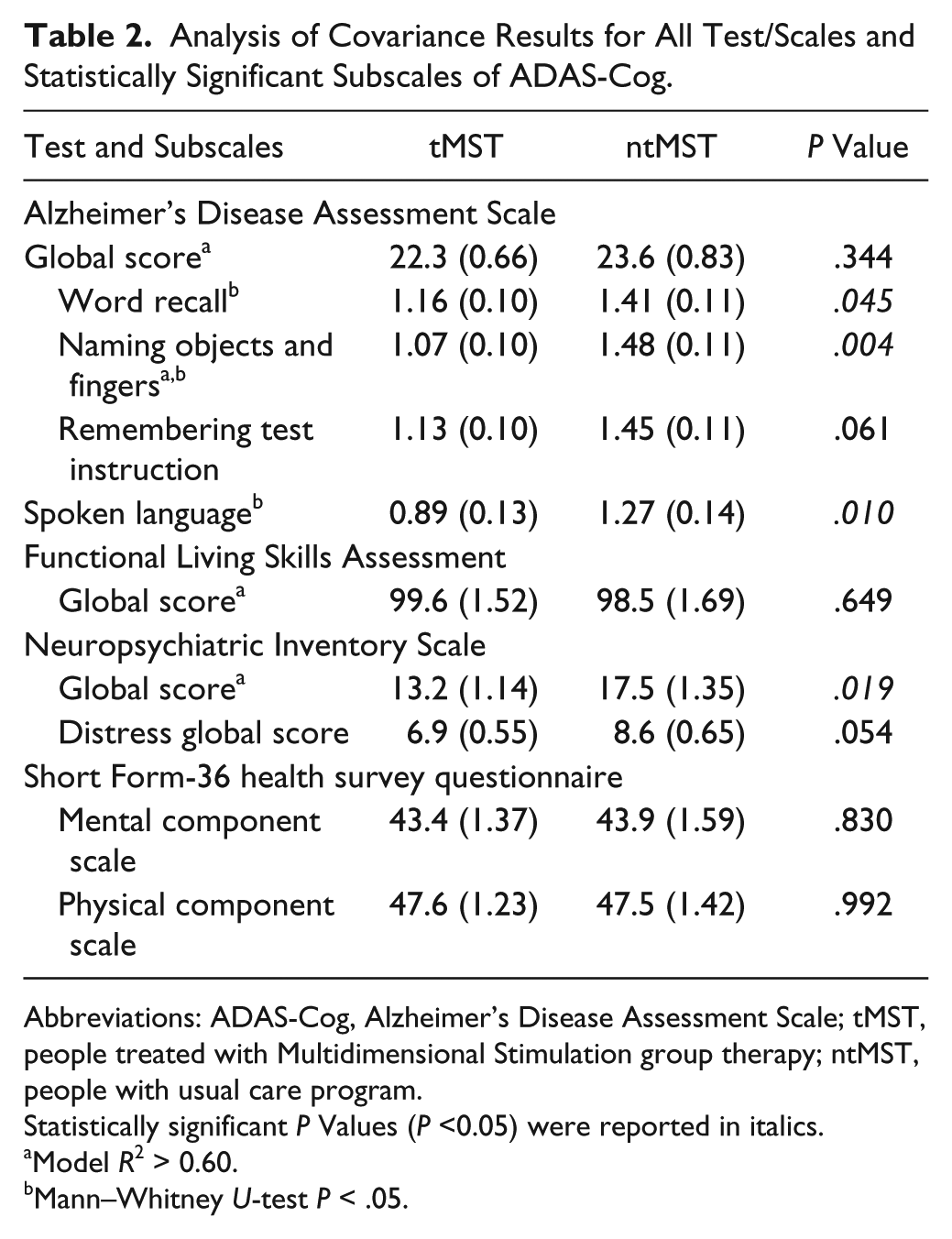
Abbreviations: ADAS-Cog, Alzheimer’s Disease Assessment Scale; tMST, people treated with Multidimensional Stimulation group therapy; ntMST, people with usual care program.
Statistically significant P Values (P <0.05) were reported in italics.
Model R2 > 0.60.
Mann–Whitney U-test P < .05.
fMRI Data Analysis
To investigate for fMRI task performance differences between groups at baseline and at 10 weeks, a logistic analysis was performed where percentages of correct task was the response variable and group by time interaction an explanatory covariate. To account for over dispersion of the response, the Williams scaling criterion was applied.
Statistical analysis on fMRI data was performed using SPM8 (http://www.fil.ion.ucl.ac.uk/spm). Images were realigned, coregistered, normalized (MNI space), and spatially smoothed. Single subject statistical analysis (first level) was then performed with a general linear model (GLM) to detect the activation areas during the task (t-contrast: categorical-fluency vs control-condition). The corresponding contrast images (1 image for each subject, obtained as the product between the GLM parameter estimates–betas–and the contrast vector) entered in the group analyses (second level).
First, to describe the main effect of the language task (typical activation pattern) and to extract regions of interest (ROIs) running Marsbar (http://marsbar.source-forge.net/) to be used as a priori ROIs for subsequent analyses on PWA (see below), we performed a 1-sample t test in the HC group (supplemental Figure S1 and Table S1).
The following second-level analyses were then performed in PWA: (a) 1-sample t tests in the PWA (both tMST and ntMST) at T_0 to describe the main effect of the language task at baseline; (b) 1-sample t tests in the PWA (both tMST and ntMST) at T_1 to describe the main effect of the language task after 10 weeks; (c) a flexible-factorial analysis including 3 factors (subject definition; group [tMST or ntMST]; time [T_0 or T_1]) to test the effect of treatment (tMST vs ntMST, group-by-time interaction: contrast 1: tMST [T_1 > T_0] > ntMST [T_1 > T_0]; contrast 2: ntMST [T_1 > T_0] > tMST [T_1 > T_0]). Normalized grey matter volume was included as a covariate. The maps resulting from the second-level analyses on PWA were thresholded with 2 approaches: first, we performed a statistical analysis within the ROIs identified in the control group by using correction for multiple comparisons (family-wise error [FWE], P < .05); then, for exploratory purposes, nonhypothesized group differences outside the ROIs were described considering an uncorrected P < .001 threshold with 10 or more contiguous voxels.
Finally, to investigate the relationship between changes in behavior and changes in magnitude of activation in tMST compared to ntMST, we performed an additional regression analysis considering score changes by groups. For each PWA we generated a single contrast map (T_1 > T_0) and we extracted the mean beta value within the 10 ROIs identified as critical for language functioning in the control group (see Table S2) running Marsbar tool (http://marsbar.sourceforge.net/). Then, we plotted ADASCog delta score (T_1 minus T_0 scores) against the beta values for all PWA subjects by groups in a linear regression analysis.
Results
The statistical analyses consisted of 28 PWA given MST and 24 given standard treatment of care (Figure 2). The 2 groups were similar at baseline in sociodemographic characteristics (age P = .58; gender P = .95; education level P = .47), global cognitive level (MMSE, P = .58), and brain hippocampal volumes (left hippocampus P = .76; right hippocampus P = .38; Table 1).
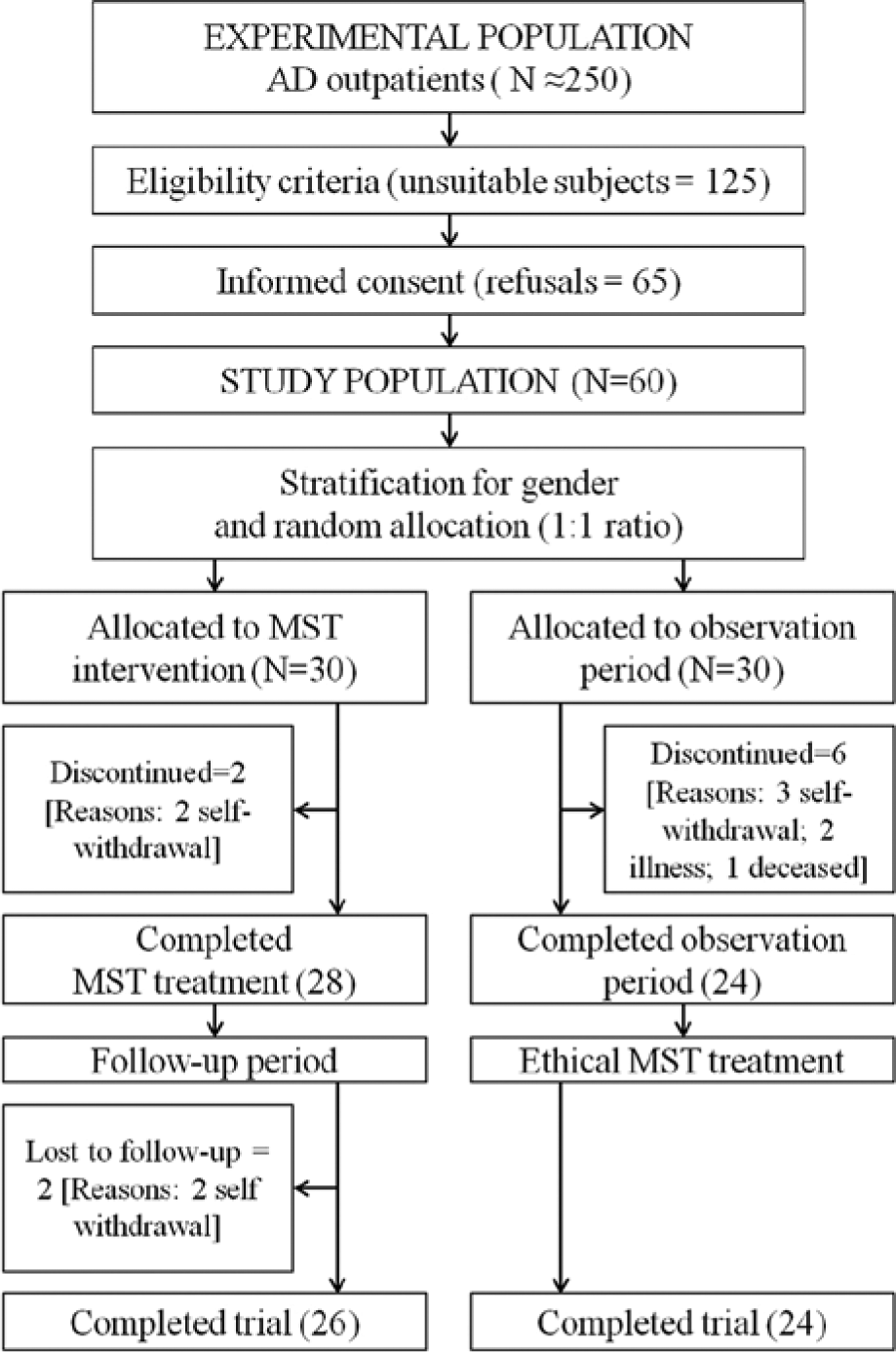
Trial profile.
Neuropsychological and Behavioral Results
The results obtained by PWA and the comparison between the 2 groups (tMST vs ntMST) on test and scales are summarized in Table 2. Behavioral symptoms showed a significant reduction in tMST with respect to ntMST (NPI global score P = .019). The tMST group also obtained a significant improvement in language (spoken language P = .01; naming objects and fingers P = .004) and memory (word recall P = .045; remembering test instructions P = .041) subscales of ADAS-Cog. No statistically significant differences between baseline and T_1 were observed in the measures of functional status (FLSA P = .649) and physical well-being (SF-36 MCS P = .83; SF-36 PCS P = .99).
Finally, we obtained no statistically significant slope of the regression model for any of the previous described cognitive (language and memory subscale of ADAS-Cog) and behavioral (NPI values) measures considered in the tMST group at 22 weeks with respect to baseline and 10 weeks results.
fMRI Results
Regarding fMRI, only data relative to 22 PWA (12 tMST and 10 ntMST) entered the second-level fMRI analyses (the details of this subsample are shown in Supplemental results and Table S2). The task performance of the included subjects on correct responses was 83.1% to 84.2% (tMST-ntMST) at baseline and 88.9% to 87.8 % (tMST-ntMST) after 10 weeks. The fMRI task performance differences within group (tMST P = .37; ntMST P = .70) and between groups at baseline and 10 weeks were not statistically significant (P = .47).
In line with previous findings,35,36 the healthy controls exhibited a typical activation pattern of paced overt verbal fluency task: areas related to category-driven word generation (left inferior and middle frontal cortex, the superior and middle temporal regions, left thalamus and lentiform nucleus), areas associated with paced response and overt articulation (cingulate cortex, right superior parietal cortex, insular cortex, thalamus, lentiform nucleus and cerebellum; see supplemental Figure S1 and Table S1 for details). These clusters were chosen as a priori ROIs for subsequent analyses.
As shown in Figure 3A, a significant activation (PFWE < .05) in PWA was found at T_0 only in the left superior temporal gyrus (BA 22). For exploratory purposes, considering an uncorrected threshold P < .001 with 10 or more contiguous voxels, we found brain activations also in the left inferior frontal (BA 44) gyrus.
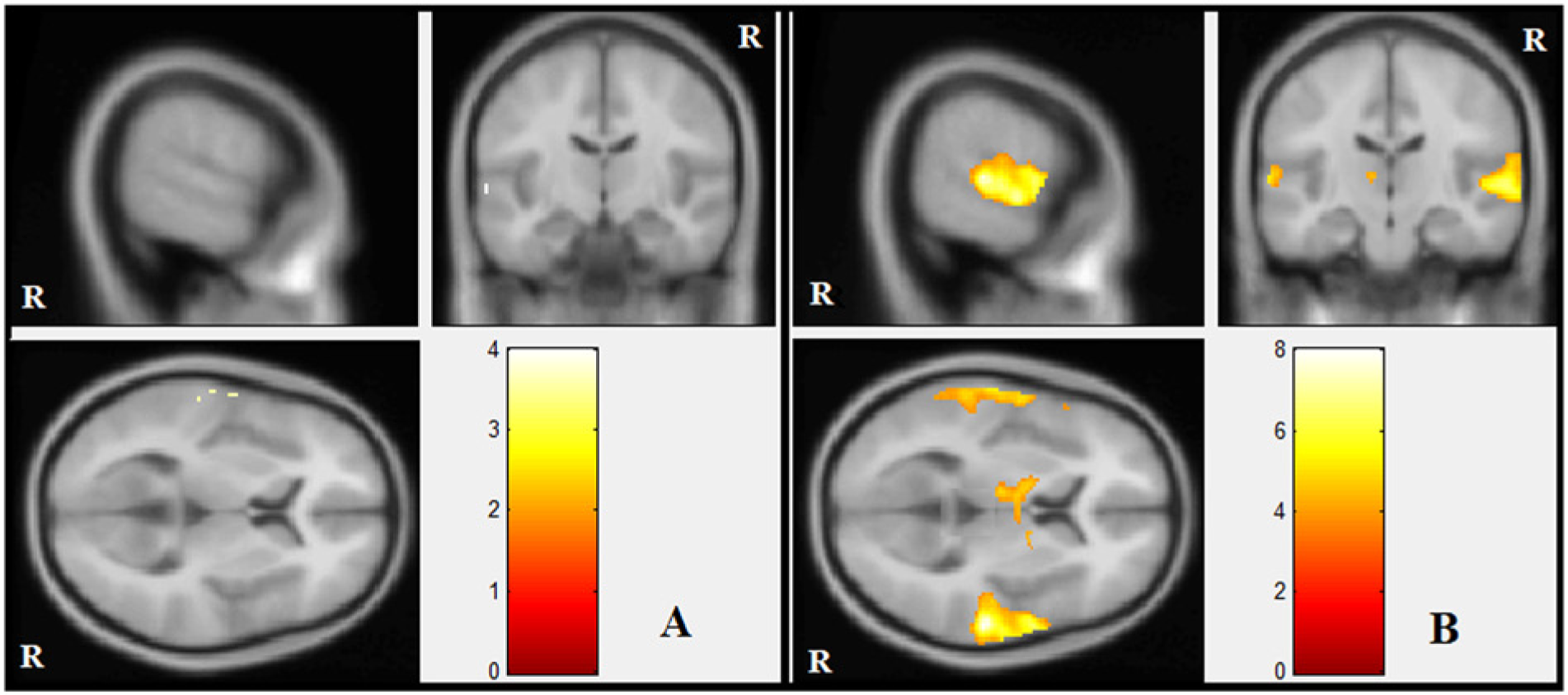
Main effect of paced-overt verbal fluency task in PWA: brain areas showing a significant activation at baseline (A) and after 10 weeks (B).
At T_1 (Figure 3B), the activation pattern found at baseline was strongly increased, resulting in significant activations (PFWE < .05) in the left inferior frontal and superior temporal gyri, the right superior temporal cortex (BA 22-41), the left cingulate cortex (BA32), the bilateral basal ganglia, thalamus, and the right superior parietal lobule (BA 7). Considering an uncorrected threshold P < .001 with more than 10 contiguous voxels, we found an additional brain activation in the right cerebellum.
Results of the flexible factorial analysis evaluating the effect of treatment (group-by-time interaction) are reported in Table 3: the tMST group showed a significant intervention-related increase in activation (contrast 1: tMST [T_1 > T_0] > ntMST [T_1 > T_0], PFWE < .05) of the bilateral superior temporal gyrus (right > left) and the right lentiform nucleus and thalamus. Considering an uncorrected threshold P < .001 with more than 10 contiguous voxels, we observed in the tMST group an additional increase in brain activation in the right insular cortex with respect to the ntMST due to the MST intervention. No significant activation were found with the opposite contrast (contrast 2: ntMST [T_1 > T_0] > tMST [T_1 > T_0]). The plots in Figure 4 illustrate the mean beta values for each group (ntMST and tMST) at T_0 and T_1 extracted from the 4 clusters described in Table 3.
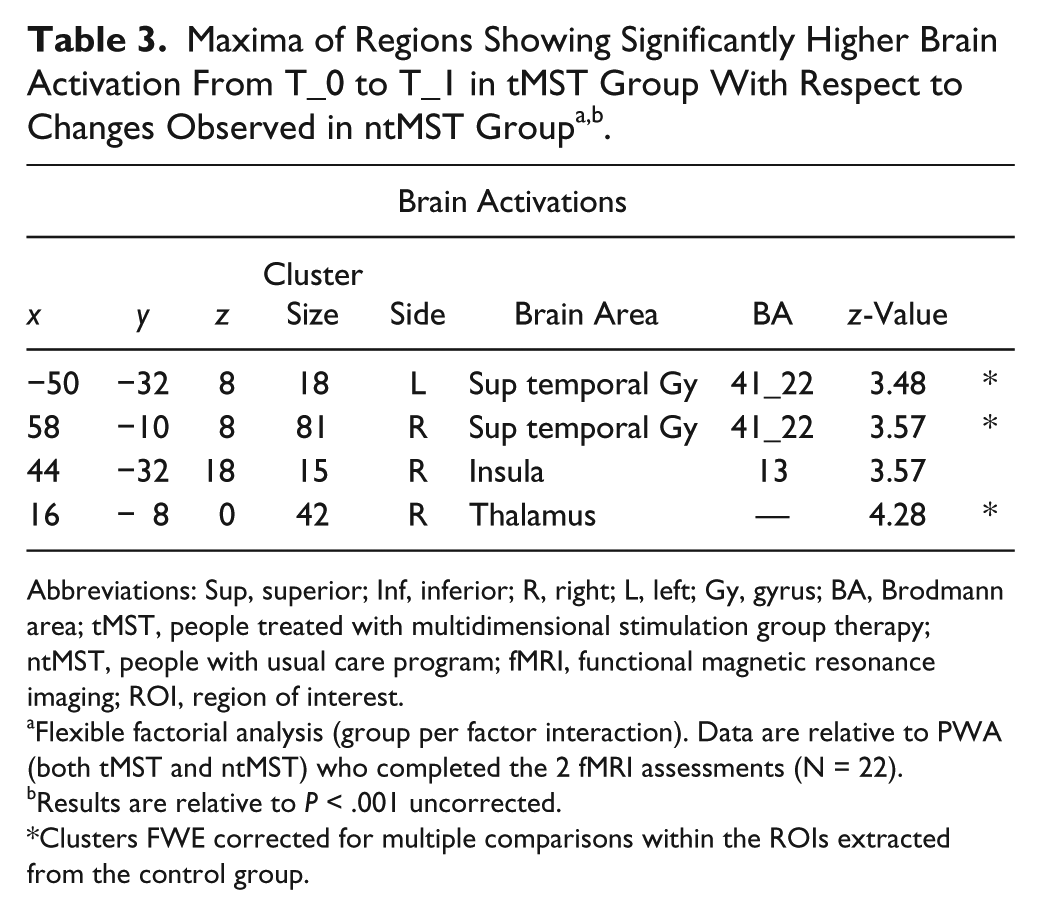
Abbreviations: Sup, superior; Inf, inferior; R, right; L, left; Gy, gyrus; BA, Brodmann area; tMST, people treated with multidimensional stimulation group therapy; ntMST, people with usual care program; fMRI, functional magnetic resonance imaging; ROI, region of interest.
Flexible factorial analysis (group per factor interaction). Data are relative to PWA (both tMST and ntMST) who completed the 2 fMRI assessments (N = 22).
Results are relative to P < .001 uncorrected.
Clusters FWE corrected for multiple comparisons within the ROIs extracted from the control group.
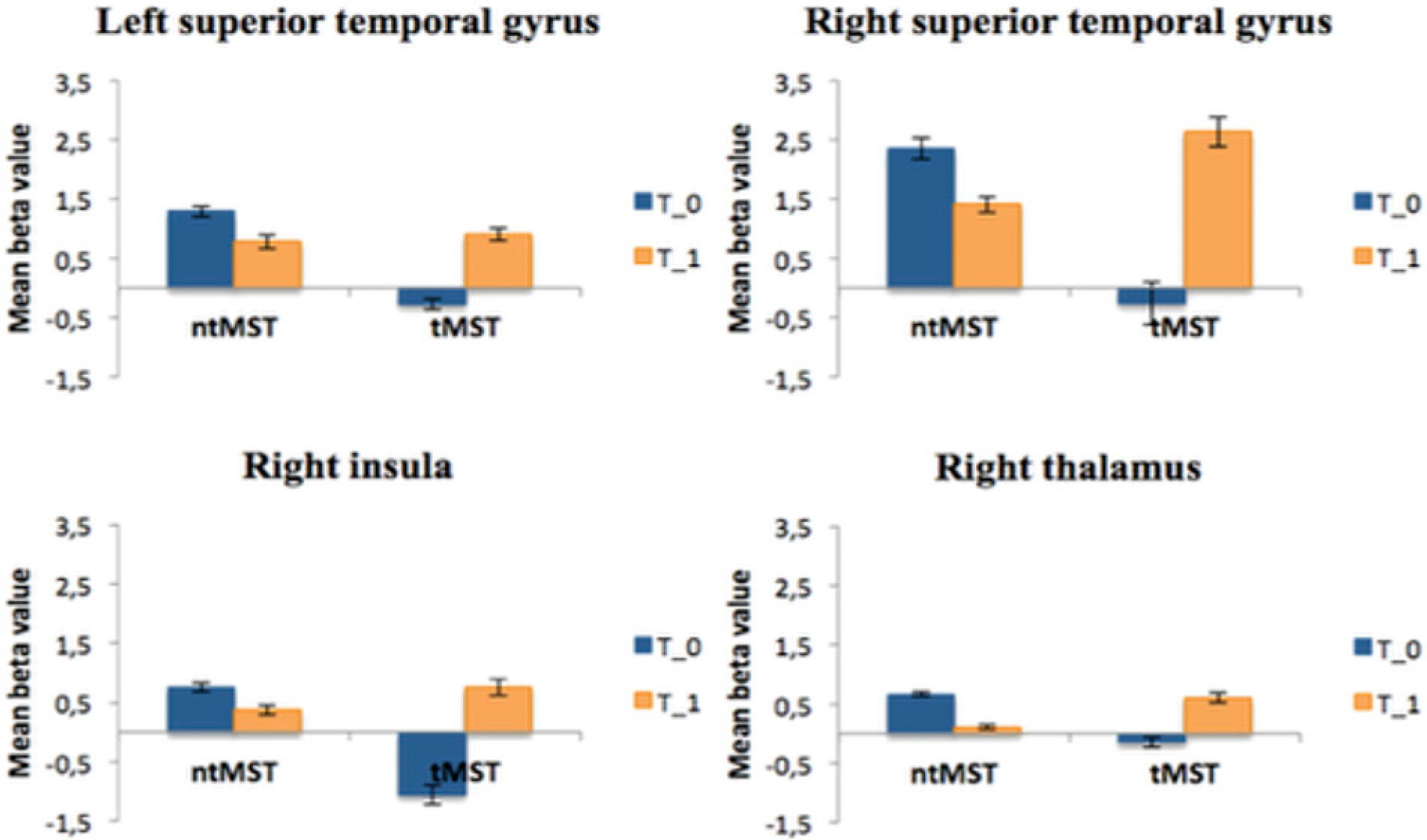
Plots show mean beta values for each group (ntMST and tMST) at baseline (T_0) and after 10 weeks (T_1) extracted from the 4 clusters refer to contrast: tMST (T_1 > T_0) > ntMST (T_1 > T_0) (see Table 3).
Finally, the results of regression analysis are reported in Figure 5. In the tMST group we found a significant correlation between increase in magnitude of activation in the left superior temporal gyrus (BA 22/41—ROI 2), precuneus (BA7—ROI 5), left thalamus (ROI 9), and change in ADAS-Cog. Conversely, only one significant correlation was found in ntMST group between the left superior temporal gyrus (ROI 2) and change in ADAS-Cog. The negative correlation is due to the ADAS-Cog score: a decrease in ADAS-Cog score is indicative of cognitive improvement.
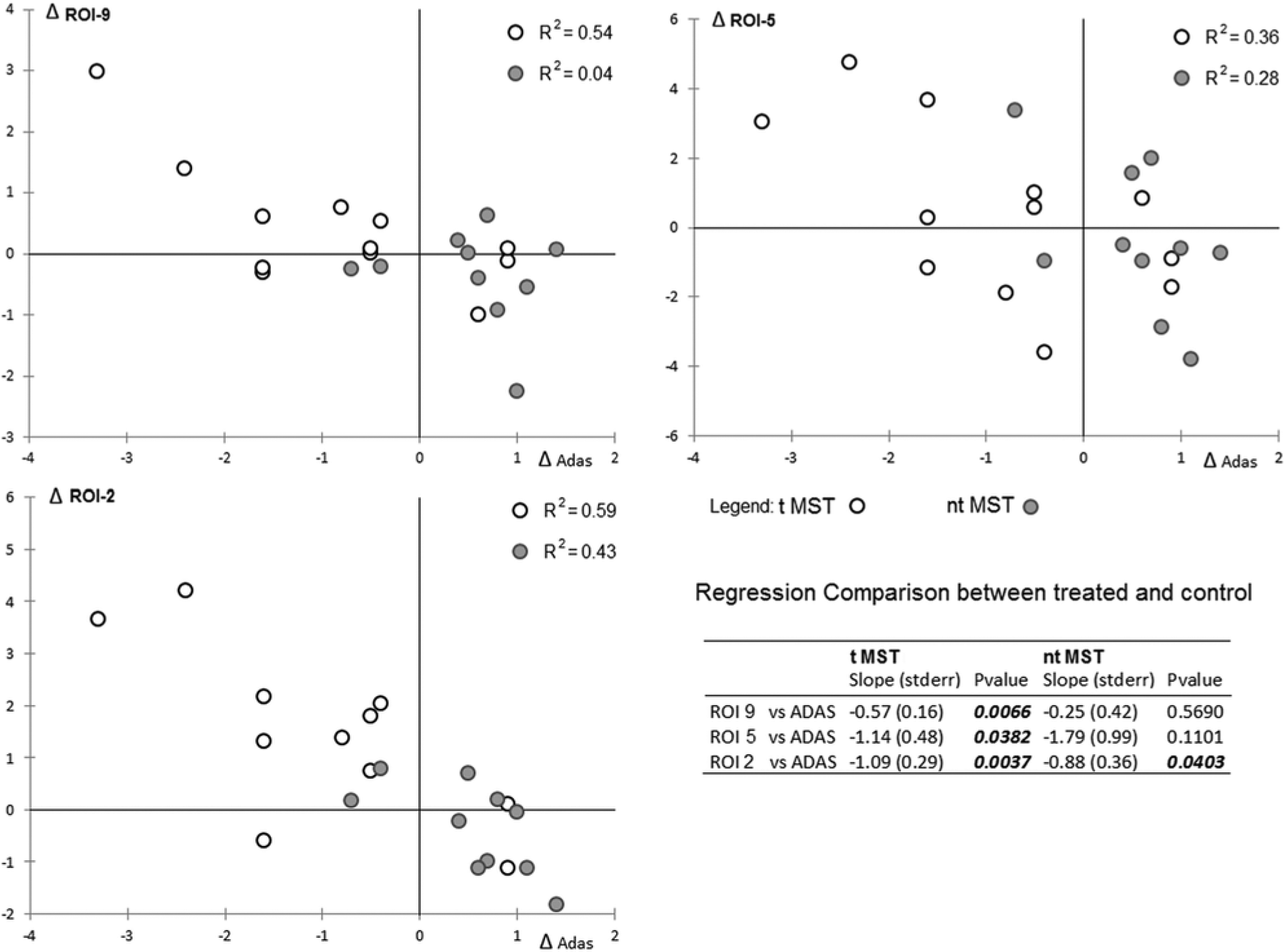
Scatterplots show statistically significant results of regression analysis considering score changes by groups.
Discussion
The results obtained in this RCT study supported the initial hypothesis that MST has an impact on at least 2 AD domains: behavior-reduction of BPSD and improvement in some cognitive abilities.
Regarding the behavioral domain, these results confirm our previous findings24,25 and are in line with other nonpharmacological studies that reported a reduction of BPSD with the single components of our therapy.37-41 MST can be easily implemented with both ambulatory patients, such as in our case, and institutionalized ones and applies to people with BPSD in the moderate range. As severe psychotic symptoms (hallucinations, significant delusions, or evident aggression) would preclude the participation in group therapy, we did not include this type of PWA in this study. Examining the single items of NPI, we observed that the BPSD which benefit most from MST were depression, anxiety, irritability, and aberrant motor behavior. Teri and her group 37 observed a decrease of depression in PWA after a treatment based on physical activity. Interestingly, different mechanisms were recently suggested to support the notion that exercise may have the potential to slow the decline of AD.19,42 There is the possibility that new brain cells can be created within the critical parts of the hippocampus in PWA who are physically fit. There is also the possibility that increased neural connectivity can be obtained through the neuroplastical activity of BDNF, whose levels appear to be increased by exercise. 43 Gitlin et al have reported38,39 a reduction of BPSD as a result of an occupational therapy intervention with empowerment of caregiver coping abilities. They also showed that nonpharmacologic management of BPSD is a recommended, cost-effective treatment as it can significantly improve quality of life and patient–caregiver satisfaction. 15 Reduction of apathy, a BPDS symptom very difficult to treat, has been reported with an occupational therapy approach, 40 and even more “cognitive-oriented” techniques. 44 However, we believe that MST, a multidimensional treatment including all of these techniques, is the most suitable to obtain positive results, in concordance with Arkin’s opinion: “Clinically, there is much to be said for leaving the combined intervention intact. By offering a variety of activities, you are providing multiple and different opportunities for participants to be successful.” 21 Moreover, we are now well aware of the possible side effects and risks of psychotropic medications in PWA. Consequently, nonpharmacological interventions have become the first-line approach for BPSD.15,41 In this perspective, the MST approach can be helpful to avoid the excessive use of these drugs for BPSD.
As far as the cognitive domain is concerned, we found an improvement of language and memory ADAS-Cog subscales. This is in line with a recent study by Hall and colleagues 13 investigating the effects of CST 9 on specific areas of cognition. They attribute the changes in language and memory to the language-based nature of CST that enhances neural pathways responsible for processing of syntax, possibly aiding also verbal recall. Moreover, they hypothesize that these CST-induced changes promote the functioning of alternative neural pathways. 45 As with CST, 12 our MST was group-based and included, in the first step of level 1 (Reality Orientation activities and cognitive exercises), many tasks aimed to reinforce oral and written language. Furthermore, group therapy has been shown to facilitate social interaction among participants and to consequently promote language function, 46 thereby reducing the additional handicap due to social isolation of PWA. 17 For the first time, we are able to discuss also the neural mechanisms that may underlie these intervention-related changes on language by using fMRI. The fMRI results at T_1 with respect to T_0 showed increased brain activation in left frontotemporal areas (BA 22/44), right superior temporal cortex, bilateral basal ganglia, cingulate cortex, and right superior parietal cortex. In the tMST group, an intervention-related increase in activations was found in the bilateral superior temporal cortex (BA 22/41), the thalamus, and the anterior insular cortex. It is known that thalamus and basal ganglia play an important role in word generation, and recent data suggest that the thalamus acts as a central monitor for language-specific cortical activities, supported by the basal ganglia in both perceptual and productive language execution. 47 Moreover, the insular cortex plays an important role in speech and emotional experience, and it has been demonstrated that hypometabolism of the anterior insula is associated with progressive nonfluent aphasia. 48 Furthermore, MRI studies have shown that the insula is interconnected with the temporal and orbitofrontal cortices and inferior frontal gyrus. 49 The obtained fMRI intervention-related changes may reflect a restoration of neural function in the underactive language network via the compensatory strengthening of specific brain regions. 45 Further intervention-related changes, although using an encoding-recognition task, were described using fMRI by Clare and colleagues. 6 They performed an RCT on cognitive rehabilitation in people with dementia and a subset of participants also underwent fMRI scanning. Four right brain regions forming part of the network for visual associative learning (fusiform face area, medial prefrontal gyrus, parahippocampal cortex, and temporal parietal junction) showed increased activation due to the treatment and the authors inferred that these results primarily reflect restoration of function in PWA.
The changes we saw in fMRI support the notion that even the AD brain still has plasticity resources and can react to positive environmental stimuli. Obviously, intervention in the predementia stage could improve the memory domain even more so, assuming that the more precocious the cognitive intervention is, the better the result will be. In this perspective, it is interesting to note that some recent studies reported increased hippocampal activity after memory training in MCI people, suggesting that the hippocampus may retain sufficient neuroplasticity in this clinical situation.50,51 However, even if this will probably be the right strategy in the future, our study, along with others,13,22,39 demonstrates that cognitive stimulation can be useful in people with overt AD.
Regarding the long-lasting effect of the treatment, our data showed that the improvement in cognitive and behavioral areas is preserved at 22 weeks. The persistence of effects, along with generalization of gain in everyday life, is the critical point of nonpharmacological therapies and is being explored in ongoing trials. 11 The necessity of a long-term treatment to maintain positive effects engenders the problem of the treatment costs. However, it must be considered that MST is a group treatment, potentially allowing for a more effective use of personnel resources when compared to individual-specific techniques. Moreover, relatives and caregivers assisting PWA at home can be trained for this type of treatment to reinforce and make the benefits more enduring. 24
We consider the differences in cognition and behavior are clinically meaningful. PWA in the treated group showed a reduction of BPSD of almost 20% from the baseline level. Moreover, this result was due above all to reduction of symptoms such as depression, irritability, and aberrant motor behavior, which have a particular negative impact on caregivers in our clinical experience. 52 We consider this result clinically significant, because it can allow a reduction of the use of antipsychotic drugs, whose harmful effects on PWA is now well known. As for the clinical value of results in the cognitive domain, we believe that obtaining even a moderate improvement of language and memory is a meaningful result: memory impairment is the principal symptom of PWA and is a source of depression for them and of burden for caregivers (eg, due to repetitive questioning) 53 ; impairment of language, on the other hand, favors social isolation and has particular negative sequelae for the interaction with family members, increasing their burden of care. In the progression from moderate to severe stages in AD, worsening language abilities, or aphasia, has been suggested to have more clinical relevance than other domains. As a matter of fact, decline in language has been shown to correlate with noncognitive items, such as personal care, hobbies, occupations, and behavior. 53
Overall, despite the significant results in improving different aspects of PWA, our study is not without limitations. Although the improvement in cognitive and behavioral areas was preserved in the tMST group at 22 weeks, the length of follow-up was relatively short. Thus, whether or not the treatment effect produced by the MST approach is long-lasting remains unknown at this time. Future studies should investigate MST’s efficacy over longer durations of time. Furthermore, a direct comparison between the tMST and ntMST groups at T_2 was not possible due to ethical concerns. Our ethical committee requested that we also treat the ntMST group after T_1 evaluation.
In conclusion, MST is a nonpharmacological approach for mild to moderate PWA that was shown to have a positive impact on behavioral and cognitive functions, enhancing patients’ motivation, promoting the use of their remaining function, and preventing further loss in agreement with the statement “use it or lose it.” 54
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by 2011-2012 Ricerca Corrente (Italian Ministry of Health).