
Abstract
Background. In France in 2009, patients admitted to Multidisciplinary Inpatient Rehabilitation for stroke were sent to a neurological rehabilitation center (NRC) or a general or geriatric rehabilitation (GRC) service. Objective. To describe the functional outcome of stroke patients admitted for rehabilitation in France in 2009, both globally and as a function of the rehabilitation setting (GRC or NRC). Methods. Data from the French Hospital Discharge Diagnosis databases for 2009 were included. Two logistic regression models were used to analyze factors related to improvement in dependence score and discharge home. Odds ratios (ORs) were also calculated. Results. Among the 83 505 survivors of acute stroke in 2009, 28 201 were admitted for rehabilitation (33.8%). Of these, 19 553 went to GRC (69%) and 8648 to NRC (31%). On average, patients admitted to GRC were older (78.6 years vs 66.4 years), P < .001). At the start of rehabilitation, 50% of NRC patients and 56% of GRC patients were heavily dependent, but level of dependence was similar within each age-group. Rehabilitation in NRC lead to a greater probability of functional improvement (OR = 1.75, P < .001) and home discharge (OR = 1.61, P < .001) after adjustment for gender, age, Charlson’s comorbidity index, initial level of dependence, type of stroke, and total length of stay. Conclusion. This study confirms, on a national level, the functional benefit of specialized rehabilitation in NRC. These results should be useful in the improvement of care pathways, organization of rehabilitation, and discharge planning.
Introduction
Stroke is a frequent and serious pathology. It is one of the major causes of disability, the second most frequent cause of dementia, and the third most frequent cause of mortality. 1 The cost of stroke is considerable ($22.8 billion in the United States in 2009) and in France, 29% of the costs of the first year poststroke are incurred in the post–acute care inpatient sector.2,3
The efficiency of the care pathway for post–acute stroke patients is a major issue for patient rehabilitation and recovery.4,5 In the acute phase, management within a stroke unit has been shown to be effective. 6 In the postacute phase, many studies and meta-analyses have indisputably demonstrated the effectiveness of specific, multidisciplinary rehabilitation.7-13 Functional prognosis, morbidity and mortality, quality of life, and home-discharge possibility have all been shown to improve when patients are cared for within a specialized center. A recent study showed that the effectiveness of specialized care in the subacute phase, whatever the severity of the initial impairment, was directly related to the level of organization and coordination of rehabilitation. 14
In France, after initial care in a stroke unit (approximately 10 days), the patient may be discharged directly home or he or she may be sent for rehabilitation, which, in France, may be carried out in a neurological rehabilitation center (NRC) with specialized, coordinated rehabilitation or in a general or geriatric rehabilitation center (GRC). 15 In a previous study, we showed that in France, the vast majority of patients admitted for rehabilitation went to GRC.16,17 Older patients with a severe initial impairment and those with cognitive impairments tend to be more frequently admitted to GRC. The number of rehabilitation beds (NRC + GRC) in France is estimated at 175/100 000 inhabitants. Decisions regarding admission to both types of rehabilitation (GRC or NRC) are made by the neurologist, following advice from a physiatrist when the patient is in a stroke unit.
Factors that favor admission to a NRC relate to initial care in a stroke unit and the number of NRC beds or places in the region. The majority of poststroke patients are admitted to GRC, and this mostly depends on factors such as the number of places available in each type of rehabilitation in the region and the networks between acute care and rehabilitation.
The impact of specialized rehabilitation on independence has never been studied on a national level. We feel that it is important to study this impact in order to improve the management of stroke patients in France and elsewhere.
The aim of this study was to describe the functional outcome of stroke patients admitted for rehabilitation in France in 2009, both globally and as a function of the rehabilitation setting (GRC or NRC).
Methods
Data Source
Data were obtained from the French national hospital discharge diagnosis databases: PMSI MCO for Acute Care (AC) and PMSI SSR for Rehabilitation. Although these databases are separate, patients can be followed throughout their hospital stays using an anonymous identification number which is unique to each patient. The databases were obtained from the national hospital information agency (Agence technique de l’information sur l’hospitalisation [ATIH]) and identification numbers were analyzed by the French Institute for Public Health Surveillance (Institut de Veille Sanitaire, InVS).
Data Selection
Patients who were discharged between January 1 and December 31, 2009 with a main diagnosis of stroke were first identified in the AC database and then searched for in the 2009 Rehabilitation database using the anonymous identification number. Both databases contain information regarding the patient’s demographic characteristics (age, gender) as well as the main diagnosis and comorbid factors based on the International Classification of Disease, 10th revision.
Admissions recorded in the AC database with a main diagnosis denoted by one of the following codes were included in the study database: I60 for subarachnoid hemorrhage, I61 for intracerebral hemorrhage, I63 for cerebral infarction, I64 for nonspecified stroke, and G46 for vascular syndromes (if one of the previous stroke codes was a secondary diagnosis), and I62 for other nontraumatic intracranial hemorrhages. Day hospital patients were excluded. Only the first major admission of the year with a main diagnosis of stroke was retained for each patient. Patients with anomalies in their identification number (748, 0.7%) as well as those who died during acute care (15 274, 15%) were excluded since they would not be found in the Rehabilitation database. The patients included were then searched for in the Rehabilitation database. Only those whose admission for rehabilitation began during the same month or the month following discharge from acute- care were considered as compatible with post–acute stroke care and were included.
Variables Calculated
Several variables were calculated. Charlson’s index was calculated from the comorbid factors stated in the AC database and adapted to the study: All the pathologies relating to this index were taken into account according to published algorithms, 18 with the corresponding weightings, except for cerebrovascular diseases, which were the factor that was common to all patients, and age which was studied separately. Level of dependence was analyzed using 5 variables in the Rehabilitation database: 1 behavioral variable and 4 variables relating to physical dependence (ambulation, dressing, feeding, and continence). These variables were all scored between 1 and 4 (1 = independence, 2 = supervision, 3 = requires partial assistance, and 4 = requires total assistance) each week of the rehabilitation. The behavior variable related to the patient’s level of social interaction (gets on with and participates with others, in social or therapeutic situations). A score of 2 denotes a need for supervision in the case of unusual or stressful situations. This score was considered poor if it was higher than 2. Two functional dependence scores were calculated by summing the scores of the 4 physical dependence variables, one in the first week of rehabilitation and the other in the last week: Physical dependence was considered high for scores greater than or equal to 12. Changes in physical dependence between the first and last week of rehabilitation were calculated by subtracting the initial score from the final score.
Statistical Analysis
Analyses were carried out over the whole of 2009 with the exception of length of stay in rehabilitation, discharge mode, and changes in level of dependence, which were limited to the patients admitted to rehabilitation during the first semester (between January and June; 14 795 patients) because of the large number of very long stays in rehabilitation.
Chi-square tests were used to compare percentages and for analyses of associations between qualitative variables in the whole group and also in each age subgroup. A Kruskal–Wallis test was used to analyze between-group differences for the quantitative variables. Two multivariate analyses were carried out using logistic regression: One analyzed factors associated with improvements in the dependence score and the other analyzed the factors associated with discharge home. The associations between improvement in independence and the postrehabilitation outcome (including deaths) were analyzed as a function of the following variables: age, gender, type of stroke, comorbid factors, and length of stay.
All statistical analyses were carried out using SAS Enterprise Guide version 4.3 software.
Results
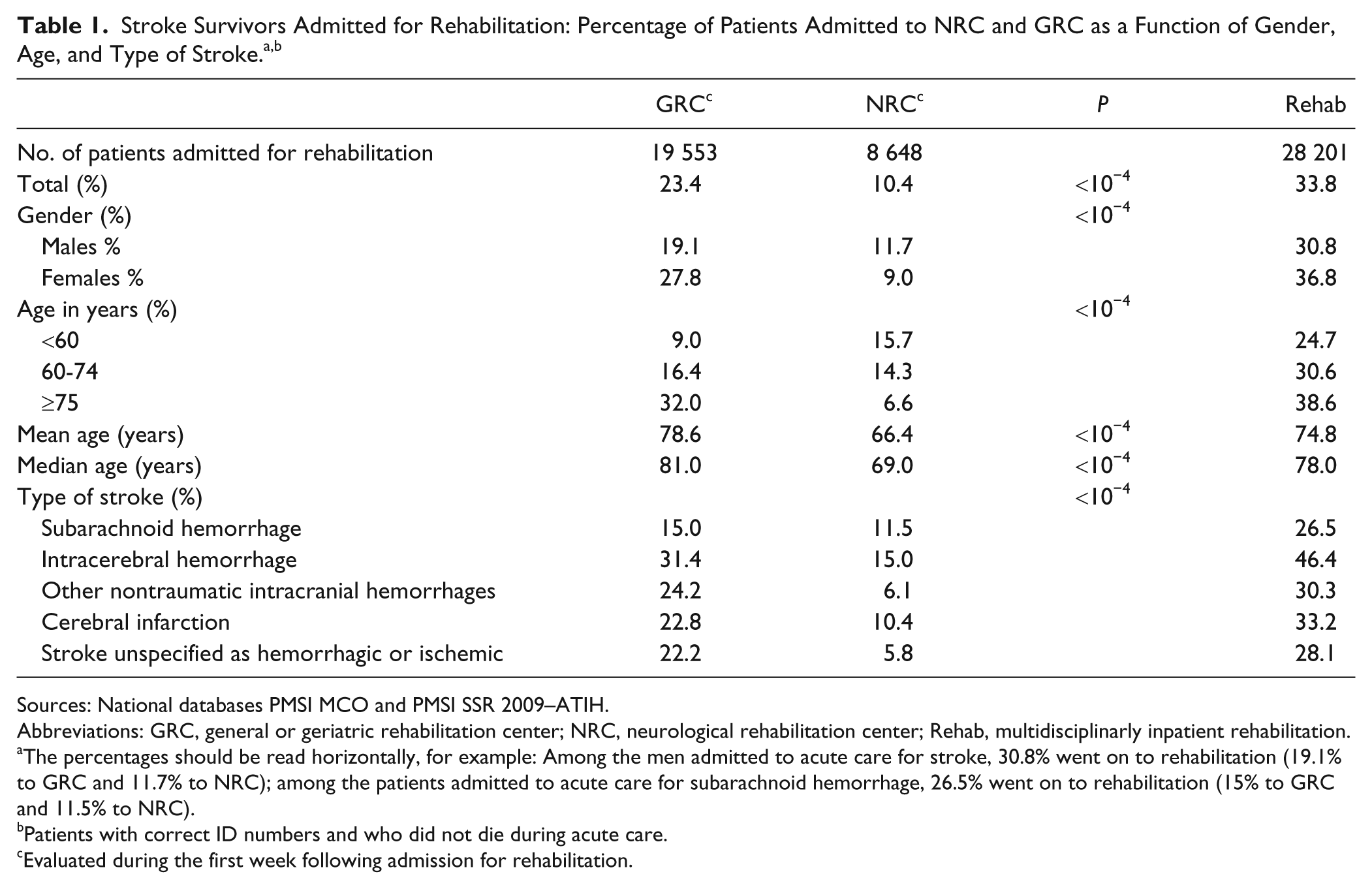
In 2009, the number of patients admitted for stroke rehabilitation following acute care was 28 201 out of 83 505 survivors at discharge from acute care (33.8%; Table 1). Among them, 19 553 (23.4%) were admitted to GRC and 8648 (10.4%) to NRC. Mean age was 74.8 years; 78.6 years in GRC, and 66.4 years in NRC (P < 10−3).
Sources: National databases PMSI MCO and PMSI SSR 2009–ATIH.
Abbreviations: GRC, general or geriatric rehabilitation center; NRC, neurological rehabilitation center; Rehab, multidisciplinarly inpatient rehabilitation.
The percentages should be read horizontally, for example: Among the men admitted to acute care for stroke, 30.8% went on to rehabilitation (19.1% to GRC and 11.7% to NRC); among the patients admitted to acute care for subarachnoid hemorrhage, 26.5% went on to rehabilitation (15% to GRC and 11.5% to NRC).
Patients with correct ID numbers and who did not die during acute care.
Evaluated during the first week following admission for rehabilitation.
Level of Dependence at Admission for Rehabilitation
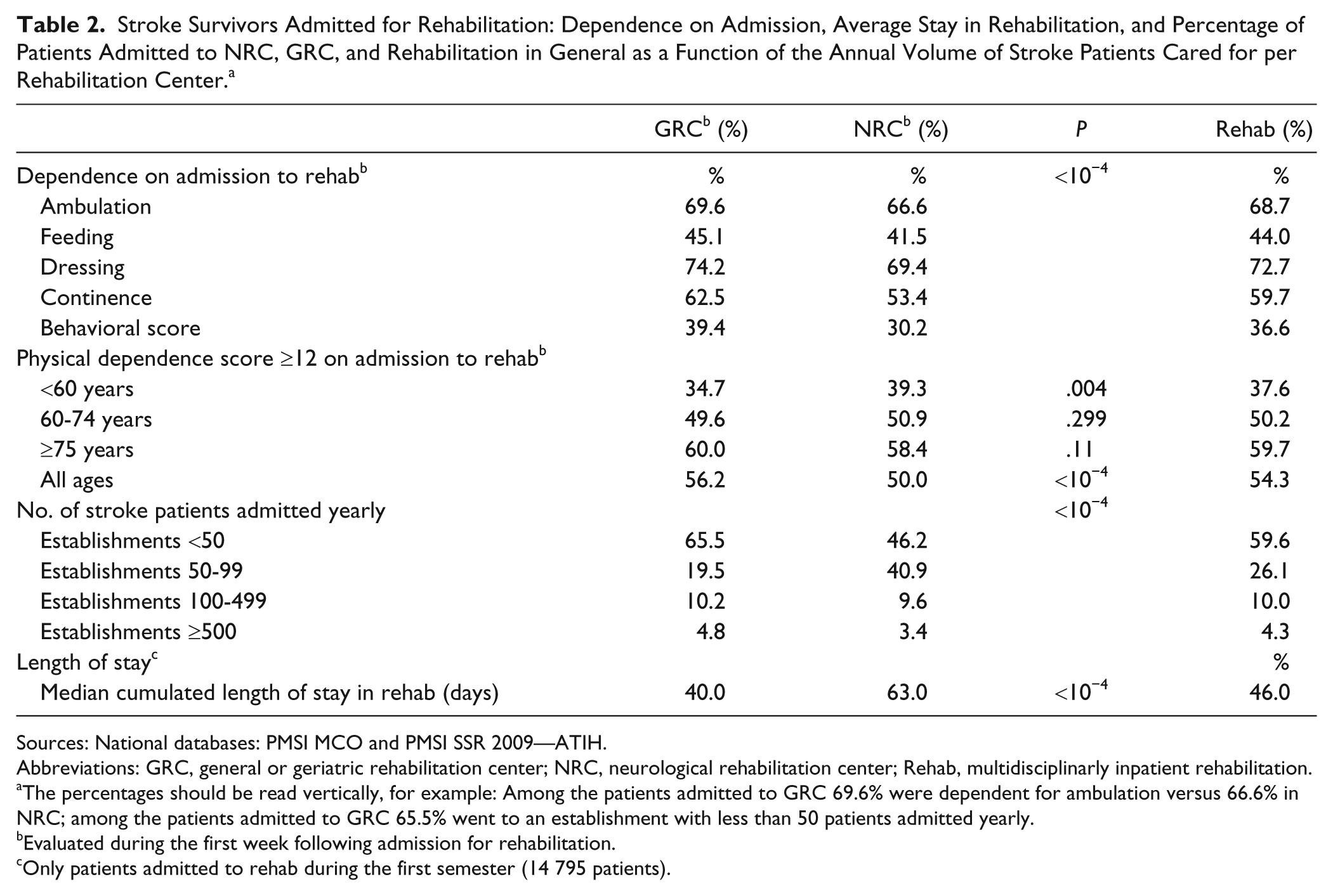
On admission for rehabilitation, one third of the patients had an altered behavior score. Almost 70% required total or partial assistance for ambulation (68.7%), 72.7% for dressing, 44.0% for feeding and 59.7% for continence (Table 2). More than half of the patients had a high global physical dependence score (≥12), this proportion increased with age from 37.6% before the age of 60 years to 59.7% older than 75 years. When all ages were pooled, the crude frequency of heavily dependent patients was lower in NRC than in GRC for each of the physical and behavioral items (P < .001). However, the frequency was comparable within age-groups or was higher in NRC than GRC (for the <60 age-group).
Stroke Survivors Admitted for Rehabilitation: Dependence on Admission, Average Stay in Rehabilitation, and Percentage of Patients Admitted to NRC, GRC, and Rehabilitation in General as a Function of the Annual Volume of Stroke Patients Cared for per Rehabilitation Center. a
Sources: National databases: PMSI MCO and PMSI SSR 2009—ATIH.
Abbreviations: GRC, general or geriatric rehabilitation center; NRC, neurological rehabilitation center; Rehab, multidisciplinarly inpatient rehabilitation.
The percentages should be read vertically, for example: Among the patients admitted to GRC 69.6% were dependent for ambulation versus 66.6% in NRC; among the patients admitted to GRC 65.5% went to an establishment with less than 50 patients admitted yearly.
Evaluated during the first week following admission for rehabilitation.
Only patients admitted to rehab during the first semester (14 795 patients).
Level of Dependence at Discharge From Rehabilitation
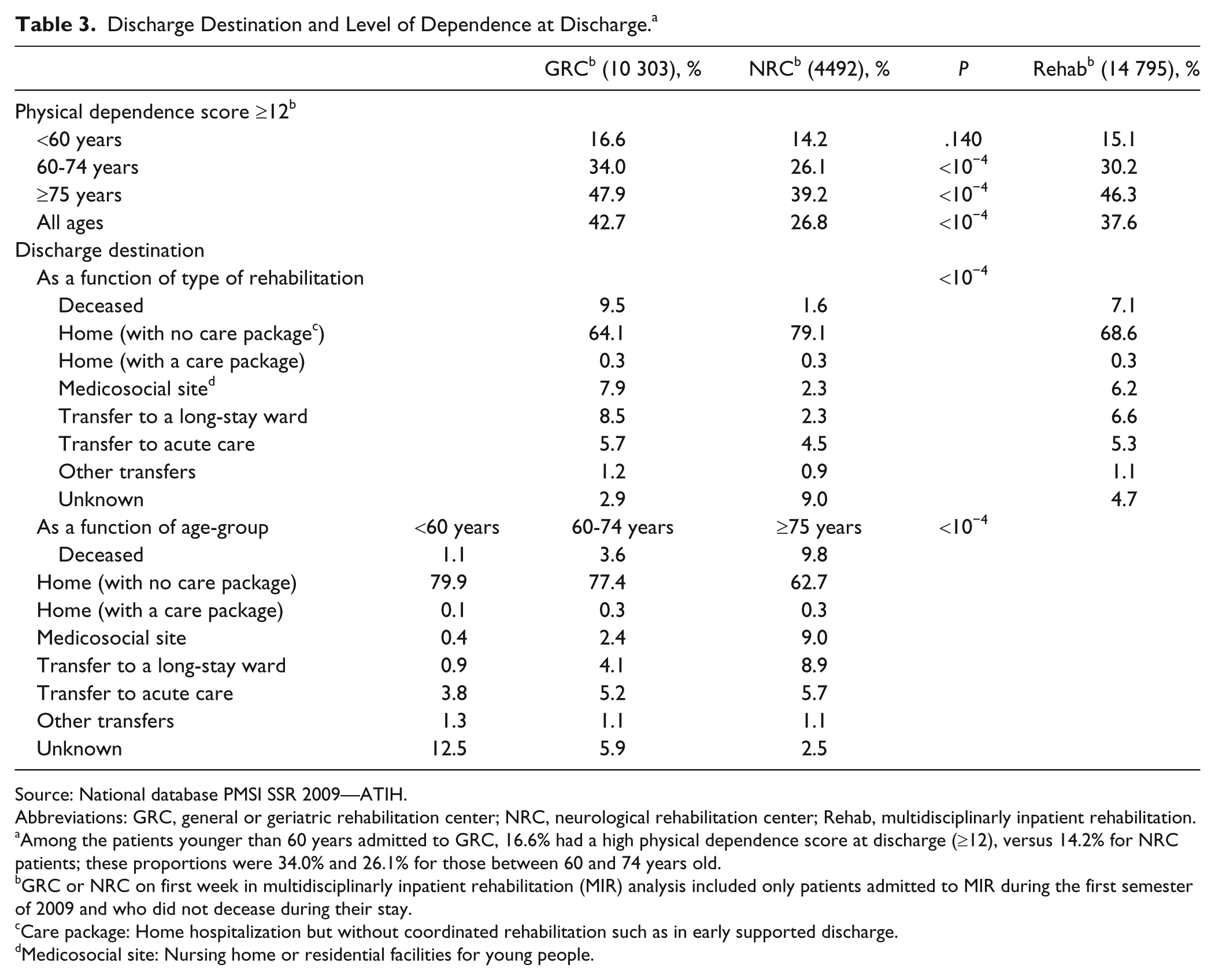
In all, 7.1% of patients died during rehabilitation. At discharge from rehabilitation, the frequency of patients with a high global physical dependence score (≥12) remained high. Of these patients, only 37.6% were still alive (Table 3). Global dependence score increased for 11% of patients, did not change for 36%, and decreased for 45.2%. An improvement of at least 4 points was found for 1 out of 5 patients. In all the age-groups, the frequency of patients who became less dependent was greater for NRC. The percentage of patients with a high global dependence score in NRC decreased from 50% on admission to 27% at discharge in contrast with 56% to 46% in GRC (data not shown).
Discharge Destination and Level of Dependence at Discharge. a
Source: National database PMSI SSR 2009—ATIH.
Abbreviations: GRC, general or geriatric rehabilitation center; NRC, neurological rehabilitation center; Rehab, multidisciplinarly inpatient rehabilitation.
Among the patients younger than 60 years admitted to GRC, 16.6% had a high physical dependence score at discharge (≥12), versus 14.2% for NRC patients; these proportions were 34.0% and 26.1% for those between 60 and 74 years old.
GRC or NRC on first week in multidisciplinarly inpatient rehabilitation (MIR) analysis included only patients admitted to MIR during the first semester of 2009 and who did not decease during their stay.
Care package: Home hospitalization but without coordinated rehabilitation such as in early supported discharge.
Medicosocial site: Nursing home or residential facilities for young people.
Significant differences between increases in independence depending on the type of rehabilitation received were found for each age group. For patients older than 75 years, there was an improvement in the total physical dependence score of 54.2 % for those in NRC and 35.8% for those in GRC.
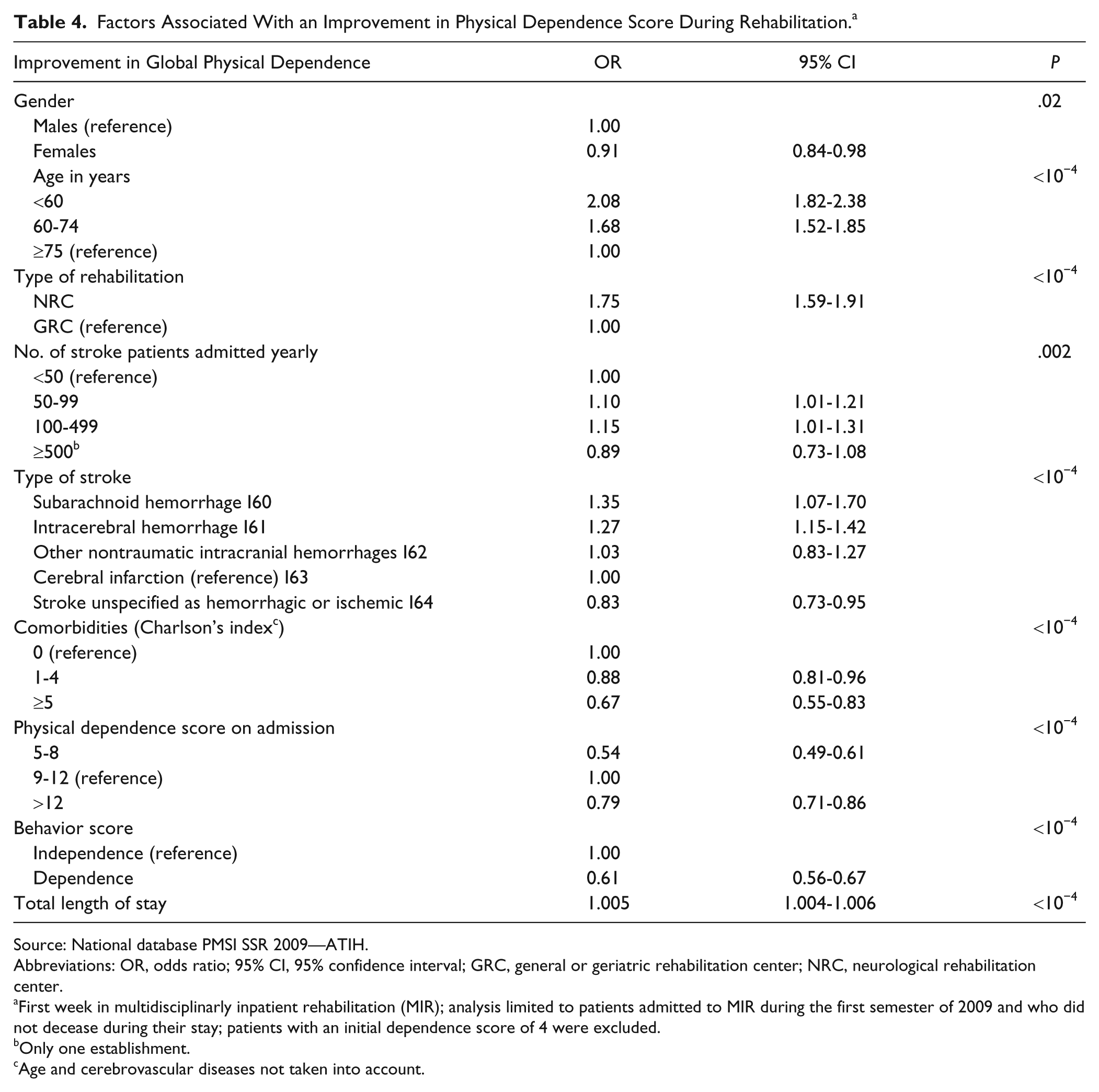
The multivariate analysis showed that certain sociodemographic criteria were related to a lower probability of recovery (Table 4): female gender and the presence of comorbid factors. A high level of physical dependence at admission for rehabilitation was also related to a poorer recovery as was a reduced behavior score.
Factors Associated With an Improvement in Physical Dependence Score During Rehabilitation. a
Source: National database PMSI SSR 2009—ATIH.
Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval; GRC, general or geriatric rehabilitation center; NRC, neurological rehabilitation center.
First week in multidisciplinarly inpatient rehabilitation (MIR); analysis limited to patients admitted to MIR during the first semester of 2009 and who did not decease during their stay; patients with an initial dependence score of 4 were excluded.
Only one establishment.
Age and cerebrovascular diseases not taken into account.
Recovery was more frequent in NRC (compared with GRC, odds ratio [OR] = 1.75, 95% confidence interval [CI] = 1.59-1.91) and in hospitals or clinics that admit between 50 and 500 stroke patients for rehabilitation per year.
Discharge Home Following Rehabilitation
Nearly 7 out of 10 patients were discharged home at the end of rehabilitation (Table 3). The multivariate analysis showed that older age reduced the probability of being discharged home (Table 5). There was an interaction between gender and age with a decreased OR for females compared with males after the age of 75 years (significant for the 75- to 84-year age-group). The presence of comorbid factors was also related to a lower probability of being discharged home, as was physical dependence and a poor behavior score.
Factors Related to Home Discharge. a
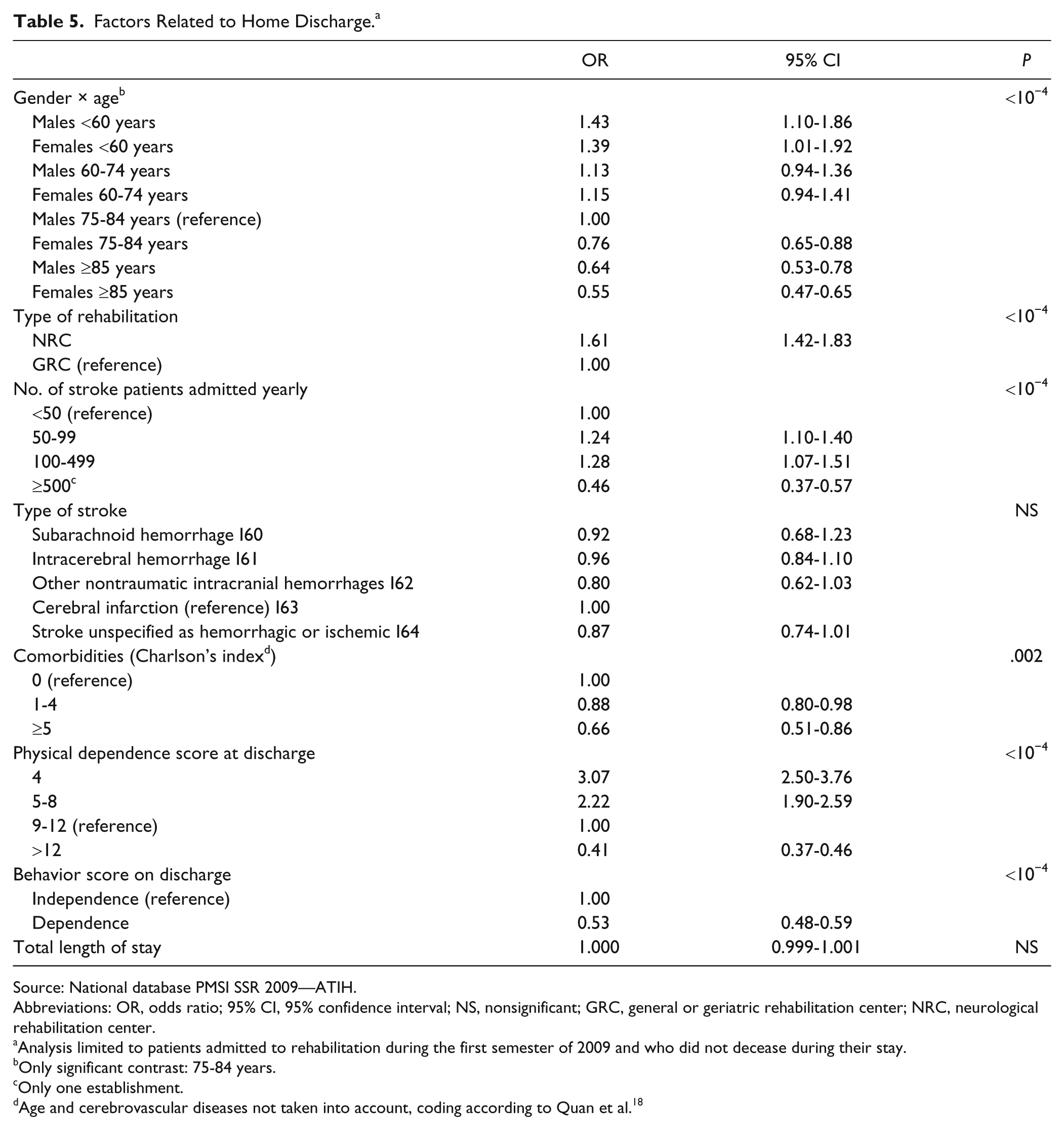
Source: National database PMSI SSR 2009—ATIH.
Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval; NS, nonsignificant; GRC, general or geriatric rehabilitation center; NRC, neurological rehabilitation center.
Analysis limited to patients admitted to rehabilitation during the first semester of 2009 and who did not decease during their stay.
Only significant contrast: 75-84 years.
Only one establishment.
Age and cerebrovascular diseases not taken into account, coding according to Quan et al. 18
Rehabilitation setting was also related to discharge with a greater frequency of home discharge following NRC compared with GRC (OR = 1.61, 95% CI = 1.42-1.83) and in rehabilitation centers (whatever the type) that admitted 50 to 500 stroke patients per year.
Mortality Rate During Rehabilitation
The proportion of patients who died after entry to rehabilitation was 7.1% and this proportion increased with age (9.8% of those older than 75 years). The multivariate analysis (not presented) showed that NRC significantly decreased the probability of death compared with GRC (OR = 0.298, 95% CI = 0.23-0.39)
Discussion
To our knowledge, this is the first study to evaluate the functional outcome of stroke patients admitted for rehabilitation following acute care based on a national sample of patients.
Changes in Level of Dependence
The results of this study showed that almost half of stroke patients were heavily dependent on admission for rehabilitation. A previous study showed that of all the patients admitted for rehabilitation (whatever the disease), post–acute stroke patients are the most dependent. 16
The percentage of patients who died during rehabilitation was 7.1%. This is a high percentage, which is close to that described in the literature.17,19
The percentage of poststroke patients who remained heavily dependent at discharge from rehabilitation was high (37.6%). The majority of these patients were discharged home. A recent declarative, cross-sectional study in the general French population reported that among those who declared having had a stroke with lasting sequelae, almost 1 in 2 was dependant for at least one activity of daily living (washing, dressing, or eating). 20 These data show that it is very important that discharge from rehabilitation should be well organized, particularly for patients who are discharged home. Care should be managed by coordinated teams such as Early Supported Discharge (ESD), 21 which involves visits from nurses and nursing auxiliaries. In 2009, only 0.3% of stroke patients received ESD. It seems important that ESD should be expanded to more patients and that it should also include rehabilitation.
NRC Versus GRC
In France, rehabilitation is carried out in 2 different settings: NRC (specialized, coordinated rehabilitation) and GRC (general or geriatric rehabilitation). The difference between the 2 is essentially administrative and some GRC that regularly take stroke patients are organized in a similar manner to NRC. This said, almost two thirds of the GRC stroke patients were hospitalized in GRCs that admitted less than 50 stroke patients per year. Therefore, we can consider that most of these patients received unspecialized rehabilitation.
With regard to functional outcome, patients have a greater chance of improvement and a greater chance of returning home if they receive rehabilitation in an NRC. In a recent study, Saposnik et al 14 showed that manner in which rehabilitation is coordinated is clearly related to outcome. The authors found that the number of patients needed to be treated in order to avoid one death or institutionalization at 30 days poststroke was equal to 9 in a comparison of coordinated rehabilitation with noncoordinated rehabilitation. Importantly, they found that this effect occurred regardless of age. This confirms the benefit of rehabilitation in NRC rather than GRC, which has already been demonstrated by many studies for all age-groups.
When data from NRC and GRC were pooled, the number of patients that a center admits annually had a large effect on patient outcome. This could be explained by the level of training and specialization of the medical, paramedical, and rehabilitation staff. It must be noted that only one center admitted more than 500 patients per year. However, this center consisted of a group of hospitals in the Paris region, which includes GRC and NRC as well as long-term care and therefore the results for this center cannot be interpreted.
Within NRC, the manner in which rehabilitation is coordinated affects progress and independence. The CERISE project recently compared outcomes following NRC rehabilitation in post–acute stroke patients in 4 European countries.22,23 The authors concluded that although all patients received specialized care, differences specific to each country (such as time spent in physiotherapy- or autonomy-centered time with nurses) had a direct effect on improvements. Thus in Switzerland and Germany where patients receive the most physiotherapy, improvements in motor capacity were greater than in the United Kingdom or in Belgium. In contrast, in the United Kingdom where, in addition to the physiotherapists and occupational therapists, the nursing staff also encourages independence, patients gained a greater level of independence in activities of daily living. These different studies demonstrate the importance of care in NRC for stroke patients and the present results further confirm this.
In a previous study, we showed that the criteria regarding the type of unit to which patients were admitted depended essentially on age, cognitive dependence, the number of NRCs in the area, and initial admission to a stroke unit.16,17 Because of the importance of the consequences, the rehabilitation pathway should be improved. Specialized care should be available for a larger number of patients. In order to achieve this, the criteria used in decisions regarding patient destination should be more standardized and NRC departments should be better organized and more numerous. This would enable a more systematic admission of poststroke patients to NRC.
Many reforms are currently underway in France to this end. 24 These reforms follow the national plan for the improvement of stroke care launched by the French Health Minister.
Greater specialization of GRC and NRC as well as more effective networks should improve recovery and rehabilitation of stroke patients.
Limitations
This study is based on national medico-administrative databases, which were quasi-exhaustive (estimation in 2009 at 99% for the PMSI MCO and 96% for the PMSI SSR). However, the quality of the data depends on the type of information system used and its medico-administrative nature; the information in these databases is based on the validity of the diagnostic coding and the variables that describe patient characteristics and their stays. The validity of the PMSI MCO for stroke and particularly its positive predictive value is not yet known in France. A national validation study is currently underway. Particularly, factors such as cognitive impairment and depression are not recorded in either the PMSI MCO or the PMSI SSR despite the fact that they may have an effect on recovery and influence decisions regarding the most appropriate care pathway for the patient.
Conclusion
This study is one of the first large studies in the world to carry out an exhaustive evaluation of the impact of rehabilitation on stroke. The results showed that a large number of heavily dependent patients were admitted for rehabilitation (most patients to GRC) and that physical dependence affected nearly 4 out of 10 patients at discharge. Despite this, most patients were discharged home at the end of their stay.
The importance of the rehabilitation setting on the functional outcome of post–acute stroke patients, their level of dependence and risk of death has already been reported in the literature but the present study confirmed this on a national level. In the context of the new stroke reforms in France, this information should be useful for the reorganization of rehabilitation, to ensure that patients are admitted to the appropriate type of rehabilitation setting, to improve discharge planning (more than one third of patients remain heavily disabled following rehabilitation) and to improve interaction between NRC and GRC.
Footnotes
Acknowledgements
We would like to thank Johanna Robertson for translating this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.