
Abstract
Background. Turning is a challenging task for stroke patients. Programs that effectively target turning, however, have not been established. Objective. This study examined the effects of a novel turning-based treadmill training on turning performance, gait symmetry, balance, and muscle strength in patients with chronic stroke. Methods. Thirty participants were randomly assigned to the experimental group that received 30 minutes of turning-based treadmill training or to the control group that received 30 minutes of regular treadmill training, followed by a 10-minute general exercise program for 12 sessions over 4 weeks. Primary outcomes (overground turning speed and temporal–spatial characteristics of straight walking) and secondary outcomes (balance and muscle strength) were assessed at baseline, after training, and at 1-month follow-up. Results. Fifteen participants per group were 54.2 ± 9.6 years old, poststroke 2.6 ± 1.9 years, and walked overground at 0.59 ± 0.28 m/s. Sixteen had an ischemic and 14 a hemorrhagic stroke. There were significant interaction effects between groups and time on turning speed regardless of turning direction, straight-walking performance (speed and temporal symmetry), strength of hip muscles and ankle dorsiflexors, and balance control (Berg Balance Scale, weight shifting in the forward direction and vestibular function). Compared with the control group, the experimental group showed greater improvements in these measures following training. These improvements persisted at the 1-month follow-up evaluation. Conclusions. Turning-based treadmill training may be a feasible and effective strategy to improve turning ability, gait symmetry, muscle strength, and balance control for individuals with chronic stroke.
Introduction
Gait recovery is critical for individuals who have suffered a stroke. 1 Approximately two thirds of stroke patients eventually walk with or without assistance. 1 However, many individuals still exhibit hemiplegic gait patterns and cannot achieve the walking dexterity required for all activities of daily living. Advanced gait training programs have therefore been emphasized in recent years, including dual-task training, 2 obstacle crossing in a virtual reality environment,3,4 and robotics-assisted practice of stair climbing. 5
Up to 40% of all steps taken in everyday walking are turns. 6 Turning requires the central nervous system to coordinate whole-body reorientation toward a new travel direction. 7 Balance maintenance during turning involves complex integration of multiple sensory systems (vestibular, visual, somatosensory) and motor output. 8 Moreover, there are increased medial–lateral impulses during turning as compared with straight walking. 9 The outer limb requires relatively greater activation of the ankle dorsiflexors during the swing phase and greater activation of the ankle plantar flexors during the stance phase to provide body propulsion. The inner limb requires increased extensor muscle activity to generate supportive action and to maintain whole-body stability in the stance phase. 10
Turning is often compromised in individuals with stroke and is one of the most frequent activities leading to falls within this population. 11 Following stroke, individuals demonstrate inadequate propulsion and weight shifting, along with insufficient extensor and ankle dorsiflexor strength.12-14 Abnormally large and disrupted sequences of gaze, head, and body motion because of deficits in sensorimotor integration have also been observed during turning. 15 Kobayashi et al 16 reported that patients with hemiplegia had difficulty walking along curvilinear paths. Recent studies also suggest that these patients turn more slowly because of the absence of kinematic and muscular modulations in the affected leg.17,18 Moreover, longer turn time were correlated with poor functional balance ability (indicated by Berg Balance Scale [BBS]) and temporal gait asymmetry. 17
As a result of these difficulties with turning, this activity has been indicated as a major target for gait rehabilitation. 19 Effective training programs specifically targeting turning characteristics, however, have not been established. Since motor learning involves repetition of desired movements (ie, specificity of training), “specific and repetitive” rehabilitation protocols that focus on turning may optimize turning-related outcomes. 20 We therefore hypothesized that a novel treatment—turning-based treadmill training—would lead to greater improvement in turning performance as compared with regular treadmill training in subjects with chronic stroke. In addition, as turning requires side-specific muscle modulation of the lower limbs and medial–lateral balance control, 18 we hypothesized that the turning-based treadmill training would improve gait symmetry during straight walking, muscle strength of the lower extremities and standing balance.
Methods
Participants
Participants with chronic stroke were recruited from medical centers and the surrounding community. Stroke diagnosis, age, gender, stroke type, lesion side, and duration of hemiparesis were obtained from patient interviews and medical charts. To be included in the study, participants with stroke had to satisfy the following criteria: (a) 6 months post first-ever stroke with unilateral motor deficits, (b) the ability to walk independently for at least 6 m with or without use of walking aids (to ensure they were able to complete the 5-m walk test used in the current study), (c) a Brunnstrom stage of affected lower extremity greater than 3, and (d) the ability to follow verbal instructions. Exclusion criteria were (a) unstable medical conditions (eg, deep vein thrombosis, aspiration pneumonia, or superimposed sepsis) and (b) history of other diseases known to interfere with participation in the study (eg, heart failure, hemi-neglect, or diabetic neuropathy).
Experimental Design
The study was a single-blind randomized controlled trial. An individual unassociated with any other study procedure selected one of a set of sealed envelopes to assign participants to either the experimental or control group (block randomization) before the intervention began. Participants received 30 minutes of turning-based treadmill training (experimental group) or regular treadmill training (control group), followed by a 10-minute general exercise program, for 12 sessions over a 4-week period. All outcomes were measured the day before intervention (pre), the day after completing the intervention (post), and the 30th day after completing the intervention (follow-up) by a physical therapist blinded to group assignment. Study outcomes (see below) were related to turning, walking, standing balance, and muscle strength of the affected lower extremity. During each assessment, the use of walking aids was allowed for safety. If a patient used a walking aid at the preintervention assessment, the same aid was used at the post and follow-up assessments to minimize potential bias. Participants provided written informed consent of all study procedures, which were approved by the institutional review board of Taipei City Hospital (TCHIRB-1000609).
Interventions
Turning-based treadmill training
A rotational treadmill (Rmax Science & Technology Co, Ltd, New Taipei City, Taiwan; Figure 1A) was designed to provide turning-based treadmill training. This treadmill is similar to a regular treadmill except for its circular running motor belt (0.8-m radius), which forces patients to continually turn rather than walk straight. The circular belt rests on a base of the same size secured to the floor. Available treadmill speeds ranged from 0.15 to 2.80 m/s. Safety features included front and side handrails around the walking area, a harness connected to an overhead suspension system, and an emergency stop button located on the side handrail.
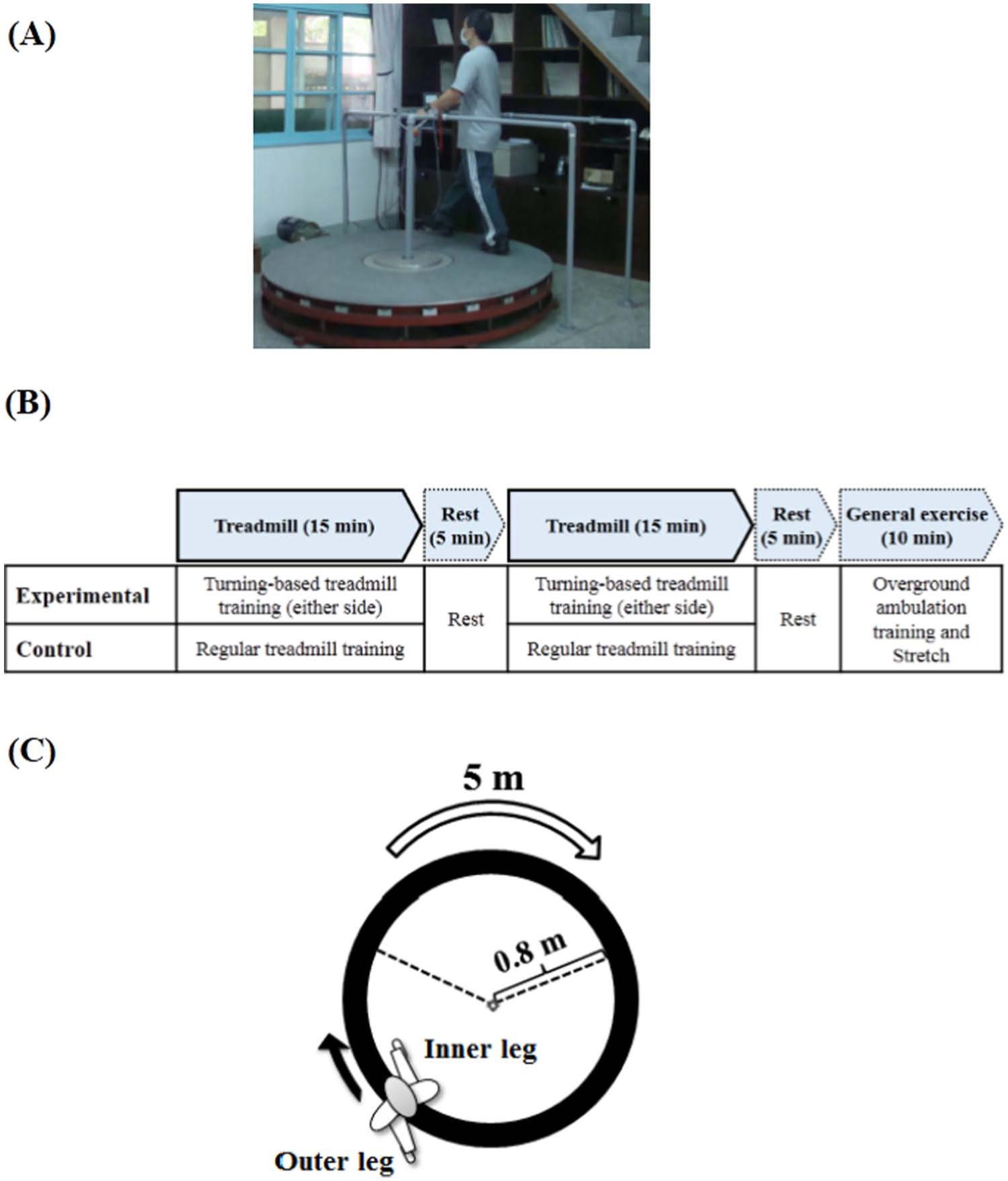
(A) Turning-based treadmill training on the rotational treadmill. (B) The training schedule of one session in experimental (upper) and control (below) groups (C) Schematic of the walkway used for turning performance.
Participants walked on the perimeter of the circular belt as it rotated either clockwise or counterclockwise. Participants were trained in both directions, with the affected leg as the inner limb for 15 minutes and then as the outer limb for 15 minutes with a 5-minute break in between. The order of walking with affected limb as the inner or outer leg was alternated in each consecutive session. During each training session, an experienced physical therapist encouraged participants to walk with large strides and upright posture. All participants wore an unweighted safety harness to prevent falls. Participants were also allowed to place their hands on the handrail for balance support but were instructed to refrain from holding the handrail. They were also allowed use of lower extremity orthoses if needed. As progressively faster speeds are needed to continue challenging the locomotor abilities of individuals with hemiparesis, 21 the treadmill speed, which began as each individual’s comfortable turning speed on level ground, was increased by increments of 0.05 m/s every 5 minutes as tolerated. Additionally, as the speed of turning toward the affected and unaffected side may differ, 17 training speed was progressed individually for each direction. The criteria for increasing speed was determined by the ability to remain an upright posture and a perceived exertion of “somewhat hard” or lower (ie, a Borg rating of perceived exertion <13). 22 Training speed in a given session was started with the fastest speed obtained during the previous session.
The participant was informed of potential discomforts and adverse effects (ie, musculoskeletal soreness, dizziness, or fall) prior to each training session. The training was immediately stopped if the participant reported any discomfort. A 5-minute rest after completing the treadmill training was allowed. After the rest, a 10-minute general exercise program, including overground ambulation training to assist skill transfer, was performed. This training included both straight walking and turning, and verbal cues were provided as necessary for gait correction. Lower extremity stretching was then performed for cool-down purposes (Figure 1B).
Regular treadmill training
The control group received training on a standard treadmill (Biodex, Shirley, NY). Other than the type of treadmill, the training protocol was the same as that described for the experimental group. Training speed was initially set at the individual’s comfortable walking speed on level ground and increased by increments of 0.05 m/s every 5 minutes. Participants were trained in two 15-minute phases, followed by a 10-minute general exercise program similar to the experimental group.
Outcome Measures
Primary outcomes
Turning performance was assessed during a walk along the circumference of a 5-m curved path with radius of 0.8 m (Figure 1C) toward the affected (affected leg as the inner leg) and unaffected (unaffected leg as the inner leg) side. 23 Participants were asked to perform the turn at a comfortable speed 3 times in each direction in random order. The time needed to complete the curved path was recorded, and the average of 3 trials was used for data analysis. Average speed was derived from dividing the distance by the time. The intrarater reliability for turning speed was .98 toward the left side and .99 toward the right side of healthy adults in our pilot study.
The speed and temporal–spatial parameters of comfortable-speed straight walking were obtained from the GAITRite system (CIR system, Inc, Havertown, PS), which contains pressure-sensitive sensors. The walkway was 4.75 m long and 0.9 m wide, and the pressure-sensitive area was 4.30 m long and 0.61 m wide. The contact time and location of each footfall were recorded and analyzed on a laptop with application software for calculation of temporal–spatial parameters. The concurrent validity in healthy subjects 24 and the reliability in stroke subjects 25 of the GAITRite system have been established. Gait parameters of interest were walking speed, cadence, and stride length. The average of three trials was used for data analysis. In addition, the temporal and spatial asymmetry ratios were calculated using the following formulas 26 :


Secondary outcomes
The BBS consists of 14 functional tasks commonly performed in daily life. It addresses 2 dimensions of balance: the ability to maintain upright posture, such as standing unsupported, and to make appropriate adjustments for voluntary movement, such as a 360° turn. Higher scores (maximum = 56) indicate better balance. The scale is a valid and reliable tool for evaluating balance recovery in the stroke population. 27 In this study, the score of one item, the 360° turn, was also analyzed separately as it was closely related to our primary outcome of turning.
Standing balance was assessed by the limits of stability (LOS) and Sensory Organization Test (SOT; Balance Master, NeuroCom International, Inc, Clackamas, OR). The LOS test quantifies the maximum distance a person can voluntarily displace their center of gravity in space toward a target direction. 28 Four directions (forward, backward, nonaffected side, and affected side) were assessed in random order. For each direction, reaction time was defined as the time in seconds between the command to move and the subject’s first movement, and endpoint excursion was defined as the distance of the first movement toward the targeted direction, expressed as a percentage of maximum distance (100% of theoretical LOS). Shorter reaction time and greater endpoint excursion indicated better balance control toward each direction. The SOT assesses 3 sensory components (vision, somatosensory, and vestibular) of standing balance under 6 different visual and support-surface conditions. 29 Based on these individual tests, an overall equilibrium score was calculated based on the amount of sway during a 20-second SOT trial. A score of 100 indicates no sway, whereas 0 indicates sway beyond the theoretical LOS.
Lower extremity muscle strength was evaluated using a handheld dynamometer (Power Track II, Jtech Medical Industries, Inc, Herber City, UT). The strength of hip flexors/extensors/abductors, knee flexors/extensors, and ankle dorsiflexors/plantar flexors were tested. The “make” test method was used whereby the examiner held the handheld dynamometer stationary while the subject exerted a maximal force against it.26,30 The testing position for each muscle followed standard protocols.30,31 For each muscle, the maximum force produced during each of three 5-second contractions were averaged and used for analysis.
Statistical Analysis
All analyses were performed using the SPSS 17.0 statistical software. Descriptive statistics were generated and distributions of variables were expressed as mean ± standard deviation. Intergroup differences among baseline characteristics were evaluated using an independent t test or χ2 analysis. Two-way analysis of variance with repeated measures was used to determine the effects of intervention on each dependent variable. Model effects were group (experimental, control), time (pre, post, follow-up), and their interaction. Post hoc pairwise comparisons between pre- and postintervention in each group, and independent t test between groups, were used to examine significant models. To detect the retention or loss of treatment effects at follow-up evaluation, post hoc pairwise comparisons were further used to examine outcomes at 1-month follow-up as compared with the initial posttraining assessment. Statistical significance was set at .05.
Results
Fifteen participants in the experimental group and 15 participants in the control group completed all assessments and treatment sessions (Figure 2). One subject in the experimental group and one subject in the control group reported musculoskeletal soreness after one session, but the soreness did not persist more than 48 hours. Three subjects in the experimental group and 2 subjects in the control group reported dizziness when intervention was started in the first session. The symptom disappeared within 5 minutes and did not interfere with their participation. No other adverse effects were reported or noted. There were no significant differences in baseline demographic or clinical features between the groups (Table 1). Similarly, there were no significant group differences in any of the preintervention primary or secondary outcome measures (Tables 2 and 3).
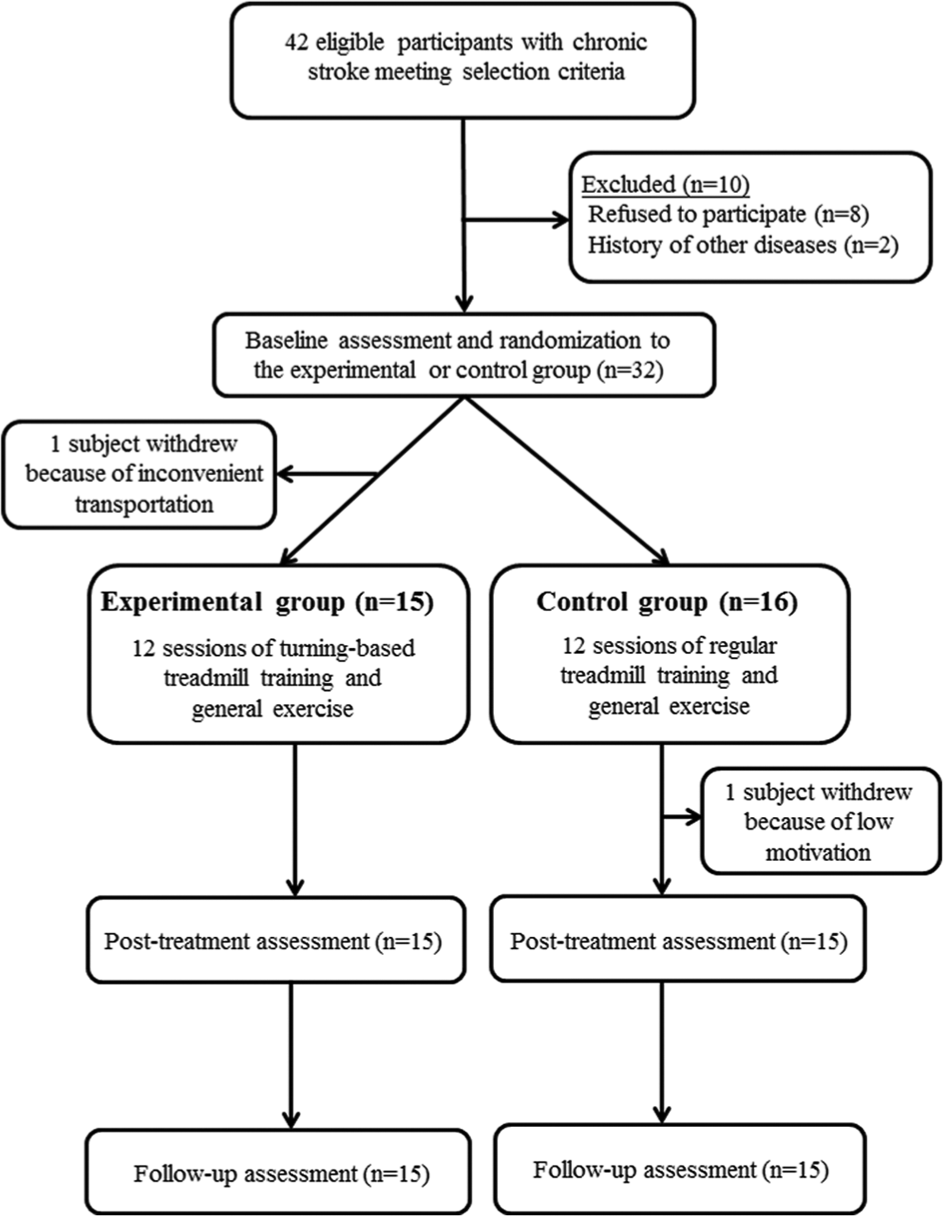
Flowchart of participants recruited in this study.
Baseline Demographic and Clinical Characteristics of Participants. a
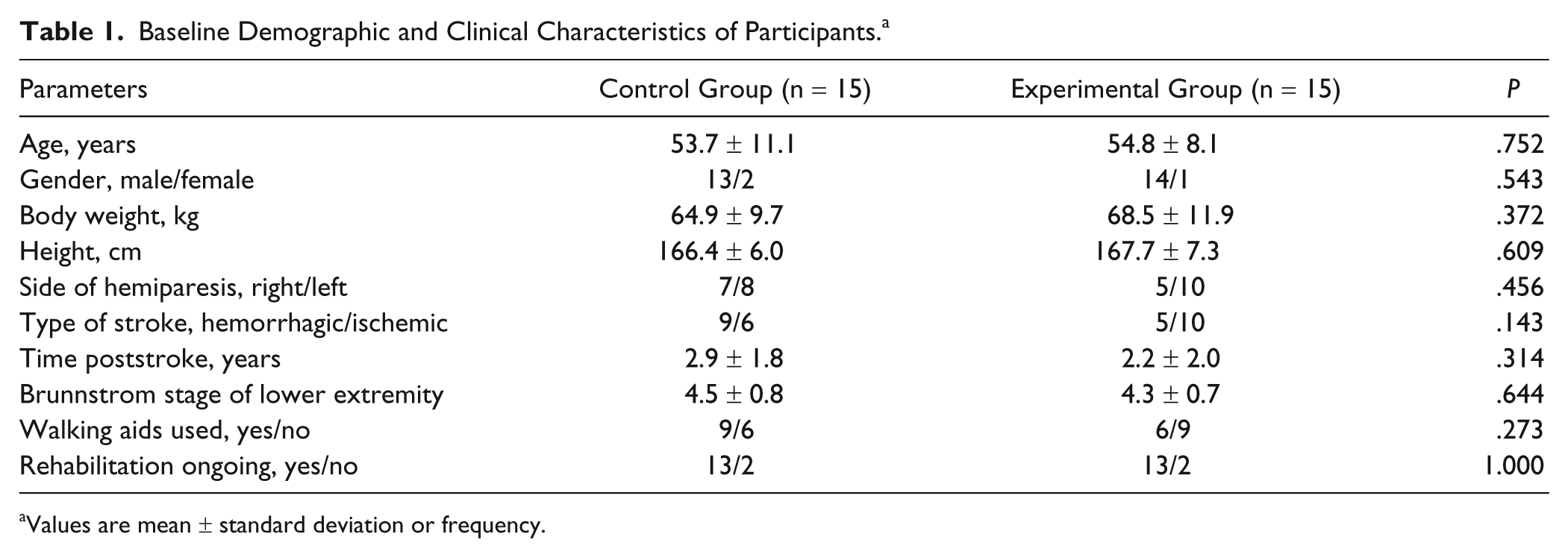
Values are mean ± standard deviation or frequency.
Gait Performance.
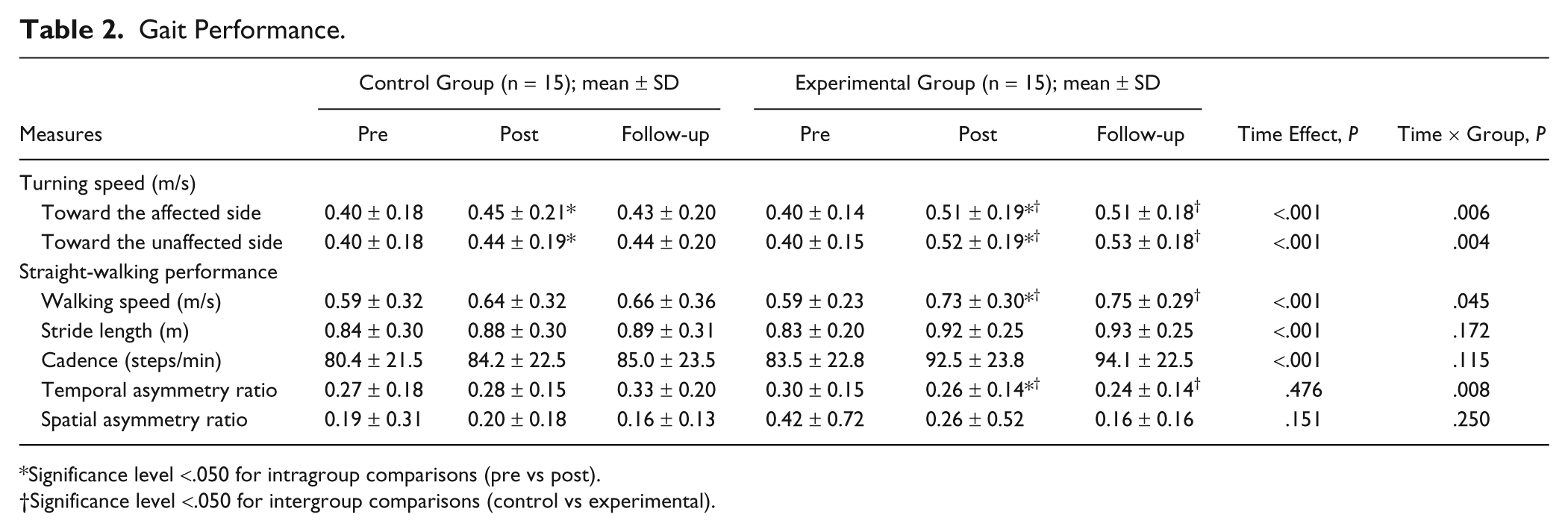
Significance level <.050 for intragroup comparisons (pre vs post).
Significance level <.050 for intergroup comparisons (control vs experimental).
Balance Performance and Muscle Strength.
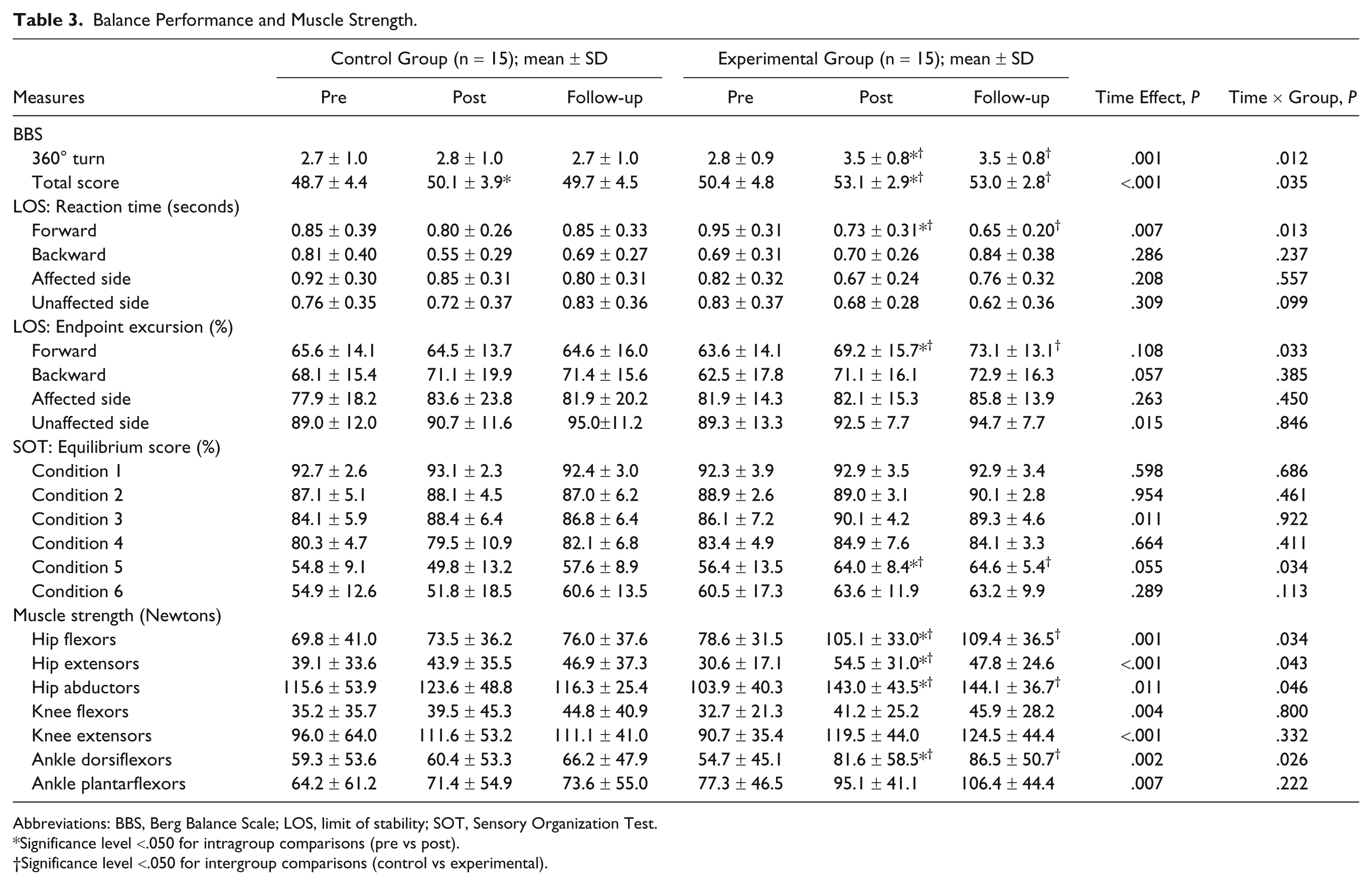
Abbreviations: BBS, Berg Balance Scale; LOS, limit of stability; SOT, Sensory Organization Test.
Significance level <.050 for intragroup comparisons (pre vs post).
Significance level <.050 for intergroup comparisons (control vs experimental).
Treadmill Speed
The mean training speed was increased from 0.57 ± 0.32 to 0.89 ± 0.36 m/s in the control group during the 4-week treatment period. In the experimental group, the mean training speed was increased from 0.45 ± 0.17 to 0.81 ± 0.24 m/s for turning toward the affected side and from 0.47 ± 0.13 to 0.82 ± 0.24 m/s for the unaffected side during the 4-week treatment period. The initial and the final treadmill speeds were similar between groups.
Primary Outcomes
Significant interactions (P < .006) between group and time were present for turning speed toward both sides (Table 2). Post hoc analysis revealed that both groups improved turning speed toward the affected (control, P = .024; experimental, P < .001) and unaffected sides (control, P = .005; experimental, P = .001) after training, but the improvement was greater in the experimental group (affected side, P = .029; unaffected side, P = .007; Figure 3). For each group, turning performance was similar at the follow-up assessment compared with the posttraining assessment.
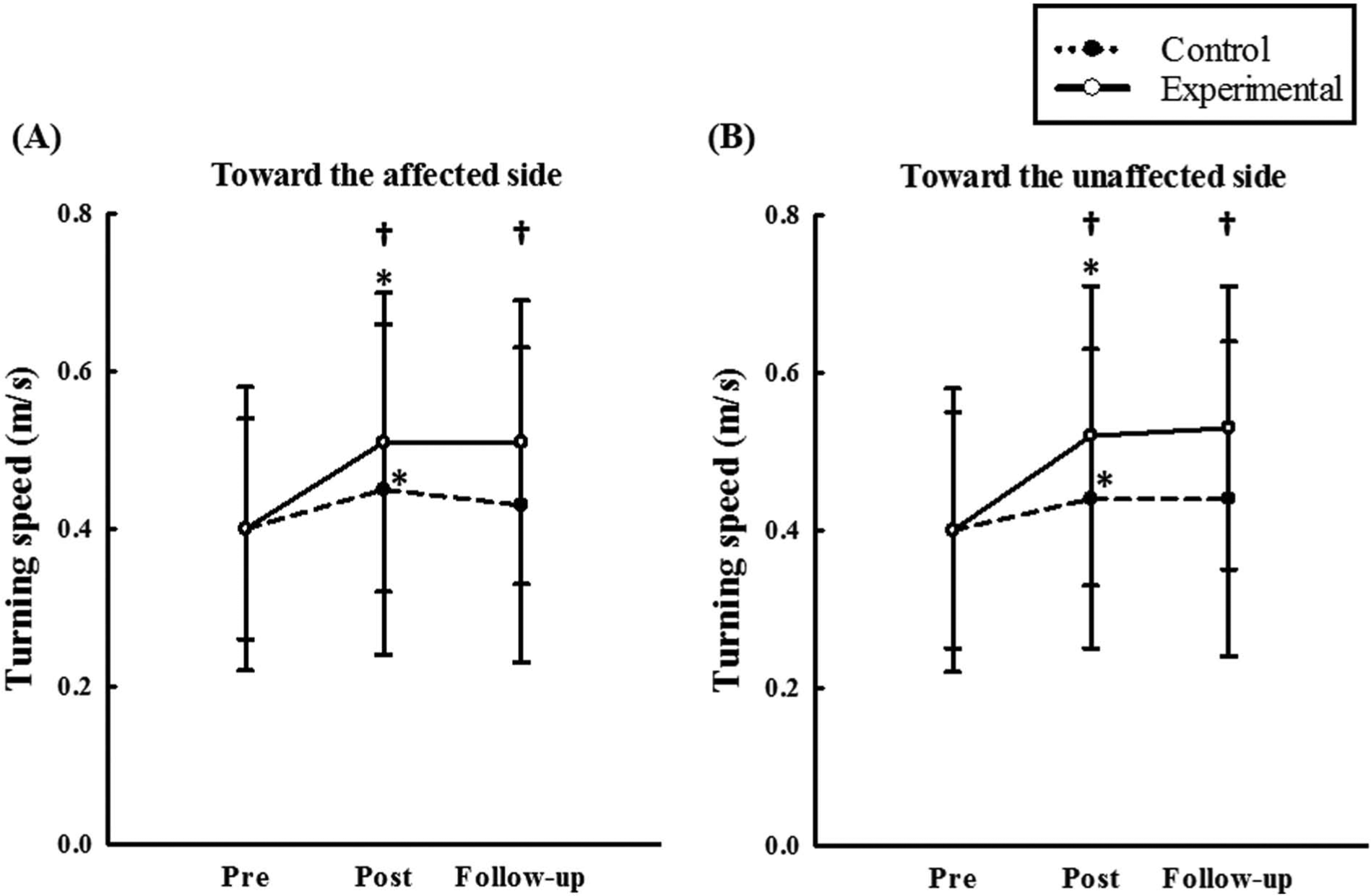
Turning speed toward the affected side (A) and the unaffected side (B). Both groups improved turning speed toward both the affected and unaffected sides after training, but greater improvements were observed in the experimental group (affected side, P = .029; unaffected side, P = .007). The improvements at posttraining were retained at follow-up in the experimental group.
Significant main effects (P < .001) of time were observed for stride length and cadence (Table 2). Specifically, stride length was longer and cadence was faster at the posttraining assessment compared with the pretraining assessment. Group by time interactions (P < .045) occurred for both walking speed and the temporal asymmetry ratio. As compared with the control group, the experimental group demonstrated greater improvements in walking speed (P = .036) and temporal asymmetry ratio (P = .044). For each group, walking speed and the temporal asymmetry ratio were similar at the follow-up compared with the post-training assessment.
Secondary Outcomes
Significant main effects of time (P < .015) were observed for the endpoint excursion of LOS toward the unaffected side and the equilibrium score of the SOT in condition 3 (sway-referenced vision, fixed support; Table 3). Specifically, the endpoint excursion of LOS toward the unaffected side was greater and the equilibrium score of the SOT in condition 3 was higher at the posttraining assessment as compared with pretraining assessment. Group by time interactions (P < .035) were observed for BBS, 360° turn, LOS reaction time, LOS endpoint excursion in the forward direction, and the SOT equilibrium score in condition 5 (absent vision, sway-referenced support). As compared with the control group, the experimental group demonstrated greater improvement in each outcome (ie, 360° turn, P = .003; reaction time of LOS, P = .045; endpoint excursion of LOS, P = .038; equilibrium score of SOT, P = .036). The improvements in the BBS were noticed in both groups (control, P = .001; experimental, P < .001) with greater improvement in the experimental group (P = .048). Within each group, all improvements made at posttraining were retained at follow-up.
Significant main effects (P < .011) of time were also observed for muscle strength in all muscles evaluated (Table 3). Significant group by time interactions (P < .046) were present for strength of the hip flexors, hip extensors, hip abductors, and ankle dorsiflexors. As compared with the control group, the experimental group demonstrated greater improvement for each outcome (ie, hip flexors, P = .037; hip extensors, P = .027; hip abductors, P = .032; ankle dorsiflexors, P = .007). Within each group, all improvements made at posttraining were retained at follow-up.
Discussion
The main finding of this study was that 12 sessions of a 30-minute turning-based treadmill program was more effective than the regular treadmill program for improving turning speed, regardless of turning direction, in people with chronic stroke. These improvements in turning performance were also accompanied by concurrent increases in muscle strength, balance control, and straight-walking performance. These improvements persisted at 1-month follow-up.
Treadmill training is an effective treatment for enhancing walking speed in people who have suffered a stroke. 20 We therefore included the principles of motor learning and brain reorganization, including repetition of desired movements and training specificity, in our program designed for turning training. The turning speeds of our patients at the pretreatment evaluation were comparable to previous reports. 32 In the present study, turning-based treadmill training resulted in a 26% and 28% increase in turning speed toward the affected and unaffected side, respectively. To our knowledge, evidence-based interventions designed to improve turning speed in individuals with stroke are unavailable. Since turning speeds were reported as 1.2 ± 0.2 and 0.9 ± 0.2 m/s in young and older healthy adults, respectively, 23 turning-based interventions with longer duration, higher frequency, or greater numbers of sessions may lead to even faster turning speeds in subjects with stroke. Moreover, the relationship between turning speed and poststroke fall incidence has not yet been established. The fall incidence/risk after increasing the turning speed warrants further study, especially for stroke patients with fall history.
Compared with regular treadmill training, turning-based treadmill training was more effective at improving standing balance, as evidenced by shorter reaction time in the LOS test and increased body excursion during voluntary weight shifting in the forward direction. Successfully shifting weight forward is a prerequisite for the control of both linear and curvilinear walking. Through improvements in dynamic balance control, also demonstrated by the BBS, improvement in walking speed was noted in addition to turning performance. The 360° turn, one of the tasks in the BBS, was also improved significantly more after the turning-based training than after the regular treadmill training. Future study is therefore warranted to examine if balance improvements associated with turning-based treadmill training influence recovery of independent walking in nonambulatory subacute stroke.
Interestingly, no training-related improvements were observed in the ability to shift one’s weight toward the affected side. In another study using Tai Chi as a balance intervention, chronic stroke patients improved weight-shifting toward the affected side after 12 weeks of training, and improved weight shifting in the forward direction after only 6 weeks. 33 Although Tai Chi includes more sensorimotor component than turning-based treadmill training, the results from that study also suggest that longer practice time may be required to increase weight-shifting ability. Further studies are needed to investigate whether increasing the duration of training with the affected limb as the inner limb could result in greater improvements of weight shifting toward the affected side based on the obligate nature of the inner limb during turning.
Stroke patients often have impaired vestibular sensation and are therefore more dependent on visual feedback for standing balance. 34 After turning-based treadmill training, subjects demonstrated increased SOT equilibrium score in condition 5. In this situation, subjects are forced to use vestibular feedback to maintain balance, as vision is deprived and somatosensory information is distorted. Prior to turning, an increase in the weighting of vestibular inputs is required to prepare for the ensuing change in direction. 35 As such, improved utilization of vestibular feedback, together with somatosensory inputs (although improvements were not significant in our study), following turning-based training would be expected to result in better turning performance.
Straight-walking cadence and stride length increased in both groups. Improvement of temporal symmetry, however, was only noted following turning-based treadmill training. These results are supported by a previous report in patients with chronic brain damage due to stroke. 36 Moreover, turning speed has been linked to the degree of gait asymmetry 17 and the kinematics and electromyographic patterns of turning shown in healthy individuals are not observed in the affected leg in individuals with stroke. 18 Through relearning of the motor patterns in our turning training, asymmetric gait pattern can be improved. Moreover, both hip flexor and ankle dorsiflexor strength play a role in gait velocity and temporal asymmetry during walking after stroke.26,37 Hip extensors are important for weight transference onto the contralateral leg while hip abductors are important for medial–lateral stability during gait. The strength improvements observed in these muscle groups may therefore underlie the superior gait performance after turning-based training. Still, turning-based treadmill training was not superior with regard to improving knee extensor and ankle plantarflexor strength. Previous studies have indicated that regular treadmill training improves strength of these muscles in chronic stroke patients.38,39 Low reliability of handheld dynamometry for the assessment of knee extensor strength in healthy subjects has been reported, 40 which is believed to be caused by insufficient examiner’s strength. Interpretation of results with respect to knee extensors strength should therefore be considered with caution.
As compared with regular treadmill training, turning-based treadmill training resulted in greater improvements in straight-walking performance. This result is somewhat surprising, as it seems to contradict the theory of training specificity. However, the process of motor learning is complicated. Individuals with chronic stroke maintain the capacity to enlarge the cortical representation of lower extremities in response to training, yet cortical excitability is lower than those with shorter post-onset duration. 41 A challenging and more difficult task that was previously unfamiliar and relatively new, however, may increase the possibilities of brain activation to generate behavioral recovery. 42 Turning is a task finely modulated from the basic pattern underlying straight-walking, as it requires more balance maintenance and limb coordination. 43 Walking on a rotational treadmill is unfamiliar and subjects may pay relatively more attention during this intervention. Such innovative and challenging tasks may therefore increase motivation, stimulate coordinated muscle activity, and induce cortical reorganization resulting in better walking performance. Exploration of the specific neuromuscular modulations during turning and the effects of task difficulty on neural plasticity would further elucidate the mechanisms of these positive results.
As demonstrated by 1-month follow-up data, participants retained positive training effects on turning speed, straight-walking performance (speed and asymmetry), standing balance, vestibular function and muscle strength. These positive effects after intervention and at follow-up suggest that the presented turning-based treadmill training program should be recommended to enhance long-term functional mobility in individuals with chronic stroke.
Limitations
As this study is the first study to examine the effects of turning-based treadmill training in the stroke population, we only recruited ambulatory patients. We thus cannot generalize our findings to other populations. For safety concerns, several patients used walking aids and/or orthoses during the assessments and intervention. Although the intergroup differences in the use of walking aids at baseline did not show statistical differences, the interpretation of gait improvements needs to consider possible beneficial effects of walking aids. 44 Another limitation is the relatively high number of study outcomes relative to cohort size. However, the partial η2 for each outcome was .10 to .19, meaning that the effect sizes of outcome were medium (partial η2 = .06) to large (partial η2 = .14). 45 Although our study indicates potential benefits of turning-based training, intergroup differences on gait and balance did not exceed reported minimal detectable change.46,47 The determination of optimal parameters for turning-based treadmill training is needed in future studies. The effects of overground turning-based training should also be explored.
Conclusions
Our results indicate that the turning-based treadmill training is a feasible and effective intervention to improve turning ability, gait symmetry, muscle strength, and balance control in subjects with chronic stroke. A further prospective study on the changes in neuromuscular modulations and fall incidence with a larger group of stroke subjects using this turning-based treadmill training may be of clinical and socioeconomic significance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Support for this study was provided by the National Health Research Institutes of the Republic of China (Grant No. NHRI-EX100-10039EI, NHRI-EX101-10039EI).