
Abstract
Background. Although a growing body of evidence has highlighted the role of cognitive rehabilitation (CR) in the management of cognitive dysfunctions in multiple sclerosis (MS), there is still no evidence for a validated therapeutic approach. Objective. We propose a new therapeutic strategy characterized by a computer-based intensive attention training program in MS patients with predominant attention deficits. We aim to investigate the effectiveness of our rehabilitation procedure, tailored for those with impaired abilities, using functional magnetic resonance imaging (fMRI). Methods. Using a double-blind randomized controlled study, we enrolled 12 MS patients, who underwent a CR program (experimental group), and 11 age-gender–matched MS patients, who underwent a placebo intervention (control group). fMRI was recorded during the execution of a cognitive task broadly used for assessing attention abilities in MS patients (paced visual serial addition test). Results. Significant effects were detected both at a phenotypic and at an intermediate phenotypic level. After CR, the experimental group, in comparison with the control group, showed a specific enhanced performance in attention abilities as assessed by the Stroop task with an effect size of 0.88, which was associated with increased activity in the posterior cerebellar lobule and in the superior parietal lobule. Conclusions. Our study demonstrates that intensive CR tailored for those with impaired abilities affects neural plasticity and improves some aspects of cognitive deficits in MS patients. The reported neurophysiological and behavioral effects corroborate the benefits of our therapeutic approach, which might have a reliable application in the clinical management of cognitive deficits in MS.
Introduction
Cognitive dysfunction, which is reported in 40% to 60% of relapsing-remitting (RR) multiple sclerosis (MS) patients,1,2 has been shown to negatively affect various aspects of cognitive function, including attention, information processing abilities, learning, and memory function. 3 Moreover, cognitive impairments are associated with reduced functional status in MS. 1 Pharmacological treatments4,5 have been investigated as remedial treatments for cognitive dysfunctions in people with MS. Besides pharmacological treatments, there is a role for nonpharmacological interventions such as cognitive rehabilitation (CR).6-12 CR techniques are designed to either restore functions or develop strategies to compensate for cognitive dysfunction. Research on the management of cognitive dysfunction in MS patients has been limited. However, in the past few years, some studies have evaluated symptomatic treatments for cognitive dysfunction in MS, and some of the results have been promising.6-8,11 The few existing CR programs within MS have been aimed at improving attention deficits8,11,12 and memory function.6,7,9,10 Although some studies exist that show a benefit from CR for persons with MS, others9,10,12 have failed to show a clear benefit. As a result, researchers and clinicians experience difficulty in drawing firm conclusions regarding effectiveness. 13 However, a major limitation in applying CR to restoring cognitive resources in MS patients might be that not all cognitive dysfunctions benefit from CR. This is because of the fact that cognitive functions affected in the MS population are widespread, involving memory, attention, language, and executive functions. Thus, the selection of homogeneous patient populations (in terms of clinical disability and limited cognitive impairment) and tailored rehabilitative strategies play a crucial role in the decision-making process for rehabilitation programs in MS.
Given the limitations of CR discussed above, the present study is aimed at determining the impact of a specific intervention to improve or restore impaired attention functions in RR-MS patients with predominant attention deficits. The idea of a neurorehabilitation program tailored to a specific cognitive deficit affecting MS patients restricts sample selection but, otherwise, eliminates potential confounders linked to the presence of additional cognitive impairments (that are characteristic of patients with severe cognitive impairments) and thus helps with the interpretation of the results. We examined the effects of our CR approach in restoring attention abilities both at a phenotypic level (by means of neuropsychological performance) and at an intermediate phenotypic level by using functional magnetic resonance imaging (fMRI), which represents a very sensible tool to explore subtle active processes of neuroplasticity that might be driven by CR.
Methods
Participants
We enrolled all patients who met the criteria for clinically definite RR-MS, recruited at the Department of Neurology, University “Magna Graecia” of Catanzaro. From an initial cohort of 117 RR-MS patients, we enrolled only those patients who fulfilled the following criteria: (1) no evidence of a severe cognitive impairment as evaluated by a detailed neuropsychological assessment (see the section “Neuropsychological Assessment”); (2) MS patients with predominant deficits in either attention and/or information processing speed, working memory, and/or executive functioning (ie, failure in at least 1 of the following tests: symbol digit modality test (SDMT), trial making test (A-B), paced auditory serial addition test (PASAT), and Stroop word-color task [ST]); (3) no additional impairment in other cognitive domains (ie, language, verbal, and spatial memory); (4) no clinical relapses and steroid treatment for at least 1 month prior to study entry; (5) no concomitant therapy with antidepressant or psychoactive drugs; (6) Expanded Disability Status Scale 14 score ranging from 0 to 4; (7) no history of psychiatric problems, according to the structured clinical interview of the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th ed) 15 ; and (8) optimal visual acuity. The clinical assessment also included the Fatigue Severity Scale. 16 From the initial cohort (n = 117 RR-MS patients), 26 MS patients were selected for the rehabilitation program (Figure 1). Sociodemographic data, neurological data, and written informed consent (approved by the ethical committee of the University “Magna Graecia” of Catanzaro) were collected from all participants enrolled in the study.
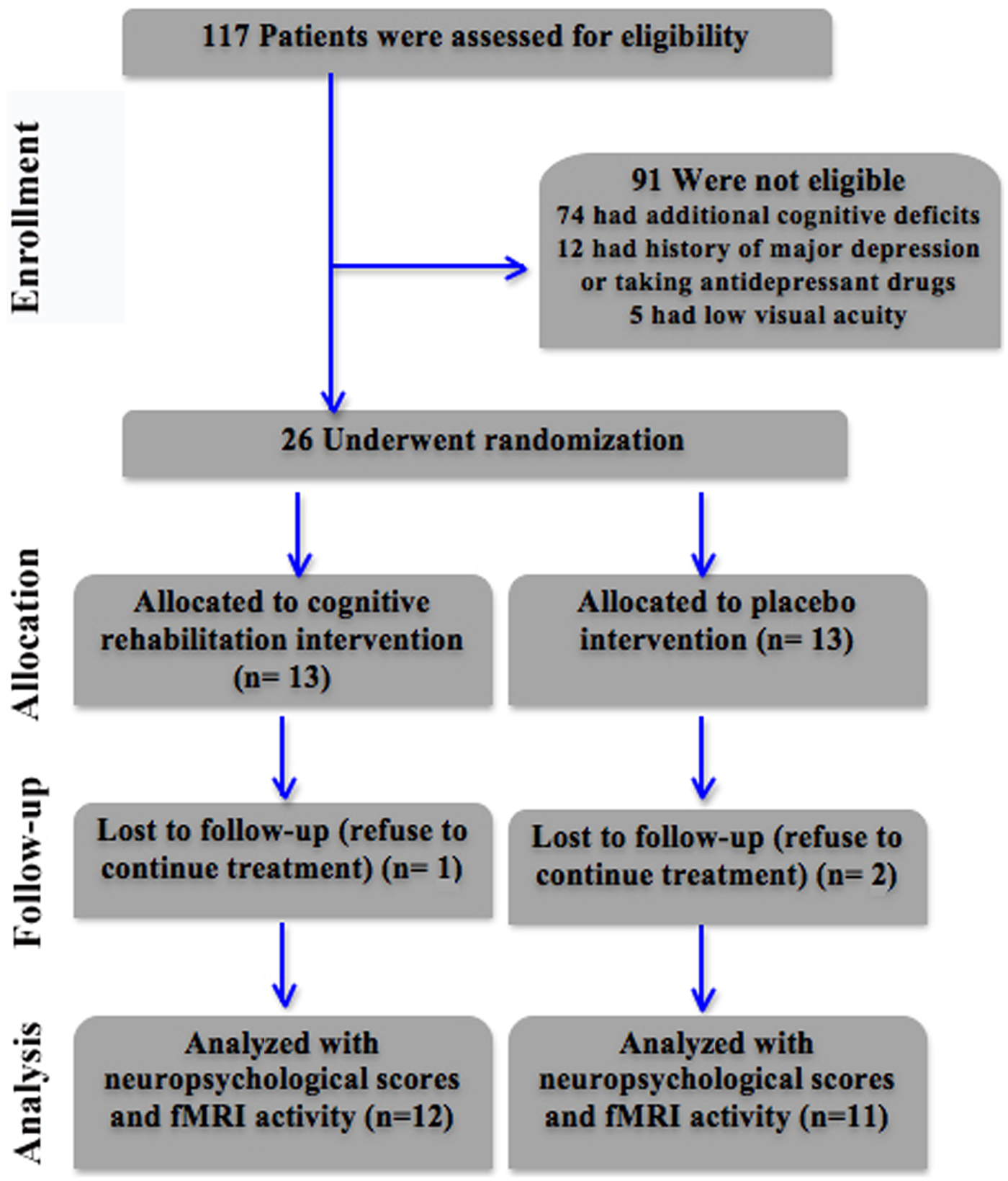
Flow diagram of participant recruitment and participation in the study: the experimental group participated in an individualized CR program for attention deficits (Rehacom software); the control group received motor therapy re-education (placebo intervention).
Neuropsychological Assessment
All patients completed an extensive series of neuropsychological tests that were administered by an experienced clinical neuropsychologist blinded to any other result. The vast majority of cognitive tests came from the brief repeatable battery (BRB) of neuropsychological tests, 17 one of the most widely used instruments to estimate cognitive dysfunction in MS patients. Cognitive performances were recorded at baseline and after 6 weeks (using form A and B to avoid learning effects). 18 The BRB includes the selective reminding test (SRT), the 10/36 spatial recall test (SPART), the SDMT, the word list generation, and the PASAT. The SRT assesses verbal learning and delayed recall. It includes a list of 12 words and uses 6 consecutive learning trials and a delayed trial (SRT-CLTR; SRT-LTS). The 10/36 SPART is a modified version of the 7/24 SPART and assesses visuospatial learning and delayed recall (SPART-I; SPART-D). Word list generation explores verbal fluency on semantic stimulus by asking the participants to produce as many words as possible belonging to a semantic category. The PASAT and SDMT assess sustained attention, information speed processing, and working memory. To test additional attention abilities and executive functions (such as executive control and task switching) not explored by the BRB, we also included the ST 19 and Trial Making Test form A-B 20 (forms A and B have been used). Results were compared with published Italian norms. 18 Finally, we tested global cognitive function using the Mini-Mental State Examination. 21
As previously reported by our group,22,23 as well as by others, 24 we considered those patients who scored 2 SDs below the mean normative values on at least 3 tests in our extensive neuropsychological battery to be cognitively impaired. MS patients who failed a maximum of 2 tests were classified as cognitively unimpaired and were included in the study. We further investigated the presence of depressive and anxiety symptoms using the Beck Depression Inventory 25 and the State-Trait Anxiety Inventory Y1 and Y2 (STAI Y1 and STAI Y2). 26
Design and Procedures
Our study was a double-blind randomized controlled trial divided into 4 principal stages. The first stage was based on the recruitment of the patients for the study (see inclusion criteria reported above). The patients were not informed about their group assignment, and the rationale about their training performed in our clinical center (experimental group) or at home (control Group). Similarly, the psychologist (carrying out the neuropsychological baseline assessment [T0] and posttreatment investigation [T1]) as well as the primary researcher and data entry assistants were all blinded to the group membership of the patients. In the second stage, the eligible MS patients underwent MRI examination (T0). In the third stage, participants were randomly assigned to 2 groups (experimental or control) using a computer-generated, site-stratified, randomization schedule. Randomization was stratified according to age (older or younger than 31 years) and educational level (more or less than 13 years of education). For each stratum, random numbers were assigned to the participants and put into envelopes; it was determined randomly whether the even or odd number would enter the experimental group. Participants were assigned to the study according to the numbers they received on opening the envelopes. The different steps in this process were administered by different research assistants who were blinded to the other processes.
The experimental group met twice a week for 1-hour sessions for 6 consecutive weeks. Sessions consisted of computer-assisted training of several attention ability and information processing tasks. Cognitive training was performed using the software RehaCom (www.Schuhfried.at). We decided to use this system because RehaCom is Europe’s leading software for CR, and this is now used in more than 1000 hospitals and practices across Europe. Moreover, several previous studies have used RehaCom to evaluate the impact of CR in patients with schizophrenia, 27 MS,8,12 and head trauma. 28 This software has a specific interface consisting of a special keyboard that has been designed to minimize the interferences caused by motor and coordination disabilities. This tool can be installed on a standard PC and stimulates specific cognitive functions at different levels of complexity and with different modes of input/output. Each cognitive performance and its progress can be recorded and saved on the hard drive. The study treatment consisted of “divided attention,” “attention and concentration,” and “vigilance” programs. In divided attention, the patient is required to simulate a train driver, carefully observing the control panel of the train and the countryside. Several distractions, such as crossing animals and train speed must be taken into account, with increasing levels of difficulty. In the procedure attention and concentration, an individual picture (target) is presented and then compared with a matrix of pictures. The patient has to recognize the target picture (coded as symbols, items, animals, or abstract figures) and select it from the matrix. The abilities to differentiate and to concentrate are trained simultaneously. The level of difficulty rises as the number and complexity of pictures to recognize increases. Finally, during the vigilance program, the patient is trained to sustain his or her attention for a long period of time by providing response times limited to the various items. The task of the patient is to control a conveyor belt and to select the objects that differ from a sample in one or more details. The control group underwent a similar exposure to computerized tests, consisting of 12 individual 1-hour sessions over a 6-week period (2 sessions per week). In particular, the control group performed a visuomotor coordination task by using an in-house software with which they had to simply respond quickly and accurately to the appearance of target visual stimuli (numbers 2–4–6–8) on the screen by pressing the corresponding number key on the keyboard. The level of difficulty rises as the speed of external stimulation, defined as interstimulus interval, rises from 3 s (level 1) to 500 ms (level 12). All performances were recorded on an external hard disk and analyzed in our research center. All patients completed the training at home with optimal performance. An experienced treating clinician was responsible for setting up the rehabilitation program and assisting patients during the study and control treatments.
Finally, at the end of the 6-week training, participants from both groups were given a blind evaluation, using the same protocol as at a baseline (T1). Two MS patients from the control group and 1 from the experimental group decided to not continue with the protocol. Thus, 12 MS patients from the experimental group and 11 from the control group completed the protocol.
fMRI Task
Participants were instructed to perform a commonly employed cognitive paced visual serial addition test (PVSAT) that is known to evoke robust activations within neural circuits underlying attention and executive functioning abilities29,30 and that can be used as an alternative for the PASAT. 31 This paradigm has been previously described in detail.29,30 fMRI data were acquired during a 6-minute block design with 1 active and 1 baseline condition (each lasting 27 s) repeated 6 times. During the 6 active PVSAT blocks, the participants were required to add up visually presented randomized single digits (presented every 3 s), adding each digit to the one immediately preceding it. The absence or presence of any involuntary abnormal movement during the activation or while in the resting state as well as the behavioral performance during the task were monitored during scanning. Before the fMRI session was performed, all participants completed a 10-minute practice session (which included different stimuli presented in the scanner) to practice the PVSAT task until they could perform it with ease and accuracy. Cognitive performances during the fMRI task were similar between the groups, either at baseline or during the retest phase.
Image Acquisition
The neuroimaging study was performed on a 3-T unit with an 8-channel head coil (Discovery MR-750, General Electric, Milwaukee, Wisconsin). The protocol included the following: (1) whole-brain T1-weighted scan MRI scanning, (2) fast fluid-attenuated inversion recovery (FLAIR) axial images, and (3) echo planar images (EPIs) sensitive to the blood oxygenation level dependent (BOLD) contrast.
Lesion Load Quantification
Total lesion load quantification was performed using a supervised automated segmentation method 32 that used the image intensities of the FLAIR images to train a classifier (cellular neural network–based approach). An experienced neuroradiologist (blinded to any other result of this study) double checked the cellular neural network–related final maps and manually performed lesion load quantification using MRIcro software (http://www.mricro.com).
fMRI Analyses of Regional Effects
fMRI data were preprocessed using SPM8 (http://www.fil.ion.ucl.ac.uk/spm/). EPIs were realigned to the first scan by rigid body transformations to correct for head movements, then normalized to the EPI standard template in the MNI space (Montreal Neurological Institute) using linear and nonlinear transformations, and finally smoothed with a Gaussian kernel of full width at half maximum of 8 mm. Participants displaying head movements >2 mm were excluded from the analyses.
These analyses aimed to (1) identify the brain regions activated by the PVSAT task for each group and (2) define the main effect of group, time, or the interaction between the 2 (2 × 2 analysis of variance [ANOVA] model). To these ends, a random-effect model was implemented using a 2-stage process (first and second level) that allows inferences about the general population from which participants are drawn. For each participant, we used a general linear model to evaluate regionally specific effects of task parameters on BOLD indices of activation. 33 At the first level, subject-specific contrast images were generated for the PVSAT versus baseline contrast. Each contrast was entered into a second-level general linear model to obtain the following: (1) SPM t maps (1-sample t test) to carry out the main effect of PVSAT for each group (see Supplementary material) and (2) SPM F maps related to the 2 × 2 ANOVA model.
Two approaches to threshold maps were applied. First, based on previous findings, we decided to use the bilateral anterior cingulate cortex (Brodmann’s area [BA] 32), lateral premotor cortex (BA 6), dorsolateral prefrontal cortex (BA 9/46), ventrolateral prefrontal cortex (BA 44/45), superior and inferior parietal lobule (BA 7/40), superior and middle temporal gyrus (BA 21/22/42), thalamus, caudate, and the whole cerebellum as a priori regions of interest (ROIs) given their critical engagement on attention abilities and working memory processes as assessed by PASAT or PVSAT.29,30,34-37 All ROIs were created with the “aal.02” atlas included in the Wake Forest University Pickatlas software version 1.04 (http://www.fmri.wfubmc.edu/download.htm). Statistical analyses within ROIs were thresholded by using correction for multiple comparisons (family-wise error [FWE], P < .05). For exploratory purposes, nonhypothesized group differences (ie, outside the ROIs) were only considered if a cluster of 10 or more contiguous voxels exceeded an uncorrected P < .001 threshold at the local maximum voxel. Moreover, because we hypothesize that attentional improvement per se could be related to functional changes, a linear regression analysis was used to determine the relationship between cognitive scores and functional changes.
Statistical Analysis
Statistical analyses were performed with Statistica Version 6.0 (www.statsoft.com). Demographic, radiological, and neuropsychological differences between groups were tested using the unpaired t test. For ordinal variables (Expanded Disability Status Scale and educational level), the Mann–Whitney U test was used to assess differences between groups. Behavioral changes associated to CR therapy were calculated as differential T1 − T0 (delta) scores. The magnitude of change resulting from the intervention was calculated using Cohen d, where an effect size value of 0.2 is considered a small effect, 0.5 is considered a medium effect, and values of 0.8 and above are considered large effects. All statistical analyses had 2-tailed α levels of <.05 for defining significance.
Results
Clinical and Neuropsychological Findings
At the time of inclusion, the 2 groups were perfectly matched for all demographic and clinical variables (see Table 1). At baseline, there were no significant differences between the experimental group and the control group in any of the neuropsychological tests (all P > .05; Table 2). During the retest phase, any clinical relapse or radiological change (ie, lesion load) is detected in the patients. At a phenotypic level, the differential T1 − T0 (delta) scores for each neuropsychological test were compared between the experimental and control groups. Although the experimental group performed better than the control group in all attentional/executive functions tests, statistically significant differences were only found in the ST (P < .007, d = 0.88; see Table 3). There were no observable benefits in mood status, although the experimental group showed an almost significant improvement in anxiety scores after CR (STAI-Y2; P = .056), with a large effect size (d = −0.84).
Participant Characteristics a
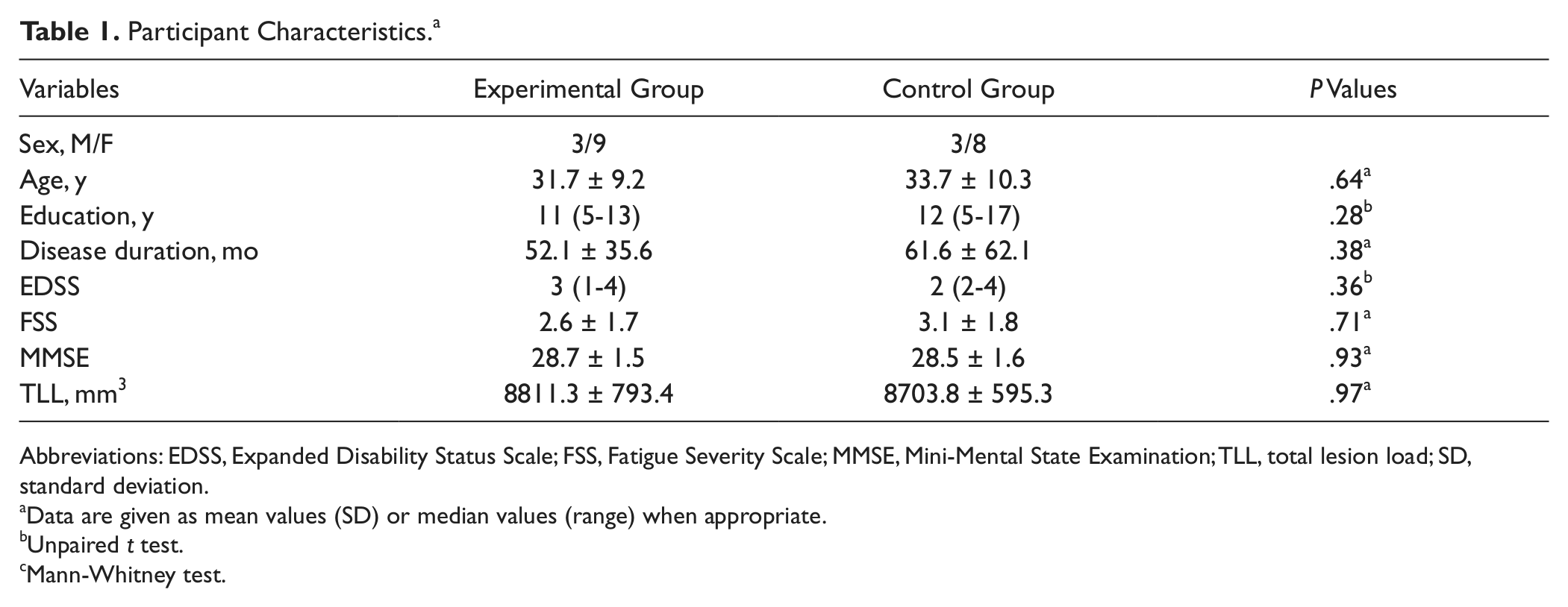
Abbreviations: EDSS, Expanded Disability Status Scale; FSS, Fatigue Severity Scale; MMSE, Mini-Mental State Examination; TLL, total lesion load; SD, standard deviation.
Data are given as mean values (SD) or median values (range) when appropriate.
Unpaired t test.
Mann-Whitney test.
Neuropsychological Performances in the Experimental and Control Groups at Baseline
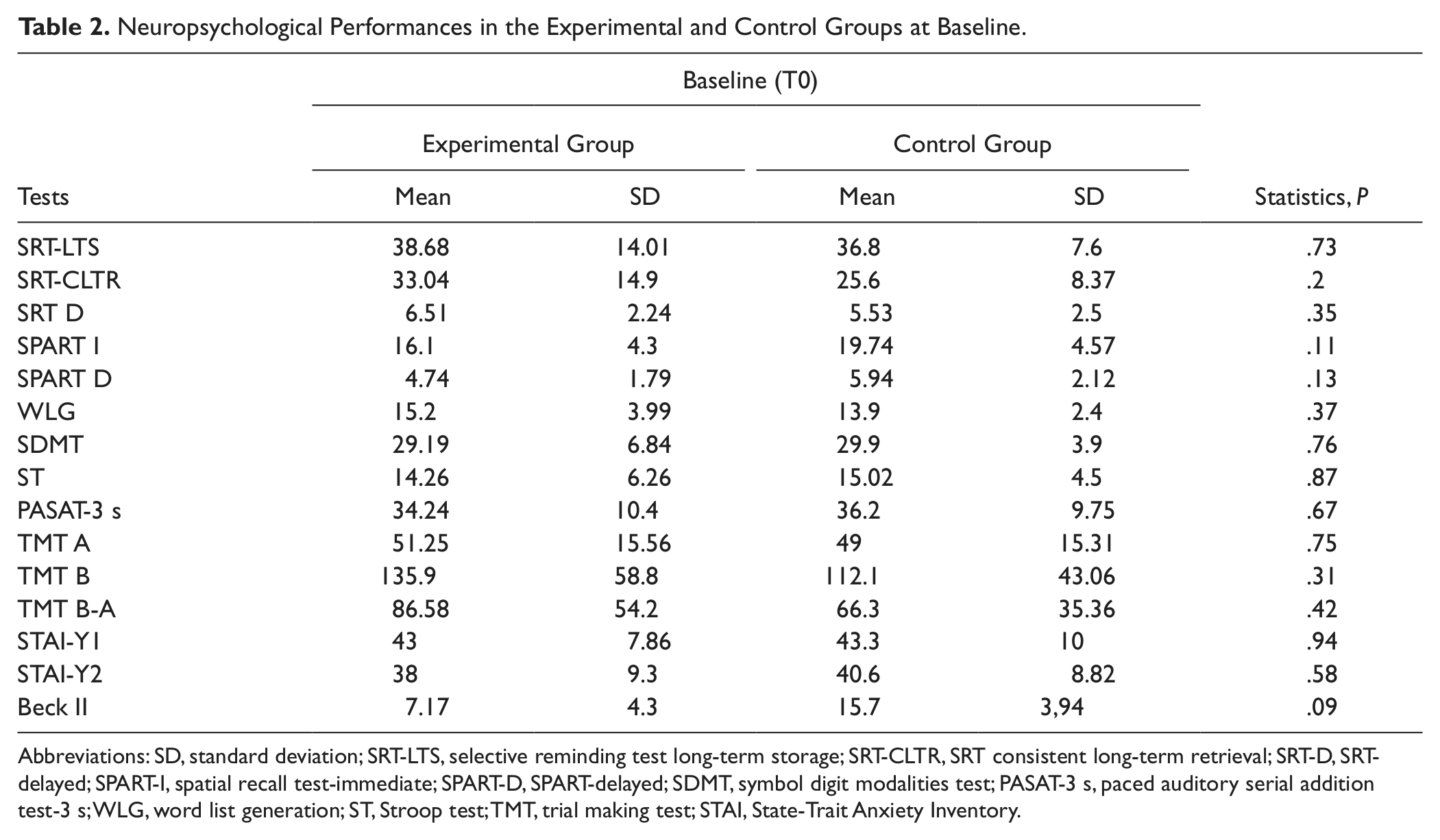
Abbreviations: SD, standard deviation; SRT-LTS, selective reminding test long-term storage; SRT-CLTR, SRT consistent long-term retrieval; SRT-D, SRT-delayed; SPART-I, spatial recall test-immediate; SPART-D, SPART-delayed; SDMT, symbol digit modalities test; PASAT-3 s, paced auditory serial addition test-3 s; WLG, word list generation; ST, Stroop test; TMT, trial making test; STAI, State-Trait Anxiety Inventory.
Neurocognitive Performances and Measures of Functional Scales in the Experimental and Control Groups at Baseline and Retest
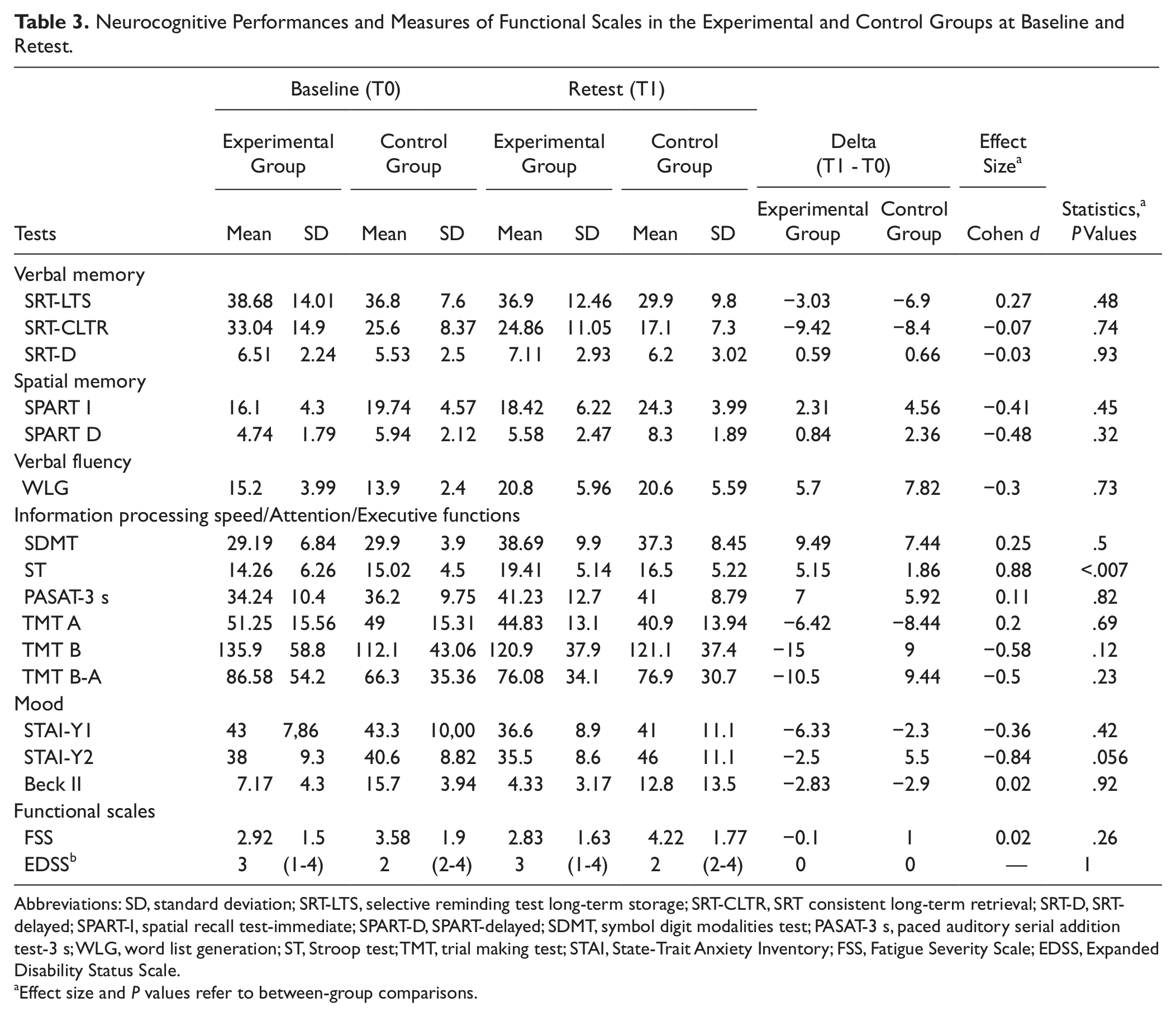
Abbreviations: SD, standard deviation; SRT-LTS, selective reminding test long-term storage; SRT-CLTR, SRT consistent long-term retrieval; SRT-D, SRT-delayed; SPART-I, spatial recall test-immediate; SPART-D, SPART-delayed; SDMT, symbol digit modalities test; PASAT-3 s, paced auditory serial addition test-3 s; WLG, word list generation; ST, Stroop test; TMT, trial making test; STAI, State-Trait Anxiety Inventory; FSS, Fatigue Severity Scale; EDSS, Expanded Disability Status Scale.
Effect size and P values refer to between-group comparisons.
fMRI Data
At baseline, in each group, the PVSAT elicited a robust bilateral brain response in a well-known neural network, including the dorsolateral prefrontal cortex, ventrolateral prefrontal cortex, inferior and superior parietal lobules, medial-dorsal-ventral premotor cortex, superior and medial temporal cortices, basal ganglia, thalamus, and cerebellum (Supplementary Figure 1).
At an intermediate phenotypic level, we used a 2-way ANOVA analysis investigating the main effects on group (experimental vs control), time (T0 and T1), and the interaction between them. Considering the interaction effects, the experimental group demonstrated a specific increased activity in the right posterior cerebellar lobule (Crus I/Lobule VI; MNI local maxima: x = 44, y = −64, z = −26; F = 14.92; P FWE = .02) and the left superior parietal lobule (BA 7; MNI local maxima: x = −26, y = −62, z = 44; F = 12.13; P FWE = .04) with respect to the control group during the execution of the PVSAT task (Figure 2). Outside our a priori ROIs, no significant changes were detected. Finally, there were no significant findings, within or outside the ROIs, obtained from the main effects on group or time.
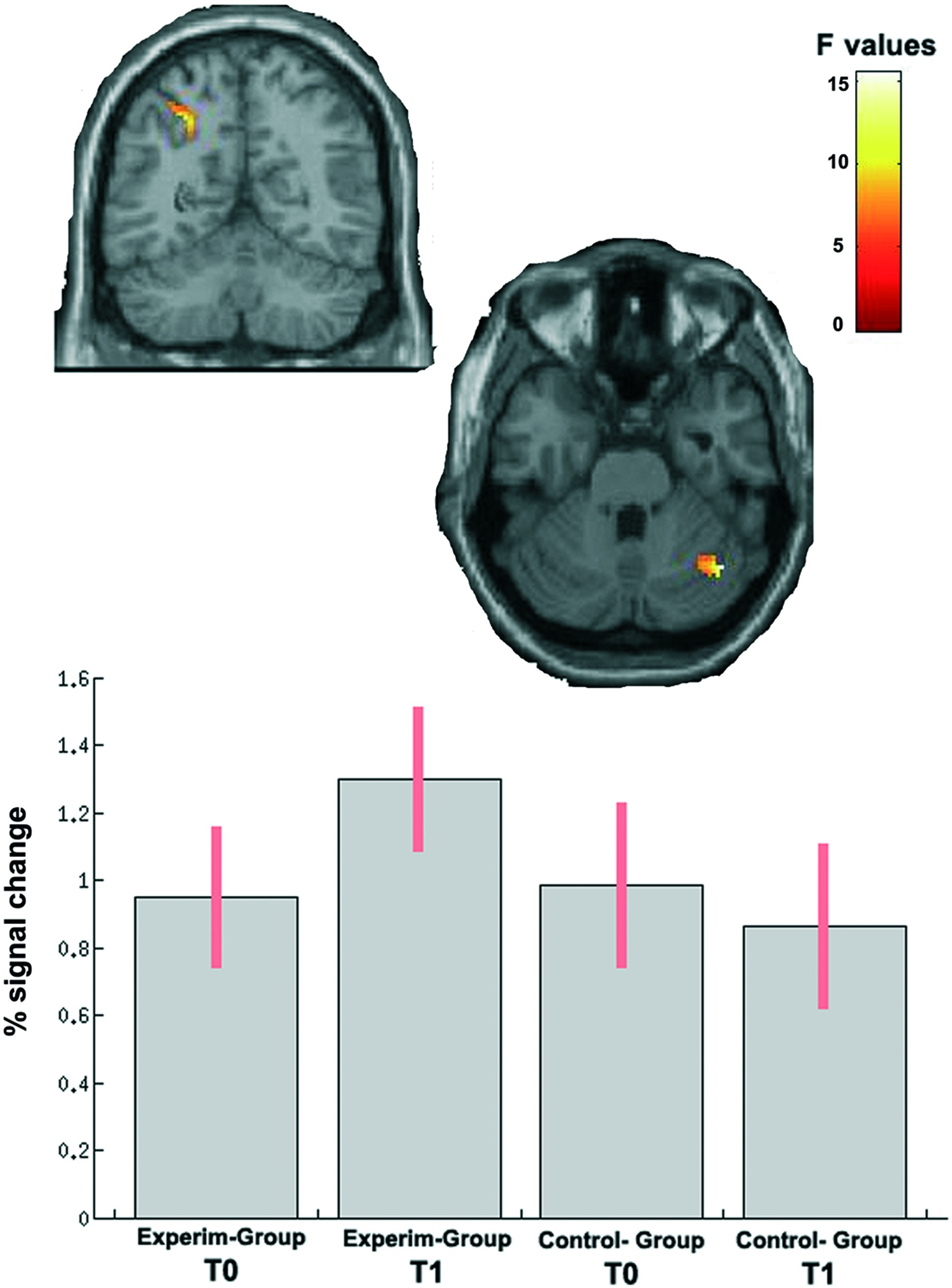
Group × Time interaction effect on fMRI data. After CR, the experimental group showed a significant overactivation (FWE < 0.05) of the right posterior cerebellar lobule and left superior parietal cortex in comparison with the control group. For each group, the parameter estimates for the contrast (PVSAT > rest) are plotted, and the highest activation was seen in the experimental group after CR.
To assess whether the detected behavioral improvement in the ST was associated with the detected cerebellar-parietal overactivity in the experimental group, an additional regression analysis was performed. A significant correlation was detected between the neurofunctional activity of the right posterior cerebellar lobule (MNI local maxima: x = 48, y = −62, z = -36; T = 14.94; P FWE < .001), the left superior parietal lobule (BA 7; MNI local maxima: x = −30, y = −62, z = 46; T = 5.66; P FWE = .02; Figure 3), and the delta scores related to ST. In other words, during the retest phase, the detected overactivity during the PVSAT task of the experimental group was positively correlated with the improvement in the ST. Outside our a priori ROIs, significant associations with ST performance were detected in the precuneus and in the dorsolateral prefrontal cortex.
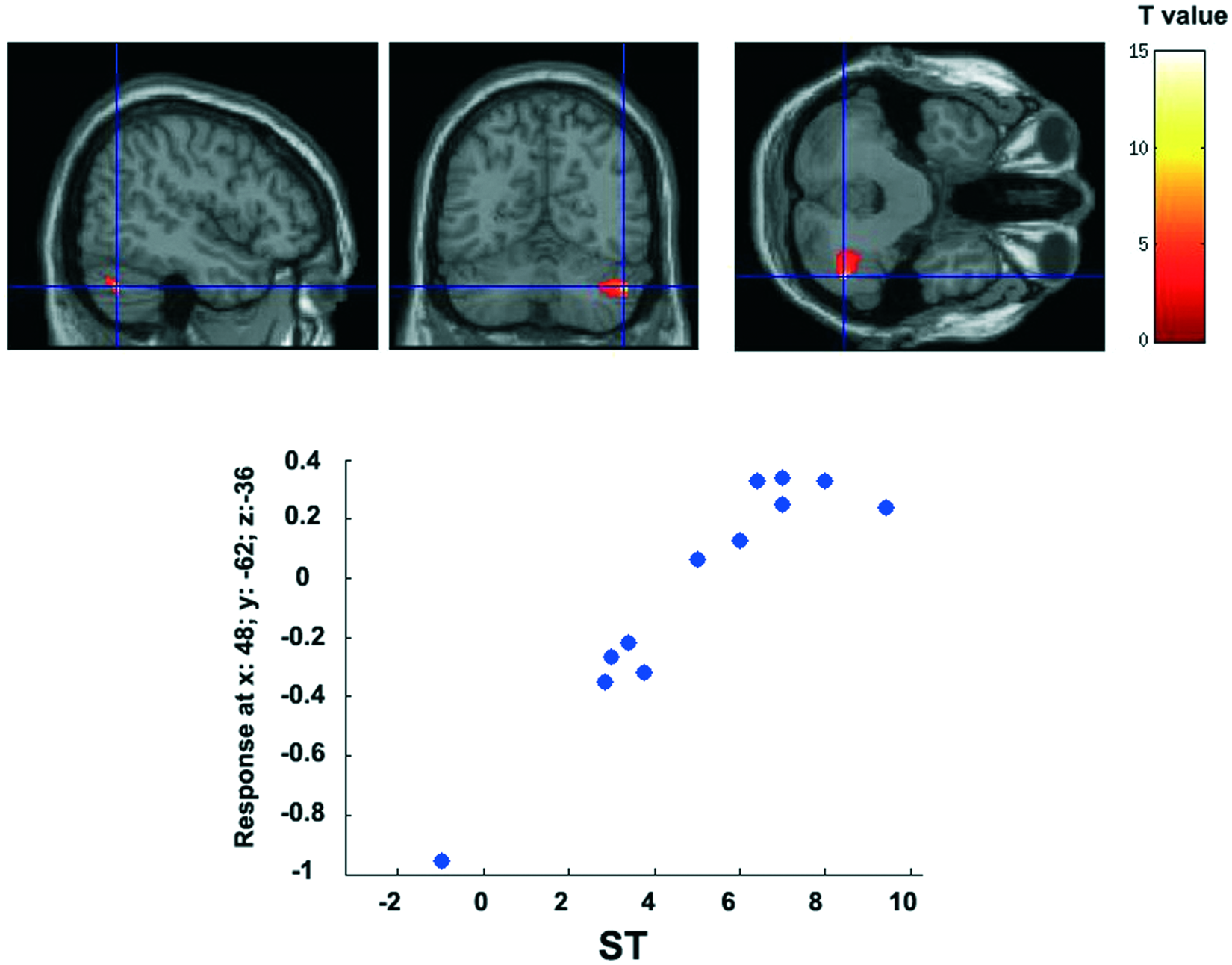
Significant correlation between brain signal activity and behavioral performance during the ST (delta scores) in the experimental group: scatter plots show the distribution of the mean signal change (y axis) of all voxels in the right cerebellar posterior lobule during the fMRI PVSAT task and ST delta scores (x axis), as shown in the lower part. Abbreviations: ST, Stroop task; fMRI, functional magnetic resonance imaging; PVSAT, paced visual serial addition test.
Because the depression status was greater in the control group than in the experimental group, all previous data were reanalyzed using Beck scores as a covariate of no interest. The overall pattern of findings remained the same.
Discussion
Our data confirm our hypothesis about the beneficial effect of CR in MS patients both at a phenotypic level (improvement in specific cognitive functions) and at an intermediate phenotypic level (functional reorganization), demonstrating that an intensive computer-based training program specifically tailored for impaired attention abilities yields adaptive neural plasticity of the associated neural network. In particular, overactivity of the posterior cerebellar lobule and superior parietal cortex might represent a new endophenotype for future cognitive rehabilitative approaches.
The first goal of CR therapy is to delay and attenuate the severity of MS-related cognitive deficits. If cognitive deficits are recognized early, it may facilitate the planning of other rehabilitation services and reduce the patient’s levels of dependence. However, conflicting findings have been reported about the effectiveness of the various CR techniques.6-12 The lack of conclusiveness in these studies appears to be mainly caused by methodological problems, such as high variability in the selection of clinical phenotypes, the use of unstandardized training tools, and the lack of a control group. On the other hand, the most convincing evidence comes from some studies8,11 that focused cognitive intervention on a limited cognitive domain. In particular, rehabilitation of attention abilities would seem to provide the most evident beneficial effects. This hypothesis has been recently demonstrated by an elegant fMRI study, where the authors demonstrated that a CR program focused on attention and information processing yielded an enhanced neural activity in the parietoprefrontal regions during the execution of a ST. 38 Decrements in attention and overall information processing are frequent in MS and cause functional dependence and depression. 39 Research and clinical experience in the field of brain injury rehabilitation have focused extensively on the potential of the rehabilitation program to retrain attention skills, showing promising findings. 40 Attention abilities refer to the ability to maintain and manipulate information for a short period (working memory), to sustain attention over time (vigilance), and to screen out nontarget information (resistance to interference or freedom from distractibility). 40 With this in mind, it is not surprising that the ST was the cognitive test for which treatment yielded a significant improvement. In fact, the ST mainly involves sustained attention, the ability to elaborate relevant/irrelevant dimensions in parallel (to screen out nontarget information), and some aspects of executive functions, such as the ability to inhibit an automatic response while performing a task based on conflicting stimuli.
fMRI analysis revealed the presence of a functional reorganization in specific brain regions. In particular, cerebellar lobule VI is involved in a number of cognitive functions, including language, visuospatial skills, and working memory. 41 As regards working memory, some models explicitly include the cerebellum as a key region. For example, Baddeley’s model 42 proposed a framework for working memory, called the phonological loop, which consists of 2 components: a phonological short-term store, which can hold speech-related information for 1 to 2 s, and an articulatory control system, which serves to subvocally refresh the contents of the phonological store. Several fMRI studies43-45 demonstrated that lobule VI represents part of the corticosubcortical circuit (including also Broca’s area) that is related to the articulatory control system.44-46 Therefore, cerebellar overactivation in the experimental group may therefore represent an increased effort to subvocally refresh phonological stimuli (“2” plus “7” etc) in an articulatory control system. A Concerning the overactivation of the superior parietal cortex, although activations in this region have been observed also during simple calculation and arithmetic procedures, 47 evidence has demonstrated that this area is involved in buffering and storage processes of relevant information for a short-term period. 48 Thus, the detected overactivity of the cerebellum and parietal cortex would seem to suggest that our proposed therapeutic strategy acts in recovering specific mechanisms of plasticity (read cognitive strategies) in MS patients, which might help decrease the emergence of cognitive impairment.
Some important caveats need to be considered in discussing our data. An important limitation of this study is the difficulty in enrolling MS patients with predominant attention deficits. Cognitive impairment involves approximately 50% of all MS patients and affects long-term memory, sustained attention, verbal fluency, information processing speed, and executive functions. That we have enrolled only 26 MS patients with predominant attention deficits from our initial group (n = 117 patients) highlights the fact that our findings cannot be generalized to all MS populations. Therefore, to sustain the usefulness of our CR therapy for minimizing the emergence of cognitive impairments in MS patients, further studies are warranted that use a larger sample and consider patients with additional cognitive deficits. Again, one might notice that the control group also showed a tendency toward improvement during the retest phase in several cognitive tests. Although we used both delta scores and alternative forms of the neuropsychological battery (A and B), subtle learning effects could not be completely ruled out. Similarly, for the experimental group, it could be hypothesized that the reported interaction effect on the functional reorganization within the cerebellum and the parietal cortex might be influenced by learning effects. To avoid this effect, patients should repeat the fMRI task twice (during the same session). However, recent evidence demonstrated that once training has been secured with some repetitions of the test, serial fMRI during PASAT performance does not display changes in activation. 49 Moreover, it is important to bear in mind that all our patients either in the T0 or T1 phases, completed a 10-minute practice session inside the scanner room before fMRI acquisition. All this evidence would seem to reduce the impact of learning effects on the reported neurofunctional changes associated with CR therapy. Again, an additional interference could be a result of the fact that the control group was treated with a visuomotor task. This placebo effect enhances the methodological robustness of our study, but it might have induced a general small cognitive improvement independent of group assignment, as previously occurred in the study by Solari et al. 12 Finally, one might question the use of the fMRI PVSAT task to investigate the neurofunctional changes underlying cognitive restoration in the ST. As demonstrated by correlation analysis, the improved performance during the ST proved to be correlated with the overactivity detected in the experimental group during the PVSAT task, suggesting a shared neural network involved during the execution of both tasks. However, future studies using absolute measures, such as task-free methods (ie, resting-stage fMRI), could be useful for further understanding the current results.
In conclusion, our data confirm the beneficial effect of the proposed CR strategy focused on attention disorders because attention represents a controlling and integrating function with implications for nearly all other cognitive systems. 11 These findings might represent an important improvement in this field of study because almost all previous studies generally used nonspecific interventions where a plethora of cognitive functions were rehabilitated.6,7,9,10,12 In fact, when CR is tailored to 1 specific cognitive domain, significant and more effective results can be found in the MS population.8,11,50
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a research fellowship FISM (Fondazione Italiana Sclerosi Multipla onlus) no. 2010/R/11 and by MIUR (Ministero Universita’ e Ricerca; PON 01_01180) grants to Prof Aldo Quattrone.