
Abstract
Health system responsiveness (HSR), a measure of patient health care experience, may influence adherence to HIV/AIDS care and be an important predictor of outcomes. We studied the relationship between HSR, patient factors, and visit nonadherence in 16 President's Emergency Plan for AIDS Relief–supported HIV/AIDS clinics in Dar es Salaam. An HSR survey was administered in 2009, and all clinic visits 1 year following the interviews were analyzed for 720 patients on antiretrovirals (ARVs). Definitions of visit nonadherence were (1) low visit constancy ([VC], no visit in
Background
Strong engagement and retention in care is critical to successful HIV treatment but remains a challenge for programs globally. 1 –3 Although there has been increasing recognition of the importance of identifying risk factors for nonretention, when defined as loss to follow-up, understanding which patients remain in care but with weaker engagement is also important. Studies in resource richer settings have demonstrated associations between increased mortality and weaker engagement, as defined by missed visits in patients already successfully linked with care. 4 –8 However, there is limited research on this in resource-limited settings (RLS) and it is a critical area to address. 9
Understanding patient and system factors associated with nonadherence to clinic visits is necessary to design and implement effective interventions that improve adherence to care. In RLS, this work has focused on critical issues including health care access (distance, cost, wait time), duration of visits, health care worker (HCW) attitudes, and patient factors including socioeconomic barriers, stigma, and issues of disclosure and knowledge related to HIV care and treatment. 9 –15 Barriers to access in these settings, defined as initiation and continuation of antiretroviral therapy (ART), include lack of knowledge about ART, perceived or actual cost of the treatment, stigma, longer distance from home to the clinic, and lack of coordination of services. 16 These risk factors are similar to those associated with poorer long-term retention in care. 7,14,17,18 However, there are still considerable gaps in understanding the full range of factors associated with lower rates of adherence to and retention in care.
Patient satisfaction and health system responsiveness (HSR) have been defined as an important component of quality of care and critical to ensuring that health systems meet patient needs and expectations. 19,20 Responsiveness measures the patient’s experience with the health care system in 8 domains: dignity, autonomy, confidentiality, communication, promptness of attention, social support, basic amenities, and choice of provider. Patient satisfaction, a more subjective measure of a number of domains of HSR, also captures the patient’s perspective of quality of care received. The importance of the patient’s perspective has been shown with high patient satisfaction correlated with increased compliance, decreased latency to care seeking, and improved understanding and retention of the medical information. 21,22 Not surprisingly, there is an overlap between system factors associated with lower adherence to care and those associated with low patient satisfaction with care and low HSR. These include long wait times, long distance of clinic from the patient’s home, and health care worker shortages that are incorporated elements of HSR. 23,24 However, the relationship between HSR and adherence to HIV care has not been well described in the RLS.
Understanding the relationship between patient’s perspective of quality and HSR factors and adherence to care is critical as efforts are made to improve retention in care and HIV treatment outcomes. We report on a study to identify the association of patient factors and reported HSR on future adherence to care and retention in care for patients on antiretroviral therapy (ART) at a network of HIV clinics in Dar es Salaam, Tanzania sites supported by the US President's Emergency Plan for AIDS Relief (PEPFAR) 1 -supported Management and Development for Health (MDH). These Care and Treatment Centers (CTCs) are based on public sector hospitals or health centers and are staffed by a multidisciplinary team generally consisting of physicians, nurses, counselors, and pharmacy staff who deliver comprehensive outpatient HIV care including ART, supportive services, outreach, and outpatient management of opportunistic infections for adults and children.
Methods
Patients
From March to July 2009, the MDH implemented a cross-sectional study in 16 CTCs that examined patient and site factors associated with the patient’s reported HSR and satisfaction with care. The MDH survey was administered to nonpregnant adult patients at each clinical site in a systematic fashion. Patients were approached if they had been in care at the site for at least 6 months and were consented to the survey and its linkage to their clinical data. After obtaining verbal consent, the survey was administered by single trained research nurse.
A total of 809 patients completed the survey and had available clinical data 1 year following their survey date. In all, 5 patients who had died within 1 year of the survey date, 4 who did not have a clinic visit following the interview date, and 80 who were not on ART at the time of the survey were excluded from the analysis because of lower frequency of required visits (every 6 months versus every 3 months for patients on ART). In total, 720 patients were included in the final analysis.
Survey
The HSR survey was developed from other surveys measuring HSR 25 and structured on the World Health Organization (WHO) HSR domains. It was then adapted based on the focus groups with patients and staff. Patients were asked to rate services in areas including access, communication, confidentiality, and perceived quality. Responses were that a service was either received or not received and were rated on a 5-point Likert scale. The Likert-scale ratings were further dichotomized into top 2 and lower 3 responses (ie, very good/good versus moderately good/fair/poor). Surveys also collected sociodemographic information including age, household assets, education, distance from the clinic, and health status.
Clinical Data and Site Characteristics
Survey data were linked with clinical data from the MDH clinical care database using a unique patient identifier. Clinical data included date of enrollment at the clinic, date of starting ART, age, gender, serial CD4 counts, visit dates, and receipt of recommended care (tuberculosis [TB] screening, cotrimoxazole treatment if eligible, CD4 count monitoring, and time to starting ART once eligible). Date of initial HIV diagnosis could not be reliably ascertained from the existing data.
Site factors included site size and staffing measured as number of patients to 1 full time equivalent (FTE). Site size was determined by average monthly patient volume, where small sites served <200 patients per month, medium sites 200 to 1000 patients, and large sites >1000 patients per month.
Outcome Definitions
Adherence to care was defined through several approaches based on the data available within the MDH database as well as the recent publications looking at different ways to measure adherence and engagement with care (Table 1). 2 All outcomes were measured during the year following the survey administration. The outcomes included visit constancy (VC), gaps in care, and visit in the last quarter (VLQ). The VC was defined as the proportion of quarters (3-month periods) with at least 1 completed clinic visit in the year following the survey. The VC was categorized into 3 groups: having at least 1 completed clinic visit in (a) 0 or 1 quarter, (b) 2 or 3 quarters, or (c) all 4 quarters. Gaps in care was defined as the maximum time interval between 2 completed clinic visits in the year following the survey, which was dichotomized into 2 groups; less than 60 days or greater than or equal to 60 days. The VLQ is the percentage or patients with a visit in the last quarter (3-month period) in the year following the survey. The MDH requires that all patients on ART come to the clinic monthly.
Definition of Terms Measuring Adherence to Care in the Year Following the Interview.
Statistical Analysis
The sample size was powered to estimate the overall rates of satisfaction within a ±8% confidence interval (CI), with an α of .05 and a β of 90%. Bivariate logistic regressions were used to describe the association between patient sociodemographic factors and patient-reported ratings of HSR with the 3 adherence to care outcomes. In order to determine the independent predictors of adherence to care for each outcome, all covariates associated with adherence to care at a P value <.20 level were entered into a backward elimination model using a stay criteria of 0.5. The final models included site factors and accounted for clustering at the site level using generalized estimating equations. A P value <.05 was considered statistically significant. All analyses were performed using SAS version 9.1.3 (SAS Institute Inc, Cary, North Carolina).
Human Participants Protection
The study protocol was reviewed and approved by IRBs at Harvard School of Public Health, Harvard Medical School in the United States and Muhimbili University of Health and Allied Sciences and the National Institute of Medical Research in Tanzania. All analysis was done using de-identified data.
Results
Population
Baseline characteristics of the patients are shown in Table 2. Patients were predominantly females (74%), with a median age of 36, and 62.7% (450) had completed primary school education with 26.3% (189) having at least some secondary school education. All had been in care greater than 6 months and had been on ARTs for a median of 1.5 years (range 3 days-4.5 years), with over 50% with a CD4 count >350 cell/mm3 and 22% with CD4 count <200 cells/mm3 at the time of the interview.
Demographics of Patients Included in the Analysis.

Abbreviation: ART, antiretroviral therapy.
a One point each for radio, bicycle, electricity, running water, television, car, owns house.
Adherence to Care
The majority of patients were adherent to care regardless of the definitions used (Figure 1). In all, 86 % had a visit in the last quarter, while slightly fewer (77.7%) had a visit in all 4 quarters. The lowest performance was in gap in care, with 49.6% having a maximum gap in care of 60 days or longer, of whom 21.9% had a gap between 60 and 90 days, 5.6% had 90 to 120 days, and 22.3% had 120 or longer. However, we found that close to one-half of the patients who had full VC (visit every quarter) had a gap of 60 days or more between at least 2 or more of these visits.

Percentage adherence by various definitions.
Factors Associated with Adherence to Care
Factors significantly associated with decreased adherence to care defined as largest gap in care >60 days were younger age (≤24 years, adjusted odds ratio [AOR]: 3.86 [95% CI: 2.02-7.40]), medication side effects not explained during visit (AOR: 2.21 [95% CI: 1.49-3.28]), and shorter time on ART (between 3 and 6 months, AOR: 2.44 [95% CI: 1.40-4.25]; between 0 and 3 months, AOR: 1.49 [95% CI: 1.09-2.03]). Factors associated with having no VLQ included younger age (≤24 years, AOR: 3.40 [95% CI: 1.63-7.07]), HCW not having explained things in a way the patient understood (AOR: 4.83 [95% CI: 1.39-16.78]), and shorter time on ART (3-6 months, AOR: 3.09 [95% CI: 1.72-5.57] and 0-3 months, AOR: 5.04 [95% CI: 2.47-10.30]). Young age and shorter time on ART were also associated with lower VC (at least one-quarter with no visit; ≤24 years, AOR: 4.65 [95% CI: 2.36-9.17]), time on ARTs of 6 to 9 months (AOR: 2.73 [95% CI: 1.44-5.18]), 3 to 6 months (AOR: 5.26 [95% CI: 3.17-8.74]) and 0 to 3 months (AOR: 5.90 [95% CI: 3.18-10.96]). The HCW not explaining things in a way the patient understood (AOR: 4.10 [95% CI: 1.54-10.89]) and higher patient to staff ratio (>200 patients per HCW, AOR: 1.46 [95% CI: 1.03-2.08]) were also associated with lower constancy. Higher comfort rating of the clinic (AOR: 1.66 [95% CI: 1.19-2.31]) was associated with lower constancy but not with other measures of lower care adherence (Table 3).
Adjusted Odds Ratios and Confidence Intervals for Select Patient and Health System Responsiveness Factors by Visit Adherence Definitions.a
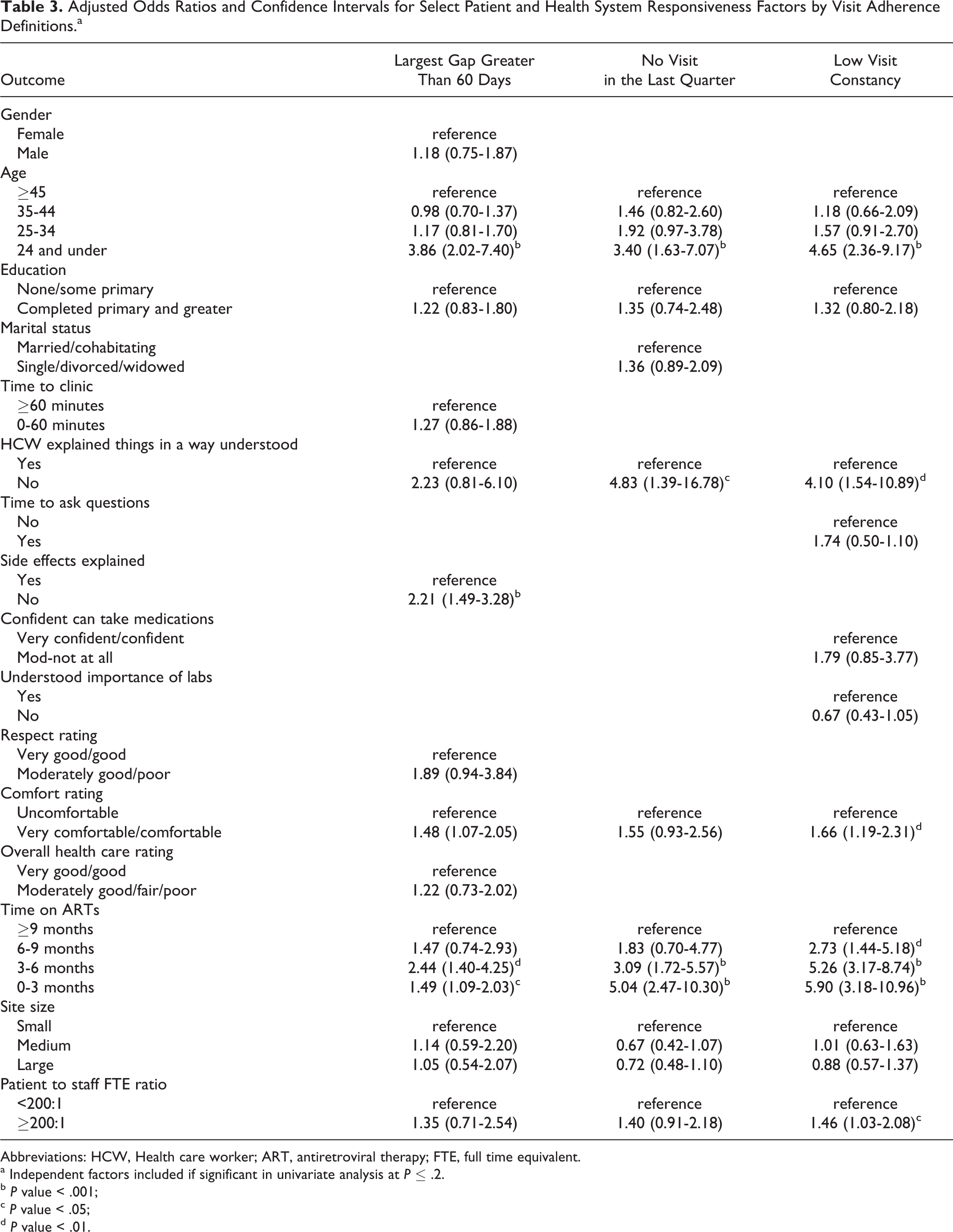
Abbreviations: HCW, Health care worker; ART, antiretroviral therapy; FTE, full time equivalent.
a Independent factors included if significant in univariate analysis at P ≤ .2.
b P value < .001;
c P value < .05;
d P value < .01.
Discussion
We found relatively high rates of adherence to care for patients on ART in the setting of a network of PEPFAR-supported clinics in urban Tanzania as measured by having a recent visit and VC, defined as a visit each quarter. However, one-half of the patients were not being seen at the intervals considered standard of care for patients on ART at MDH-supported HIV Care and Treatment Clinics, which are monthly visits. Patient factors associated with decreased adherence to care were younger age and shorter time on ART. Among the HSR domains, only poor HCW communication was consistently associated with decreased adherence to care.
Rates of adherence in our cohort were higher than the results from resource richer settings such as the United States. For example, in a study by Giordano, 4 36% of the patients were nonadherent as defined by VC, with 36% having <1 visit per quarter. Furthermore, in a cohort of 842, Torian 26 found that only 45% had regular care, defined as at least 1 visit every 6 months. Most studies from the RLS have focused on loss to follow-up rather than adherence to care, although some definitions overlap. 3,27 In Kenya, Ochieng-Ooko 27 reported that 4.3% were lost to follow-up as defined by a gap in care of 3 months or more. Other studies using gaps in visits to define lost to follow-up have reported rates of 15% in Malawi 12 and 16% in South Africa. 17 Although loss to follow-up has been associated with poor outcomes in RLS, there is only limited data on the impact of lower adherence to care among patients with weaker engagement but who remain in care in these settings. 7
A number of patient factors were associated with adherence to care. Younger patients and those with a shorter time on ART had lower adherence to care across all definitions, similar to factors identified in studies from the United States, 4,26,28 although an association between age and strength of engagement with care has not been reported in the RLS. Differing from the other studies in RLS, we did not find an association between gender, CD4 count, and education with adherence to care. Some may be related to the cohort. For example, 80.4% reported having completed an education level of primary school or higher, limiting the power to detect differences based on the level of formal education achieved. Although male gender has been associated with poorer outcomes in Tanzania, we found men and women were equally likely to maintain adherence to care, regardless of the definition used, pointing to other reasons for this association. 29 Similarly, other studies in Africa found competing work schedules as self-reported causes for nonadherence to care. 27,30 We did not find an association between employment status and visit adherence in our cohort, although many of the patients were self-employed (39.2%) and so may have had more flexibility than those employed in the formal sector.
Poor HCW communication was the only domain of HSR associated with lower adherence to care using 2 of the 3 definitions. Provider communication has the potential to impact adherence to care in many ways. Previous studies have identified it as a critical component to ensuring patient understanding of the importance of regular visits. Furthermore, it has been associated with medication adherence and outcomes 21,31 as well as a major determinant of the patient satisfaction. 22 A number of HSR domains were not associated with adherence to care in this study but found to be important in other studies. Distance or difficulty in travel to the clinic were not associated with adherence to visits, factors that have been associated with missed visits, in South Africa 9,32 and Kenya. 27 This may be in part due to the urban setting, where the range in travel time is not as broad as in the more rural settings and the relatively small percentage who had to travel longer than 60 minutes.
Patients seen at clinics with higher patient load per provider also had significantly lower adherence, as measured by the VC. There was an association with other nonadherence measures as well, although this did not reach statistical significance. Although we were not able to measure wait time, increased patient load could result in longer wait times and decreased time with the provider, which have been found to be predictors of lower patient satisfaction in South Africa and the United States. 23,24
The way in which nonadherence to care is measured will effect what factors predict patients most at risk for care nonadherence and how patients are categorized. For example, 50.2% of the patients who were adherent based on VC had a gap in care of 60 days or longer (Table 3). Similarly, 8% of the patients who were seen in the last quarter did not have a visit every quarter, so would have been classified as nonadherent using VC but not by the VLQ. Work to understand which definition or combination of definitions is correlated with the outcomes of care is needed to identify which patterns of care nonadherence are of greatest concern to HIV care and treatment programs.
There were a number of limitations of this study. Our population had already been in care 6 months at the time of their survey, and so we were not able to capture patients who fall out of care soon after entry. Furthermore, we adapted measurements of HSR, which may not have captured certain components. Ratings were not anchored such that patient’s ratings were balanced against their expectations and high ratings across most measures of the HSR limited power to identify predictors. 33 We also relied on self-report for quantitative measures such as travel time and could not be verified. Finally, we did not track whether patients transferred to other clinics or stopped ART, so what we defined as nonadherent may actually be patients who were receiving appropriate care elsewhere or who had died.
Understanding the relative rates of adherence to care, the best method of measuring this, as well as identifying patient and HSR factors associated with stronger engagement and retention are increasingly critical to improving HIV treatment outcomes, especially as time in treatment has lengthened. Engagement with care requires a continuous relationship with the providers and is associated with higher rates of medication adherence, better opportunistic infection prophylaxis, and overall improved outcomes in patients with HIV. 5,6,8,34 Furthermore, it has been shown to decrease risky sexual behaviors that may reduce transmission to others. 4 The potential benefit of HIV treatment programs is partially limited by the strength of engagement with care, and more research is needed to characterize engagement with care to devise effective ways to strengthen it. 35–37 Elements of HSR, such as HCW communication, have been shown to promote adherence. 21 However, there has been little research to explore this further, especially in the RLS, and most studies have focused only on patient satisfaction. 21 –24 Understanding how factors of HSR affect adherence is important to implement effective interventions. This would allow for identification of poor engagers so that care could be strengthened before they can be lost to follow-up, improving overall patient outcomes in HIV care and treatment programs.
Footnotes
Acknowledgments
The authors would like to thank the clinic’s patients, staff, site managers, and supervisors of all the sites that participated in this study, Harvard University Center for AIDS Research (CFAR), which supported and funded the study through
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Harvard University Center for AIDS Research (CFAR) supported and funded the study through