
Abstract
Multiple studies have demonstrated increased rates of osteopenia and osteoporosis in HIV-infected patients but there have been no published studies on current screening practices. We conducted a retrospective chart review of 2924 patients attending an urban HIV clinic. Thirty patients (1%) had dual-energy x-ray absorptiometry (DXA) scans. Patients undergoing DXA scans were more likely to be older, women, and have nondetectable HIV viral load and CD4 count ≥200. The most frequently cited indications for screening were perimenopausal or postmenopausal status and HIV infection. Of the patients screened, 96% had osteopenia or osteoporosis with a median T-score of −1.9 and a median of 3.8 osteoporosis risk factors in addition to HIV. Of the 20 practitioners in the clinic, only 7 had patients with screening DXA scans. DXA scans are underutilized in the HIV population given the high rate of osteopenia and osteoporosis detected in this study.
Keywords
Introduction
With the success of antiretroviral therapy in increasing life span of HIV-infected patients, conditions associated with aging have become more prevalent. These diseases often occur at earlier ages and have more severe manifestations in HIV-infected patients. One such condition is low bone mineral density (BMD). Studies have shown that HIV-infected patients have higher rates of osteopenia and osteoporosis than the general population. 1 –6 Although the causes of this association are not yet clear, it may be related to an aging HIV population, 7,8 high prevalence of osteoporosis risk factors in patients with HIV, 9 –13 metabolic complications of highly active antiretroviral therapy (HAART), 9 –21 and perhaps effects of the virus itself. 1 –13 Screening guidelines for osteoporosis in the general population are well established but most do not include HIV as a risk factor. 22 –26 Screening recommendations specific to HIV-infected patients have recently been published 27 –29 but it is unclear if these guidelines are inclusive enough.
Even less clear than the osteoporosis screening guidelines for HIV-infected patients is what practitioners actually do when providing care. There are no published studies describing who is screened for osteoporosis and for what indications. Given the fact that low BMD increases fracture risk and that fractures are associated with significant morbidity and mortality, identifying and treating low BMD before fractures are important aspects of providing care to HIV-infected patients. The aim of this study is to assess current screening practices for osteoporosis in HIV-infected patients.
Materials and Methods
Study Design
We conducted a retrospective chart review of patients attending an urban HIV-only clinic in Baltimore, Maryland. The electronic database of 2924 HIV-infected patients aged 18 years or older seen from July 2007 to August 2010 was searched using the terms “DEXA” (previously preferred over “dual-energy x-ray absorptiometry [DXA]”), “osteoporosis,” “osteopenia,” “osteoporotic,” and “osteopenic.” Of the patients identified by these parameters, DXA scans were completed in 30 patients. Paper clinic records from January 2000 to July 2007, electronic clinic records from July 2007 to August 2010, and electronic records from the affiliated hospital were reviewed for these 30 patients. Clinic notes in the 6 months prior to the date of DXA scan were included. This protocol was approved by the University of Maryland Medical Center Institutional Review Board.
Data Collected
Data collected included age, sex, race, height, weight, CD4 count, HIV viral load, comorbidities, medications, use of substances (alcohol, tobacco, and illicit drugs), current symptoms, DXA results, stated indication for screening, provider name, and presence of osteoporosis risk factors. Screening indications were determined by examining paper copies of the DXA scan reports and reviewing clinical progress notes. Nonspecific indications such as “health maintenance,” “screening,” and “rule-out osteoporosis” are not reported. Persons were excluded if they did not have clinic notes in the 6 months prior to the DXA scan.
Whether or not each patient qualified for screening was determined based on the review of United States Preventative Services Task Force (USPSTF), American Association of Clinical Endocrinologists (AACE), American College of Obstetrics and Gynecology (ACOG), and National Osteoporosis Foundation (NOF) guidelines (Table 1). 22 –26 From extensive lists of risk factors in these guidelines, those identified in these patients and thus included in data analysis were perimenopausal or postmenopausal status, white race, aged older than 65 years, family history of osteoporosis, evidence of osteopenia on x-ray, body mass index <18.5, immobility, hyperparathyroidism, rheumatoid arthritis, vitamin D deficiency, diabetes, sarcoidosis, chronic kidney disease, hypogonadism, and use of tobacco, alcohol, illicit substances, antiepileptics, glucocorticoids, selective serotonin reuptake inhibitors, proton pump inhibitors, and gonadotropin release hormone (GnRH) agonists.
Current Recommendations for DXA Scan Usage in Low Bone Mineral Density Screening

The DXA Interpretation
The DXA scan results were available as T-scores and Z-scores. T-scores of ≤−1.0 to ≥−2.5, and ≤−2.5 define osteopenia and osteoporosis for postmenopausal women or men older than 50 years. A history of fragility fracture is also diagnostic for osteoporosis in this population. For premenopausal women and younger men, Z-score is preferred. Z-score of ≤−2.0 plus a fragility fracture are required for a diagnosis of osteoporosis; a score of ≤−2.0 in the absence of a fracture is defined as “low bone mass for age.” As the majority of patients in this study were postmenopausal women and for ease of data interpretation, results are reported in T-score only.
Statistical Analysis
Prevalence of each indication, demographics, and risk factors were calculated. Differences in means were tested with t-tests and differences in proportions were tested by chi-square or Fisher exact test (where appropriate).
Results
Patient Characteristics
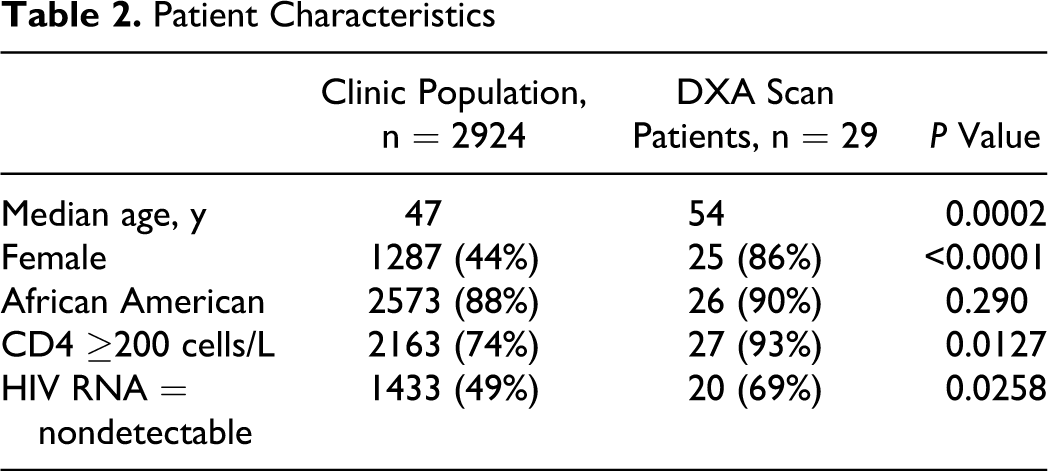
Of the 2924 patients, 30 (1%) had a total of 35 DXA scans. One patient and scan were excluded from the data analysis because of incomplete records. Of the 34 included scans, 26 (76%) were for screening and 8 (24%) were for monitoring. Patients undergoing DXA scans were primarily African American, similar to total clinic population (90% versus 88%, P = .290) but more likely to be women (86% versus 44%, P <.0001) and older (median 54 versus 47 years of age, P = .0002); ages ranged from 44 to 75 years old. They were also more likely to have nondetectable HIV viral loads (69% versus 49%, P = .0106) and have CD4 counts ≥200 cells/L (93% versus 74%, P = .0390; Table 2). Of the patients screened, 96% had T-scores consistent with osteopenia or osteoporosis with a median T-score of −1.9 (range 0.2 to −4.8).
Patient Characteristics
Indication for Screening
The most frequently cited indication for obtaining DXA screening scans was postmenopausal status, early menopause, or estrogen deficiency (18 of 26, 69%). Fracture or kyphosis, bone pain, family history of osteoporosis, and use of “steroid” were each listed as indications in 3 of the 26 patients (12%). Hyperparathyroidism and use of tobacco were each cited twice (8%). Indications noted in 1 patient each included anemia, prostate cancer, use of GnRH agonist, hypothyroidism, low testosterone, rheumatoid arthritis, and vitamin D deficiency. Indications specific to HIV infection were less frequent, with HIV or immunosuppression mentioned in 5 of 26 or 19% and extended use of protease inhibitors (PIs) in 1 of 26 (Table 3).
Indication for Screening DXA Scan

Abbreviation: GnRH, gonadotropin release hormone.
Risk Factors
Patients undergoing screening DXA scans had a median of 3.8 (range 1-9) osteoporosis risk factors in addition to their HIV status. The most common risk factors included perimenopausal or postmenopausal status and use of tobacco use, alcohol, drug, or glucocorticoid (Table 4). Use of HAART was seen in 22 of 26 patients, with the greatest use of PI-based regimens (11 of 26, 42%) over nonnucleoside reverse transcriptase inhibitor-based regimens (7 of 26, 27%), integrase inhibitor-based regimens (2 of 26, 8%), and nucleoside reverse transcriptase inhibitor alone (2 of 26, 8%). A large portion of patients was coinfected with hepatitis C (14 of 26).
Osteoporosis Risk Factors

Abbreviations: SSRI, selective serotonin reuptake inhibitor; PPI, proton pump inhibitor; BMI, body mass index; GnRH, gonadotropin release hormone.
Discussion
Multiple studies have been conducted to examine the pathogenesis and determine risk factors associated with low BMD in HIV-infected patients. However, there is a dearth of information regarding how clinicians should be and are addressing screening for low BMD in these patients.
The USPSTF, AACE, ACOG, and NOF all recommend screening of osteoporosis with DXA scans in women aged 65 years or older. In addition, all recommend screening younger women with increased fracture risk and the NOF also recommends screening some men. The inclusion of HIV/AIDS as a cause of secondary osteoporosis in the 2010 AACE guidelines marks the first mention of the association between HIV and low BMD outside of infectious disease screening guidelines (Table 1). 22 –26
Guidelines for osteoporosis screening in the HIV population are just beginning to evolve. The Infectious Diseases Society of America’s (IDSA) 2010 guidelines do not recommend routine screening of all patients with HIV but note that it should be considered in patients older than 65 years and in those either older than 50 years or postmenopausal if other risk factors for low BMD are present. 27 The European AIDS Clinical Society’s (EACS) guidelines from 2009 suggest biannual assessment of fracture risk using the World Health Organization's fracture risk assessment tool (FRAX) in patients older than 40 years, and counting HIV as an osteoporosis risk factor. If not using the FRAX tool, they advise DXA for postmenopausal women, men older than 50 years, and patients with history of low-trauma fracture, risk of falls, hypogonadism, or use of glucocorticoid. 28 A review article by McComsey et al published in October 2010 suggests screening postmenopausal women, men older than 50 years, and those with history of fracture (Table 1). 29
The present study provides the first data in the literature regarding real life practices of health care providers in screening for low BMD in the HIV population. Only 1% of patients in the clinic had DXA scans, and 96% of patients undergoing screening DXA scans had osteoporosis or osteopenia. Screening was done disproportionately in patients with well-controlled HIV (higher CD4 count and lower HIV viral load), although patients in all stages of HIV infection could benefit from prevention of fracture. Of the patients screened, 81% were women compared with 44% women in the clinic population even though data on HIV and low BMD show that men are also at risk. 30 –32
Postmenopausal status was the most frequently cited indication for screening. Of the 22 women, 19 were noted to be perimenopausal or postmenopausal and 2 were assumed to be based on age (51 and 60 years old); all but 1 had other documented risk factors for osteoporosis, making screening warranted based on IDSA, EACS, and McComsey et al recommendations. However, there are greater discrepancies in screening recommendations for men. For the 4 men who underwent screening, all of whom were diagnosed with low BMD, IDSA guidelines would exclude 3 of 4 and McComsey et al would exclude 2 of 4. The addition of hypogonadism and use of glucocorticoid in EACS guidelines allowed for the inclusion of all 4 in screening. Examples of specific patients and whether their risk factor profile qualified them for screening are provided in Tables 5 and 6. While postmenopausal status alone justified screening in those women, some of the men and premenopausal women would have been excluded using current screening guidelines. Expanding these recommendations to be more inclusive would likely increase detection of low BMD in patients who are not postmenopausal.
Appropriateness of Use of DXA in Women
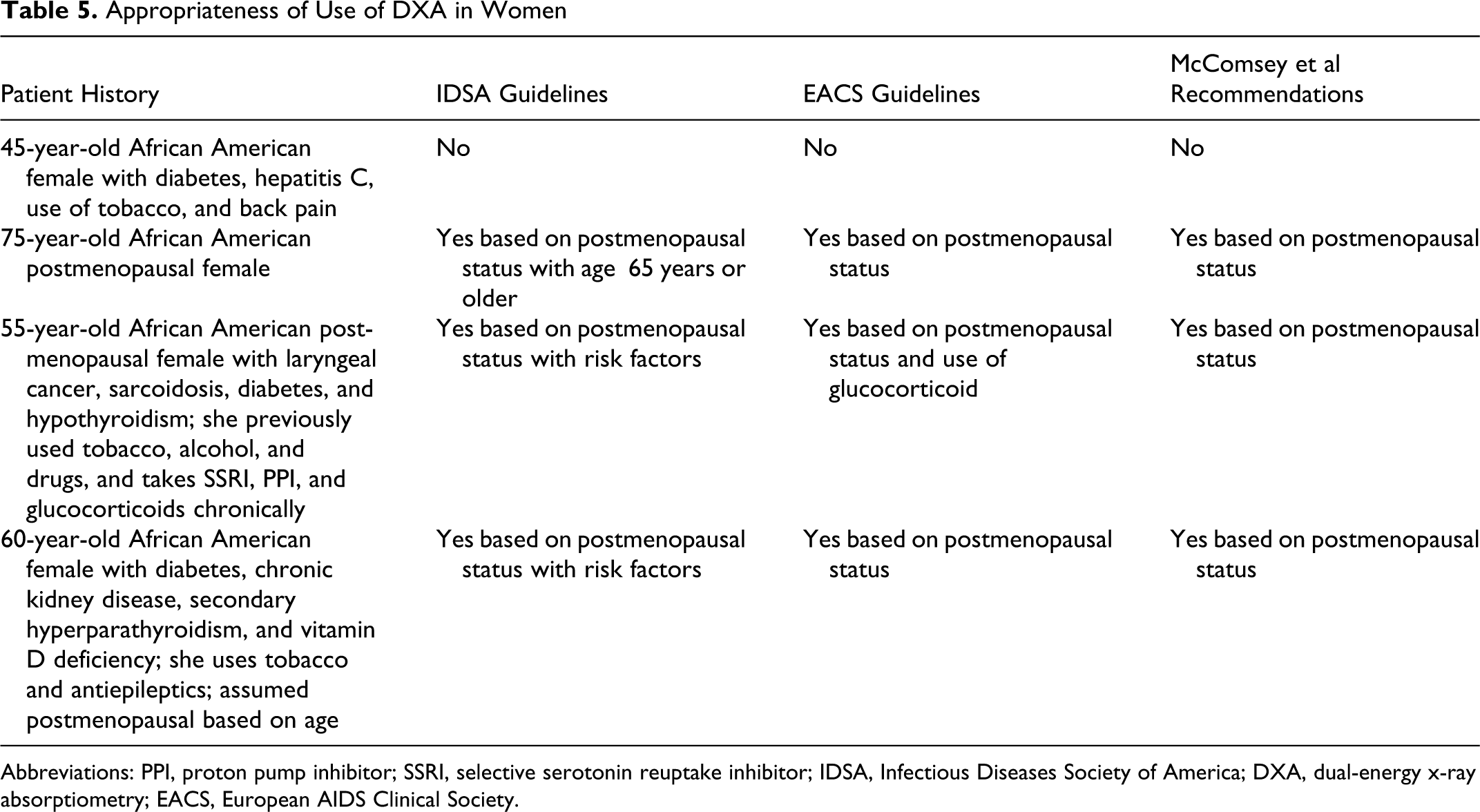
Abbreviations: PPI, proton pump inhibitor; SSRI, selective serotonin reuptake inhibitor; IDSA, Infectious Diseases Society of America; DXA, dual-energy x-ray absorptiometry; EACS, European AIDS Clinical Society.
Appropriateness of Use of DXA in Men
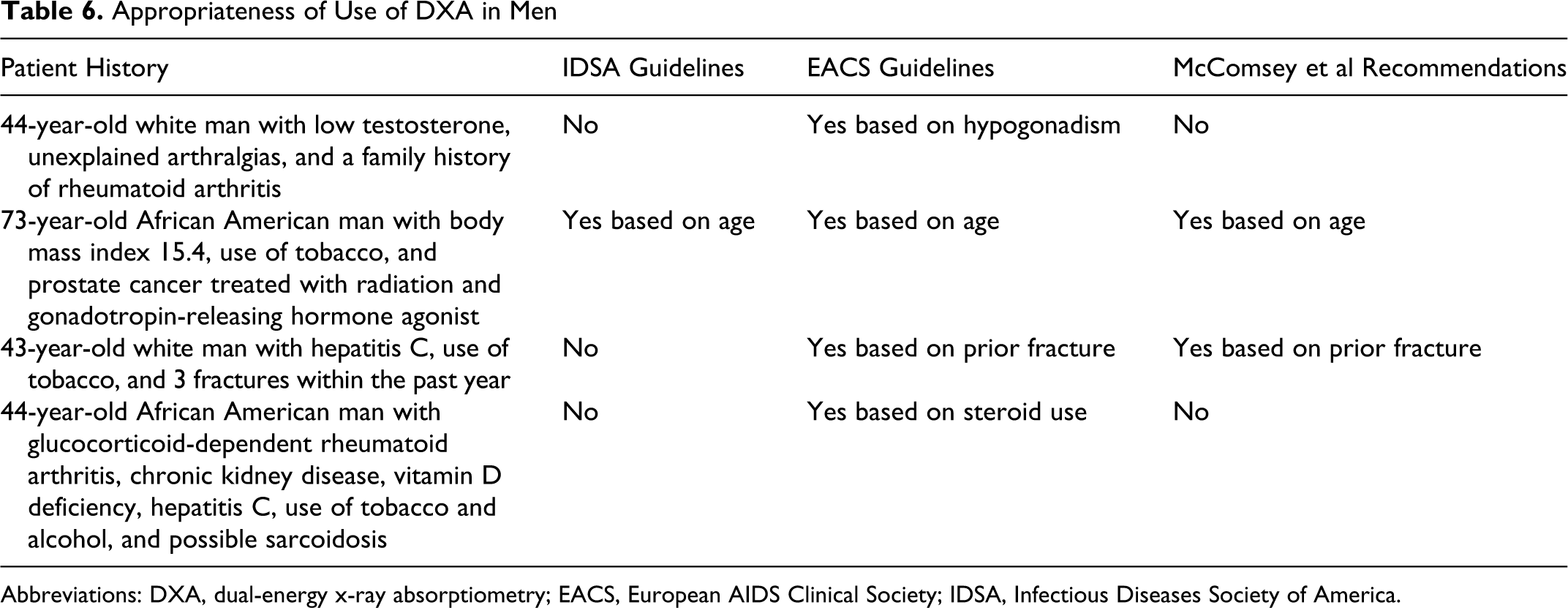
Abbreviations: DXA, dual-energy x-ray absorptiometry; EACS, European AIDS Clinical Society; IDSA, Infectious Diseases Society of America.
The patients undergoing screening DXA scans in this study tended to have multiple risk factors for osteoporosis, with a mean of 3.8 in addition to their HIV infection. This number is likely an underestimate as all the information was elicited by chart review; additional risk factors that might have been discovered by further patient interview, such as low calcium intake, high caffeine intake, or inadequate physical activity were not addressed. Because clinical notes from only 6 months leading up to DXA scan were reviewed, information that is not visited at each appointment, such as family history of low BMD or fracture, use of tobacco, postmenopausal status, and even remote fracture history may have been missed as well.
Even though 96% were diagnosed with osteoporosis or osteopenia, the indications stated by providers were not all appropriate reasons for screening. For instance, anemia, hypothyroidism, and bone pain were all given as reasons for screening but are not present in any of the extensive lists of risk factors in USPSTF, AACE, ACOG, or NOF guidelines. However, a thorough review of the medical charts did reveal multiple other well-established risk factors for osteoporosis even though these were not specified as the reason for screening.
Of 20 providers practicing at this HIV-only clinic in the study period, DXA scans had only been completed in patients of 7 providers. This suggests a potential unfamiliarity of providers with recent literature regarding low BMD in HIV infection.
The primary limitation of this study is the small sample size, with only 30 of 2924 patients having had any DXA scans in a 10-year period. This small sample size shows that HIV providers are insufficiently screening for osteoporosis and limits evaluation of the demographics, risk factors, and DXA scan results. The fact that the source used for the initial screening was only the electronic medical record should not have significantly limited the sample size since paper chart problem lists were abstracted into the electronic medical record. Additionally, it is probable that screening improved as more data on HIV and low BMD became available and that the majority of scans would have been completed later in the study period.
In summary, our study shows that screening for osteoporosis and osteopenia in HIV-infected patients is inadequate, given both the high rates of these conditions and the lack of any screening DXA scans by the majority of providers. More specific and inclusive guidelines are needed to improve osteoporosis screening in HIV-infected patients.
Footnotes
Authors’ Note
Presented in part as an electronic poster at the 6th International AIDS Society Conference on HIV Pathogenesis, Treatment & Prevention (Rome, Italy; July 17-20, 2011); Abstract A-361-0080-02876.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.