
Abstract
Research has demonstrated that strict adherence is necessary to maximize highly active antiretroviral therapy (HAART) benefits. This is particularly challenging for low-literacy populations in resource-limited settings like Morocco and motivated the implementation of a psychoeducative program for patients under HAART at Rabat University Hospital. The study aimed at assessing the program’s impact on adherence to antiretroviral medication, knowledge of HIV/AIDS and HAART, quality of life, and biological parameters. It included patients under treatment for at least 2 months that benefited from 3 to 5 educational and psychological support sessions. Data were collected at baseline, 3 and 6 months. In all, 50 patients were included. The mean age was 38 years; 52% were illiterate and 62% unemployed. Adherence scores were high at baseline (98%) and showed no significant change throughout the study. Knowledge of HAART and HIV/AIDS, and quality of life improved significantly both at months 3 and 6. Significant increase for CD4 count rates and decrease for viral load rates were also reported. The program had no significant impact on adherence but substantively developed patients' knowledge of HIV/AIDS and HAART and improved their quality of life.
Introduction
The introduction of highly active antiretroviral therapy (HAART) has dramatically improved the prognosis of HIV infection.1,2 However, the full benefits of HAART are contingent upon high adherence, 3 which can be challenging to achieve, due to the multiple and complex factors influencing it. Fear of stigmatization, omission of pills, complicated regimens, and poor understanding of treatment mechanisms of action have all been found to hinder patients' ability to take their treatment consistently.4,5 Patients in developing countries experience further constraints due to poverty and illiteracy, making it essential to implement effective strategies to improve adherence and to maintain it at good levels.3,6
Morocco is a low middle-income country with 14% of the population living under the poverty line 7 and with illiteracy rates reaching 48%. 8 The number of people currently living with HIV is estimated at 21 000 and HIV prevalence in the country is 0.1% among adults aged 15 to 49. 9 Unprotected heterosexual intercourse is the primary mode of transmission, accounting for 78% of all known HIV infections. 10
HAART was introduced in 1998 and made accessible free of cost in 2003, after the approval of the Country Round 1 proposal by the Global Fund for HIV/AIDS, Tuberculosis & Malaria, thereby increasing access of patients in need of HAART from 12% in 2004 to 30% in 2007. 10 Despite free access to treatment, which is crucial in ensuring good adherence in resource-limited settings, 11 Moroccan patients face other obstacles related to poor literacy levels, low economic status, and profound social stigmatization of HIV, which place considerable strain on them and on their families and may hinder their abilities to reach and sustain adequate adherence levels.
In light of this, the HIV/AIDS Unit of the Internal Medicine A Department at the University Hospital of Rabat implemented a psychoeducative program for patients under HAART in November 2006. This study evaluated the impact of this program on patients' adherence to HAART, knowledge on HIV/AIDS and its treatments, virologic and immunologic parameters, and health-related quality of life (HR-QoL).
Methods
Study Design and Patients
We conducted a prospective, open, nonrandomized study from November 2006 to September 2007 at the HIV/AIDS Unit of the Internal Medicine Department of Ibn Sina University Hospital in Rabat. It was approved by the University Hospital Ethics Committee and patients included responded to the following criteria:
12
tested HIV positive (with a confirmation by ELISA and Western Blot tests) attended regularly the HIV and AIDS Unit consultations were under HAART for at least 2 months before inclusion gave written informed consent.
Data regarding patients' levels of adherence, knowledge of HIV/AIDS and HAART, CD4 counts, plasma viral loads, and HR-QoL were collected at baseline, month 3 and month 6.
Psychoeducative Program
Prior to the implementation of the program, standard care of patients addressed only the clinical aspect and consisted of a medical consultation to monitor the clinical status and biological data and to deliver the treatment. The educational component focused solely on instructions for treatment uptake, without explaining the linkages between good adherence and physical, biological, and psychological benefits. No information on the natural history of the infection and its evolution was included and psychological support was absent.
The psychoeducative program was implemented in partnership with the Association Marocaine de Lutte Contre le SIDA (ALCS), who provided the educators, psychologist, and educational materials.
Every patient received in total 3 to 5 one-hour personalized educational and psychological support sessions at each medical consultation. Sessions were delivered by a multidisciplinary team who had previously received a 4-day training in communication and education techniques. The program team comprised: A volunteer medical intern, in charge of performing the adherence, knowledge, and quality of life assessments. The intern was newly recruited, to avoid bias in assessing adherence by a health care professional previously involved in patients' care. The forms were forwarded afterward to the educator to adapt the content of the educational session to the patient’s specific needs. A physician, responsible of monitoring the patient’s clinical status, biological data, and treatment. An educator, responsible of the therapeutic educational sessions based on the following educational resources: a folder featuring pictorial information on HIV transmission modes, prevention methods and mechanisms of action of HAART, accessible to a low-literacy audience, a treatment planning chart, with self-adhesive stickers showing a daily medication-taking schedule to improve treatment management strategies, a symptoms card game, showing the potential side effects of HAART and the corresponding appropriate actions to be undertaken by the patient, a psychosocial situations card game, aimed at preparing the patient to real-life situations that she/he is likely to experience; such as taking medication in public, planning a pregnancy, revealing the serologic status to the partner etc. A psychologist in charge of the individualized psychological support sessions, combining both cognitive and behavioral approaches.
Given the cultural context and the nature of the program, key positions for the intervention—the volunteer medical intern, and educator—were deliberately selected women, as female patients tend to feel more comfortable and at ease with female health care providers, while male patients tend to be more flexible. Two physicians were in charge of the medical consultations; a male and a female physician, to which patients were allocated taking into account their clinical care history and physicians' availability.
The circuit set at the HIV/AIDS Unit for each patient benefiting from the program is summarized in Figure 1.

Psychoeducative program circuit for enrolled patients at the HIV/AIDS Unit.
Assessment Tools
The program was assessed through interviewer-administered questionnaires at baseline (M0), month 3 (M3), and month 6 (M6), filled out at the beginning of each consultation. Each questionnaire included the following: The AIDS Clinical Trials Group (ACTG)
13
questionnaire on adherence, evaluating patients' quantitative adherence for the 4 days prior to the consultation. The adherence score was calculated by dividing the number of pills taken by the number of pills initially prescribed and ranged from 0 (no pill taken at all) to 1 (perfect adherence). Qualitative adherence, related to patients' respect for the medication-taking schedule and instructions, was also assessed for the 4 days prior to the consultation, providing scores ranging from 0 (never respected instructions) to 4 (always respected instructions). In absence of a “gold standard” adherence metric, and considering the cost-related, social, and cultural constraints inherent to the specific context of our study, questionnaires administered by a newly recruited health care professional were the most pertinent option, being quick to perform, inexpensive, and easily reproducible. Knowledge items with 2 sections: one exploring patients' knowledge of their treatment (drugs' names, doses, storage conditions) and marked from 3 (highest) to 0 (lowest) for each item and another section examining patients' knowledge of the HIV transmission routes, prevention modes, and clinical and biological monitoring. The scores for each question of this second section were 1 for correct answers, -1 for wrong answers, and 0 if the patient did not answer. Health-related Quality of Life (HR-QoL) questionnaire EQ5D,
14
including 5 items evaluating patients' capacities in terms of mobility, self-care, daily activity and levels of pain, anxiety, and depression. It also included a visual index scale for patients to mark their overall health-related quality of life from 0 (the lowest) to 100 (the highest).
In addition, CD4 count and plasma viral load were measured every 3 months, to examine the impact on patients' health status.
Statistical Analysis
The analysis was performed through SPSS 13.0 Software. Quantitative variables were expressed in means and standard deviations or medians and extremes, according to their distribution. They were compared using Wilcoxon or Friedman tests. Qualitative variables were compared by chi-square or Fisher tests. The significance threshold was .05
Results
In all, 50 patients were included. One patient died between M3 and M6 from causes unrelated to her HIV status; 58% were female and 42% male, with a mean age of 38.6 (±8.6); 52% were illiterate and 74% resided in urban areas; 62% were unemployed and 14% had only a temporary job; and 60% were classified under the category C of the Centre for Disease Control Classification.
The mean duration of treatment at inclusion was 16 months, with a minimum of 2 months and a maximum of 72, and with 44% of the patients having been under treatment for less than 1 year.
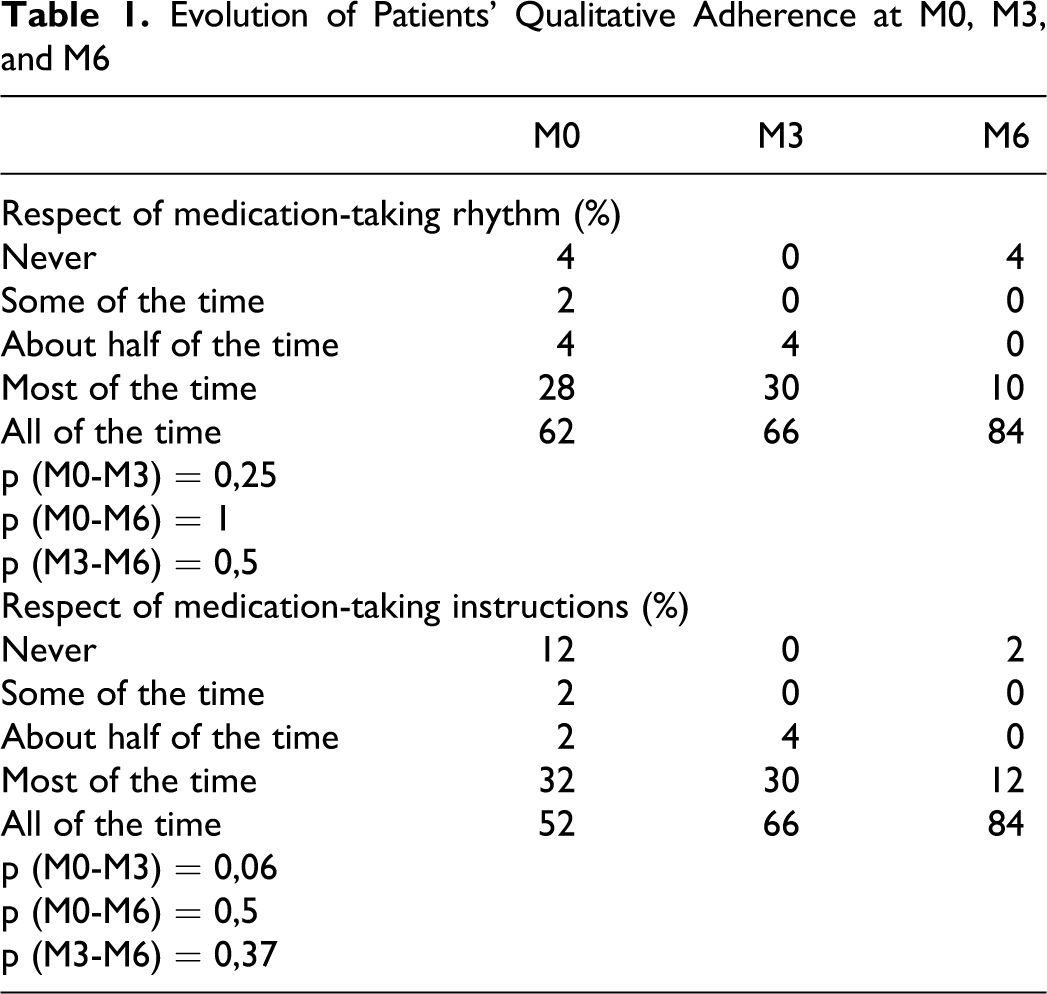
The medians of adherence scores showed no change (P = .266); they were already at the optimal level of 1 at baseline and remained so throughout the study (Figure 2). There was no significant impact of the program on qualitative adherence either, though it was slightly improved at the individual level, with the proportion of patients respecting medication-taking instructions all the time increasing from 52% at baseline to 84% at M6. Similarly, those observing their medication-taking schedule as prescribed all the time were 62% at the beginning of the study and 84% at the end (Table 1).

Evolution of quantitative adherence scores' medians at M0, M3, and M6.
Evolution of Patients' Qualitative Adherence at M0, M3, and M6
Both HIV/AIDS and HAART knowledge scores increased significantly from baseline to M6 (P < .001) with the median for HIV and AIDS reaching the maximum score at M6 (Figures 3 and 4).

Evolution of HAART-management knowledge scores at M0, M3, and M6.

Evolution of HIV/AIDS knowledge scores' medians at M0, M3, and M6.
Patients with an undetectable viral load were 52% at baseline and reached 72% at M6 (P = .05). CD4 count medians increased significantly throughout the study (P < .001); from 288.5/mm3 to 554/mm3, which corresponded to a raise of 92% (Figures 5 and 6).

Evolution of viral load medians at M0, M3, and M6.

Evolution of CD4 count medians at M0, M3, and M6.
HR-QoL median scores improved considerably and continuously throughout the study (P < .001) reaching the maximum score of 1 at M6 (Figure 7). Further, quality-of-life scores on the visual scale showed a significant increase, from a median of 60 at baseline to 70 at M3 and reaching 80 at M6 (P < .001; Figure 8).

Evolution of HR-QoL scores' medians at M0, M3, and M6.
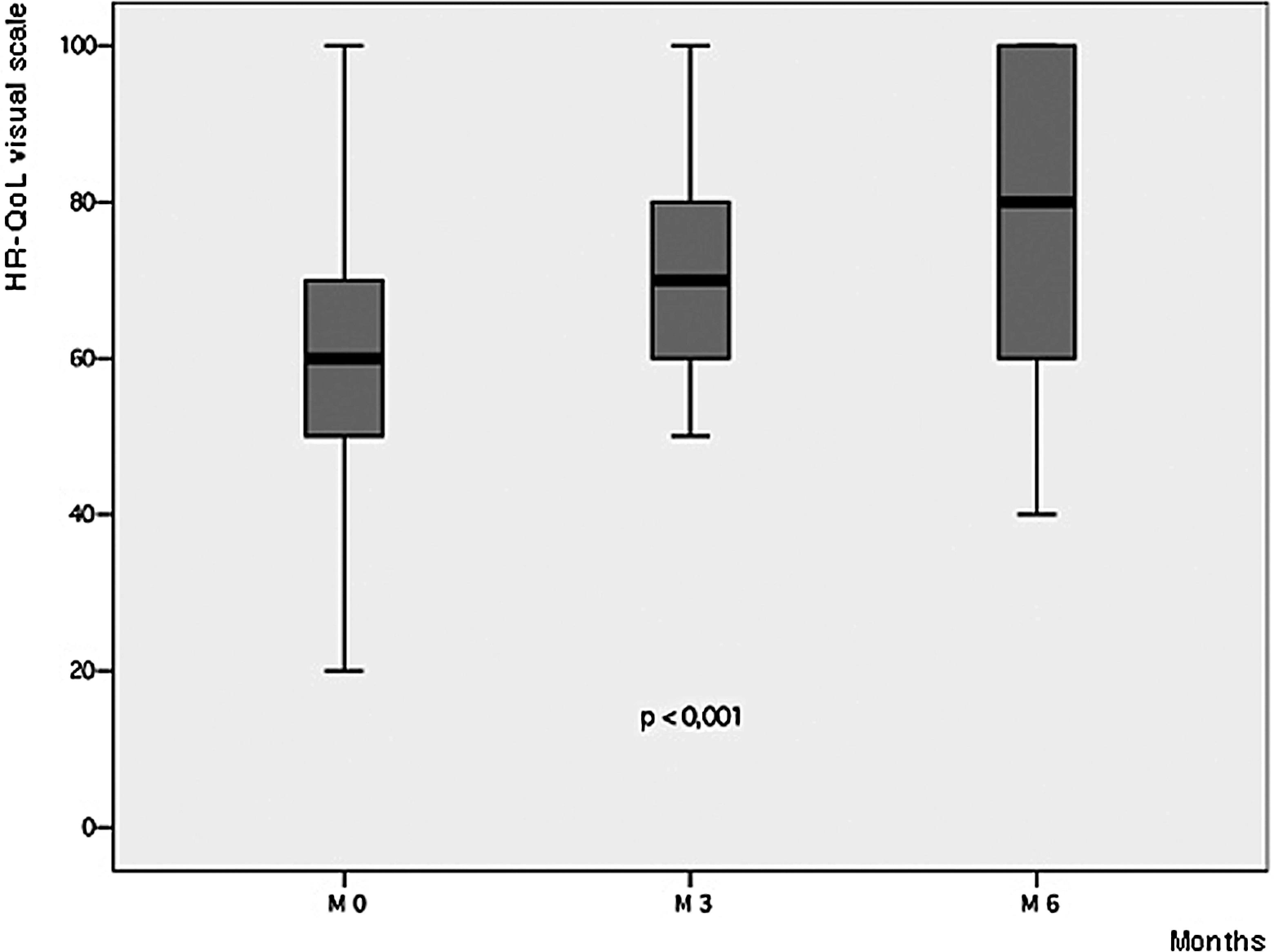
Evolution of HR-Qol visual scale scores’ medians at M0, M3, and M6.
Discussion
This study demonstrated that patients derived considerable benefits from the implementation of the psychoeducative program.
In terms of adherence, quantitative assessments did not show any significant changes: the median adherence score was maximal (=1) at baseline and remained at this level at M3 and M6. Patients were adequately adherent prior to enrolling into the program, which could be explained by several hypotheses. First, the majority (60%) was diagnosed at the AIDS stage and the dramatic improvement experienced after starting HAART may have been a strong adherence driver. 15 Second, it is important to highlight some of the radical methods previously used by the health care team to foster adherence while initiating HAART through religious oaths over strict observance of medication-taking prescriptions and threats to suspend delivery of treatment otherwise. Institutional factors are also important to emphasize, since free access to HAART and uninterrupted supply have proven to be crucial to achieve and maintain good levels of adherence in resource-constrained settings.6,16,17
In a 12-month study conducted to evaluate the impact of a similar intervention on a comparable group of 96 patients at the University Hospital of Casablanca, Marchand et al found a baseline adherence score of 0.7, which improved at M3, amounting to 0.87, and to 0.91 at M12. 18 In another resource-limited setting at Jos University Hospital in Nigeria, Abah et al examined the impact of a program to support adherence among 121 patients recently enrolled in the Harvard-Pepfar HAART initiative and showed that the proportion of patients who had an adherence level superior to 95% increased from 79.4% of the cohort at the beginning of the study, to 92.4% at the end. 19 The differences between the populations studied and the type of care and adherence information and support received prior to the implementation of educational programs could explain the various results obtained. We did not observe any statistically significant improvement of qualitative adherence, though at the individual level, the proportion of patients who respected medication-taking schedule all the time increased noticeably; from 52% at baseline to 66% at M3 and 84% at M6. Likewise, patients who took their treatment following the instructions all the time formed 62% of the cohort at baseline, 66% at M3, and reached 84% at M6. This was likely due to the educational sessions that enabled patients to understand the mechanisms of action of their medicines and the importance of disciplined medication-taking. Similar results were reported by Pradier et al 20 who described the efficacy of structured counseling and educational interventions to enhance adherence to HAART through developing patients' self-care management abilities.
Knowledge of HAART management and HIV/AIDS improved significantly (P < .001) and continuously between M0, M3, and M6. Weak baseline scores could be attributed to patients' low educational level, as more than half of the cohort was illiterate, but also to the lack of explanations from the health care team on the disease and on the principles of treatment. There was excessive emphasis put on strict adherence without providing patients with the necessary information on the dynamics of HIV replication and the mechanisms of action of the different antiretroviral drugs, both of which justify the need for a strict adherence. The categorization of patients as passive recipients of care is quite frequent in public health structures in Morocco, as patients who usually resort to public health facilities have often a poor economic status and a low literacy level, and tend to follow the instructions of the health care team without questioning them. Health care professionals are also poorly trained to actively involve patients in therapeutic management and decision-making processes and are often burdened by excessive demands on their time due to the lack of human resources in public health facilities. 21 Similar results were reported by Marchand et al, 18 though a slight decrease in the median of knowledge scores was observed during the second half of the study, as most educational sessions were delivered during the first half. The knowledge acquired may have been forgotten or modified in absence of reactivation of the learning process, 22 which pinpoints the necessity to establish sustainable follow-up mechanisms adapted to the educational needs of patients. Furthermore, in a low-literacy population that benefited from nurse-delivered antiretroviral treatment adherence, Kalichman et al showed an important improvement of patients' knowledge and respect for medication-taking instructions, 23 and in a study conducted by Weiss et al 24 among 997 patients on the linkages between HIV and HAART knowledge and adherence, patients' level of knowledge was found to be significantly associated with better adherence to treatment.
Though our patients adequately adhered from baseline and regardless of their knowledge level, we can argue that a long-term follow up on the educational sessions would maintain the level of knowledge acquired at M6 through a permanent reactivation of the understanding of simple yet key elements of viral physiology and HAART principles and would help prevent adherence breaks.
We also found positive biological outcomes, with a significant increase for CD4 count rates (P < .001) and a proportion of patients with virologic undetectability increased by 40% between baseline and M6. These trends reflected the optimal adherence levels reported and their positive impact on patients' biological parameters. Marchand et al, Abah et al, and Dieckhaus et al reported all improvements in biological outcomes due to an educational program too, with a significant decrease in patients' viral load medians and increase in CD4 count medians.18,19,25 Interestingly, the study of Goujard et al 26 demonstrated an increased adherence to medication and a consistent impact on knowledge, but these elements did not translate into measurably better immunologic or virologic outcomes. We could point at the differences between the study populations and the initial levels of biological parameters to explain these different findings. However, a meta-analysis of randomized controlled trials evaluating educational interventions on HAART adherence performed by Simoni et al 27 confirmed that they tended to have a positive impact on immunovirologic data, showing an undetectable viral load of 62% for all patients who had benefited from an intervention, versus 55% for patients in control groups.
HR-QoL is a crucial concern for patients under HAART, 28 but it has been poorly addressed by research. In our study, HR-QoL scores' medians improved importantly from baseline to M3 (P < .001), reaching the optimum rate of 1 at M3 and remaining at the same level at M6. Similarly, medians of HR-QoL visual scale scores increased continuously from M0 to M6. The rapid positive evolution of HR-QoL between M0 and M3 and its timing right after implementation of the initiative supported the strong linkages between the psychoeducative program and the improvement of patients' quality of life.
Indeed, through exploring patients' individual experiences living with HIV and their perceptions of the disease; through identifying and addressing their uncertainties, fears, and feelings of loneliness and despair; and through working on their self-confidence and esteem, the program helped them to mobilize the necessary capacities to build a stable emotional state and to establish strategies enabling them to face circumstances or situations that may have a negative impact on this stability. 28 The psychological support sessions also offered a space where social obstacles such as stigmatization, discrimination, and silence around the HIV status inside the family or in working settings were identified and analyzed, and solutions to overcome these barriers were discussed. The desire to build new relationships or to found a family arose for several patients. Some of them asked to meet other HIV-positive people and suggested to replace the individual psychological support sessions by group therapies where they could share their experiences, concerns, and needs with other HIV-positive patients. Along with the effects of the psychological support sessions, which substantively addressed the emotional and social aspects of patients' life, we can argue that the improvement of patients' knowledge of their disease and treatment also contributed to improve their quality of life, as it positioned them as active and knowledgeable partners in their clinical, biological, and therapeutic management and no longer as mere passive recipients, reducing their feeling of fatality and impotence with regard to the disease.
Similar positive results have been reported in other studies which looked at the impact of psychological support interventions on patients' quality of life. Pradier et al described the major benefit as the creation of a dialogue platform for patients, positively modifying their perception of the entire health care facility, which they started to see as a space for sharing and emotional balancing. 20 In a randomized trial, Murphy et al also showed the positive impact of psychological support on the mental health of the intervention group in comparison with the control group. 29 Goujard et al did not find any significant change in quality-of-life scores between intervention and control groups and attributed these results to a “ceiling effect,” as most patients recruited for the intervention group were asymptomatic and had already a high HR-QoL score at baseline. 26 In a meta-analysis conducted by Crepaz et al on the impact of cognitive and behavioral interventions on HIV-positive patients' psychological status in 15 clinical randomized trials, symptoms of anxiety, depression, and stress—which formed part of the assessment of our patients' quality of life, in addition to mobility, daily activities, and feeling of pain—were found to have improved. 30
We are aware of the potential biases and limitations of this study. First, the absence of a control group is a major limitation, as the comparison of the outcomes of the experimental group to those of a control group would have given more consistency to our results. Second, we only recruited patients who were regularly monitored and this might have influenced our results, as patients regularly attending medical consultations are more likely to adhere properly to their medication. Also, due to the low level of education of the population, most questionnaires were administered by a health care professional and not individually filled out by patients. Despite efforts in ensuring a safe environment for patients to comfortably share their medication-taking behaviors by administering questionnaires by a newly recruited and trained medical intern, the interviewer-administered approach might have influenced the responses given. Lastly, the lack of long-term follow-up is also a limitation of our study and a more extended evaluation period would have enabled us to better assess the long-term impact of the intervention.
Conclusion
This study brought additional evidence on the positive impact of psychoeducative interventions for HIV-positive patients under HAART in resource-limited settings.
Through a comprehensive approach, combining educational and psychological support components and integrating psychosocial aspects into patients' care, the program helped to establish crucial linkages between the disease, the emotional status, and the social life of patients, and to effectively address potential threats to their stability and adequate treatment management. The dramatic improvement in patients' quality of life was one of its major achievements and provides evidence for all health professionals involved in HIV care to further invest in the quality of life of people living with HIV.
Footnotes
Study presented at the Poster exhibition of the XVII International AIDS Conference, August 3-8, 2008, Mexico City (THPE0139). Source of support for attendance of the conference: Mexico Youth Force.
Acknowledgments
The authors of this article would like to thank all patients who participated to the study. They extend their gratitude to the ALCS team for supporting the implementation of the psychoeducative programme and to the medical and paramedical staff of the Internal Medicine A Department at the Ibn Sina University Hospital.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.