
Abstract
Venous insufficiency mostly arises from valvular incompetence in the great saphenous vein (GSV) and small saphenous vein (SSV). However, non-saphenous reflux (NSR) remains relatively unexplored in clinical practice and ultrasound investigations. This study reports an uncommon anatomical finding and the associated venous reflux, which is believed to involve the peripheral nerve. A systematic database search was conducted to identify patients from our clinic previously diagnosed with an interfascial vein in the lateral calf compartment during duplex ultrasound examination. Subsequently, a questionnaire was distributed to those who volunteered to participate, collecting further demographic details and clinical information related to peripheral neuropathy of the calf. Ultrasound findings, including venous competency and diameter measurements, were included for data analysis. In total, 20 legs with an interfascial vein were identified from 19 patients between 2008 and 2022. Of the 6 patients who returned the questionnaire and provided consent for inclusion, 2 reported lateral calf pain in the lower calf. Calf numbness was noted in 2 patients, primarily affecting the upper and mid portions with 2 further patients reporting foot drop. Reflux flow in the interfascial vein was detected in 5 patients. Sonographic findings revealed interfascial vein diameters range from 1.1 to 4.0 mm, with a mean of 2.4 mm. The distance between the interfascial vein and SSV varied, with a mean of 36.3 mm. Based on topographic anatomy and reflux flow originating from sciatic nerve varices, we hypothesize that the interfascial vein identified in our patients likely represents the superficial peroneal nerve vein. This study sheds light on the existence of an interfascial vein in the lateral calf compartment and its role in producing lateral calf neuropathy.
Introduction
Venous insufficiency occurs when valves are unable to prevent backflow, resulting in varicose veins which can be visually disturbing and painful, and other associated signs and symptoms. This ailment predominantly affects the superficial veins of the lower limb, notably the great saphenous vein (GSV; 82.7%) and small saphenous vein (SSV; 10.9%). 1 The literature provides compelling evidence on the distribution and patterns of saphenous reflux.2-4 However, there is a gap in recent research concerning the various forms of non-saphenous reflux (NSR). 5 With advancements in ultrasound technology and improved visualization of smaller veins, an increasing number of veins associated with anatomical variations are being discovered during meticulous ultrasound examinations. In this case series study, we report a rare type of NSR occurring in an interfascial vein within the lateral compartment of the calf.
Methods
This ambispective cohort study was conducted by a group of experienced vascular surgeons and sonographers in 2023. The retrospective investigation involved searching the Western Sydney Vascular Laboratory’s (NSW, Australia) database for venous insufficiency duplex ultrasound (DUS) examinations performed between January 1, 2008 and December 31, 2022. The focus was on sonographic findings related to veins in the lateral compartment of the leg, employing keywords, such as “lateral SSV,” “lateral accessory SSV,” “interfascial vein,” “intrafascial,” “lateral calf vein,” and “parallel to the SSV.” Exclusion criteria included patients under 18 years of age or those who did not complete their DUS for any reason. Those whose reports met the criteria were contacted and, if willing, consented to participate in the study. Their medical records, archived images, and ultrasound reports underwent a thorough review for data analysis. A prospective study then collected demographic details and clinical information pertaining specifically to peripheral neuropathy of the calf through a distributed survey questionnaire. Our study was approved by the Human Research Ethics Committee of the University of Sydney (Protocol No. 2022/667).
Results
Twenty legs from 19 patients were identified with interfascial vein(s) in the lateral calf compartment. Six patients provided written consent and completed the survey questionnaire.
Table 1 presents the demographics, clinical characteristics, and clinical presentations of the included patients (right leg—3; left leg—3). There were 4 females and 2 males with a mean age of 65.7 years (range = 38-85 years). The participants’ ethnicity included Asian (3), Caucasian (2), and Middle Eastern (1). The body mass index (BMI) was unavailable for 2 patients, normal for another 2, and indicated overweight for 2. Three of the 4 females had between 2 and 4 pregnancies. With regards to surgical history, 1 participant had a total knee replacement and 2 had varicose veins surgery. Based on the Clinical-Etiology-Anatomy-Pathophysiology (CEAP) classification, the patient’s clinical severity was graded as C1 (1), C2 (1), C3 (0), C4 (2), C5 (1), and C6 (1).
The Demographics, Clinical Characteristics, and Clinical Presentations of the Patients Who Were Identified With an Interfascial Vein in the Lateral Compartment of the Calf.
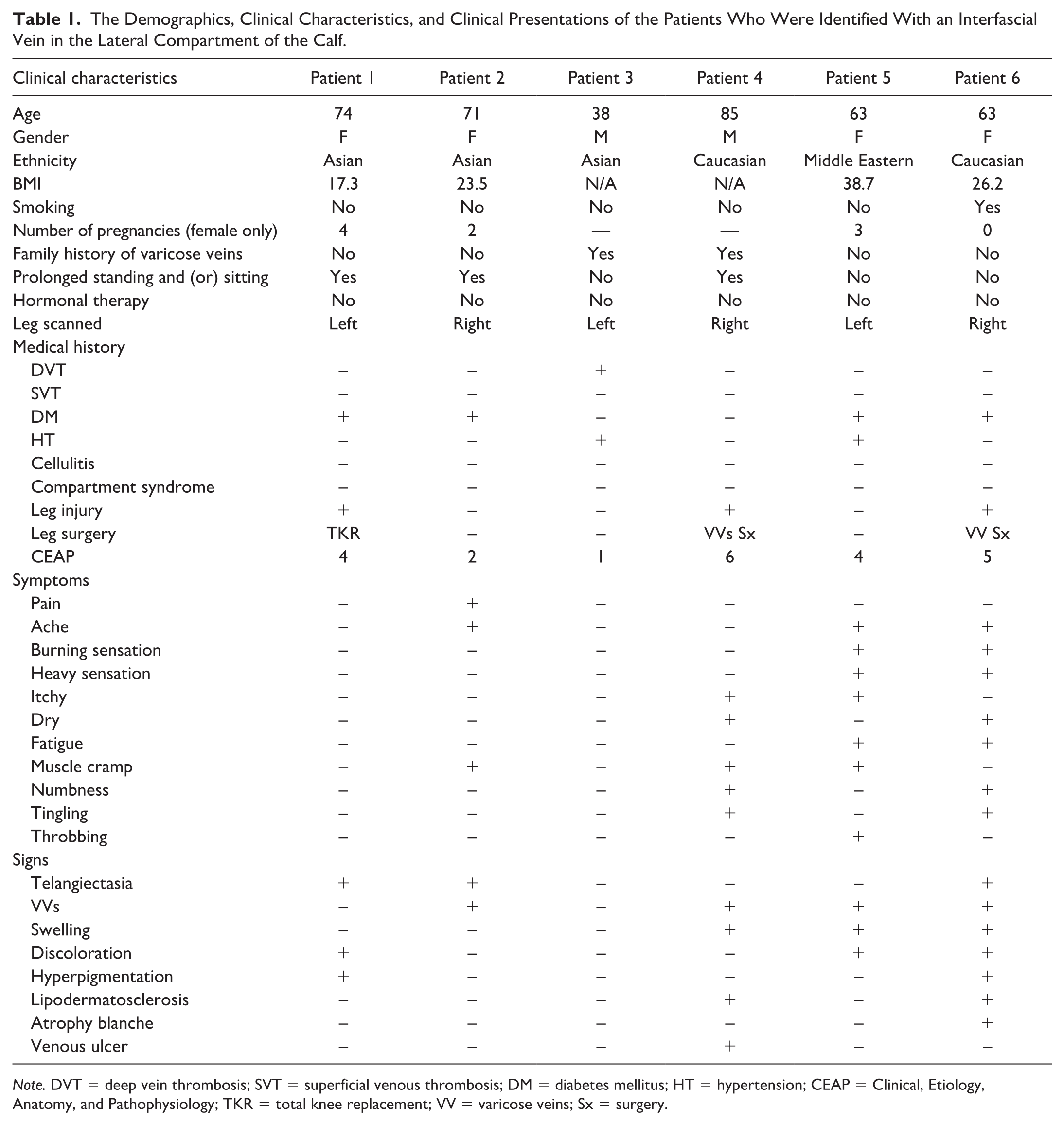
Note. DVT = deep vein thrombosis; SVT = superficial venous thrombosis; DM = diabetes mellitus; HT = hypertension; CEAP = Clinical, Etiology, Anatomy, and Pathophysiology; TKR = total knee replacement; VV = varicose veins; Sx = surgery.
Table 2 outlines the clinical symptoms in the lateral calf and presents sonographic findings related to the interfascial vein located in the lateral calf compartment. None of the 6 patients were clinically diagnosed with sciatica. Two patients reported experiencing lateral calf pain, both localized in the lower calf. Calf numbness was observed in 2 patients, predominantly affecting the upper and mid portions. In addition, 2 patients mentioned having foot drop. Venous reflux was detected in 5 of the 6 patients. The maximum diameter of the interfascial vein ranged from 1.1 to 4.0 mm, with a mean of 2.4 mm (SD = ±1.0). A considerable variation in the distance between the SSV and the interfascial vein was found among patients, with a mean of 36.3 mm (SD = ±29.1).
Clinical Symptoms and Sonographic Findings Specific to the Lateral Calf Compartment and the Interfascial Vein.
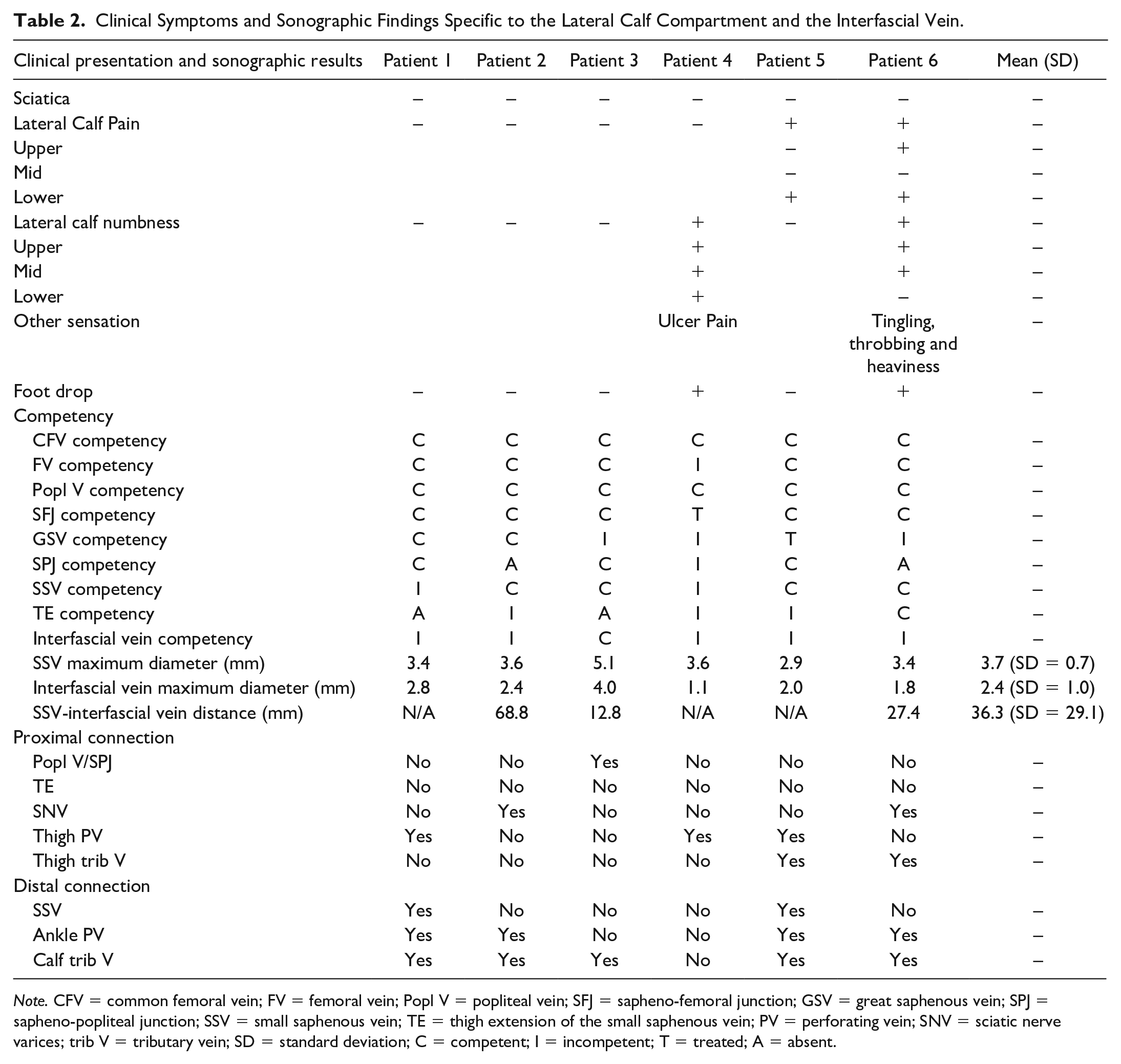
Note. CFV = common femoral vein; FV = femoral vein; Popl V = popliteal vein; SFJ = sapheno-femoral junction; GSV = great saphenous vein; SPJ = sapheno-popliteal junction; SSV = small saphenous vein; TE = thigh extension of the small saphenous vein; PV = perforating vein; SNV = sciatic nerve varices; trib V = tributary vein; SD = standard deviation; C = competent; I = incompetent; T = treated; A = absent.
When categorizing patients into competent or incompetent groups according to normal or reflux flow in the interfacial vein (group I—competent; group II—incompetent), as outlined in Table 3, noticeable distinctions were found between the 2 groups in terms of symptoms, and proximal and distal connections; however, no statistically significant difference was identified as described below.
Clinical Symptoms and Sonographic Findings in Groups With Competent and Incompetent Interfascial Vein Located in the Lateral Calf Compartment.
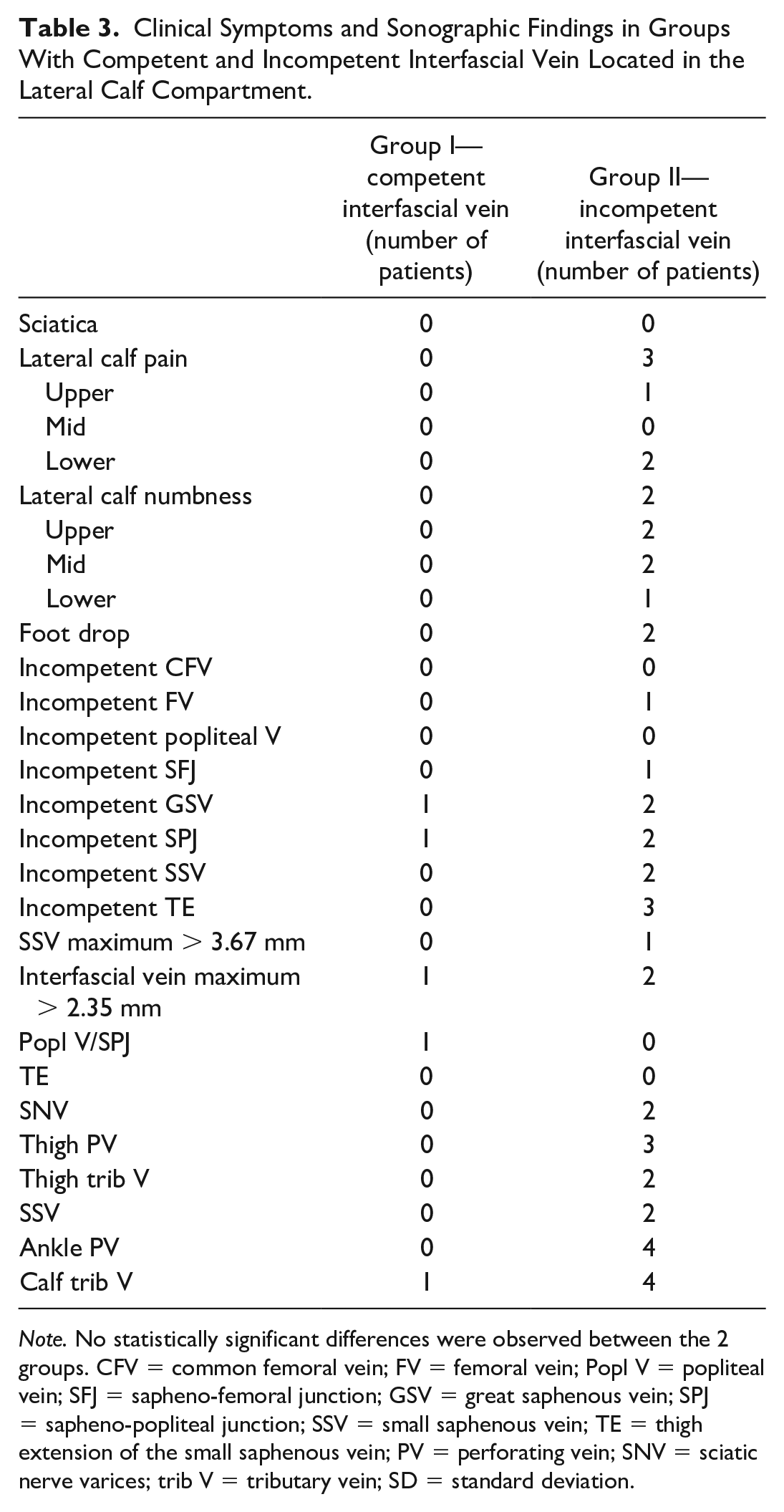
Note. No statistically significant differences were observed between the 2 groups. CFV = common femoral vein; FV = femoral vein; Popl V = popliteal vein; SFJ = sapheno-femoral junction; GSV = great saphenous vein; SPJ = sapheno-popliteal junction; SSV = small saphenous vein; TE = thigh extension of the small saphenous vein; PV = perforating vein; SNV = sciatic nerve varices; trib V = tributary vein; SD = standard deviation.
Case Report and Sonographic Findings (Patient 6)
To illustrate the findings of an interfacial vein, we further discuss patient 6, a 63-year-old female patient who attended the vascular laboratory with chronic venous insufficiency affecting both legs (see Figure 1). She reported experiencing bilateral aching and discomfort but never had any venous treatment. Her right leg DUS examination indicated normal deep venous drainage, including the common femoral vein (CFV), femoral vein (FV), and popliteal vein. The sapheno-femoral junction (SFJ) was competent. However, GSV incompetence was demonstrated with reflux flow originating from incompetent lymph node venous networks. The sapheno-popliteal junction (SPJ) was congenitally absent, and both the SSV and thigh extension (TE) demonstrated venous flow in the normal direction. An interfascial vein within the lateral calf compartment in a spiral course was identified with reflux originating from the veins of the sciatic nerve (see Figure 2–4).

Clinical image of the patient who had an interfascial vein in the lateral calf compartment (use of photos with written permission from the patient). While the interfascial vein may not be easily visualized on the skin surface, its associated varicose tributary veins can be observed in the posterolateral region of the lower calf.
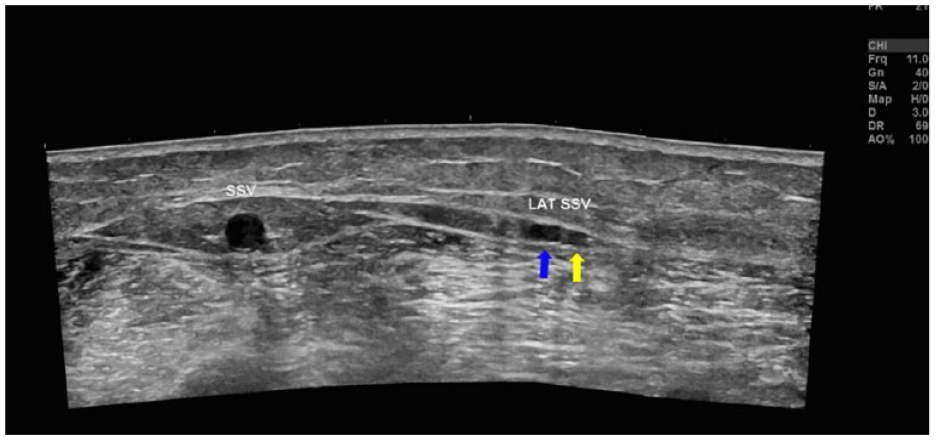
Panoramic view of the posterolateral calf showing the topographic location of the interfascial vein in relation to the SSV. Blue arrow: interfascial vein (labeled as LAT SSV in the image); yellow arrow: superficial peroneal nerve.
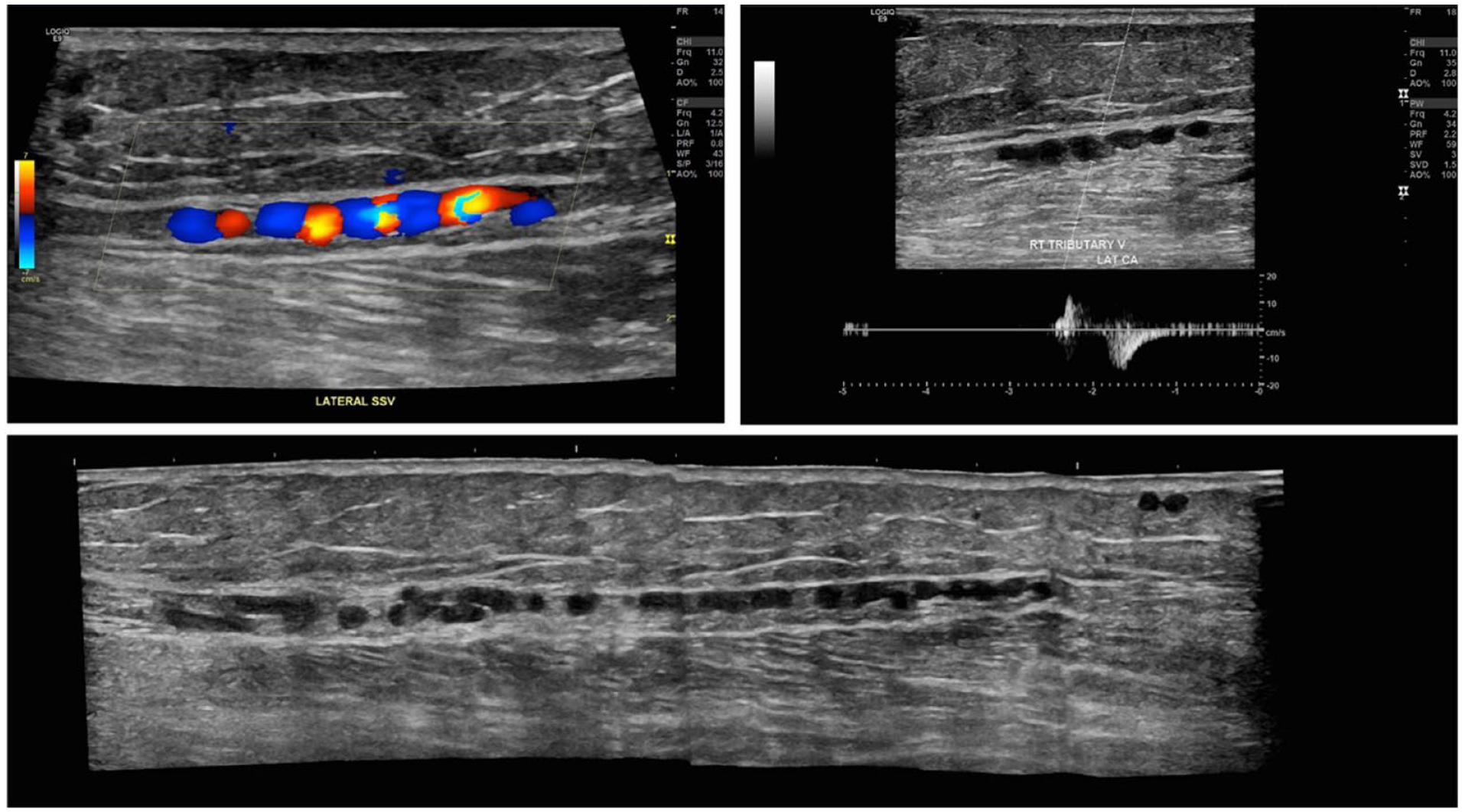
Longitudinal view of the interfascial vein in the lateral calf compartment. Top left: color Doppler shows the spiral course of the vein resembling a “string of beads” sonographic appearance. Top right: spectral Doppler analysis demonstrates venous reflux with provocative maneuver. Bottom: Panoramic view of the interfascial vein in the long axis showing the spiral course.
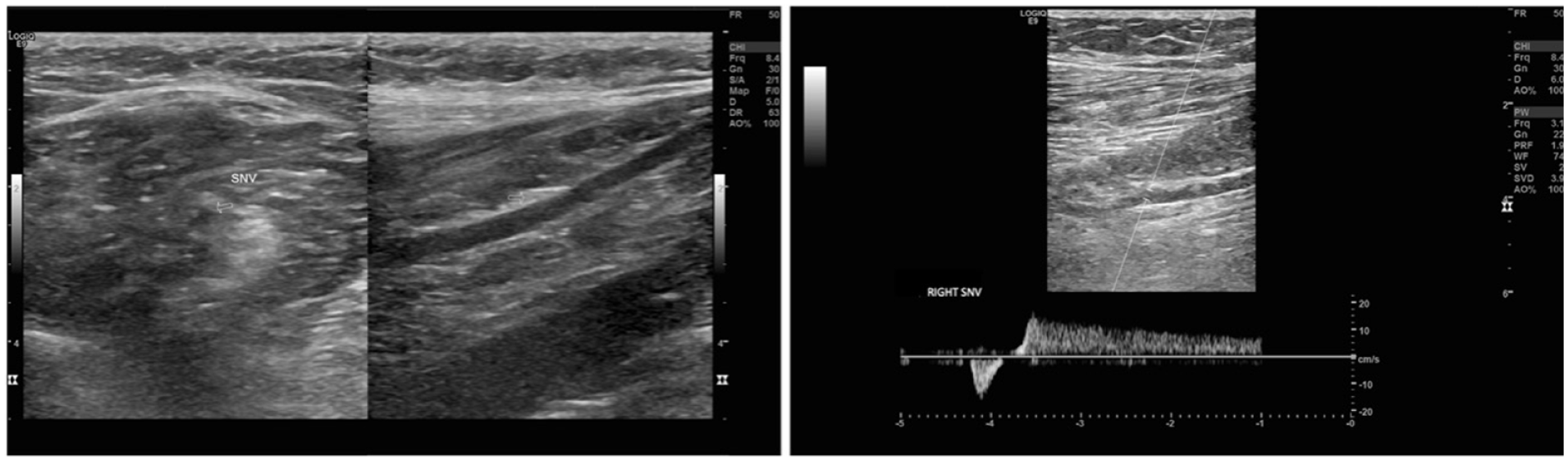
Transverse and longitudinal B-mode image of the vein of the sciatic nerve (left) with spectral Doppler analysis showing venous reflux with provocative maneuver (right).
Discussion
In the posterior calf, the SSV is recognized as an interfascial vein due to its unique anatomical characteristic as it is encapsulated within the saphenous envelope formed by the saphenous and muscular fascia. As a truncal vein, it arises from the lateral marginal vein (LMV) of the foot but can also originate from the lateral malleolar plexus or lateral perforators of the foot. 6 After passing behind the lateral malleolus, it travels upward along the posterior mid-line of the calf, connecting with the posterior or posterolateral surface of the popliteal vein in the popliteal fossa or continues up as the TE with its flow further drained via GSV, posterior thigh muscle veins, and the deep femoral vein (DFV). 6 The duplication of the SSV and the presence of a superficial accessory branch alongside the saphenous fascia that overlies the SSV have been observed.7,8 Nevertheless, it is important to clarify that the vein we have described in this case study should not be mistaken for the SSV or its superficial accessory. This is due to its distinct location in the lateral calf compartment, independent of the saphenous compartment despite the connections with ankle perforators and SSV at the lower calf.
The persistent LMV is an uncommon vein located in the lateral calf, often found in patients with Klippel-Trenaunay syndrome (KTS) or congenital lipomatous overgrowth, vascular malformations, epidermal nevi, and skeletal deformities (CLOVES) syndrome within the spectrum of phosphatidylinositol 4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA)-related overgrowth syndromes (PROS). 9 According to Fereydooni et al, this LMV is a vein that persists from embryonic development and does not fully regress at birth. It may originate near the lateral malleolus, traveling upward toward the thigh with diverse drainage patterns, including the popliteal vein, DFV, and even the GSV in cases of deep vein aplasia. The LMV, due to its valveless nature and association with venous malformation, can result in venous hypertension.9,10 The fact that the LMV lacks fascial encasement is a distinctive feature that we used to differentiate our interfascial vein from the LMV. In addition, since none of our patients exhibited clinical features of KTS, such as port-wine stains or limb hypertrophy, we suggest that the vein identified in our patient cohorts may not be the LMV under these circumstances.
In the ultrasound investigation to explore unusual causes of varicose veins in the lower limbs, Lemasle and Greiner (2019) identified that the superficial fibular (peroneal) nerve vein (SPNV) correlates with sciatic nerve varices (SNV). This tubular-shaped vein runs alongside the SSV within a compartment similar to that of the SSV, tracing the path of the superficial peroneal nerve (SPN). It was reported that the SPNV connects with the SSV in the lower third of the calf, feeding the varicosities in the lower half of the calf. 11 The presence of SPNV was also documented in a study of the SPN by Canella et al, 12 in which the authors discovered a small vein close to the SPN along its entire course. Based on the topographic anatomy, we believe that the interfascial vein we identified in our patients is likely to be a representation of SPNV, as illustrated in Figure 5. Nevertheless, the results of the study showed the interfascial vein located at an average distance of 36.33 mm lateral to the SSV and may travel spirally rather than in a straight course within its fascial compartment.
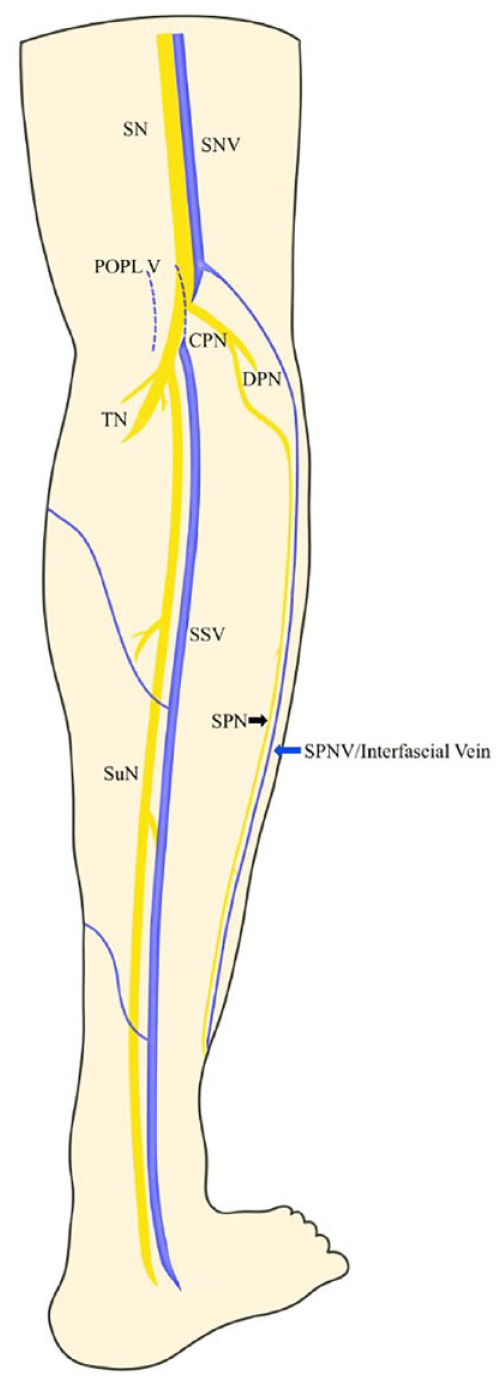
Anatomical diagram—posterolateral view of the calf.
The SPN is one of the terminal branches of the common peroneal nerve, a branch of the sciatic nerve, which controls the motion and sensation in the anterolateral aspect of the calf and the dorsum of the foot. This nerve courses above the upper fibula, deep to the peroneus longus (PL) muscle. It traverses through the peroneus muscle, positioning itself between the PL and peroneus brevis (PB) muscles. As it descends, it runs more superficially between the PB and extensor digitorum longus (EDL) muscles. The nerve becomes superficial by piercing the deep (crural) fascia in the lower one third of the calf and further bifurcating to medial and intermediate dorsal cutaneous nerves.13,14 Despite variations in the emergence of the SPN, the nerve can be easily identified by palpation and visualization due to its superficialization near the lateral malleolus. 15 Furthermore, the short-axis sonographic honeycomb appearance also aids the identification of the nerve, where the hyperechoic and hypoechoic structure correspond to the epineurium and fascicles, respectively. 16 In our experience, the interfascial vein we observed is mostly located adjacent to a small round-shaped honeycomb structure that is located within a compact fascial compartment as depicted in Figure 3. Moreover, the area surrounding the interfascial vein, enclosed by the fasciae, has less adipose tissue compared with the saphenous compartment of the SSV. It is also worthwhile mentioning that 2 of the 6 patients had venous reflux originating from the SNV. This observation provides additional support to the perspectives of Ricci and Labropoulos (2005), indicating that the SNV extends past the popliteal crease and reaches the lateral calf, influencing the superficial peripheral nerve system, referred to as sciatic-peroneal varices.17,18
Trauma or compression of the SPN may produce pain, numbness, tingling, and weakness in foot eversion or even lead to foot drop. Our investigation revealed that patients in group II reported pain and numbness in various locations, contrasting with asymptomatic individuals in group I, although no statistically significant difference was found. Concerning the saphenous veins, while endovenous ablation is now recommended for correcting saphenous reflux, the authors propose opting for sclerotherapy over ablation due to the proximity to the SPN, aiming to reduce the risk of iatrogenic nerve injury. 19
Limitations
There are several limitations inherent in our case series study. First, our sample size is small due to the low prevalence of the interfascial vein, reducing the statistical power for analyzing any causal relationship between the SPNV and other associated veins. In addition, there was a lack of alternative imaging modalities employed to confirm the presence of SPNV in the identified individuals. Finally, the authors cannot ascertain whether treating the incompetent SPNV would alleviate clinical symptoms, as none of the 6 patients had undergone venous treatment at the time of writing.
Conclusion
This study contributes to the expanding knowledge of NSR, particularly veins of the peripheral nerves in the lower limb, emphasizing the importance of a comprehensive ultrasound examination and understanding of anatomical variations. Further research with larger sample sizes and longitudinal follow-up may provide additional insights into the clinical implications and management of such interfascial veins in the lateral calf compartment.
Footnotes
Author Contributions
GL designed the present study, collected data, and wrote the manuscript. JC and IM supervised the entire project to ensure the accuracy and integrity of data. JC and GL collaborated on the manuscript revision, and all authors gave the final approval for the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study received ethical approval from the Human Research Ethics Committee (HREC) of the University of Sydney (UYSD) (Protocol No. 2022/667).
Guarantor
GL is the guarantor of this article.