
Abstract
Introduction:
The advent of Doppler ultrasound has revolutionized the diagnosis of even subclinical atherosclerosis of the neck vessels. The aim of this study was to evaluate the contribution of Doppler ultrasound of the supra-aortic trunks in the etiological evaluation of ischemic stroke.
Methods:
Our cross-sectional and analytical study with retrospective and prospective data collection more than 8 years from January 1, 2010, to December 31, 2017, involved patients aged at least 21 years who were hospitalized for ischemic stroke. Doppler ultrasound of the supra-aortic trunks allowed us to group carotid atherosclerotic plaques into 5 grades according to the Gray-Weal classification modified by Geroulakos. Similarly, we assessed the degree of carotid stenosis in these patients. Factors associated with atherosclerotic plaques and stenosis were determined using multivariate logistic regression. Associations with a P < 0.1 in univariate regression were included in the multivariate model. Differences were considered significant for P < .05.
Results:
We recruited 271 patients with a mean age of 60 ± 12 years. Hypertension, increased low-density lipoprotein, diabetes, smoking, and obesity were present in 76.8%, 74.7%, 36.5%, 9.6%, and 80.1%, respectively. Atherosclerotic carotid plaques were found in 76.0% of the patients. For the left carotid artery, Grade I, II, and III plaques were present in 32.4%, 30.5%, and 21.4% of these patients, respectively, and the results were similar in the right carotid artery. Age ≥60 years, female gender, and increased low-density lipoprotein were significantly associated with carotid atherosclerosis (odds ratio = 12.6, P = .003; odds ratio = 3.23, P = .001; and odds ratio = 4, P = .002, respectively). Carotid stenosis ≥50% was found in 5.9% of patients with plaque, and age >70 years was significantly associated with these stenoses (odds ratio = 4.74, P = .045).
Conclusion:
Our study showed a high prevalence of atherosclerotic carotid plaques (76.0%) and stenosis (5.9%) among patients with ischemic strokes who had Doppler ultrasound of the neck vessels. Age is a powerful risk factor associated with carotid atherosclerosis and stenosis. Female gender and dyslipidemia are also significantly associated with carotid atherosclerotic plaques.
Introduction
Stroke is the second leading cause of death and disability in the world with more than 13 million new cases each year. 1 Its prevalence varies from one country to another, and its morbidity and mortality are strongly impacted by the level of development of the country. In Cameroon, the overall mortality rate is approximately 26.8%, compared to 21% in Togo.2,3 Ischemic stroke represents 80% of strokes, and according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification, carotid atherosclerosis is one of the main causes.4,5 Thus, atherosclerosis of the carotid trunks is thought to be the cause of 15% to 20% of disability-adjusted life years (DALYs), depending on the study, and 10% to 15% of all strokes.6-8 Also, among the 30% of ischemic strokes classified as undetermined, low-grade carotid atherosclerotic plaques, which do not meet the etiological criteria for cerebral ischemia, are thought to be the cause in the majority of cases. 9
The incidence of ischemic stroke events would be related to the characteristics of the atherosclerotic plaques. Thus, patients with significant stenotic plaques would have a neurological event in 20.6% of cases within 3 years and ischemic stroke in 11% of cases within 2.7 years. 10 The advent of Doppler ultrasound has revolutionized the diagnosis of even subclinical atherosclerosis of neck vessels. 11 With a sensitivity of 86% and a specificity of 87%, supra-aortic Doppler ultrasound appears to be the gold standard of diagnosis in terms of cost, reproducibility, and safety for the patient.12,13 A meta-analysis published in 2005 found equivalence in the detection of carotid stenosis between supra-aortic Doppler ultrasound, magnetic resonance imaging, and angiography. 14 Thus, Doppler ultrasound of the supra-aortic trunks is a suitable tool for the early diagnosis of patients at risk for ischemic stroke in income-limited settings. In view of the increasing phenomenon of ischemic stroke and the urgency of a preventive approach, our study aims to evaluate the prevalence and factors associated with atherosclerosis and carotid stenosis in patients hospitalized for ischemic stroke at the Douala General Hospital (DGH).
Methods
We conducted a cross-sectional and analytical study with retrospective and prospective collection more than 8 years from January 1, 2010, to December 31, 2017. The study was conducted in the neurology and cardiology units of the internal medicine department of the DGH over a period of 6 months, from November 1, 2017, to May 30, 2018. The study population consisted of all records of patients aged at least 21 years who presented with a brain imaging confirmed ischemic stroke and in whom a supra-aortic Doppler ultrasound was performed and documented during our study period.
We initially obtained ethical clearance from the Ethics Committee of the University of Douala. Data were collected from the patient’s files and from the patient or a relative, as well as from the ultrasound scanners in the cardiovascular examination room. The supra-aortic Doppler ultrasound data were collected on the hard disk of the General Electric ultrasound machine (VIVID 3) with a Sony printer and 4 probes, including a 10-MHz linear probe used for vascular ultrasound. The supra-aortic trunk vessels included the common carotid artery (CCA) and its bifurcation, internal carotid artery (ICA), external carotid artery (ECA), and the V1 (origin) and V2 (intraforaminal) vertebral artery segments.
Definition of Variables
Carotid atherosclerotic plaque was defined as the presence of arterial wall thickening of greater than 50% of the wall immediately upstream or downstream or as a localized area with intima-media thickness >1.5 mm protruding into the arterial lumen. 15 The ultrasound classification of Gray-Weale modified by Geroulakos in 1993 has been used to classify the appearance of atherosclerotic plaques into 5 grades: Grade I (anechoic plaque with <15% intense echoes), Grade II (predominantly anechoic or hypoechoic plaque with 15% to 50% intense echoes), Grade III (predominantly isoechoic or hyperechoic plaque, heterogeneous with 50% to 85% echoes), Grade IV (isoechoic or hyperechoic plaque, uniformly, with >85% echoes), and Grade V (calcified plaque). 16 This allowed us to classify carotid arterial atherosclerosis into nonstenotic (no reduction in the arterial lumen, <125cm/s peak systolic velocity), stenotic (varying according to the degree of lumen occlusion: <50%, 50% to 69%, and ≥70%), subocclusion, and complete occlusion.
A DALY was defined by cerebral computed tomography evidence of ischemic lesions, which has a high sensitivity. 17 A participant was considered hypertensive if he or she had a history of hypertension or had blood pressures of ≥140 mmHg systolic and/or ≥90 mmHg diastolic. 18 Diabetes mellitus was defined by the presence of a history of diabetes mellitus or a fasting blood glucose level ≥1.26 g/L in the presence of diabetic symptoms or an instantaneous blood glucose level >2 g/L or glycosylated hemoglobin >6.5%. 19 Dyslipidemia was defined according to the National Cholesterol Education Program Adult Treatment Panel III criteria with adjustment for overall cardiovascular risk (total hypercholesterolemia ≥2 g/L, hypertriglyceridemia >1.5 g/L, increased low-density lipoprotein (LDL) ≥1.6 g/L but considered here as low as >1 g/L, and low high-density lipoprotein (HDL) <0.4 g/L in men and 0.5 g/L in women) and/or previous diagnosis of dyslipidemia. 19 Smoking was defined as current smoking or cessation of smoking for less than 3 years. 19 Overweight was defined by a body mass index (BMI) between 25 and 29.9 kg/m2 and obesity by a BMI ≥ 30 kg/m2. 20
Statistical Analysis
Data were treated and analyzed using SPSS 20 software. Quantitative data were presented as mean ± standard deviation, while qualitative data were presented as counts and frequencies. The frequency of atherosclerosis and stenosis was determined and associated with different characteristics of the study using chi-square test. Factors associated with atherosclerosis and stenosis were determined using multivariate logistic regression. Associations with a P < .1 in univariate regression were included in the multivariate model. Differences were considered significant for P < .05.
Results
The study was carried out on 271 participants with ischemic stroke aged 60 ± 12 years, and 48.3% were women. Demographic, clinical, and past history characteristics of the participants are presented in Table 1. Of the participants, 43.5% were employed, 36.5% were diabetic, and 76.5% had hypertension. The prevalence of overweight/obesity was 80.1%. Dyslipidemia was present in 88.4% of participants, while increased LDL cholesterol (≥1 g/L) was present in 74.7% of participants.
Characteristics of Participants.
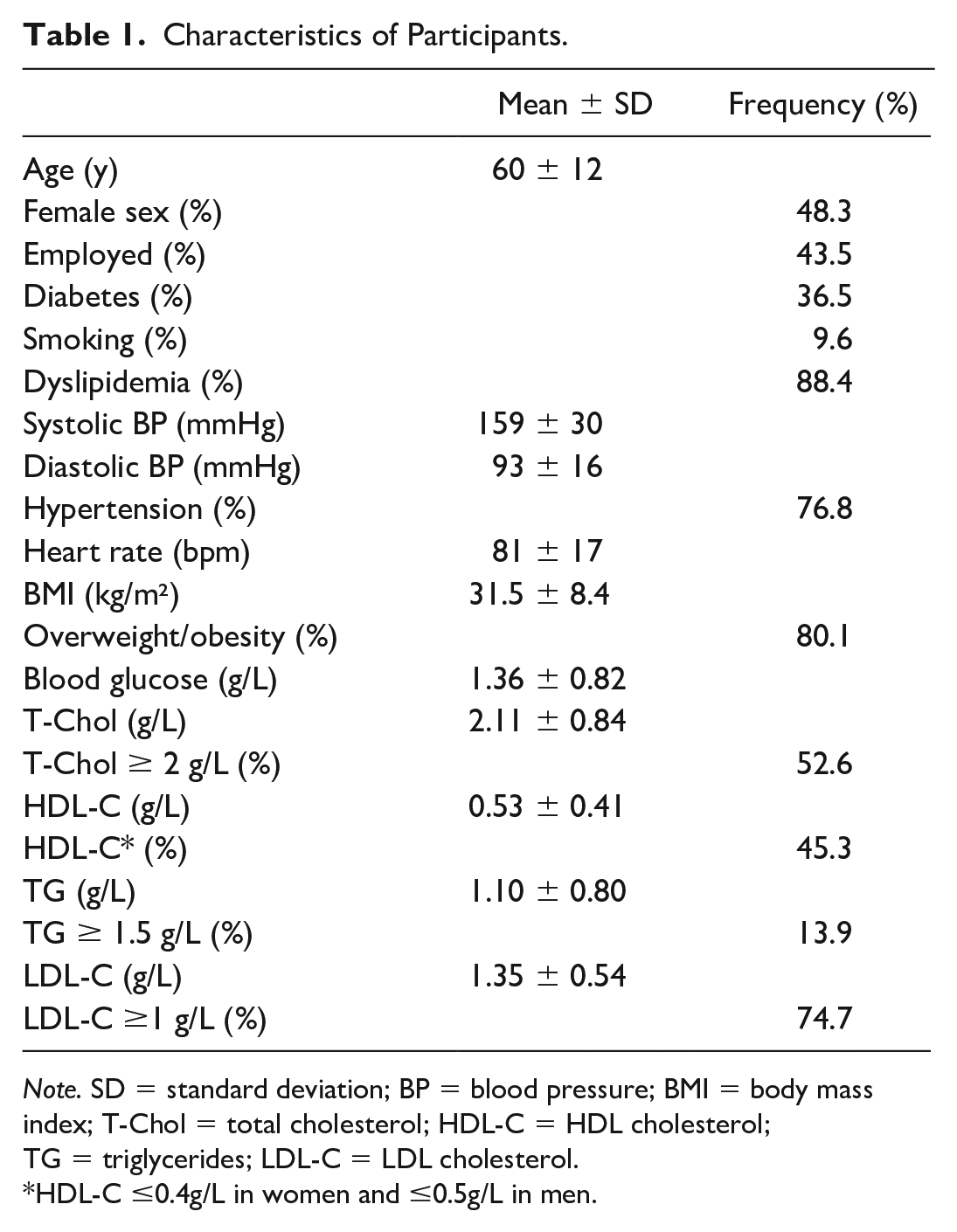
Note. SD = standard deviation; BP = blood pressure; BMI = body mass index; T-Chol = total cholesterol; HDL-C = HDL cholesterol; TG = triglycerides; LDL-C = LDL cholesterol.
HDL-C ≤0.4g/L in women and ≤0.5g/L in men.
Prevalence of Atherosclerosis and Stenosis
The frequency of participants with atherosclerosis involving the right or left carotid artery was 76.0% (206 participants). The frequencies of the different grades of atherosclerosis in the right and left carotid arteries are presented in Figure 1. In the left carotid artery, Grade I, II, III, and IV atherosclerotic plaques represented 32.4%, 30.5%, 21.4%, and 9.1% of participants, while Grade V represented 6.6%. The results were similar in the right carotid artery.
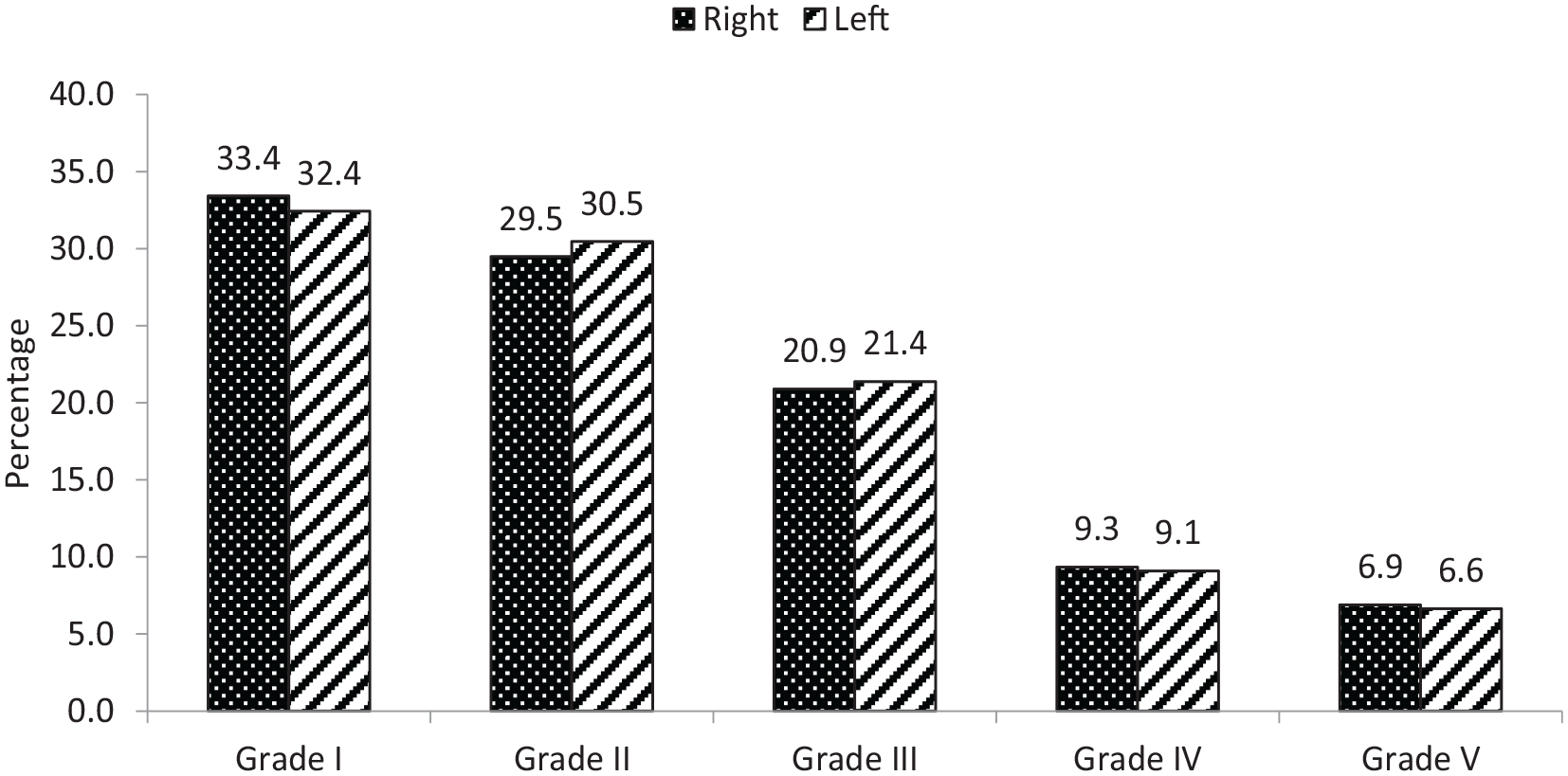
Frequency of different grades of atherosclerotic plaque in the right and left carotid arteries among the 271 participants.
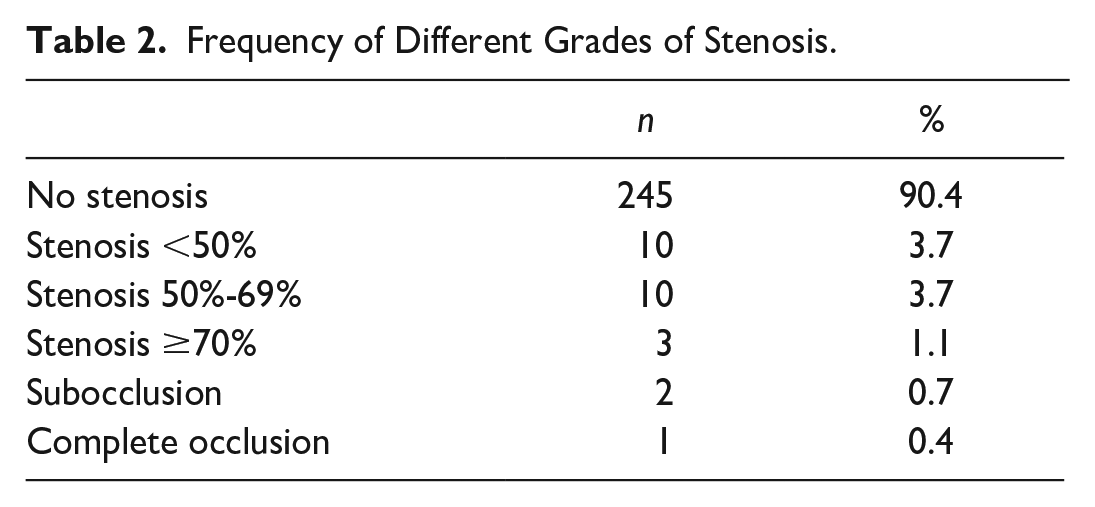
The prevalence of different grades of stenosis is presented in Table 2. Stenosis was present in 9.6% of participants (26 participants). Among those participants, 10 had a stenosis of 50% to 69%, 3 had stenosis ≥70%, 2 had subocclusion, and 1 had complete occlusion.
Frequency of Different Grades of Stenosis.
Factors Associated With Atherosclerosis and Stenosis
Tables 3 and 4 present the frequencies and determinants of carotid atherosclerosis and stenosis, respectively, according to the characteristics of the participants. The frequency of atherosclerosis increased significantly with age from 44.4% for those <40 years to 90.6% in participants aged 60 to 69 years, although we found a slight decrease in participants aged ≥70 years. Atherosclerosis was also significantly more common in women than men, in employed participants, and in those with LDL cholesterol ≥1 g/L. After multivariate analysis, age was an independent determinant of atherosclerosis, with risk increasing significantly after 60 years compared to <40 years. Female sex (odds ratio [OR] = 3.32, P = .001) and LDL cholesterol ≥1 g/L (OR = 4.00, P = .002) were also independent determinants of atherosclerosis. Table 4 shows that stenosis was also significantly associated with age, with a frequency significantly higher in participants aged ≥70 years compared with those aged 40 to 49 years, while no case of stenosis was found in participants aged <40 years. After multivariate analysis, age remains significantly associated with stenosis in participants aged ≥70 years compared with those aged 40 to 49 years (OR = 4.74, P = .045).
Determinants of Atherosclerosis in the Population.
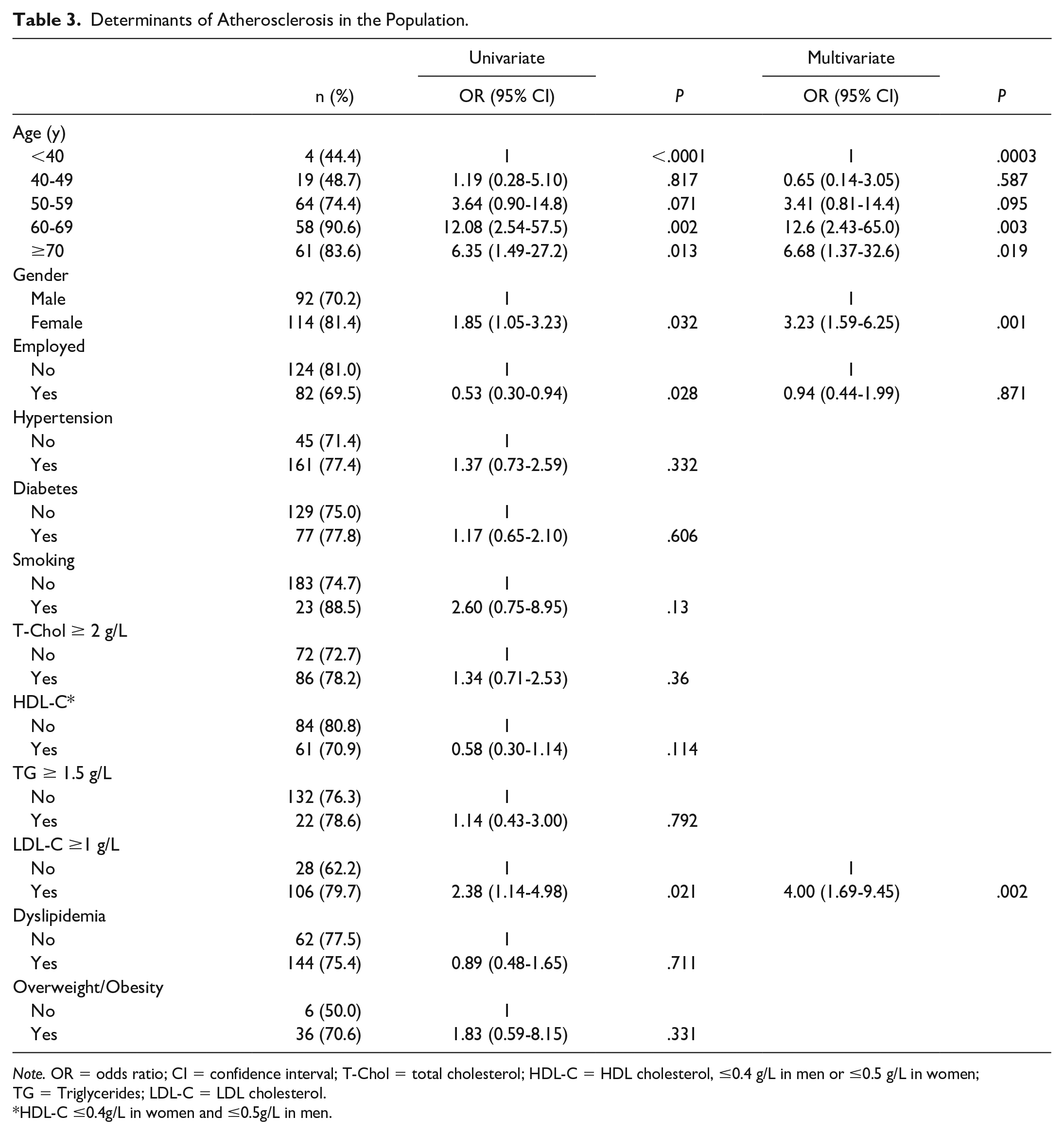
Note. OR = odds ratio; CI = confidence interval; T-Chol = total cholesterol; HDL-C = HDL cholesterol, ≤0.4 g/L in men or ≤0.5 g/L in women; TG = Triglycerides; LDL-C = LDL cholesterol.
HDL-C ≤0.4g/L in women and ≤0.5g/L in men.
Determinants of Stenosis in the Population.
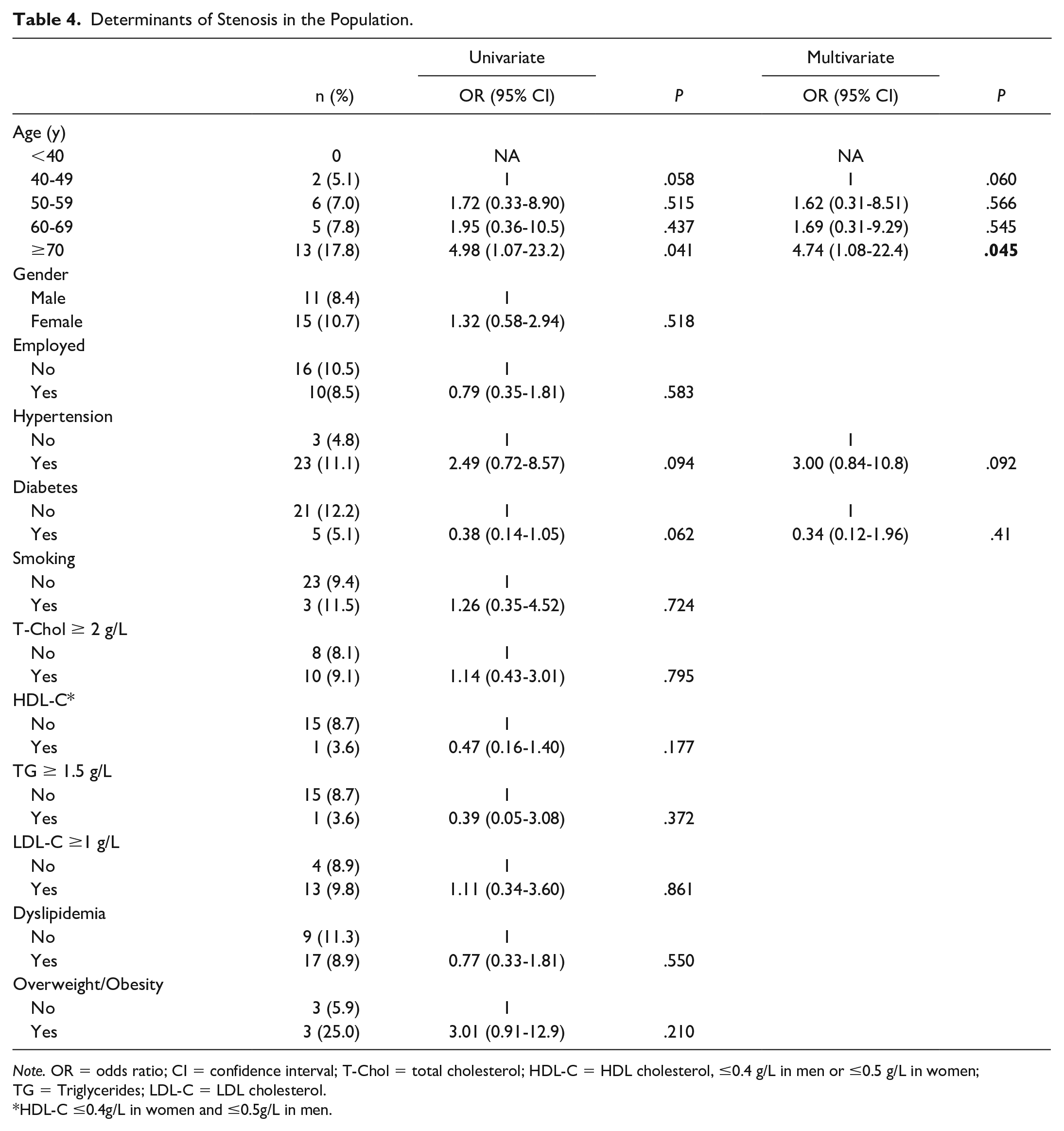
Note. OR = odds ratio; CI = confidence interval; T-Chol = total cholesterol; HDL-C = HDL cholesterol, ≤0.4 g/L in men or ≤0.5 g/L in women; TG = Triglycerides; LDL-C = LDL cholesterol.
HDL-C ≤0.4g/L in women and ≤0.5g/L in men.
Discussion
In our study, among the 271 patient records analyzed, 206 participants (76.0%) presented with atherosclerosis of the right or left carotid artery. Although ischemic stroke risk factors have been previously described in the African populations, 3 no study (to the best of our knowledge) has characterized atherosclerosis in Cameroonian stroke patients. Therefore, our study provides important data for public policies on stroke prevention and mortality. The prevalence of risk factors for atherosclerosis described in the literature and found in our population was as follows: dyslipidemia in 88.4%, increased LDL cholesterol in 74.7%, hypertension in 76.5%, diabetes in 36.5%, and smoking in 9.6%. Overweight/obesity, which is an indirect factor interacting with some of the other factors, was present in 80.1% of the participants. The high prevalence of risk factors found in our study is due to the selected population which consisted of mostly elderly patients with cardiovascular pathology, including ischemic stroke. In contrast, in the general population, the prevalence of atherosclerotic risk factors is much lower and varies with age. 11 The slight male predominance can be explained by the fact that between the ages of 45 to 85 years, stroke is more frequent in men than in women. 21
In our study population, the characteristics of atherosclerotic plaques were almost identical in the left and right carotid arteries. In the left carotid artery, 32.4% were Grade I, 30.5% Grade II, 21.4% Grade III, 9.1% Grade IV, and 6.6% Grade V. The Grade I to III atherosclerotic plaques, also characterized as young plaques, comprised the majority with decreasing frequency. This trend is similar to that of Geroulakos et al 16 in a study published in 1993 which showed that in patients with symptomatic atherosclerotic plaques, 90% were Grade I, 53% Grade II, and 34% Grade III.
Some authors found that the incidence of DALYs at 3.3 years in atherosclerotic plaque patients did not follow this trend, with 3.5% for Grade I, 1.95% for Grade II, 5.4% for Grade III, and 2.67% for Grade IV. 22 The high prevalence of atherosclerotic plaques in our study can be attributed to our study population, recognizing that carotid atherosclerosis is the main cause of DALYs between 45 and 70 years of age. 23 This, together with the fact that the most symptomatic plaques (Grades I and II) were in the majority in our study, is similar to the results found in the literature. 24 In our population, age ≥70 was significantly associated with carotid atherosclerosis (from 60 to 69 years with OR = 12.6; P = .003 in multivariate analysis and age ≥70 years with OR = 6.68, P = .019 in multivariate analysis). Increasing age is found consistently in reported studies and is considered to be the most powerful factor in the development of carotid atherosclerotic lesions.11,25,26 The only difference among the studies is the average age which varies from 50 to 70 years. 27 This can be explained by the fact that atherosclerosis is a slow process that starts in childhood and manifests itself in adulthood, accentuated by the presence of certain risk factors. 28
In our study, increased LDL cholesterol was significantly associated (OR = 4; P = .002 in multivariate analysis) with the presence of carotid atherosclerosis. Increased LDL cholesterol remains central to the process of initiation and growth of carotid atherosclerotic plaques through infiltration and accumulation in the vessel wall. 29 These results are similar to those found in the literature, both in patients with DALYs 27,30 and in the general population. 11 Also, female gender was significantly correlated with the presence of carotid atherosclerosis (OR = 1.85, P = .032 in univariate analysis and an OR = 3.23, P = .001 in multivariate analysis) in our study. These results are contrary to those of most studies that found male sex to be a factor associated with atherosclerosis.6,11,31 Our results can be explained by the fact that obesity and dyslipidemia are more frequent in adult women in Cameroon. 32 After further analysis, we found that female participants were less numerous in the younger age group (40-49 years) and more numerous in older age groups (60-69 and ≥70 years) compared with males. This can mostly explain the significant association of gender with atherosclerosis, since age is the leading factor influencing the atherosclerotic process. 25 These findings also confirm the higher risk of cardiovascular disease complications in postmenopausal women compared with men. 21
Hypertension, diabetes, and smoking were not significantly associated with carotid atherosclerosis (OR = 1.37, P = .332; OR = 1.17, P = .606; and OR = 2.6, P = .13, successively). These results are contrary to those found by Gnonlonfoun et al 30 in Bénin in 2016, Ikama et al 27 in Congo in 2012 in patients with DALY, and Babaka et al 11 in Senegal in 2016 in the general population of a semi-urban setting. Thus, the lack of significant association in our study may be due to the fact that hypertension, diabetes, and smoking were confounding factors. This is because they are identified in the literature as risk factors for atherosclerosis, 6 but also as independent risk factors for DALY.33,34
In our study, 9.6% of the participants had carotid stenosis, of which 3.7% had stenosis <50%, 3.7% had stenosis between 50 and 60%, 1.1% had stenosis ≥70%, 0.7% had subocclusion, and 0.4% had complete occlusion. Despite the high prevalence of atherosclerotic carotid plaque in our study, only 5.9% had a stenosis ≥50%. In a meta-analysis published in 2015 by Gupta et al, 35 the risk of ischemic stroke was increased 2.6-fold in individuals with 50% to 99% carotid stenosis. This discrepancy between the presence of atherosclerotic plaques and carotid stenosis in our study can be explained by the fact that it is the appearance of the plaques that is mainly responsible for the occurrence of DALYs. 10 In our study, only age ≥70 years was significantly associated with carotid stenosis (OR = 4.74, P = .045 in multivariate analysis). In the majority of studies, in addition to age, hypertension and smoking were associated with carotid stenosis.6,36 Age remains a strong risk factor for carotid stenosis in almost all studies, explained by the mechanism of age-related arterial stiffness.6,37 Although the mechanisms of action of hypertension and smoking in the development of carotid stenosis are known, 6 these factors were not found in our study. This result may be explained by the fact that hypertension and smoking are also independent risk factors for ischemic stroke,33,34 thus acting as confounders, as our population consisted of patients with ischemic stroke.
Conclusion
Doppler ultrasound of the supra-aortic trunks is of great importance in the diagnosis and care of patients with ischemic stroke. In our study, it showed a very high prevalence of atherosclerotic carotid plaques (76.0%) and carotid stenosis (5.9%) among patients hospitalized for ischemic stroke. Age, dyslipidemia, and female gender are risk factors for the occurrence of carotid atherosclerotic plaques which may progress to stenosis, with age ≥70 years being the main factor.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.