
Abstract
Polymerization contraction stress of dental composites is often associated with marginal and interfacial failures of bonded restorations. The magnitude of stress depends on composite composition (filler content and matrix composition) and its ability to flow before gelation, which is related to the cavity configuration and curing characteristics of the composite. This article reviews variations among studies regarding contraction-stress-testing methods and contraction stress values of current composites, and discusses the validity of contraction stress studies in relation to results from microleakage tests. The effects of lower curing rates and alternative curing routines on contraction stress values are also discussed, as well as the use of low-elastic-modulus liners. Moreover, studies with experimental dimethacrylate-based composites and recent developments in low-shrinkage monomers are described.
Introduction
Dimethacrylate-based composites have been used in dentistry for over 30 years. Developments in filler technology and initiation systems have considerably improved composite physical properties and expanded their clinical applications. Notwithstanding, since early composites, the volumetric shrinkage resulting from conversion of dimethacrylate monomers into long, cross-linked polymeric chains has been identified as a critical limitation that needed to be addressed (Bowen, 1963). Bonding of composite to cavity walls seemed to be a reasonable solution for the problem. This quest prompted prolific research activity on the subject of dental adhesives and dentin permeability, that brought remarkable advances such as wet bonding and self-etching primers. Unfortunately, in spite of the significant increase in bond strength values reported over the years, the occurrence of microleakage and gap formation, mostly at the dentin/composite interface, did not seem to decrease at a similar rate (Hilton, 2002; Irie et al., 2002). Concurrently, research on polymerization kinetics and polymerization contraction stress began to intensify, producing enhanced knowledge of factors influencing the magnitude of forces developed at bonded interfaces.
Dental composite polymerization shrinkage ranges between 2 and 6% by volume (Labella et al., 1999). Besides volume reduction, chain growth and cross-linking also result in increased elastic modulus (Braem et al., 1987; Dauvillier et al., 2000). During polymerization, there is a stage in monomer conversion, referred to as the ‘gel point’, at which an insoluble network is formed within the resin phase. At this point, the elastic modulus of the composite has increased substantially, and the composite’s elastic limit has reached a level that does not allow enough plastic deformation (or flow) to compensate for the reduction in volume. Beyond this stage, additional contraction may generate significant stress within the composite. If composite is bonded to cavity walls, shrinkage forces will develop, resulting in stresses on the bond between composite and tooth structure. These forces are not uniformly distributed along the cavity walls (Kinomoto and Torii, 1998). The bond strength between tooth and composite also varies along the bonded surface (Shono et al., 1999). Therefore, in areas where the shrinkage forces are higher than the composite-to-dental-substrate bond, a gap will develop, increasing the chance for post-operative sensitivity and recurrent caries (Brännström, 1984; Eick and Welch, 1986). A recent study demonstrated that the percentage of dentinal gaps in a composite restoration placed in vivo may vary between 14% and 54% of the total interface, depending on the materials and techniques used (Hannig and Friedrichs, 2000). Other consequences of contraction stress are the development of enamel cracks (Jorgensen et al., 1975; Kanca and Suh, 1999) and cuspal movement (Sheth et al., 1988; Sulliman et al., 1993; Alomari et al., 2001).
The phenomenon of force development in contracting materials was first described in the dental literature by Bowen (1967). In that study, the author discussed the influence of setting material confinement as the main factor associated with contraction stress. But it was not until studies by Davidson and de Gee (1984) and Feilzer et al. (1987) that the subject of polymerization contraction stress began to be studied in depth. It is well-established that the magnitude of contraction stress development depends on factors related to the geometry of the cavity preparation (or the testing specimen), as well as on the compositional and curing characteristics of the composite.
The most frequent method of measuring contraction stress is the tensilometer (Bowen, 1967). In this test, contraction stress values vary according to the ratio of the bonded to the free surface area of the composite. This ratio has been called the configuration factor, or C-factor (Feilzer et al., 1987). It has been hypothesized that a large unbonded area would facilitate composite plastic deformation during polymerization before the gel point is reached, thus reducing the final stress values (Feilzer et al., 1990). This concept of the effect of configuration factor on contraction stress has been validated, to a certain extent, by microtensile bond strength studies reporting that values to deep dentin were lower when specimens were obtained from restored cavities, compared with specimens obtained from flat dental substrates (Yoshikawa et al., 1999; Nikaido et al., 2002). It was hypothesized that lower bond strengths were caused by a higher incidence of gaps at the dentin-resin interface due to higher contraction stresses (Yoshikawa et al., 1999). The volume of shrinking composite also influences stress values (Miguel and de la Macorra, 2001). This finding supports those of a previous study that showed that the incidence of marginal gaps in composite restorations was related to the volume of composite and to the bonded cavity wall area (Hansen and Asmussen, 1985).
Contraction stress is also determined by characteristics of the composite. Filler content and resin matrix composition dictate the amount of volumetric shrinkage and elastic modulus values of the material (Labella et al., 1999). Polymerization activation mode and types and concentrations of initiators regulate degree of conversion and reaction kinetics (Venhoven et al., 1996). The higher the degree of conversion, the higher the final shrinkage and elastic modulus of the composite, both of which contribute to producing higher stresses (Braga and Ferracane, 2002). Similarly, faster polymerization rates imply that the polymerizing matrix moves more quickly through the critical conversion for gelation, rapidly producing stiffness in the composite and simultaneously reducing its flow capacity (Feilzer et al., 1993). Since the gel point refers to a particular degree of conversion, it itself should not be affected by alterations in reaction kinetics. However, a faster reaction rate would be associated with a more rapid growth of modulus both before and after the gel point, and this necessarily will result in more rapid development of stress compared with a slower curing scheme.
Based on the knowledge accumulated over the years, different approaches have been proposed to reduce the magnitude and the effects of contraction stress in dental composites. These methods include incremental placement technique (Lutz et al., 1986), development of light units with gradually increasing irradiance or pulsed emission (Kanca and Suh, 1999), and the use of low-modulus intermediate layers (Unterbrink and Liebenberg, 1999). Also, modifications of the current Bis-GMA resin-based composites have been proposed as a means to reduce stress without compromising composite mechanical properties (Condon and Ferracane, 1998, 2002).
The purpose of this article is to discuss, based on the scientific evidence, the variety of available alternatives to reduce polymerization contraction stress and improve interfacial integrity of direct and indirect bonded restorations.
Contraction Stress Measurements
Polymerization contraction stress has been evaluated by many different methods. Stress distribution in simulated cavities has been estimated by finite element analysis (Versluis and Tantbirojn, 1999; Ausiello et al., 2002) and photoelastic analysis (Kinomoto and Torii, 1998; Kinomoto et al., 1999). Direct measurements of stress (or strain) are usually accomplished with the use of strain gauges (Sakaguchi and Ferracane, 1998) or a tensilometer (Bowen, 1967; Feilzer et al., 1987; Condon and Ferracane, 1998). In the typical test set-up with a tensilometer (Fig. 1), the composite is placed between two opposing mounting rods (made of metal or glass), one of which is attached to a load cell and the other to a movable cross-head on the testing machine. A feedback system, composed of an extensometer attached to the rods, is used to maintain a constant distance between the rods and to simulate a situation of confinement for the shrinking composite. In this set-up, the value recorded represents the force necessary to counteract axial composite shrinkage and maintain rod distance at its initial value. One calculates the nominal stress by dividing the measured force by the cross-sectional area of the mounting rod.
As in any mechanical test, there is some controversy about a few aspects of the tensilometer method. The main point of dispute seems to be the compliance of the testing system. During the test, some of the contraction force is dissipated through deformation of the components of the testing system (e.g., load cell, mounting rods, adhesive layer). However, when a feedback system is used, compliance is reduced to a near-zero condition, since virtually all deformation occurring outside of the extensometer limits is not taken into account. Some authors believe that this rigid situation overestimates stress values, since tooth compliance would prevent development of such high stresses (Miguel and de la Macorra, 2001; Watts et al., 2003). When a feedback system is not included in the testing apparatus, shrinking composite is free to pull the rods together, and the value registered is the result of the contraction force exerted by the material. In this case, the values registered are usually lower than those found when a feedback system is used (Hegdahl and Gjerdet, 1977; Bouschlicher et al., 1997; Chen et al., 2001; Miguel and de la Macorra, 2001). Depending on the rigidity of the test set-up, the relationship between stress and the ratio of bonded-to-unbonded surfaces of the composite specimen (C-factor) varies. In near-zero compliance set-ups, this relationship is direct (Feilzer et al., 1987; Choi et al., 2000a). An inverse relationship has been observed when non-rigid set-ups were used (Bouschlicher et al., 1997; Watts et al., 2003).
Another important aspect of contraction stress tests is that only the forces developing uniaxially are registered. Due to specimen geometry and boundary restraints, the distribution of forces in the specimen is rather complex. A finite element study (Laughlin et al., 2002) verified that forces developed during composite contraction generate a triaxial stress state, due to the high aspect ratio of specimen diameter to height. Therefore, contraction values registered by means of the tensilometer represent only a fraction of the forces exerted on the system by the shrinking material. The composite sample thickness also affects stress distribution. Some investigators (Feilzer et al., 1989) have suggested that, in thin composite films, the contraction vector is strongly influenced by the boundary restraints. In fact, the above-mentioned study (Laughlin et al., 2002) verified that the end restraints affect the entire volume of the shrinking composite. Apparently, this effect is accentuated in thin layers, contributing to an inverse relationship between film thickness and contraction stress (Alster et al., 1997a,b).
A few studies have tried to correlate the results from contraction stress tests with those from microleakage tests. The thickness of unfilled resin used to bond composite to glass in the tensilometer was shown to be inversely related to the contraction stress, and also caused a reduction in microleakage of class V cavities restored in one single increment (Choi et al., 2000a). Comparison between results of contraction stress tests and microleakage in class I porcelain inlays having all enamel margins showed that resin cements present higher contraction stress values and higher microleakage scores when tested in dual-cure mode compared with self-cure mode (Braga et al., 2002a). However, in the same study, scanning electronic microscopy analysis was unable to detect differences in terms of percentage of interfacial gaps. A direct relationship was also verified between contraction stress and microleakage in class V cavities for three commercial restorative composites (Ferracane and Mitchem, 2003). It should be kept in mind that the values obtained from contraction stress tests represent the average of a heterogeneous stress distribution, while marginal gap formation is the result of a localized bond failure. Moreover, the analysis of sectioned specimens is very limiting, and may not be representative of the whole specimen. Therefore, the fact that some correlation between contraction stress and microleakage could be observed is a very positive indicator of the validity of the stress test method.
Polymerization Contraction Stress of Current Composites
Studies evaluating the contraction stress of current commercial composites are summarized in the Table. Similar to other mechanical tests, the absolute values of the results from different contraction stress studies are hardly comparable. Testing system compliance, composite sample dimensions, force monitoring period, and direction of photo-activation may all vary.
Nevertheless, with respect to the compositional characteristics of composites, it has been observed that microfill composites tend to develop lower contraction stress than hybrids (Bouschlicher et al., 1997; Condon and Ferracane, 2000; Lim et al., 2002; Braga et al., 2003). Microfilled composites present lower elastic modulus than, but volumetric shrinkage similar to, that of hybrids, despite the lower filler content of the former (Labella et al., 1999). This apparent contradiction is explained by the presence of pre-polymerized filler particles in most of the microfilled composites, which serves to reduce the amount of resin matrix available to shrink. As a result, the contraction stress for microfills is generally smaller than that of more densely filled composites.
The contraction stress of packable composites has been evaluated (Chen et al., 2001). All five packable materials tested presented significantly higher stresses than the non-packable control. Since the control material had a filler level similar to that of the packable composites tested, the authors suggested that, rather than being correlated to the overall filler content, stress was related to the presence of large filler particles in the packable composites. It was supposed that these large fillers contributed to an increase in elastic modulus compared with that of the control, resulting in higher contraction stress. It should be noted, however, that other studies have shown similar elastic modulus and volumetric shrinkage for packable and non-packable composites (Choi et al., 2000b), which emphasizes the importance of control choice in such comparative studies.
Flowable composites present stress values similar to those of more densely filled materials (Braga et al., 2003). Their low filler content causes them to develop high volumetric shrinkage, approaching 6% in some products (Bayne et al., 1998; Labella et al., 1999). This finding, in spite of the low elastic modulus, seems to be the main cause for their high contraction stresses. Clinically, this result means that the risks of interfacial debonding for flowable and non-flowable composites due to shrinkage stress are similar. Nevertheless, the low elastic modulus of flowable composites may be advantageous for maintaining the interfacial integrity of the restoration in the face of different sources of stress (Kemp-Scholte and Davidson, 1990b).
The contraction stresses of three dual-cure resin cements were evaluated in both dual-cure and self-cure modes (Braga et al., 2002a). For all cements, the contraction stress in dual-cure mode (4.5–6.4 MPa) was higher than that in self-cure mode (3.4–4.0 MPa). The reduced stress in self-cure mode may have been the result of two concurrent factors. First, it is likely that there was a delay in stress build-up within the cements in self-cure mode due to a slower setting rate and a resultant extended flow and pre-gel shrinkage stage. Second, a lower degree of conversion of the cements in the absence of photo-activation (Braga et al., 2002b) should result in a reduction in both the volumetric shrinkage and the elastic modulus of the material.
Influence of Photo-activation Methods on Contraction Stress
As mentioned previously, contraction stress magnitude is highly dependent on the composite’s viscous component. Stress reduction by viscous flow may occur in two ways. First, the unbonded composite allows the material to deform when shrinking (external flow). Second, the longer it takes for the composite to develop a high elastic modulus, the more time is available for polymeric chains to deform and slip into new positions to adjust to the shrinkage (internal flow), reducing or delaying contraction stress build-up. In other words, if a higher proportion of the total volumetric contraction takes place while the composite remains in a non-rigid state, a smaller fraction of the shrinkage will effectively be responsible for stress development (Watts and Al Hindi, 1999).
To some extent, it is clinically possible to reduce composite curing rate by lowering the light intensity used for photo-activation. Conversion rate is proportional to the square root of the power density (PD = mW/cm2) (Bouschlicher and Rueggeberg, 2000). Alternative curing routines using stepped, pulsed, or ramped energy delivery have been developed with the intent of improving restoration interfacial integrity by reducing composite curing rate, therefore increasing its flow capacity (Uno and Asmussen, 1991; Christensen et al., 1999; Kanca and Suh, 1999; Hofmann et al., 2002). However, to be effective, these new ‘soft start’ curing methods should be able to reduce contraction stress and improve marginal integrity significantly, without compromising the degree of conversion or composite mechanical properties.
Studies evaluating alternative curing routines with respect to contraction stress development are few. One light unit that provided a logarithmic energy increase (Trilight, 3M ESPE, St. Paul, MN, USA) was found to originate lower contraction forces (approximately 33%), lower curing rate (approximately 20%), and similar degree of conversion compared with continuous-light activation (Bouschlicher and Rueggeberg, 2000). In the same study, use of a stepped curing mode (Highlight, 3M ESPE) did not significantly reduce contraction force. A two-step curing technique allowed for stress reduction between 19% and 30% for three different composites when compared with a continuous-light exposure using equivalent energy density, without compromising the degree of conversion (Lim et al., 2002). According to the authors, when a two-step curing routine is adopted, three aspects should be observed: the initial light intensity, the exposure duration of the initial low-intensity irradiation, and the time interval between the two irradiations.
Marginal integrity studies with ‘soft start’ polymerization show contradictory results. While some studies showed improved marginal integrity with non-continuous curing methods (Mehl et al., 1997; Luo et al., 2002), others did not find significant differences between those and conventional (continuous) curing (Friedl et al., 2000; Sahafi et al., 2001). One aspect that remains unclear is the effect of non-continuous irradiation on polymer structure. It has been hypothesized that low curing rates may result in longer polymeric chains and less cross-linking, thereby affecting the mechanical properties of the polymer (Asmussen and Peutzfeldt, 2001). However, others have characterized the structure and properties of cross-linked dimethacrylate polymers cured at low and high conversion rates, and found no significant difference in properties or overall conversion rates (Lovell et al., 2001).
Besides the curing rate, another aspect related to photo-activation that affects contraction stress is the total energy delivered to the composite (ED = PD x time = mW x s/cm2 = mJ/cm2). Use of high energy density to cure composite has been associated with superior mechanical properties and degree of conversion (Rueggeberg et al., 1994). The relationship between energy density and degree of conversion, however, is not linear (Sakaguchi and Berge, 1998). In other words, there is a limit where higher energy levels do not correspond to significant increases in degree of conversion or mechanical properties (Suh, 1999). Unfortunately, the relationship between energy density and post-gel shrinkage strain was found to be linear (Sakaguchi and Berge, 1998; Silikas et al., 2000). Therefore, high energy densities translate into higher stress levels, but do not necessarily result in high degrees of conversion or superior mechanical properties.
The relationship between degree of conversion (DC) and contraction stress seems to be more complex. Apparently, there is a threshold in the DC above which non-significant increases correspond to significantly higher stress levels (Braga and Ferracane, 2002). Clinically, it is almost impossible to determine which energy level would provide the best relationship among degree of conversion, mechanical properties, and contraction stress. Still, it is important to keep in mind that over-exposing the composite to photo-activation might increase the risk of marginal and interfacial debonding, as well as a heat build-up within the tooth.
The Use of Low-elastic-modulus Liners as Stress-absorbing Layers
The magnitude of stress developed at the restoration interface is related to the compliance of the surrounding structures. If the substrate to which the shrinking composite is bonded can yield to contraction forces, the developed stress is lower (Alster et al., 1997b). The application of a low-elastic-modulus material to the cavity walls represents a way to increase the compliance of the prepared cavity artificially. Besides the elastic modulus of the liner, the thickness of the applied layer may also influence stress relief. The thicker the layer, the better are the chances of significant stress relief (Unterbrink and Liebenberg, 1999). Finite element analysis studies support this idea (Rees et al., 1999; Ausiello et al., 2002).
Use of a 150-μm layer of unfilled resin under a bulk-cured layer of a high-modulus composite was shown to improve marginal sealing of class V restorations significantly and reduce stress values significantly (Kemp-Scholte and Davidson, 1990a). More recently, it was verified that application of unfilled resin layers, in the range of 100 to 200 μm, reduced contraction stress between 13 and 24%, and significantly reduced microleakage in class V cavities (Choi et al., 2000a). However, as noted by the authors, the clinical use of unfilled resin in thick layers is problematic. First, the material is radiolucent, interfering in radiographic diagnosis, and, second, the material’s fluidity would make application somewhat difficult in some areas of the cavity.
Use of low-viscosity (‘flowable’) composites as stress-absorbing-layer materials has been advocated by many authors (Behle, 1997; Unterbrink and Liebenberg, 1999; Jackson and Morgan, 2000). In general, flowable composites have lower elastic moduli than more densely filled materials (Labella et al., 1999; Price et al., 2000; Sabbagh et al., 2002). However, the results of microleakage studies conducted in vitro are contradictory. While some authors reported lower microleakage with the use of a pre-polymerized layer of flowable composite (Jain and Belcher, 2000; Peutzfeldt and Asmussen, 2002; Yazici et al., 2003), others were unable to detect any improvement in marginal integrity (Leevailoj et al., 2001; Wibowo and Stockton, 2001). Besides differences in layer thickness among studies, a possible explanation for this inconsistency is the broad range of elastic moduli of flowable composites. One study (Labella et al., 1999) reported values between 6.5 and 12.5 GPa for 12 different flowable composites. For comparison purposes, in the same study, the elastic modulus of an unfilled Bis-GMA resin was 4.6 GPa. Another study (Sabbagh et al., 2002) reported values ranging between 1.4 and 4.4 GPa for five low-viscosity materials.
A previous study (Braga et al., 2003) verified the influence of the elastic modulus of a pre-cured composite layer on the contraction stress developed by a subsequent layer of densely filled composite. Four flowable composites were evaluated, with elastic moduli ranging between 4.1 and 8.2 GPa. An unfilled resin (elastic modulus: 2.1 GPa) was also included in the study. In spite of the high thickness of the pre-cured layer used in the study (1.4 mm), a large and significant stress relief (approximately 41%) was observed only with the unfilled resin as the pre-cured material when compared with the value obtained with a pre-cured layer built with a densely filled composite (elastic modulus: 12.3 GPa). Only one of the flowable composites allowed for a potentially significant stress relief (approximately 19%).
Strategies for Stress Reduction in Experimental Bis-GMA-based Composites
Modifications of composite composition have been proposed for the reduction of contraction stress development. The general idea is to increase the opportunity for stress relief by flow, since the monomers present are the same found in the currently commercial composites and, therefore, the same levels of volumetric shrinkage are expected.
The use of non-bonded nanofillers (40-nm colloidal silica) was tested as an alternative to provide internal sites for stress relief without compromising composite mechanical properties (Condon and Ferracane, 1998). In the experimental nanofilled composite, close to 50% reduction in stress was observed when non-functional silane-treated particles were added, compared with the control material that contained particles with a functional (methacrylate) silane. The experimental hybrid composite produced 31% less stress when non-silanated nanofill particles were added. Though it was not directly observed, the proposed mechanism of stress relief was that non-bonded nanofillers allowed the resin matrix to flow around them and react without constraint, similar to the mechanism proposed for the stress reduction in unfilled resins with admixed porosity (Alster et al., 1992). No reductions in flexural modulus, degree of conversion, or fracture toughness were observed in these experimental materials (Hilton et al., 1997). A recent study (Condon and Ferracane, 2002) further investigated the effect of non-bonded nanofiller and verified that the optimal non-bonded nanofiller content was independent of the presence of filler particles of different sizes.
The effect of increased inhibitor concentrations (BHT, butylated hydroxytoluene) on contraction stress, degree of conversion, and volumetric shrinkage has also been evaluated (Braga and Ferracane, 2002). A significant stress reduction (approximately 39%) was observed when BHT concentration was increased from 0.05% (by weight) to 1.0%. The inhibitor molecules react with the free radicals generated by photo-activation, and polymerization proceeds at a reduced rate until inhibitor is completely consumed. This reduction effectively extends the pre-gel phase. Intermediate inhibitor concentrations caused significant reductions in curing rate, but not in contraction stress, suggesting that the reaction speed must be reduced below a certain threshold if contraction stress is to be significantly reduced. Degree of conversion and volumetric shrinkage were not significantly affected. However, further studies are necessary to verify whether composites with high inhibitor concentrations have adequate mechanical properties.
The addition of high-density polyethylene spheres (HDPE) to hybrid and nanofilled experimental composites has also been shown as a stress relief mechanism (Ferracane et al., 2003). In both cases, the addition of 20 wt% of HDPE spheres led to significant stress reduction compared with the respective control groups (between 26% and 29%). In the hybrid composite, polyethylene spheres replaced filler, and stress reduction seemed to be related to a reduction in elastic modulus. In the nanofilled composite, spheres were added to the control material without altering the resin-to-filler ratio. In that case, stress reduction was associated with a reduction in volumetric shrinkage. However, a general trend for lower mechanical properties with increased HDPE levels was observed, most noticeably with the hybrid materials.
Recent Developments in Low-shrinkage Monomers
Several approaches have been pursued in the past to reduce polymerization shrinkage in dental resins. Expanding monomers based on spiroorthocarbonates (SOC) were first attempted for dental composites, but the materials were not successfully commercialized (Thompson et al., 1979). The addition of SOCs to dimethacrylate resins cured by free radical polymerization (Stansbury, 1992) and to epoxy resins cured by cationic polymerization (Byerley et al., 1992; Eick et al., 1993) has been attempted within the past 10 years. Though studies showed lower shrinkage and subsequently lower shrinkage stress with the epoxy-based systems, it is likely that the reductions are related to lower overall monomer conversion in these systems (Chappelow et al., 1997). The ‘radical ring opening’ approach, using unsaturated spiroorthocarbonates or vinylcyclopropanes (VCP), has also been pursued to reduce composite shrinkage (Miyazaki et al., 1997; Moszner et al., 1997). Though no commercial product has been realized from these approaches to date, work is continuing.
Cycloaliphatic epoxy resins (also called oxiranes), formulated with polyols, such as polytetrahydrofuran, have been investigated and proposed as photocurable, cationic polymerized resins for dental composites with nearly one-half of the polymerization shrinkage of Bis-GMA-based resins (Tilbrook, 2000). These resins also have the advantage of no air-inhibited layer and high strength, but relatively high water sorption. Similar alternatives to dimethacrylates for dental composite matrices were recently discussed by Guggenberger and Weinmann (2000), who described a family of molecules called siloranes, the name being derived from the combination of siloxanes and oxiranes (epoxies). These molecules polymerize by cationic photoinitiation and produce dental composites with comparable properties and slightly reduced shrinkage compared with Bis-GMA-based materials. We have evaluated some of the properties of silorane- and oxirane-based composites and have verified that they do, in fact, have lower volumetric shrinkage and lower contraction stress than commercial Bis-GMA-based composites when tested after 60 minutes and 10 minutes, respectively (Fig. 2). Since cationic polymerizations typically continue for extended periods of time, there is a possibility that ultimate stress levels may be higher than those shown here. It should also be noted that the extent of the reaction was not measured for the composites shown in the Fig., and this would obviously affect the final stress values as well.
An esterified multi-methacrylate oligomer of poly(isopropylidenediphenol) (BPA) mixed with TEGDMA produced resins with a 10–15% reduction in polymerization shrinkage compared with Bis-GMA-based resins (Culbertson et al., 1997b,c). However, these new resins did not cure as well as the Bis-GMA-based materials, and again, this factor is the likely reason for their lower contraction. The contraction stress of these materials has not been tested, but due to their greater rigidity than Bis-GMA, it is doubtful that they would have lower shrinkage stress.
Interesting bismethacrylates with lower shrinkage than Bis-GMA have been produced by reacting various branching molecules at the hydroxy groups of the Bis-GMA (Holter et al., 1997). However, initial results suggest that these polymers have a low elastic modulus. While this low modulus and lower shrinkage would likely result in lower contraction stress than in Bis-GMA-based polymers, the low modulus (50% of Bis-GMA-based resins) may limit their usefulness as dental restorative resins. New trimethacrylate monomers (1,1,1-Tris[4-(2’-hydroxy-3’-methacryloxyloxypropoxy)phenyl]ethane and 1,1,1-Tris[4-(2’-hydroxy-3’-methacryloxyloxypropoxy)phenyl]methane) were developed, producing composites with slightly reduced polymerization shrinkage and lower water sorption than Bis-GMA-based composites, but with similar conversion and flexural strength (Chung et al., 2002a,b).
Other approaches proposed for reducing polymerization contraction in dental composites include the development of liquid crystal monomers (Rawls et al., 1997) and cyclopolymerizable di- and multi-functional acrylate resins (Stansbury et al., 1995). A methacrylated derivative of styrene-allyl alcohol, MSAA, to be used as a comonomer for dental composites, was synthesized to improve strength and conversion (Culbertson et al., 1997a). In one study, MSAA was used to replace 20% of Bis-GMA in a highly filled Bis-GMA/TEGDMA composite and showed a 20% reduction in polymerization contraction stress (Condon and Ferracane, 2000). The addition of large amounts of MSAA has a significant negative effect on mechanical properties, however.
Conclusion
Polymerization contraction stress has been the subject of intense research activity over the last few years. Though most of the factors involved in stress development have been identified, further studies are necessary to access the individual contributions of the composite’s physical properties (namely, volumetric shrinkage and elastic modulus) and curing kinetics (as a factor determining stress relief by viscous flow), and the potential interactions between them. Some of the proposed non-continuous curing routines have been shown to reduce contraction stress significantly. However, results of interfacial integrity studies are inconsistent, and, in some cases, stress reduction might be caused by a lower degree of conversion. Stress reduction with the use of low-elastic-modulus liners seems to require materials with stiffness close to that of unfilled resins. Apparently, many of the flowable composites currently available are too rigid to be used for this purpose. Developing low-shrinkage monomers that could match other clinically important properties found in Bis-GMA-based composites is a challenging task. Nevertheless, some studies have shown promising results regarding contraction stress reduction.
Contraction Stress of Current Composites
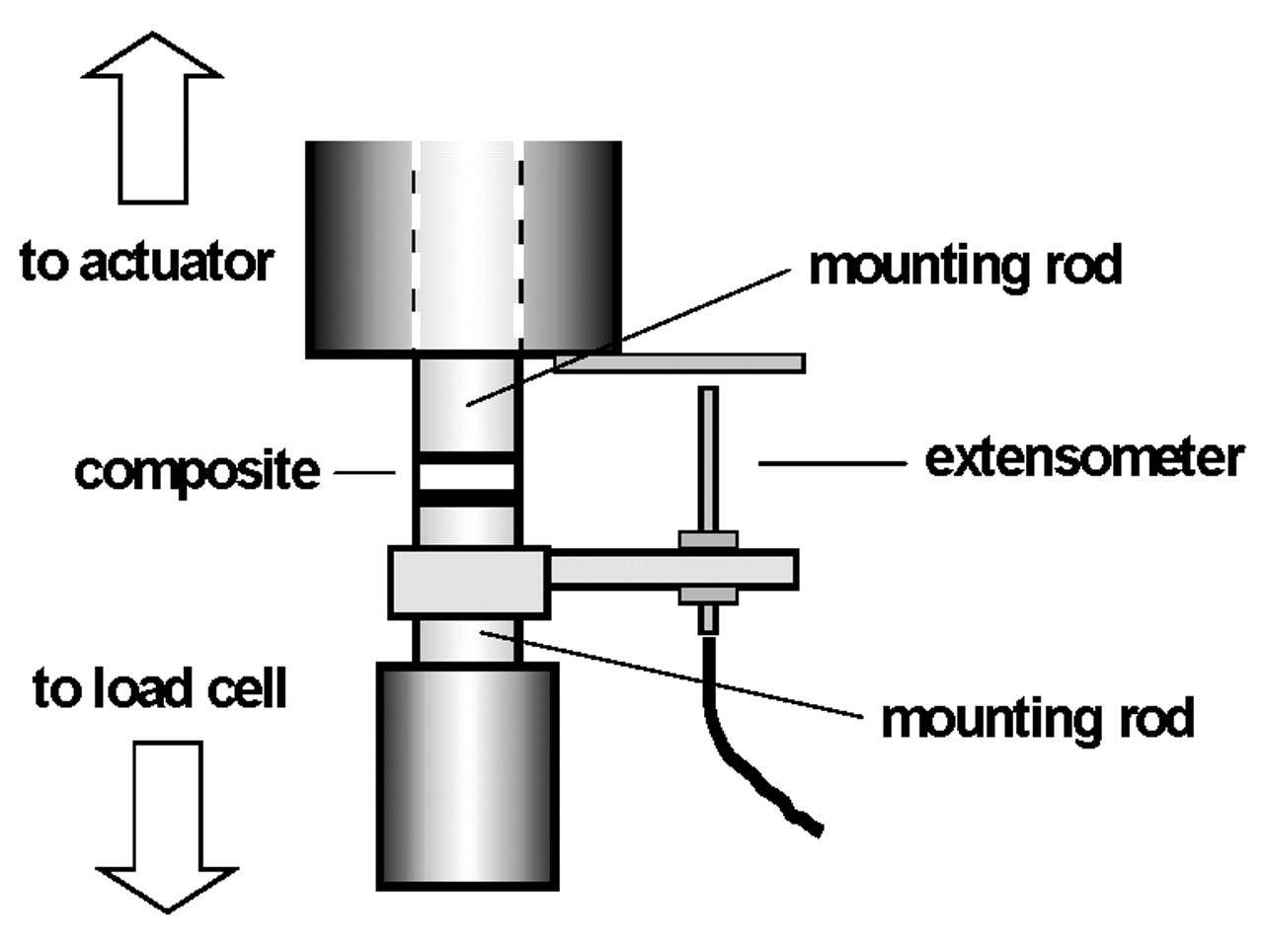
Diagram of the contraction stress test set-up.
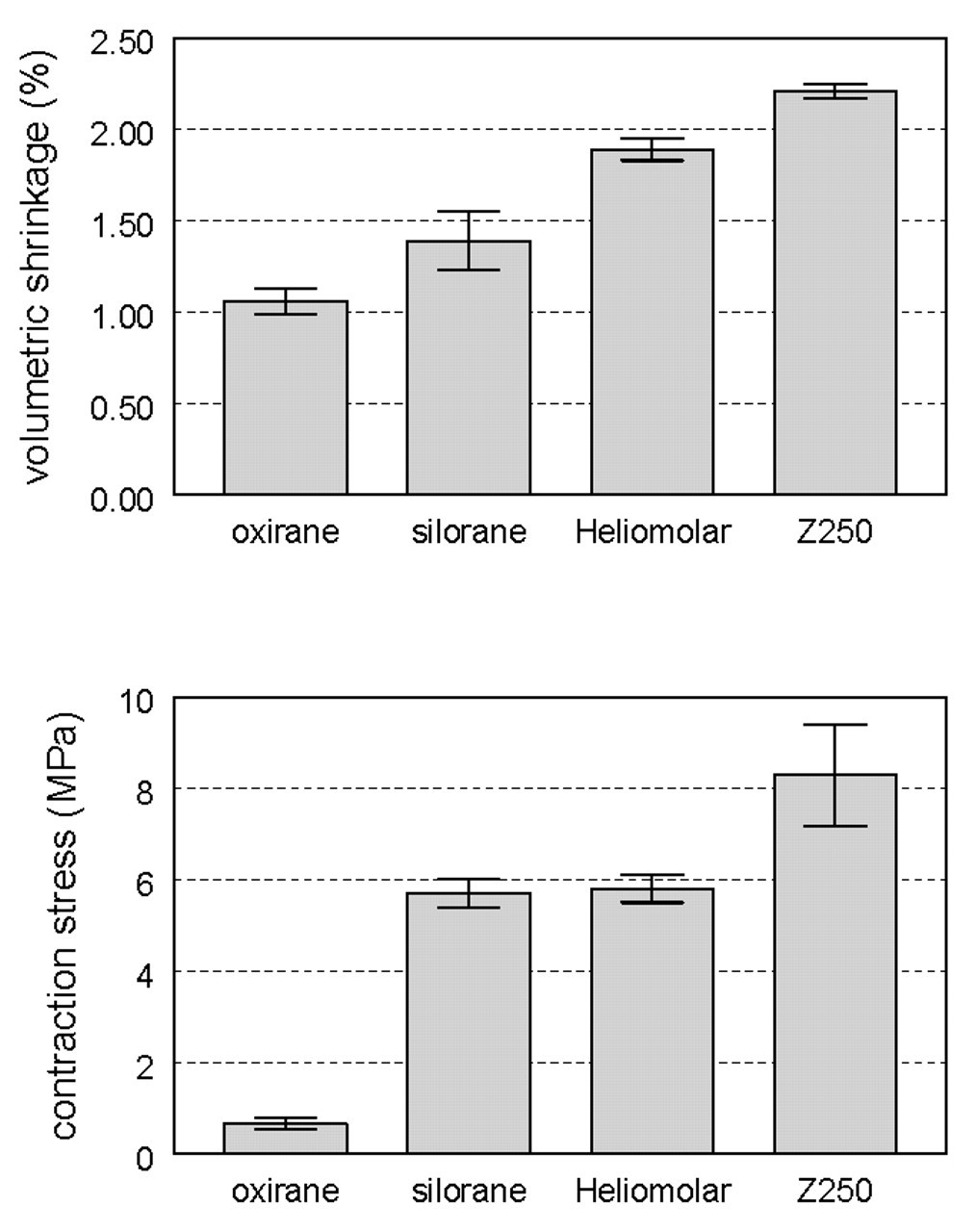
Volumetric shrinkage (top) and contraction stress (bottom) of an oxirane- and a silorane-based composite compared with two commercial composites.
Footnotes
Acknowledgements
This paper is based on a presentation at the 39th Meeting of the Brazilian Academy of Dental Materials (July, 2003). Portions were printed as proceedings in, and are reprinted here with permission of, the Journal of Applied Oral Science.