
Abstract
This qualitative study reports how 20 spiritual care leaders provided leadership in the early months of the COVID-19 pandemic. The patterns and themes that emerged centered around the changing world of chaplaincy, the administrative role of the leader, and the personal story of the leader. Spiritual care leaders demonstrated creativity with the potential to shape chaplaincy in positive ways, expanding the reach of spiritual care.
Leaders play an important role in teams and organizations. They help set direction, strategic goals, for teams and organizations. They also help teams work together productively to achieve those goals. Research describing the work of spiritual care leaders is relatively new and still limited. An important early study examined chaplaincy programs in 17 leading US hospitals (Cadge, 2012). Based on her interviews with chaplaincy leaders and staff chaplains, Cadge described three broad types of chaplaincy departments: professional, traditional, and transitional. In the professional departments (4 of the 17), chaplains were well integrated into their institutions. They were salaried employees, followed protocols to routinely respond to specific situations (e.g., code blue), were members of the interdisciplinary care team, part of many hospital committees, and saw care for patients and families as their priority. Transitional departments (3 of the 17) were in the process of becoming professional. Among the factors associated with the chaplaincy department type, Cadge observed “professional and transitional departments have…grown and became integrated into their hospitals through the efforts of managers who became familiar with the language and priorities of the healthcare system. These managers then developed strategies to build their departments” (p. 119).
Cadge’s (2012) observation about the importance of spiritual care managers’ becoming “familiar with the language and priorities of [their] healthcare system” highlights the importance of the relationship between spiritual care managers and the executives to whom they report (p. 119). Antoine et al. (2020, 2021) interviewed 11 healthcare executives before the COVID-19 pandemic to learn what they knew about and valued in the spiritual care programs in their organizations. They found the executives valued the support that chaplains provided to healthcare colleagues in tragic situations and during organizational change. The executives also valued chaplains for their high-quality care, reliability, and responsivity to emergent patient and staff needs, and for their clinical training and experience working within a complex environment.
While Cadge’s (2012) research pointed to the important role of spiritual care leaders in building effective spiritual care programs, Kim et al. (2022) addressed the issue of the competencies needed for this work. They examined the applicability for spiritual care leaders of the seven domains of the Healthcare Leadership Model of the National Center for HealthCare Leadership. The domains include health system awareness and business literacy, self-awareness and self-development, relations, execution, and transformation. Based on Behavioral Event Interviews with 10 spiritual care managers, they found the Model provided a useful framework for understanding the competencies required for effective healthcare spiritual care management and leadership.
The COVID-19 pandemic has had an enormous disruptive impact on healthcare around the world. Studies have described the impact of the pandemic on spiritual care services and the creative ways that healthcare chaplains responded (Desjardins et al., (in press); Harrison & Scarle, 2020; Snowden, 2021). For example, between May and September 2020, Jones et al. (2020) interviewed 17 Australian spiritual care practitioners, 6 were spiritual care managers. They reported several ways that chaplains responding to the pandemic including providing a calm presence, being available, holding out hope, and introducing creative ways to provide spiritual care.
The importance of good leadership becomes more evident when a crisis occurs. The COVID-19 pandemic created immense challenges for leaders and managers in all healthcare sectors, including managers of spiritual care programs. To better understand the role of Spiritual Care Leadership in the pandemic, Szilagyi et al. (2022) conducted a focus group with a panel of 10 international leaders in spiritual care and research who had been involved in research on spiritual care during the COVID-19 pandemic. The participants were asked to describe leadership characteristics and actions that shaped the integration or perceived value of chaplains during the COVID-19 pandemic. Six themes emerged as central to determining chaplains’ integration, perceived value, and contributions during the pandemic: professional confidence, engaging and trust-building with executives, decision making, innovation and creativity, building integrative and trusting connections with colleagues, and promoting cultural competencies. Aside from this study, there are no other reports examining how managers of spiritual care programs responded to the challenges of the COVID-19 pandemic.
Objective
The objective of this study was to describe how a sample of spiritual care leaders (directors/managers) across the United States provided leadership in their departments and organizations in the early months of the COVID-19 pandemic.
Methods
Participants
The study employed qualitative interviews with managers of spiritual care programs in United States healthcare organizations. The project sought to recruit participants with diverse perspectives on the effects of the pandemic on healthcare organizations and spiritual care programs. These included geographic location, including pandemic hotspots; type of healthcare organization (faith-based, academic medical centers, community hospitals, and safety net hospitals); and management role (organization director for spiritual care, regional director for spiritual care, and manager for hospital spiritual care program). As this was a joint project between Ascension and Transforming Chaplaincy, participants included spiritual care leaders within the Ascension system as well as contacts from Transforming Chaplaincy. Ascension refers to one of the largest Catholic health care systems in the United States with hospitals in 12 states. Transforming Chaplaincy is an organization that promotes evidence-based spiritual care and the integration of research into professional practice through education, consultation, and research projects.
Interviews
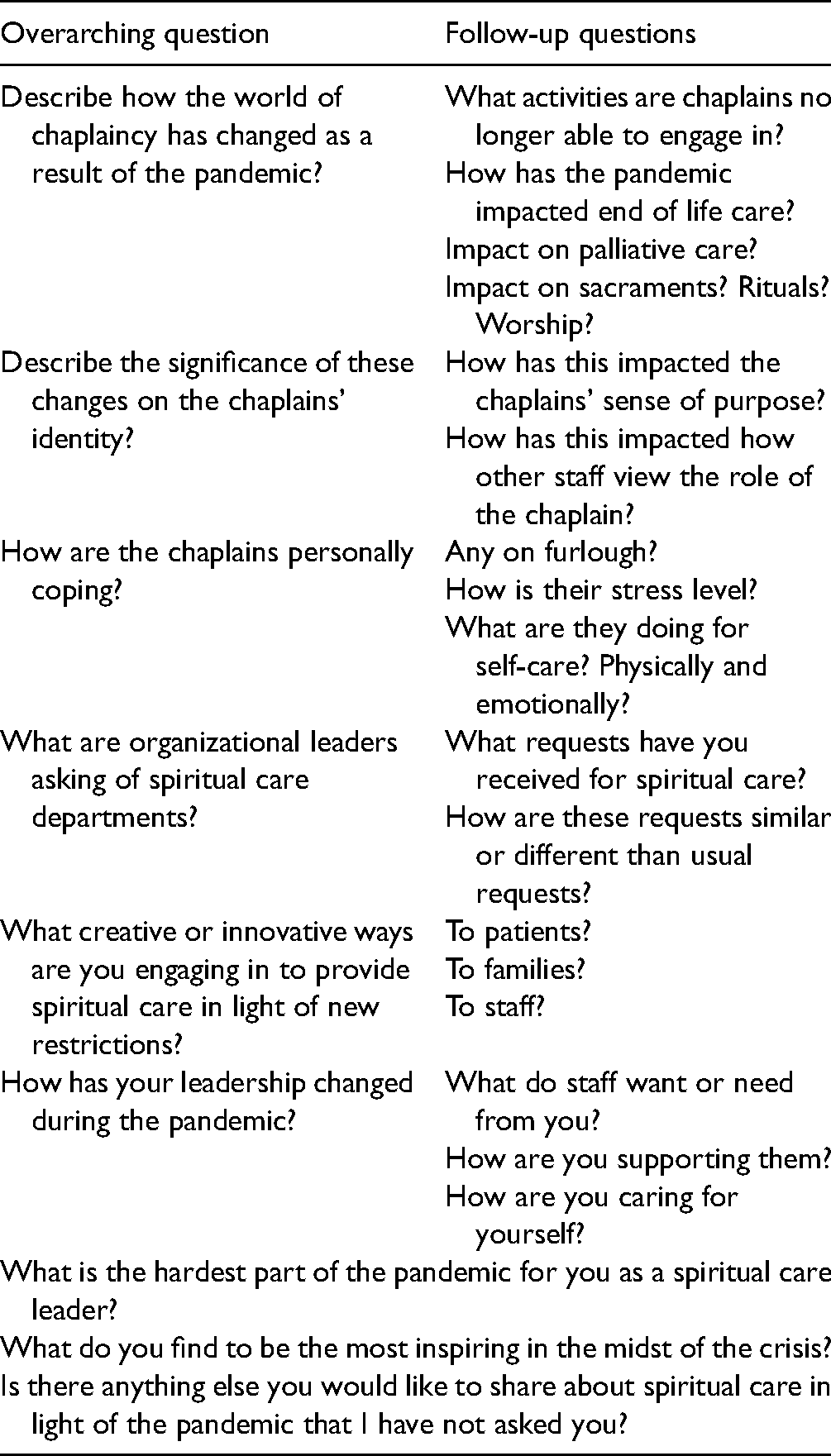
The interviews were conducted in the early months of the pandemic between late March and early June 2020. Participants were asked open-ended questions about their experiences of leading a spiritual care department during the COVID-19 pandemic (refer to Table 1 for the interview questions). Participants were interviewed virtually utilizing Zoom or Google Meet. Interviews lasted approximately 45–75 min. The Ascension cohort interviews were conducted by the lead author and the Transforming Chaplaincy cohort interviews were conducted by the second author. Interviews were recorded and transcribed verbatim. The project received an expedited review from the Ascension IRB as well as from the RUSH University Medical Center IRB.
Interview questions.
Methodology
This analysis of the interviews utilized hermeneutic phenomenology. One of the key philosophers for hermeneutic phenomenology is Martin Heidegger whose principles of the person provided a methodological foundation. There are five key facets to Heidegger's concept of the person including:
Persons as having a world. The person as a being for whom things have significance and value. The person as self-interpreting. The person as embodied. The person in time (Leonard, 1994, pp. 43–63).
One of the fundamental aspects of Heideggerian phenomenological methodology is its focus on essences or themes that emerge from studying the lived experiences of persons and thus give subsequent meaning to a phenomenon—meaning that may be hidden in empirical research approaches. Heidegger's phenomenology is concerned with ontology: in the case of this study, we asked how does the COVID-19 pandemic influence leading a spiritual care department and how does Spiritual Care Leadership evolve because of the pandemic.
Data Analysis
Transcribed interviews were uploaded into the qualitative data analysis software program Atlas.ti. 8 Windows (2019). Interviews were analyzed by a team that included all authors. Three interviews were initially read by the entire team to ensure there was consensus regarding the creation of a code book of patterns that were present in all interviews and themes that represented the ways the patterns manifested themselves. Once the code book was established, interviews were divided among team members so that every interview was coded in teams of two. The entire research team met regularly to discuss the analysis process, explore emerging themes, and to make any necessary changes to the code book. Heidegger's five principles of the person provided the foundation for creating the codebook and analyzing the interviews. The research team collectively identified the patterns and themes.
Results
Sample Characteristics
Twelve Ascension leaders were solicited for participation. Only one declined resulting in a 92% participation rate for the Ascension cohort. Twelve leaders were approached by Transforming Colleagues: nine were able to participate (75% participation rate). Participants included leaders of spiritual care departments located across the United States. Some participants had the job title of manager while others were labeled a director. Therefore, this paper will utilize the term “leader” as inclusive. The Ascension cohort included 11 leaders and the Transforming Chaplaincy cohort included 9 leaders (Table 2).
Study participant description (N = 20).
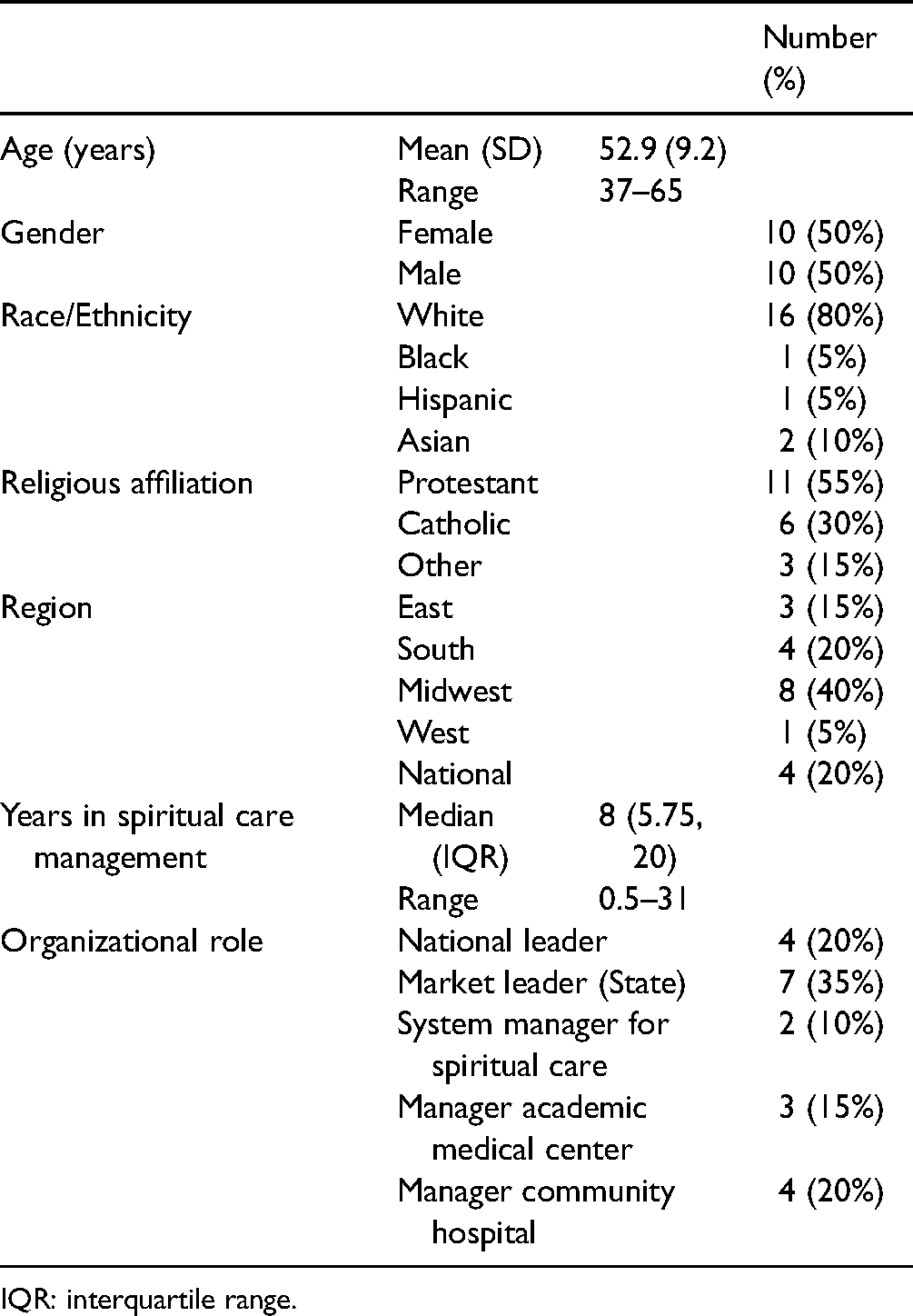
IQR: interquartile range.
Stories of Spiritual Care Leadership: Phenomenological Patterns and Themes
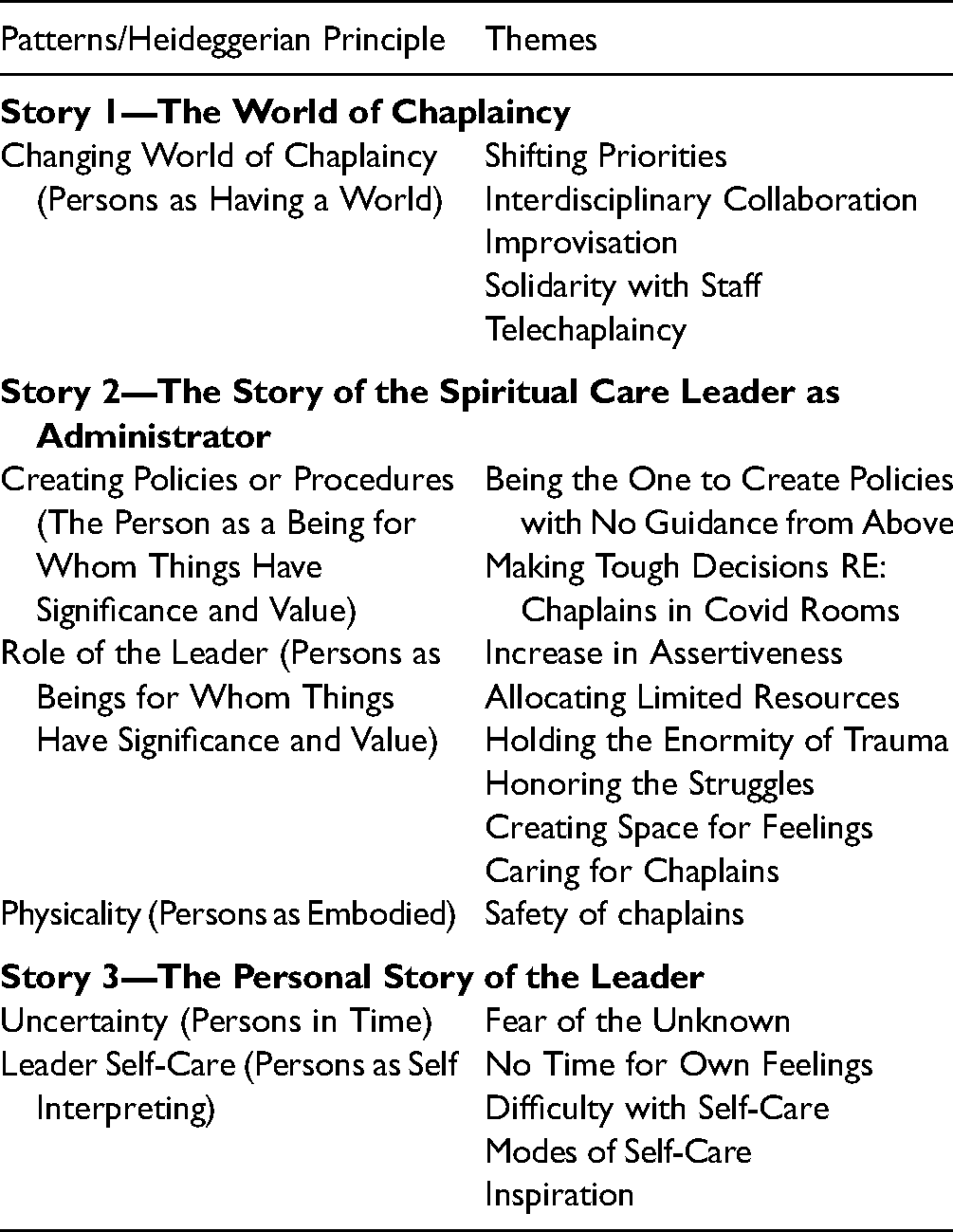
Three stories make up the larger story of Spiritual Care Leadership during the COVID-19 pandemic including (1) the story of the changing world of chaplaincy; (2) the story of the spiritual care leader as administrator; and (3) the personal story of the leader. These stories consisted of phenomenological patterns manifested in various themes (Table 3).
Patterns and themes.
The Story of the Changing World of Chaplaincy
Heidegger's first principle of the person is “persons as having a world.” Spiritual care leaders function within multiple worlds: professional chaplaincy; healthcare; individual hospitals; and the administration of those hospitals. All study participants talked about how the world of healthcare and the hospital changed overnight with the onset of COVID-19. For spiritual care leaders, this acutely manifested itself in terms of the impact on the world of chaplaincy and subsequently their leadership. The pattern of the Changing World of Chaplaincy was present in all interviews. This pattern manifested itself in five key themes: (1) shifting priorities; (2) interdisciplinary collaboration; (3) improvisation; (4) solidarity with hospital staff; and (5) the shift to telechaplaincy.
World of Chaplaincy Theme—Shifting Priorities: Prior to COVID-19 chaplains were present at codes, crises, and deaths, primarily to care for family members of patients. However, with the advent of COVID-19, hospital visitation policies prevented families from being in the hospital. In some cases, chaplains themselves were prevented from entering the rooms of COVID-19 patients either due to a lack of personal protective equipment (PPE) or to protect chaplains who were at high risk. These factors contributed to shifting priorities turning the world of chaplaincy upside down overnight. One participant summarized, “I think it has made us rethink what does it mean to be a leader in a time of great need, and how can we support, through our pastoral and spiritual skills, those that serve under us. It has made us rethink who we are amid great pain and suffering.”
World of Chaplaincy Theme—Interdisciplinary Collaboration: Interdisciplinary collaboration rose to new heights as chaplains were invited into new conversations. It’s like we’ve never been as prominently featured as we are right now and it’s actually been breathtaking to see that happen, but I see it happen on a micro level as well where, you know, I and my team, we get invited into things we never got invited to even in a faith-based system. It’s like everybody wants us at the table and it’s actually a little bit disorienting because of how much that’s happened.
A doctor said to me, “Hey, I’ve got a lot of doctors that are saying that they really don’t know how to emotionally connect with their patients through virtual visits, And I think you and your team could have a lot to teach us about that,” Meaning that we have something to teach about how to connect with people emotionally, how to establish rapport in a rapid way emotionally in times of stress.
Chaplains were asked to collaborate with healthcare colleagues in multiple ways including:
- Praying at unit and safety huddles. - Coordinating with nurses to call into patient rooms or call families at home. - Serving on teams because of the unique skill set of chaplains. - Providing a new or stronger presence on palliative care teams. - Partnering with Employee Assistance Programs (EAPs) to care for healthcare colleagues. - Training Catholic nurses to provide the Eucharist when nothing else would help patients and no priest was available. - Providing consultation as experts including (1) Educating physicians on how to form relationships with patients or families virtually, (2) Honoring the healthcare colleagues who died due to COVID-19, and (3) Collaborating on “No One Dies Alone” programs.
World of Chaplaincy Theme—Improvisation: Traditional modes of care during the pandemic became impossible. Things like having chaplains physically in patient rooms, being physically present with families, and offering in-person sacraments and rituals, were no longer safe or practical. It is accelerating the creativity and innovation around delivery models of spiritual care. With COVID-19 and how unprecedented it is in so many ways for us, chaplains are having to be creative in the ministry of presence, and what presence means, what presence can look like, as well as looking at pastoral methods to get at that care.
If you watched the movie “Moneyball,” which is about baseball, they're moving towards a whole statistical model and the manager doesn't want to do it, so he keeps putting in whoever he thinks is best, and so finally what the GM does is he just fires everybody that the manager has. He's like you can't use them because they're not there anymore, and I think that's kinda what's happened to us. We're like oh, what we could have fallen back on, because that's what we knew, and we knew worked, is not there, so I guess we'll just try something new.
Spiritual care departments were able to quickly pivot to creative ways of providing care and rituals. For example, one department created a way for Muslim associates to pray. “Because of the restrictions, we took out our regular prayer rugs and put them in plastic.” One department created a ritual for dying patients that included a card sent to families so loved ones would know, “caregivers were present, hands were held, soothing sounds in the room were playing, words of comfort or prayers were spoken. It is really traumatic for families not to be there, so we’re trying to mitigate that just in the smallest of ways by letting them know there was some love presence around the patient.”
World of Chaplaincy Theme—Solidarity with Staff: Providing spiritual care to healthcare colleagues has always been part of the chaplain's role. However, the needs of staff became a primary focus, not just in terms of traditional spiritual care to individuals, but reinforcing that chaplains are with staff in the crisis. “Being there at change of shift and when they’re coming in and they’re getting their temperature checked and to be able to say some word of blessing that is authentic and natural, not a formal blessing, to folks as they start their days.”
Some of the other things leaders shared were taking candy to night shift, environmental or transport staff to show that spiritual care was available to them in addition to the day shift medical teams. One department created daily emails with a reflective poem, or calming video for staff. Early in the pandemic one of the biggest fears nursing staff shared with chaplains was how to care for their clothes so they did not pass COVID-19 onto loved ones. A spiritual care leader collaborated with nurse leaders and their Ascension Foundation to create “go bags” for nurses so they could put their stethoscope, lab coat, etc., in it and place the bag in the trunk of their cars. The bags included laundry detergent and a sheet with safety tips for how to keep loved ones safe when the nurse came home from work. The Foundation paid for the bags and the nurse educators created the safety tips. This is a prime example of collaboration and solidarity.
World of Chaplaincy Theme—Telechaplaincy: With many traditional methods of being present with patients and families removed due to safety concerns during the pandemic, the role of telechaplaincy increased dramatically. Leaders spoke of some chaplains’ hesitancy to make phone calls, use iPads, Zoom, or FaceTime as a means for connecting the chaplain to the recipient of care or connecting patients with loved ones. Leaders commented that chaplains who were comfortable using these modes of communication in their personal lives were able to easily adapt them to their chaplaincy. “We've never, never been involved in telephone ministry to the degree we are now and that has had a huge impact on being a chaplain. It's also something that has drawn us I think into creative areas, into innovation in ways that I don't think we had thought about before, like having a prayer service for staff on Zoom.”
Due to safety concerns, chaplains were not able to physically go into patient rooms, visitors were not allowed in the hospital, and chaplains with comorbidities or weakened immune systems were forced to work from home. Departments pivoted to having chaplains call patients from the nurses’ station. Chaplains working from home were able to call patients’ families. These chaplains often began their day by checking in with charge nurses to find out which families were top priority. For those chaplains still working inside the hospital, iPads, tablets, and phones became essential tools in the chaplain toolkit. Spiritual care department leaders often worked with their local foundations to secure funding to purchase iPads or tablets.
Reaching loved ones virtually was essential as COVID-19 patients died without their loved ones. Nurses and chaplains worked together to have loved ones present virtually as the families said their goodbyes. Hospital policies varied in terms of whether Catholic priests were allowed to be physically present in patient rooms. “We had to FaceTime or Zoom with a priest and then remotely provide a sort of Sacrament of the Sick, you know, for a dying patient in that kind of circumstance.”
The Story of the Spiritual Care Leader as Administrator
Spiritual care leaders carried the burden of leading their chaplains amid an unprecedented crisis. They juggled the needs of patients, patient families, chaplains, healthcare colleagues, and the larger hospital system. Protecting the significant needs of all entities was difficult as sometimes they were in conflict. This story includes three patterns with themes that overlap at times. These included creating policies or procedures; the role of the leader; and physicality concerns. The first two patterns adhere to Heidegger's concept of the person for whom things have significance and value with the third adhering to the principle of the person as embodied.
Creating Policies or Procedures: This pattern resulted in two themes; making decisions with little or no guidance from administrative leaders and determining when to send chaplains into patient rooms. “I think the hardest part has been for me this, I don’t know if isolation is the right word, but isolated from my own boss and having to make these decisions that I was not confident in.” “The hardest part really has been the guilt of sending anyone in harm's way.”
In the early days of COVID-19, PPE was quite limited. Leaders had to make tough decisions about rarely, if ever, sending chaplains into COVID-19 rooms. They also had to decide which chaplains would be assigned to COVID-19 units. Some chaplains volunteered while others were assigned despite their own fears and anxieties. Another group of chaplains including Catholic priests had trouble discerning how they were going to provide spiritual care without being physically present. Leaders had to balance many variables when making decisions that were unpopular for a variety of reasons. COVID-19 drastically impacted hospital revenue and costs. In some cases, this resulted in spiritual care leaders having to make difficult decisions about which chaplains to furlough.
As visitors were restricted, department leaders had to tell local clergy they could not visit parishioners due to hospital policies. Leaders had to make tough decisions about policies or procedures for worship and rituals. In-person worship services were discontinued and some chapels were closed due to safety concerns. One of the biggest issues was how to handle Catholic sacraments for dying patients. The Pope implemented a special indulgence to account for patients who could not receive the Anointing of the Sick. However, some patients or families still insisted on receiving the Sacrament which meant creating procedures for doing so that kept everyone safe.
The Role of the Leader; This pattern included the following themes: increasing assertiveness, allocating limited resources, holding the enormity of trauma, honoring the struggles, creating space for feelings, and caring for chaplains. Leaders expressed an increase in assertiveness during the pandemic crisis. “You know, our team is very collaborative almost to a fault and that's tended to be how I have provided leadership to this department… We don’t have time now to get everybody involved in the decision. It's not a consensus process anymore. And so, that's been a little bit of a struggle for some.”
Allocating limited resources encompassed not only policies around limited PPE, but also the staffing and placement of chaplains. Departments shifted to provide more extended coverage within hospitals rather than just 9:00 am to 5:00 pm. A regional leader created a plan for sending chaplains to hospitals with the greatest need based on COVID-19 numbers. Departments themselves experienced staffing shortages as chaplains became sick with the virus. All of this resulted in the leader having to rethink how spiritual care was provided.
Many of the themes in this section had to do with caring for the chaplains in some form or another. In addition to increased administrative responsibilities, leaders were the ones who became a chaplain to the chaplains. While chaplains held the stories of patients, families, and associates, leaders held the stories of the chaplains. “Yeah, I think the hardest part for me is there were a few of our chaplains who had much higher anxiety about all this than the rest. And seeing them suffer with that anxiety was hard on me.” “That's the bottom line of my leadership here to inspire people just by letting them know how I see their struggle and how hard they’re working and how scared they are… So, that's sort of like how my leadership has changed during this time.”
Leaders were proactive in creating space for chaplains to vent and share their feelings. “We do a daily check in with the chaplains, how are you feeling? What's going on? Anything that we need to know? We're more focused on just spending a little time in that manner.” One of the key priorities for spiritual care leaders was to care for their chaplains. One participant is the spiritual care director for several hospitals within her state and has managers that help her lead. I’m having two to three leadership team meetings a week. I’ve averaged two meetings with all the staff a week in the last three weeks. We’re a big team, so I’ve got our leadership team. Even {Manager}can’t handle providing care for all these chaplains. I’ve got all of our leadership team setting up check-ins with their teams for personal sharing.
Physicality: This pattern pertains to Heidegger's principle of the person as embodied. By this, he meant that we are souls navigating the world through our bodies (Leonard, 1994). If something changes with our body, mobility, sight, hearing, etc., then we must navigate the world in new ways. One of the key roles of the spiritual care leader was to continue to provide spiritual care services while also being mindful of the physical safety of the chaplains and their families. Sending chaplains into harm's way, weighed heavily upon them. Balancing the needs of all members of the department and yet having to make logical decisions as some chaplains had comorbidities or were older in age. Some chaplains had family members who were at higher risk. Chaplains who could not visit patients in the hospital helped by making phone calls to patients’ families or checking on associates. Chaplains were able to pivot to phone calls to varying degrees resulting in leaders providing supervision in terms of navigating the world of chaplaincy in new ways without the physical presence of bodies.
The Personal Story of the Leader
Amid all the other things that the leaders were carrying, they had their own experience of the pandemic. One pattern centered around the uncertainty of the pandemic. This correlates to Heidegger's principle of the person in time. We all have a past, present, and future. We bring with us into the present our past experiences and our hopes and expectations for the future. The uncertainty of the pandemic threw all of that into question. The other pattern centered around the leaders’ self-care. Under this pattern, they described the following themes: no time for their feelings, difficulty with self-care, different modes of self-care, and what inspired them amid it all. Heidegger's principle of the person as self-interpreting coincides with this pattern. What constitutes self-care is up to the individual to interpret for themselves.
Uncertainty: At the beginning of the pandemic, there was a great deal of uncertainty related to the physical safety of selves and family members, how the virus was transmitted, who survived COVID-19 and who died, and how long the crisis would last. Spiritual care leaders experienced their own anxiety related to all these factors. “I think that the underlying dynamic is uncertainty, unknown and it's requiring all of us people of faith to have anchors that are different from anchors that are in the world of my job is secure, my salary is secure, my health is secure. Those aren’t true anymore. You know, all these assumptions that we have lived with have all been challenged.” For some leaders, these assumptions were challenged on a very personal level. “On Easter and that weekend, I was having symptoms of COVID-19, and I had to go get tested on Easter Sunday, and that whole weekend, I spent in our little isolation room. Just the thought that I had brought this to my home made me rethink everything, and it was like forget it, I’m not feeling this, you know. This is way too much of a cost. I cannot put my family at risk.”
Self-care: Leaders were so focused on juggling administrative responsibilities and caring for their chaplain teams that they described not having time to process their own feelings. “Sometimes I’m really skillful at seeing everyone else's stuff and less reflective about what I need.” They often realized they were having difficulty with self-care when there was a crisis of sorts. You know, I did have a moment of crisis in the midst of all this where, you know, my one son had a history of really aggressive temper loss. He was in the midst of something like that at home and I was short of temper. I felt really on edge. I kicked over a trashcan and I went charging across the kitchen and I literally don’t even remember what happened there. I was literally like hopping mad. I somehow jumped into a door frame. My head jammed into the corner of the doorframe. All of a sudden, I’m on the floor, my head is bleeding and I’m weeping, and my children are scared and they’re coming around. You know, my head is bleeding and then my wife helps me to the bathroom and I’m just like bleeding out of my head and just crying for like an hour, you know. So, that was—thank—you know, thank goodness, I’ve been able to do a little better since then, but that was a real wakeup for me that I’ve got to take good care of myself.
Leaders identified several things that helped with self-care including getting a good night's sleep, processing their experiences with a support system of some kind, walking or some other form of physical exercise, camping, taking a day off, scheduling family time, journaling or writing poetry, and praying or meditating. One leader described reading and the importance of genres during the pandemic. “I am a really big reader, and I read a lot of different things. I read some of everything, but right now I'm finding it is really good for me to read fantasy. It's kind of like watching an escape movie. It allows me to escape. I don't want to read a book about World War II right now.”
Participants were asked during their interviews what they found inspiring. They were inspired by several things including the way chaplains stepped up during the crisis, the gratitude from other hospital staff for the spiritual care chaplains provide, the positive exposure spiritual care received, and the deeper personal connections with colleagues as they supported one another. “I think the sense that people are working together in ways that they haven't before, less siloed, less territorial, less regional.” “What inspires me most I think is the capacity for sacrifice. When I think about our chaplains and our nurses and physicians, really everybody is involved. There's just tremendous sacrifice for the other, for the other, that is there. It just says that this is what love looks like. This is what love is.” I am incredibly inspired by the fact that the vast majority of my chaplains get up every day and consider it a privilege to go serve people in our hospital sites. They have fears, they have concerns, they have young kids at home or older spouses at home. They have challenges and they are a hundred percent committed to being present for people through this and walking through this…When people call me at night and they're upset, it has happened that some of them are like I'm just breaking down. I don't know how I can keep going home to my family, but for the most part it's them just wanting to release some tension and stress so they can come back to level and balance, so that they can walk right back in and do it all again tomorrow.
Discussion
The objective of this study was to describe how a sample of spiritual care leaders across the United States responded in the early months of the COVID-19 pandemic. Heideggerian hermeneutic phenomenology was utilized as the methodology by which interviews were analyzed. Findings from the interviews led to three stories or chapters that tell the overall story of the experiences of the leaders. The first story contained one robust phenomenological pattern, the Changing World of Chaplaincy, which manifested itself in several themes. Priorities within chaplaincy shifted challenging long-held norms of who is the recipient of care. With emphasis given to caring for staff, interdisciplinary collaboration and solidarity became primary. Leaders had to support their teams in engaging in new modes of being present. The world of chaplaincy will never be the same as innovation brought out new tools for the spiritual care toolbox.
The second story contained three patterns shedding light on the ways the pandemic shaped participants’ leadership. This story provides a key look at the ways in which the experience for leaders was different than that of individual chaplains. Spiritual care leaders had to balance multiple priorities and make difficult decisions regarding their staff, including feeling fear and guilt over assigning chaplains to COVID-19 units. They also had to provide spiritual care to their staff in new ways. Spiritual care leaders expect to support their staff during a crisis event. COVID-19 was different in that it was so pervasive, all-encompassing, and prolonged well beyond a typical crisis event.
This leads to the third story of how leaders did, or struggled to, care for themselves. For many, there was an initial adrenaline rush associated with being needed by the hospital and their team. Some leaders did a better job than others at proactively practicing self-care while others hit a crisis point as all the emotions of leading during the pandemic caught up with them. Yet, leaders were able to readily share what they found inspiring in the midst of the struggles and suffering.
Study Strengths
Other studies have described the experiences of individual chaplains during the pandemic (Desjardins, et al., (in press); Szilagyi, et al., 2022). One of the strengths of this study is its focus on spiritual care leaders and their unique perspective. Participants were drawn from across the United States and represented spiritual care leaders of a single hospital, several hospitals, and state markets including those in a large Catholic healthcare system. Another strength is the high rate of participation from those who were invited to participate. Qualitative research methodology is a strength of this study as it allowed for a deeper understanding of the experiences of spiritual care leaders leading during an unprecedented worldwide crisis.
Study Limitations
The study is based on a convenience sample of spiritual care leaders recruited through contacts and networks of the research team. More than half of the leaders who participated in the study (12/20, 60%) work in faith-based healthcare organizations, including 11 from the same organization. Faith-based hospitals make up a minority of hospital in the United States (18.5%) (Guiahi, et al., 2019). We were unsuccessful in recruiting any spiritual care leaders from safety net hospitals and only two leaders in the study worked in cities that were hardest hit by the early wave of the pandemic. While there was considerable consistency in the experiences reported by the leaders who participated in the study, we cannot know whether a different sample would have reported different experiences or interpretations of those experiences.
Implications for Future Research
Throughout the interviews, leaders referred to varying levels of the integration of their spiritual care department as well as their own personal integration as a leader within their hospital systems. Cadge (2012) has suggested that spiritual care leaders’ integration in their organizations plays an important role in the services that are provided. Since participants were not directly asked about their integration within their hospital systems, it would be helpful to conduct future research to better understand factors that contribute to or hinder the integration of spiritual care. Some leaders were invited to attend COVID-19 daily huddles, not just to offer a prayer but as a full member of the team. There was variation in the degree to which spiritual care leaders were asked to collaborate in organizational decisions. One leader stated she was only contacted by administrative leaders when money was tight, and she was asked to furlough chaplains. It is unclear what factors, including institutional culture or leaders’ skills, led to leaders and spiritual care being more fully integrated into their organizations (Szilagyi et al., 2022).
Conclusion
The COVID-19 pandemic turned the world and the world of chaplaincy upside down. Spiritual care department leaders carried burdens at multiple levels as they navigated the needs of patients, families, healthcare colleagues, and the chaplains they supervised. They worried about the physical safety of their chaplains, the chaplains’ families, and their own families’ safety. Yet, despite all of the burdens and stress, leaders helped shape care during the pandemic by tapping into creative ways to maintain the essence of spiritual care while also increasing the modalities by which it was provided. This project highlights an important component of the larger story of how the profession of chaplaincy responded to the pandemic by focusing on the important contributions made by spiritual care leaders.
Footnotes
Acknowledgments
The authors wish to thank those spiritual care leaders who shared their time and stories with us as part of this research project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.