
Abstract
How are spiritual needs addressed in long-term care? This quantitative study explored the level of spiritual care offered and qualifications of spiritual care providers in 177 LTC homes in Ontario. Data showed 49% of homes employ Spiritual Care Providers (SCPs), with more positions in urban and not-for-profit homes. Findings revealed SCPs bring a substantial skill set, attending to needs of residents, families and team members. More consistent staffing for spiritual care provision across the sector is recommended.
Keywords
In its opening sentence, the Ontario Long-term Care Homes Act (2007) recognizes that “a long-term care home is primarily the home of its residents and is to be operated so that it is a place where they may live with dignity and in security, safety and comfort and have their physical, psychological, social, spiritual and cultural needs adequately met.” Although it is true that long-term care (LTC) is healthcare and must meticulously address the medical needs of residents, LTC is also “home,” most often one's final home, and so it is vital that not only the residents’ bodies but also their spirits, are provided for.
What is spiritual care? Spiritual care is care that recognizes and responds to the needs of the human spirit (including the need for connection, emotional support, respect for values and beliefs, and the search for meaning in life/suffering). Spiritual care facilitates religious care from one's own faith leader/community, meeting needs for relationship and continued participation in religious practices/tradition. Spiritual care includes, but is not confined to, religious care.
How spiritual care has been understood and provided in LTC has evolved over the years as the role of religion in society has shifted and the population of Ontario has diversified. Because the actual provision of spiritual care in Ontario LTC is at the discretion of individual homes, there is great variation in how it is provided and there have been no data available. Many homes are increasingly wondering where spiritual care fits, who takes responsibility, and how program funding dollars are best allocated.
Literature Review
Long-term care homes in southern Ontario have their roots in the values of Judeo-Christian communities that strove to provide for people in need of care. Municipal Houses of Refuge, private hospitals, and charitable homes have evolved into today's landscape of LTC. Throughout the last century, most “nursing homes,” and especially those connected to faith communities, were assumed to be a place of ministry for local clergy and congregations, and/or employed a chaplain. The spiritual and religious needs of residents were assumed to be met in the context of the wider community (Brandeis & Oates, 2007). Over time, changes have affected the role and provision of spiritual care: LTC has become part of our highly regulated and secular healthcare system; our society is becoming increasingly diverse, culturally and religiously; and dementia is prevalent among residents. As our society's relationship with religion and spirituality has been shifting, it is less clear what meets the spiritual needs of our elders, and there is danger of spiritual care being lost in the flurry of other concerns.
Meanwhile, spirituality and aging has emerged and flourished as a field of study, drawing attention to the spiritual needs of those in later life and the importance of supporting residents’ spiritual resources, religious, or otherwise (Albans & Johnson, 2013; Kimble et al., 1995; MacKinlay, 2021; Nelson-Becker, 2018).
Ontario Legislation
It is clear in the literature that spiritual care is essential to LTC. What is not clear is how to ensure it is being adequately provided. The Residents’ Bill of Rights (Paragraph 23 of section 3 (1) of the Ontario Long-term Care Homes Act, 2007) provides that every resident has the right to pursue cultural, religious and spiritual interests and to be given reasonable assistance by the Home to pursue these interests. Further, the Ontario Long-term Care Homes Act (2007) requires that licensees “provide worship services, resources and non-denominational spiritual counselling” and that “a person who has sufficient knowledge and experience to co-ordinate religious services and spiritual care in a multi-faith setting must be designated to lead the program” (Regulation 79/10, section 85). The Ontario Ministry of Health and LTC's standards and criteria for spiritual and religious program (2007) were not updated, however, since being written in 1993, nor incorporated into the current Act, and one wonders if the benefits of spiritual care found in the literature are actually being realized.
Who Provides Spiritual Care?
Researchers have written about spiritual care needing both generalists and specialists (Bandini et al., 2019; Barton et al., 2003; Jackson et al., 2016). One could say that everything we do in LTC should consider the spirits of residents. Everyone from housekeeping, to nursing, to physiotherapy and activities staff needs general skill in spiritual care, as a compassionate presence in residents’ lives. Clinicians, especially, are increasingly aware of the need to be spiritually competent. To this end, spiritual competence is being assessed among nurses (Keenan & Kirwan, 2018), and training programs offered for clinicians (Bandini et al., 2019; Chen et al., 2020; Dezorzi et al., 2019; Scott Barss, 2020). But clinicians, to say nothing of housekeeping and activities staff, are not specialists in spiritual care and cannot be expected to adequately understand and support residents’ spiritual experience. Eldercare workers around the world are noticing this gap in care. Although support workers in rural Ireland recognize its positive impact on quality of life, they explain that it is not easy to understand their own spirituality, let alone that of persons living with dementia for whom they want to provide holistic care (Keenan & Kirwan, 2018). Meanwhile a study from the Netherlands (van der Vaart & van Oudenaarden, 2018) highlights the importance of existential questions at this stage of life and the need to provide for them, while explaining that personnel have few tools other than listening and referral to a spiritual counselor. An interesting survey of care facility workers in Japan found that although less than 7% claimed any personal religious belief, 71% expressed the desire for more support from Buddhist priests for both residents and staff in residential care (Okamura et al., 2018). Although older adults were shown to highly value the role of nurses and caregivers in fulfilling their spiritual needs and providing spiritual care, these nurses and caregivers themselves perceived arranging a referral to a religious advisor as the main aspect of spiritual care (Gautam et al., 2019).
Of Ontario's acute care hospitals with over 100 beds, 88% provide access to a chaplain (Schmidt, 2013). There is clearly a role for specialists in spiritual care in LTC as well. But not all homes employ a specialist (referred to in this paper as either a spiritual care provider or chaplain). Many administrators instead designate a “lead” from among their recreation staff to be responsible for spiritual care, who then relies on access to community resources.
This is not a situation unique to Ontario but rather echoes the experience of nursing home administrators in other parts of the world who feel responsible for arranging spiritual care for residents but discomfort with their staff's ability to provide it, and so choose to outsource, rather than employ someone with the needed specialist skill set and equip their staff with general spiritual care competency (Morley & Sanford, 2014).
The Study
To address the lack of data on spiritual care provision in Ontario LTC, this study aimed to gather information about how LTC homes in Ontario are providing spiritual care. The aim of the study was to provide that information to the homes and to make recommendations for appropriate staffing and resources to provide creative and accessible spiritual care for all.
Research Question
What is the current state of spiritual care in LTC in three areas (former Local Health Integration Networks or LHINs) in southern Ontario? (and what is the trajectory toward effective, inclusive, and accessible spiritual care into the future?)
- Who is providing it? What skills and training do they bring?
- What is being provided? (What does spiritual care currently look like?)
- What are some best practices that inspire optimum spiritual care provision?
- What are the challenges and opportunities?
This paper will address only the first question, regarding who is providing spiritual care. A second paper will focus on what is being provided, and the challenges, potential, and opportunities for spiritual care going forward.
Study Method
An exploratory quantitative survey methodology (Babbie, 1989; Del Baso & Lewis, 1997; Nelson & Allred, 2005) was used. Ethics clearance was received from the Office of Research Ethics at the University of Waterloo, #40919. The survey consisted of two stages.
First, data were gathered by telephone contact with every LTC home in three areas within southwestern Ontario to ask whether or not their home employs a chaplain/spiritual care provider, and if not, who is responsible for spiritual care/programming in that home.
Lists from the following LHINs, which are currently being phased out, were used:
South West LHIN, an area that is largely rural, with smaller homes (average size of LTC home is 95 beds) Toronto Central, Ontario's most urban LHIN, with larger homes (average size of LTC home is 163 beds) Waterloo Wellington, which combines rural and urban (average size of LTC home is 115 beds).
Each LTC home in these three areas (n = 177) was called and an email address was requested to allow us to invite those responsible for spiritual care to participate in this research. Out of the 177 LTC homes contacted, 164 indicated whether or not a chaplain/Spiritual Care Provider (SCP) was employed (93% response rate), and 109 of these homes gave us email addresses to contact (66 chaplain emails, and 43 email addresses for other team members responsible for spiritual care/programming in homes that don't have a chaplain—a 62% response rate).
In stage 2, an online questionnaire (Babbie, 1989; Del Baso & Lewis, 1997; Nelson & Allred, 2005) was developed and sent directly to the chaplain/spiritual care provider or contact person identified above (n = 109). In addition to the 66 email addresses provided for chaplains/SCPs, surveys were sent to 31 other LTC chaplains who expressed interest in contributing to this research, for a total of 97 surveys sent to SCPs in LTC. 46 surveys were completed and returned (47% response rate). We sent surveys to the 43 email addresses for “others” and received 13 survey responses (30% response rate).
The survey sent to spiritual care providers/chaplains asked questions about:
Consent to participate and for quotes to be used The LTC home served (size, private/not-for-profit/municipal, rural/urban) The person responding (job title, role, hours, experience, age, gender, faith affiliation, education and training, credentials/professional memberships) Qualifications, skills, and aptitudes needed for optimum spiritual care provision Collaboration and reporting relationships with other team members, leadership and volunteers in LTC The Spiritual Care program (what is offered formally/informally, division of time, adequacy) The role of a spiritual care provider/chaplain The purpose or importance of spiritual care in LTC Evidence/outcomes of good spiritual care Effective programs, resources or practices Challenges or obstacles in providing spiritual care in LTC.
The survey concluded with open-ended questions about:
The survey sent to those responsible for spiritual care programming in homes without a chaplain asked similar questions, with some wording slightly altered to acknowledge the difference in their role, and a few additional questions (e.g., What education, training, or experience do you find helpful in your role (of providing spiritual care)? What is your comfort level with providing spiritual care programming?). Data were extracted, calculations completed and themes were identified from responses to the open-ended questions.
Findings
This paper will share basic findings about who is providing spiritual care in Ontario LTC: What portion of homes employ a specialist in spiritual care? Are they salaried, or contract employees? Full or part-time? What education, training, and qualifications do they have? Are there differences between for-profit, not-for-profit, and municipal homes? And finally, who provides spiritual care in homes without a specialist?
Spiritual Care Provision in LTC—The Numbers
Of the LTC homes contacted by telephone, 49% attested to having a SCP (most commonly referred to as “chaplain”) on staff, while 51% said they do not, and prevalence varies between rural/urban and type of home ownership (See Table 1). Not-for-profit (NFP) homes are most likely to have paid spiritual care providers (83%), and for-profit/privately run facilities are least likely (37%), while municipal homes vary substantially between regions. Rural areas seem to have fewer employed spiritual carers than urban. Including only homes with more than 100 LTC beds (n = 84), 59.2% reported employing a spiritual care provider, in contrast to 34.2% of homes with less than 100 beds.
Percentage of Long-Term Care Homes That Employ a Spiritual Care Provider/“Chaplain.”
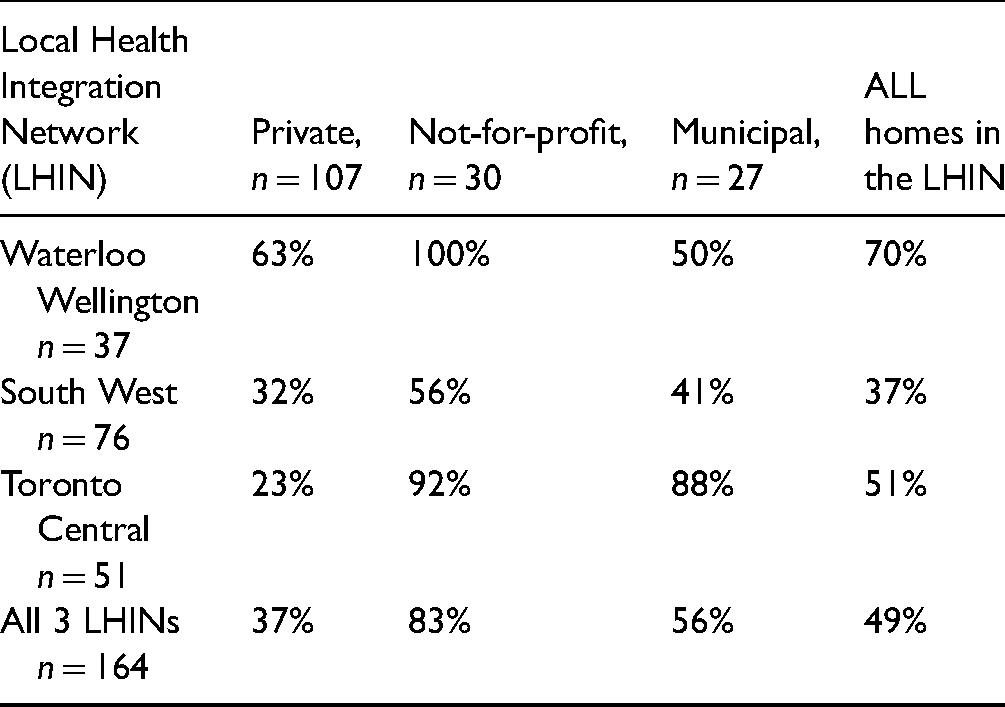
Table 2 shows that most LTC chaplains work part time, though 50% of respondents who work in NFP homes reported full-time hours. Homes surveyed employ a chaplain anywhere from one hour per week to full time (some with more than one paid chaplain). Approximately half of LTC chaplains have other employment, with several being otherwise retired.
Number of Weekly Hours, Wage and Contract/Salaried/Benefits in Homes That Employ a Spiritual Care Provider (49% of Homes).
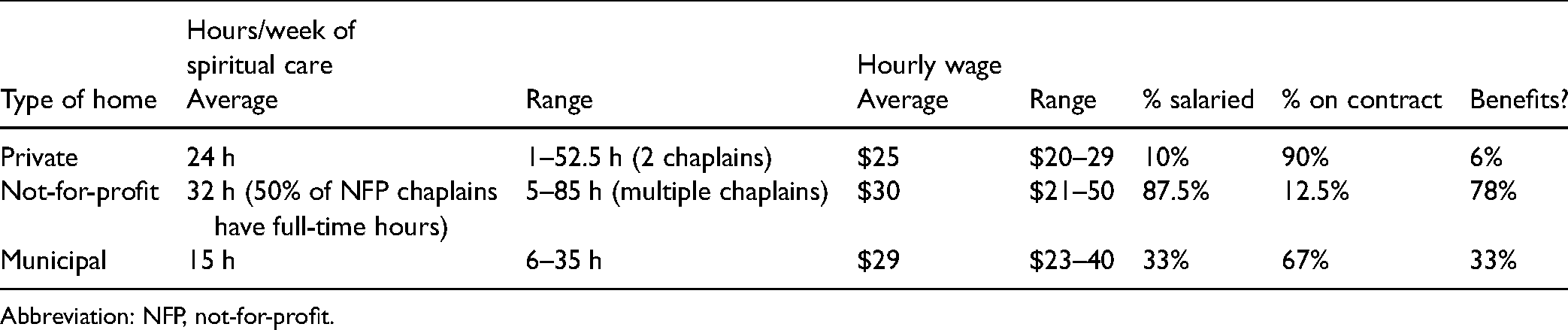
Abbreviation: NFP, not-for-profit.
When the number of chaplaincy hours reported by chaplains in this study was measured against the number of beds in the home they serve, it was calculated that the equivalent of one full-time equivalent (37.5 h) spiritual care provider is responsible for an average of 308 persons in LTC.
Regarding accountability, most SCPs (57%) report to the Recreation/Activity team lead, 20% to the General Manager/Executive Director, and several to both recreation and administration jointly. A few mentioned reporting to leaders in clinical care/nursing. Some are not clear or indicate that this reporting relationship has changed. One SCP expressed the lack of clarity, “[Accountability] is not clear. Mostly to the administrator, at times if feels that everyone would like to be supervisor of the chaplain.” (SCP36)
Who are the Current Spiritual Care Providers in LTC?
In 49% of homes surveyed, there is someone specifically employed to provide spiritual care. Who are these people, and what training and skill do they bring to LTC?
Age and Gender
From 46 responses to surveys sent to SCPs in LTC, we learned that these SCPs range in age from mid-20s to mid-80s (average of 55), and 61% are female.
Faith Affiliation
All but one respondent identified as Christian. That one person indicated that they were baptized Roman Catholic and now have a broad understanding of spirituality and other faiths. Denominational affiliation was remarkably diverse, including at least 15 denominations (out of 43 responses), and spanning Ontario's ecclesiological landscape.
Education, Training, and Experience
Over 85% of the SCPs working in LTC who responded to this survey have a university degree, and over half of these SCPs have a Master’s degree (predominantly theology/divinity), while others are pursuing one.
The Canadian Association for Spiritual Care (CASC) offers professional training for spiritual care providers in “units” of clinical pastoral education (CPE) that combine practical experience with supervision, peer engagement, and academic learning. Each unit represents 400 h of training. Two-thirds of the SCP respondents have one or more units of CPE.
Spiritual Direction is the practice of being with people as they endeavor to deepen their relationship with the divine, or to learn and grow in their own personal spirituality. 20% of survey respondents have completed a two-year training program in spiritual direction.
Chaplains surveyed have pursued sector-specific continuing education/workshops in palliative care (91%), grief (77%), dementia (65%), working with the elderly (58%), mental health (42%), multi-faith training (35%), and other training including music with seniors, advance care conversations, restorative justice, crisis intervention, post-traumatic stress disorder training, trauma care, gentle persuasion, and Stephen Ministry.
Although there is a range (from 1 to 40 years of experience), the chaplains surveyed have been providing spiritual care in some capacity for an average of 18.5 years, with an average of 9.7 years of that in LTC.
Who Provides Spiritual Care in Homes Without a Chaplain?
In homes without SCPs (51% of homes contacted, 13 surveys returned, see Table 1), this study showed that primary responsibility for the spiritual well-being of residents fell to the Director/manager/coordinator of Program/activities/recreation/life enrichment. Those in this role attested to spending from 1 to 4 h weekly (most around 2.5) attending to spiritual care. For some this time is mainly administrative, while for others it is more relational/support oriented. Respondents indicated that they did not seek out this responsibility but rather it was part of their job description, and their comfort and confidence level with the role varied widely. None had training specific to spiritual care, and respondents expressed their reliance on outside, community resources and volunteers, commenting that these are increasingly difficult to find. “I am finding the churches in the community are struggling and are not fully committed or have the time to come to the nursing home as they once were.”(R9) Note that these comments were collected before the pandemic required LTC to stop admitting volunteers.
Some of these homes have social workers and other therapists (music, horticulture, art …). Although recreation staff and nursing staff are perceived by survey respondents to “often” contribute to spiritual care for residents (57% and 40%, respectively), other therapies (25%) and social work (20%) are less often perceived to address spiritual needs.
All of these homes relied on volunteers (local clergy and other community members, family, and sometimes students and/or residents themselves) who provide between 1 and 2 h/week in homes where they only come in to lead worship, and up to 30 h/week in homes where volunteers offer worship, music, visiting, portering, and on-call service. On a continuum scale, those responsible indicated that it is quite difficult to find volunteers, and that they have relied on the same volunteers for years, despite advertising need and reaching out to local church groups. “I find it difficult to network with community churches unless there has already been a long standing community partnership—creating new partnerships is a challenge with churches as most do not return your phone call or inquiry.” (R13)
Discussion
Spiritual Care Provision in LTC—An Optional Extra?
Just under half of the LTC homes this project surveyed employ SCPs. Despite evidence that spiritual care is central to well-being in later life, and policy that requires its provision, spiritual care seems to be seen as an optional extra, rather than an essential investment.
It is illuminating to consider the difference in spiritual care provision between hospitals and LTC. In Ontario hospitals, there was found to be an average of one spiritual care provider for every 160 beds (Schmidt, 2013). Similar to LTC, spiritual care provision in hospitals was found to vary by corporation. For example, one faith-based healthcare organization had an average of 67 beds per full-time equivalent (FTE) and one publicly funded hospital had 600 beds with one FTE. So the average does not tell the whole story. But it does allow comparison with this study that found that the equivalent of one chaplain is responsible for an average of 308 persons in LTC, in homes that employ a spiritual care provider. Remember that 51% of homes contacted did not employ anyone in this capacity at all.
The homes that invest the most in the employment of spiritual care providers appear to be NFP homes that prioritize spiritual care as vital to their identity, in addition to certain NFP or municipal homes where the SCP is part of management and paid accordingly. These homes are dedicating more FTE to spiritual care, better pay, and chaplains are more likely to be salaried rather than contract workers, and provided with benefits.
Urban homes seem more likely to employ SCPs than rural homes. This may, ironically, be a factor of rural areas historically being less secular and having greater access to community clergy and church volunteers to provide services. Trained spiritual care providers are also less available in rural areas. Urban homes are more likely to acknowledge the need for a paid spiritual care provider, having less community support, more beds, and caring for a more diverse population. Into the future it seems unwise for homes, rural or urban, to count on their community for consistent and skilled provision of spiritual care.
The question of where spiritual care “fits” into the organizational and reporting structure of a LTC home is significant. Although in some homes the spiritual care provider is at the table with managers, or reports directly to the General Manager, in other facilities (57%) the SCP reports solely to the activity department, effectively restricting the influence and activity of spiritual care to one aspect (subdivision) of recreation programming. This may be a product of the LTC funding model, where spiritual care fits within the program and support services envelope. 1
Not just faith-based homes but all homes would benefit from spiritual care provision. Although spiritual care has come to be seen, in the LTC sector, as an optional extra, this study contends that it is, in fact, essential, and undergirds all care provided.
Spiritual Care Providers in LTC
Although those who currently serve as SCPs in LTC vary in age, gender, faith perspective, and training, they share the common goal of addressing the needs of the human spirit. SCPs have developed their skill set in a variety of ways, including both education and experience. Some chaplains in LTC, as in decades past, are retired community pastors, while some have specialized in chaplaincy earlier in their careers. Almost all have university degrees and most hold master’s degrees. Chaplains today are increasingly likely to also have training through the CASC in CPE. Some SCPs have completed a spiritually integrated psychotherapy program with placement in LTC which includes multi-faith and multicultural awareness as part of their theological education.
Long-term care is a unique context for spiritual care that requires knowledge and skills that are not necessarily included in academic theological/pastoral training. Whether or not they had this education before they began their position, chaplains emphasize the importance of continuing education opportunity in palliative care, end-of-life issues and advanced care planning, dementia, family systems, conflict mediation, mental health care, and grief counseling. Skill in spiritual care builds with experience (and is often recognized and valued as wisdom).
In addition to being highly educated and skilled, SCPs are people of faith, deeply rooted in compassion, love, and grace, and a solid conviction that each life is valuable and worthy of dignity and respect until the very end. It is important that SCPs embrace a faith tradition themselves, certainly not to proselytize, but to be grounded in values that give them the constitution to support others with more than human capacity. Wherever they find their own spiritual grounding, SCPs have a wealth of knowledge of the resources religious practice provides and the skills to build a relationship and make community connections. Current chaplains are predominantly Christian, and it is expected that as religious diversity grows, so too will diversity among SCPs (Cadge et al., 2019; White et al., 2020).
A well-trained SCP brings expertise in the areas that intimidate many LTC workers who are trained to care for aging bodies or their home environment: family conflict, patience in suffering, the meaning of life, emotions, prayer, confusion, dying, and death. SCPs are equipped to be the nonanxious presence on the roller coaster of later life, for elders and for those around them.
They are also creative and practiced experts in the rituals and routines that make life meaningful, from room blessings to confession and reconciliation, to practices that help acknowledge grief and loss. Competent SCPs who have training and/or experience in all of the above bring a valuable skill set into LTC.
What is Missing in Homes Without a Chaplain?
How dollars are spent is at the discretion of each organization. Those in the LTC sector that provide spiritual care are those whose decision-makers understand and value it (Jackson et al., 2016; McCarroll & Schmidt, 2020). This research showed that without a spiritual care provider, a vital skill set to provide for the well-being of individuals and the organization is missing. Those made responsible for spiritual care/programming in the absence of a chaplain have no training in this area and are often not comfortable with the responsibility, relying heavily on community volunteers for programming and on-call support.
Of course, there will always be a vital role for community connections in supporting spiritual care and programming, especially in rural areas. But the restrictions of the recent pandemic drew our attention to what supports are essential to have integral to the care team, in the absence of family and community presence. During a pandemic, as well as in more “normal” times, strong spiritual care presence provides support for team members, connections for families, opportunity to lift spirits, to express sadness, to mark transitions (honor guard) and for meaning-making through times of uncertainty and loss (Carey et al., 2020).
The changing religious landscape in Ontario makes it especially difficult to provide for spiritual needs without appropriate training. Gone are the days when visiting church services once a week would presumably check off “spiritual needs met” for everyone in the home. Familiarity with a wide variety of faith traditions is now necessary as religious diversity has increased in our society and will continue to increase in LTC as new Canadians grow older (McCarroll & Schmidt, 2020). In addition, the incoming cohort of “baby boomer” residents hopes for care that recognizes their diverse spiritual needs and better supports their individual spiritual resources (Kuepfer, 2019).
Those with responsibility for spiritual care who are not trained spiritual care providers described particular skills that they would value a spiritual care provider to bring to their home:
Understanding of and attention to the spiritual needs of the residents Listening and counseling for residents, families, and staff, as there is “so much to deal with in people's lives these days” (R4) Contributing to end-of-life care conferences and advanced care conversations (bringing specialized skills and knowledge to questions of ethics, and to palliative care) Gathering the community for meaningful moments—planning and/or leading spiritual services, including memorial services. Reducing the reliance on outside resources—taking responsibility for networking with faith communities to facilitate and improve upon the spiritual care they offer. While it is important for the entire LTC team to be competent in general spiritual care, a skilled specialist in spiritual care brings a unique and vital presence and skill set.
Limitations and Future Research
This study is limited by the geographical areas studied and by the self-selection of participants who chose to provide us with detailed information. Although we heard from those directly responsible for spiritual care, follow-up research would be interesting to discover the perspective of residents, families, other team members, and managers.
Conclusion
Spirituality is important to elders and a source of reassurance, growth, and well-being. Research also indicates that spirituality is an important component of palliative care. As many older adults are living their last years in LTC, the Ontario Long-term Care Homes Act (2007) rightly aspires to meet the spiritual needs of residents.
This research, however, indicates an uneven and haphazard use of spiritual care providers in LTC homes in southern Ontario. Currently, more than 50% of LTC homes do not employ anyone with skills or training in spiritual care. In the remaining half, while some homes provide a wonderful example of what spiritual care can offer, spiritual care providers report widely varying hours and remuneration, as well as inconsistent expectations, standards, and sense of being valued and integrated into the circle of care.
As we move into a new era of caring properly for our elders and better supporting those who support them, we must invest in a role and skill set that makes a significant difference in the spirit of LTC communities, and for all the individuals who call them home.
Recommendations
There is a need for consistent employment of spiritual care providers in every LTC home, assuring residents and families that spiritual needs will be met, and that the spirits of team members will be supported.
The LTC sector should aspire to meet a parallel standard to hospital-provided spiritual care, such that the equivalent of one full-time trained spiritual care specialist be provided for every 160 beds, at a wage in keeping with their profession.
Footnotes
Acknowledgments
This research is a collaboration with the Schlegel-UW Research Institute for Aging (RIA), at the University of Waterloo. To learn more about the RIA's work to enhance quality of life and care for older adults: ![]() . The authors are grateful for the research assistance of Peter Kim, Joseph Kim, and Chi-Ping Loreta Sinn.
. The authors are grateful for the research assistance of Peter Kim, Joseph Kim, and Chi-Ping Loreta Sinn.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.