
Abstract
Background:
Prenatal cannabis use is becoming increasingly prevalent throughout the United States. Yet little is known about how motivations for cannabis use vary across maternal sociodemographic characteristics or how motivations are related to frequency of use. We aimed to address these evidence gaps via a comprehensive descriptive analysis of existing surveillance system data.
Methods:
Using data from the 2017–2021 Pregnancy Risk Assessment Monitoring System Marijuana Supplement, we estimated weighted prevalence estimates of self-reported motivations for cannabis use during pregnancy. We examined variations in motivations across sociodemographic characteristics and frequency of use. We also examined write-in responses for motivations for cannabis use.
Findings:
In our sample representing approximately 802,954 live births from 10 U.S. states, the most common motivations for prenatal cannabis use were for mental health reasons (82.81%; 95% confidence interval [CI]: 77.52, 87.06), to relieve gastrointestinal symptoms (77.10%; 95% CI: 70.51, 82.59), to relieve pain during pregnancy (48.67%; 95% CI: 41.84, 55.56), for fun or relaxation (40.18%; 95% CI: 33.69, 47.04), and to relieve symptoms of a chronic condition (26.31%; 95% CI: 20.55, 33.01). Most women (84.32%) reported two or more reasons for use, which was associated with daily or near-daily use. Qualitative analysis of write-in responses identified alleviation of pregnancy-related symptoms (e.g., nausea/vomiting, appetite, sleeplessness) as the most common motivation for use (54.90%).
Conclusions:
Given a growing body of evidence about adverse health outcomes associated with prenatal cannabis use, findings underscore the importance of patient–provider communication and messaging about safe alternatives to cannabis use during pregnancy.
Introduction
Policies regulating cannabis use in the United States (U.S.) have undergone dramatic changes in recent years, with nearly half of states legalizing cannabis for recreational use and 40 states legalizing it for medicinal use. Concurrent with the proliferation of cannabis legalization, cannabis use among pregnant women has also increased in the United States, from 2.4% in 2009 to 16.0% in 2020.1–3 Additionally concerning, both recreational cannabis legalization and medicinal cannabis legalization have been associated with increased rates of perinatal cannabis use.4–8
As cannabis policies evolve in the United States, social norms related to perinatal cannabis use are also shifting. A recent qualitative study of prenatal cannabis use found that following legalization, women perceived easier accessibility, greater trust in cannabis retailers, reduced stigma, more patient–provider discussions about prenatal cannabis use, and greater use of cannabis products. 9 Decreased perceptions of risk have been associated with uncertainty about adverse perinatal outcomes, perceived therapeutic benefits,10–12 and conflicting views on whether cannabis is addictive. 10 In a study of perceived neonatal harms associated with prenatal cannabis use, 31% of women who had ever used cannabis reported the belief that cannabis use during pregnancy was not harmful to the baby. 13
Despite common maternal perceptions that prenatal cannabis use is low-risk, clinical guidelines concur that there is no safe amount of cannabis use during pregnancy.14,15 Indeed, a rapidly growing body of evidence demonstrates that in-utero cannabis exposure is associated with numerous adverse neonatal outcomes, including preterm birth, small for gestational age, and admission to the neonatal intensive care unit.14,16 Further adding to concerns about prenatal cannabis use, contemporary cannabis products are, on average, more than three times as potent as in prior decades.17,18 Indeed, some concentrates in cannabis products have 85 − 95% Δ-9-tetrahydrocannabinol. 19 Given the risks associated with prenatal cannabis use, understanding maternal motivations for use during pregnancy is essential to develop effective interventions.
Evidence about motivations for perinatal cannabis use, however, is limited. Quantitative studies that have examined motivations for prenatal cannabis use have typically used data from the Pregnancy Assessment Monitoring System (PRAMS), which has included optional, supplemental questions on cannabis use since 2017. 20 Prior surveillance data using PRAMS have found that the most reported motivations for prenatal cannabis were for stress management and to alleviate symptoms of nausea or vomiting.21,22 But a detailed analysis, including a more robust exploration of the write-in responses for motivations for cannabis use, was not conducted. Studies using other sources of data to examine motivations for perinatal cannabis have used single-state data, 23 which limits generalizability of findings to a larger sample, or examined motivations for use among breastfeeding women, 24 which limits interpretability of findings to women who use cannabis while pregnant.
Despite this research, evidence gaps remain, particularly around how motivations vary across sociodemographic characteristics and in relation to frequency of use. Further, open-ended responses for motivations reported in PRAMS data have yet to be explored. Given the nature of the PRAMS dataset, including the ability to aggregate data across years and states, it is an ideal source of data to address these evidence gaps. Therefore, our study aimed to (1) describe motivations for cannabis use by sociodemographic characteristics and frequency of use and (2) explore write-in responses to motivations for prenatal cannabis use.
Methods
In this mixed methods study of repeated, cross-sectional survey data, we used data from the 2017–2021 PRAMS, a population-based surveillance system of the Centers for Diseases Control and Prevention (CDC). 20 Participating PRAMS states randomly survey women annually via mail or telephone between 2 and 6 months postpartum about maternal behavior and experience before, during, and after pregnancy. 20 The PRAMS dataset was the optimal data source for this study because of the representativeness of the sample across numerous U.S. states and availability of open-ended qualitative responses about motivations for use not present in other data sources.
Sample
We included states that opted to use the Marijuana Supplement, which was used for the first time in 2017. The Marijuana Supplement collects data on maternal cannabis use, including information about prevalence, motivations for use, and modes of use. We included a total of 10 states that opted to use the Marijuana Supplement in this analysis: Alaska, Illinois, Maine, North Dakota, New Jersey, New Mexico, New York, Pennsylvania, Virginia, and West Virginia.
Motivations for prenatal cannabis use
PRAMS asks respondents whether they used cannabis during their most recent pregnancy. Respondents who reported cannabis use are then asked why they used cannabis (e.g., motivations for use). In addition to a multiple-response categorical variable, respondents who selected they used cannabis prenatally “for some other reason” were able to write in why they used cannabis during their most recent pregnancy. For these qualitative data, we conducted a content analysis 25 of the open-text responses provided for the “some other reason” responses. We first reviewed all responses inductively and generated 36 unique codes to capture the full range of reasons reported (i.e., anxiety, nausea, sleep problems, fibromyalgia, to cut back on cigarette use, partner pressure, religion, post-traumatic stress disorder (PTSD)). We then systematically collapsed these codes into broader parent categories (e.g., medical conditions, mental health conditions, pregnancy-related conditions, other). Two members of the study team independently reviewed responses and discussed discrepancies, which were resolved through consensus. Using Stata 14.1, we documented all coding decisions and category refinements to ensure consistency and transparency.
To examine motivations by frequency of cannabis use, we merged write-in responses with established response categories in the PRAMS Marijuana Supplement codebook when appropriate. When a write-in response aligned with an existing category, it was recoded accordingly (e.g., “PTSD” was recoded as a mental health condition; “to help keep food down” was recoded as a gastrointestinal issue). We assigned write-in responses that did not match a preexisting category to the “other” category.
Frequency of prenatal cannabis use
The PRAMS Marijuana Supplement includes an item that assesses the frequency of cannabis use during the respondent’s most recent pregnancy. Women who reported cannabis use were asked, “During your most recent pregnancy, about how often did you use marijuana products in an average month?” Response options included: daily, 2–6 days per week, 1 day per week, 2 to 3 days per month, 1 day per month or less, and I did not use marijuana then.
Data analysis
PRAMS data are weighted to account for the complex sample design, as well as nonresponse and noncoverage. 20 We calculated weighted prevalence estimates and 95% confidence intervals (CIs) for each motivation for cannabis use. We used Pearson χ2 tests to examine differences in motivations across sociodemographic characteristics (maternal age, race, ethnicity, parity, education, participation in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), and timing of prenatal care initiation), as well as differences in reported frequency of cannabis use. We used Stata 14.1 (StataCorp) for analysis and a two-sided significance threshold of alpha = 0.05.
Results
The final unweighted analytic cohort included 14,308 respondents representing approximately 802,954 live births. In the sample, most women were 18–24 years old (70.31%), non-Hispanic (86.95%), and White (72.60%). Just over half participated in WIC (54.44%), and the majority had a high school diploma, GED, or lower level of education (58.98%) (Table 1). Approximately 9.42% (95 CI: 8.67,10.22) of the sample reported cannabis use in the 3 months prior to or during their most recent pregnancy, with 3.68% (95% CI: 3.22, 4.20) reporting cannabis use while pregnant. Prevalence of self-reported cannabis use varied by year, ranging from 4.19% (95% CI: 3.46, 5.05) in 2017 to 1.30% (95% CI: 0.33, 0.49) in 2021 (p = 0.007).
Demographic Characteristics of the Sample by Motivation for Prenatal Cannabis Use, PRAMS, 2017–2021 (Unweighted N = 14,308, Weighted N = 802,954) a
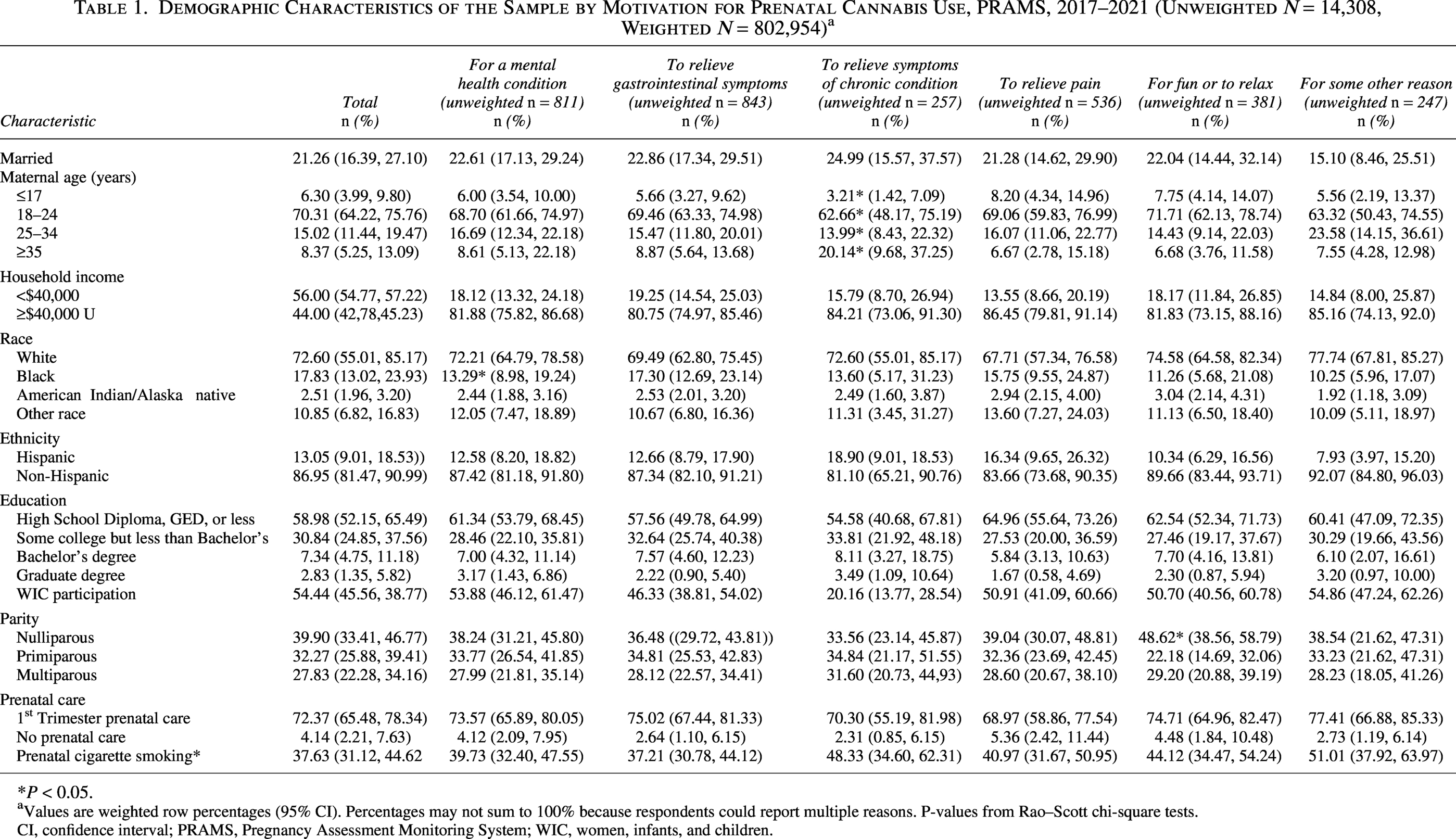
P < 0.05.
Values are weighted row percentages (95% CI). Percentages may not sum to 100% because respondents could report multiple reasons. P-values from Rao–Scott chi-square tests.
CI, confidence interval; PRAMS, Pregnancy Assessment Monitoring System; WIC, women, infants, and children.
Quantitative results for prenatal cannabis use motivations
Cannabis use motivations were broadly similar across sociodemographic groups, with a few exceptions (Table 1). First, older women more frequently reported using cannabis to manage a chronic condition, with 20.14% of women 35 years of age and older reporting this motivation (p = 0.005). Second, nulliparous women were more likely to report using cannabis for fun compared with
Among women reporting prenatal cannabis use, motivations for use varied (Table 2). Most women reported using cannabis for mental health reasons (82.81%, 95% CI: 77.52, 87.06), followed by gastrointestinal symptoms (77.10%, 95% CI: 70.51, 82.59), to relieve pain during pregnancy (48.67%, 95% CI: 41.84, 55.56), for fun or relaxation (40.18%, 95% CI: 33.69, 47.04), for other reasons (26.31%, 95% CI: 20.55, 33.01), and to manage chronic conditions (20.62%, 95% CI: 15.79, 26.47). Women who used cannabis for mental health reasons cited more frequent use, with 28.97% reporting daily use (95% CI: 22.56, 36.34; p = 0.056). Similarly, women who reported using cannabis to help with gastrointestinal symptoms more frequently reported daily or nearly daily use (daily: 28.44%, 95% CI: 22.19, 35.65; near daily: 25.32%, 95% CI: 19.53, 32.14).

Raw n with weighted proportions.
among respondents who reported any prenatal cannabis use.
categories are not mutually exclusive.
CI, confidence interval; PRAMS, Pregnancy Assessment Monitoring System.
Table 2 also displays the number of motivations for cannabis use during pregnancy by frequency of use. Approximately 84.32% (95% CI: 78.09, 89.03) of respondents reported two or more reasons for using cannabis during their most recent pregnancy. Women who reported two or more reasons for use more frequently reported daily use compared with those who reported a single motivation for use (86.96% and 10.40%, respectively).
Qualitative results for prenatal cannabis use motivations
Table 3 reports frequencies of codes for write-in motivation responses. Of those who selected “other,” 240 respondents provided write-in responses, which varied from a single word to a full sentence. Approximately 8.75% of women indicated they were unaware of their pregnancy and stopped using cannabis upon becoming aware of their pregnancy. Over half of write-in responses (54.90%) indicated that cannabis was used for a pregnancy-related symptom, including for gastrointestinal symptoms (e.g., acid reflux, nausea, or hyperemesis), sleep problems, or appetite (e.g., to stimulate appetite or help to gain weight). About one in four women indicated they used cannabis for a mental health condition (e.g., trauma, mood swings, coping, Attention-Deficit/Hyperactivity Disorder (ADHD)). In addition, 1.25% of write-in responses indicated the respondent was addicted to cannabis, and another 1.25% reported using cannabis as a substitution for another drug (i.e., opiate, tobacco).
Qualitative Write-in Reasons for Cannabis Use during Pregnancya (Unweighted n = 240; Population Size: 7,421.30)

among those who reported “other reason for use only.”
unweighted n with weighted porportions.
included respondents who stated they substituted cannabis for any opiates, meth, or cigarettes.
Discussion
In this mixed methods study using repeated cross-sectional data from 10 U.S. states, we examined motivations for cannabis use during pregnancy. Among quantitative data, most women reported using cannabis for mental health reasons (82.81%), with management of a chronic condition being the least commonly reported motivation (20.62%). Women who reported using cannabis for mental health conditions or to relieve gastrointestinal symptoms tended to report more frequent cannabis use, whereas those citing use for fun or to relieve pain or chronic condition management had more varied use patterns. Interestingly, 84.32% of women reported two or more motivations for using cannabis while pregnant, suggesting that interventions to address cannabis use may require interdisciplinary expertise (i.e., primary care providers for chronic conditions, maternity care providers for pregnancy-related conditions, and mental health providers for mental health conditions).
Despite ongoing recommendations to abstain from cannabis use during pregnancy, our qualitative results indicated that women are using cannabis to treat a wide variety of physical, mental, and pregnancy-related conditions. These findings are consistent with prior qualitative research indicating that women use cannabis during pregnancy for coping, 26 stress management, 27 self-medication for mental health or physical conditions,27,28 addiction, 28 and treatment of pregnancy-related symptoms. 28
Treatment of gastrointestinal symptoms was a commonly reported motivation in both our quantitative and qualitative results. These findings are aligned with prior evidence demonstrating that women who report nausea and vomiting during pregnancy are more likely to use cannabis than those without prenatal nausea and vomiting.2,22 Women who reported using cannabis for gastrointestinal-related issues (i.e., nausea, vomiting, hyperemesis, acid reflux, or to stimulate appetite) were more likely to report daily or near-daily cannabis use. This finding is consistent with a prior study, though small, which found that women who reported cannabis use to help with nausea or morning sickness were 12 times as likely to report past 30-day use in comparison with those who did not report this motivation. 23 Therefore, future research should examine pregnant women with gastrointestinal symptoms who use cannabis, as strong evidence demonstrates that using cannabis during pregnancy can exacerbate existing gastrointestinal symptoms and may lead to the development of Cannabinoid Hyperemesis Syndrome.29,30 Furthermore, it is well established that physiological and hormonal changes during pregnancy can cause gastrointestinal symptoms, for which numerous effective treatments with known safety data exist.
We found that women who reported more than one motivation for cannabis use while pregnant had a higher frequency of cannabis use. Blair et al. recently examined the number of motivations for prenatal cannabis use among a small sample of women (n = 59) who reported cannabis use during their pregnancy and found that women who endorsed 5 or more motivations were over 10 times as likely to report past 30-day cannabis use. 23 Similarly, a recent examination of women who used cannabis while breastfeeding found that use of cannabis for multiple reasons continues into the postpartum period, with approximately 19%, 26%, and 19% of respondents reporting two, three, or four motivations for cannabis use. 24 Therefore, our findings, in combination with existing evidence, suggest a need for comprehensive interventions to address misinformation about “benefits” of cannabis use during pregnancy and into the postpartum period.
The American College of Obstetricians and Gynecologists (ACOG) recently updated their 2017 clinical consensus, which discouraged cannabis use during pregnancy and lactation, to state there is no medical indication for cannabis use during pregnancy. 14 The 2025 ACOG guideline acknowledges the paucity of evidence on the safety of medicinal cannabis use during pregnancy. 14 In an effort to counteract increasing rates of cannabis use during pregnancy, it is important that prenatal care providers discuss safe, effective treatments for preexisting and pregnancy-related conditions with the goal of cannabis cessation or reduction in use.
This study draws attention to limitations of current surveillance data on cannabis use during pregnancy. A major limitation of existing surveillance data is the inability to adequately capture motivations for cannabis use during pregnancy, which are multifaceted. For example, response options to the motivations for cannabis use question in the PRAMS Marijuana Supplement grouped stress and anxiety together instead of examining specific mental health conditions separately. Furthermore, current surveillance systems are unable to determine whether women are using cannabis for conditions or symptoms that commonly occur during pregnancy (i.e., nausea and vomiting, lack of appetite, pregnancy-related pain) or chronic conditions (e.g., back pain, migraine, fibromyalgia). In the PRAMS Marijuana Supplement, specifically, response options do not permit an examination of the duration of conditions being treated with cannabis (i.e., before pregnancy, during pregnancy, or both) and whether use is occurring during the entire pregnancy or a specific gestational timeframe (i.e., only during first trimester to treat morning sickness). Issues with validity of categorical response options, in combination with an inability to decipher motivations for use in relation to pregnancy, limit both analytical approach and potential implications of results. In order to advance the field, it is imperative that future surveillance and research address these limitations.
Although study findings contribute novel evidence about motivations for cannabis use during pregnancy, it is important that our findings be interpreted within the context of several limitations. First, many respondents reported multiple reasons for cannabis use. Based on the wording of the PRAMS Marijuana Supplement, we were unable to distinguish which motivations were primary or most salient. Future studies should include questions that ask specifically about primary reasons for use. In addition, it was not possible to distinguish which reasons were specific to the pregnancy period versus those that reflected longer-term or preexisting patterns of use. It is important that future research address this limitation, as understanding motivations for prenatal cannabis use among those who were using prior to pregnancy is necessary to develop effective interventions. Second, although we examined the association between motivations for use and frequency of use, we were unable to determine the duration of cannabis consumption at the reported frequency levels. This limitation is particularly important given that many respondents reported using cannabis for multiple indications simultaneously. In turn, it is not possible to make certain conclusions about frequency patterns by motivations; thus, future research is needed in this area.
Our findings have implications for the development of future surveillance efforts measuring prenatal cannabis use. First, future surveillance efforts and surveys should be psychometrically tested to ensure validity and provide respondents with opportunities to be more specific about motivations for use during pregnancy in alignment with those reasons identified in this study. For example, respondents should be able to report, with specificity, the condition(s) being treated, and whether they have a medical cannabis card for the stated condition. Secondly, future questionnaires should include items about whether women are using cannabis to self-treat existing chronic conditions or pregnancy-related symptoms. Third, future surveys should include questions about whether prenatal cannabis use is a continuation of preconception cannabis use or whether it is a new behavior undertaken to treat symptoms associated with pregnancy. Lastly, in addition to addressing the noted limitation of current surveillance data, it is imperative that future research examines motivations for cannabis use, including motivations before, during, and after pregnancy. This additional research is needed to create effective messaging for patients, to educate clinicians about how to provide appropriate patient care, and to develop targeted cessation interventions during pregnancy that are effective.
Conclusion
Using national surveillance system data across multiple years, we examined motivations for cannabis use during pregnancy. Although the most frequently reported motivation for cannabis use during pregnancy was for mental health reasons, women also reported using cannabis for pregnancy-related symptoms and chronic health conditions, with a substantial portion citing multiple reasons for use. These findings underscore the complexity of motivating factors for prenatal cannabis use while simultaneously highlighting the need for nuanced patient-centered interventions prior to and during pregnancy. Although current surveillance systems provide a strong foundation in this area, additional research using improved surveillance is needed to address evidence gaps and inform effective clinical counseling, public health messaging, and patient-centered interventions.
Authors’ Contributions
K.S.: Conceptualization, methodology, project administration, data curation, formal analysis, writing—original draft, funding acquisition. S.I.: Conceptualization, methodology, project administration, writing—review and editing. S.B.-N.: Writing—review and editing, funding acquisition.
Footnotes
Acknowledgments
The authors thank the PRAMS Working Group, which includes the PRAMS Team, Division of Reproductive Health, CDC, and the following PRAMS sites for their role in conducting PRAMS surveillance and allowing the use of their data: PRAMS Alaska, PRAMS Illinois, PRAMS Maine, PRAMS North Dakota, PRAMS New Jersey, PRAMS New Mexico, PRAMS New York, PRAMS Pennsylvania, PRAMS Virginia, and PRAMS West Virginia.
Author Disclosure Statement
The authors have no conflicts of interest to disclose. Financial Disclosure: The authors have no financial relationships relevant to this article to disclose.
Funding Information
The Health Resources and Services Administration (HRSA), Department of Health and Human Services (HHS), provided financial support for this study. The award provided 100% of total costs and totaled $118,943.00. The contents are those of the authors. They may not reflect the policies of HRSA, HHS, or the U.S. Government.