
Abstract
Currently there are no validated pediatric feeding assessment tools available in Puerto Rican (PR) Spanish. This study aimed to (1) translate and culturally adapt the Pediatric Eating Assessment Tool (PediEAT) for use with PR Spanish speakers, (2) test the internal consistency of the adapted version, and (3) administer the translated and adapted PediEAT to a PR cohort and compare those results with age-matched toddlers in the mainland United States (US). We hypothesized that we would be able to effectively translate PediEAT into PR Spanish with high internal consistency and that infants in the PR cohort would have more parent-reported problematic feeding behaviors compared to the mainland US sample. The translated and culturally adapted PR Spanish PediEAT version was administered to 15 caregiver-toddler dyads in PR and the test demonstrated high internal consistency (α = 0.869). The mainland US cohort reported significantly higher PediEAT ratings of feeding difficulty than the PR cohort in the Selective/Restrictive Eating subscale (p = 0.031). This outcome may be attributed to cultural factors that are different in the PR community compared to the mainland. Future research is needed to explore these differences in more detail with a larger sample size.
Purpose
Successful feeding in infants and children requires efficient interactions among the nervous system, gastrointestinal tract, cardiorespiratory system, and oropharyngeal structures (Arvedson et al., 2019). A pediatric feeding disorder (PFD) can result when any of these components are compromised. PFDs are on the rise and highly prevalent in clinical populations (Kovacic et al., 2021). A PFD, as defined within the International Classification of Functioning, Disability, and Health framework, is “impaired oral intake that is not age-appropriate, and is associated with medical, nutritional, feeding skill, and/or psychosocial dysfunction” (Goday et al., 2019, p. 125). It is crucial to address PFDs, as they can result in significant medical (Imdad et al., 2023), quality of life (Simione et al., 2023), and economic consequences (Okada et al., 2022). Additionally, emerging research indicates that early sucking and feeding difficulties may be a biomarker for poor neurodevelopmental trajectories in cognitive, motor, and language outcomes (Adams-Chapman et al., 2013; Martens et al., 2024; Wolthuis-Stigter et al., 2017).
Pediatric feeding and access to feeding resources can be negatively impacted by national emergencies such as natural disasters, conflicts, and epidemics (O’Connor et al., 2001; Piovanetti et al., 2022; Santaballa Mora, 2018). Since 2017, there has been an onslaught of natural disasters to Puerto Rico, including Hurricanes Irma and Maria (Abbasi, 2018) and several earthquake clusters in late 2019 and early 2020 (Torres et al., 2022). These national emergencies resulted in enormous economic, infrastructural, and societal damage (RAND Corporation, 2020). These disasters have immense medical and psychological impacts on the Puerto Rican residents who do not have the same access to the diverse and robust healthcare systems that are present on the Unites States (US) mainland (Roberts & Song, 2022). For example, Puerto Rico receives the lowest amount of Medicaid funds per resident compared with every other state in the US due to disproportionate allocation of healthcare funds from the Federal Government (Colón & Sánchez-Cesareo, 2016). Thus, residents of Puerto Rico are subject to an inadequate healthcare system that may fail to meet population needs (Lafarga Previdi & Vélez Vega, 2020). All these factors can negatively impact pediatric populations in need of feeding assessment and treatment services in Puerto Rico.
The occurrence of the Zika virus epidemic in Puerto Rico from January 2016 to December 2017 further compounded feeding challenges, as it placed infants born during that time at an increased risk for PFDs. This is because the Zika virus infection during pregnancy can cause severe birth defects in infants, known as Congenital Zika Syndrome (CZS). A common and primary phenotype of CZS is congenital microcephaly (Schuler-Faccini et al., 2016). However, CZS involves a broad spectrum of clinical features that include developmental delays, ocular abnormalities, and symptoms of sensorimotor dysfunction in tone, posture, and movement (Centers for Disease Control and Prevention [CDC], 2022; Leal et al., 2017). The neural damage observed in CZS can lead to symptoms of dysphagia, or disordered swallowing, commonly seen in pediatric neurologic disorders. These symptoms include a weak and uncoordinated oral motor and pharyngeal function, sensory deficits, muscle tone differences, and inappropriate reflexes (Arvedson et al., 2019). Leal et al. (2017) investigated dysphagia characteristics in nine infants with CZS and reported that these infants demonstrated abnormal posturing and oropharyngeal deficits of incomplete lip closure, lingual incoordination, restricted jaw opening, decreased pharyngeal sensitivity, and delayed initiation of the swallow, which resulted in premature spillage of the bolus, post-swallow oropharyngeal residue, and silent aspiration.
Because natural disasters can negatively impact pediatric feeding (Santaballa Mora, 2018) and CZS can lead to severe dysphagia (Leal et al., 2017), it is paramount that areas affected by such epidemics, like Puerto Rico, have assessment tools that can accurately and reliably evaluate feeding performance in a culturally appropriate way. Evidence-based assessment is a critical prerequisite for children to receive treatment services to remediate PFDs and its consequences. Many diagnostic tools are available to assess feeding behaviors in pediatric populations and these tools vary in quality, length, age range, focus on skill vs. behavioral concerns, and psychometric properties (Heckathron et al., 2016). Most screeners for PFDs utilize caregiver reports of feeding behaviors (Jaafar et al., 2019). Although some tools have been used to analyze the diets and eating behaviors of Puerto Rican populations (Graulau et al., 2019; López-Cepero et al., 2021; Mattei et al., 2019; Preston et al., 2011), these do not specifically measure problematic feeding behaviors in infants and children. Thus, there is a need for an assessment tool that measures problematic feeding in infants and young children that is specific to the Puerto Rican language and culture. One such tool that would be valuable if translated to Puerto Rican Spanish is the Pediatric Eating Assessment Tool (PediEAT).
The PediEAT measures symptoms of problematic feeding in children ages six months to seven years via caregiver report. This tool assesses physiologic, behavioral, and mealtime aspects of feeding difficulties in young children. Content validation for the PediEAT's items’ clarity and relevance on pediatric eating behaviors has been established (Thoyre et al., 2014). Furthermore, the PediEAT has age-based scoring norms (Pados et al., 2018) and has demonstrated high internal consistency, construct validity, and temporal stability (Thoyre et al., 2018). This tool can be particularly useful in evaluating feeding skills during the six-to-18-month age range, as that is a critical time for children to learn new oral and motor skills and when they are introduced to new and more complex foods (Arvedson et al., 2019). Although the original English version of the PediEAT has been translated in Spanish, the Spanish version has yet to be assessed for its validity and reliability. Additionally, it would be important to establish a Puerto Rican Spanish version of the PediEAT because there are dialectical subtleties that make the language unique to the island's history (Beardsley, 2004; Nieves-Squires, 1998).
The aims of this study were to (1) translate and culturally adapt the PediEAT for use with Puerto Rican Spanish speakers, (2) test the internal consistency of the adapted version, and (3) administer the translated and adapted PediEAT to a Puerto Rican cohort and compare those results with age-matched infants in the mainland US. We hypothesized that the translation and cultural adaptation of the English version of the PediEAT to Puerto Rican Spanish would demonstrate acceptable internal consistency. Furthermore, we hypothesized that infants in the Puerto Rican cohort would have more parent-reported problematic feeding behaviors compared to the mainland US sample due to the negative effects that national emergencies, epidemics and pandemics can have on feeding development and performance.
Methods
This study used a cross-sectional research design. Caregivers provided written informed consent on behalf of themselves and the children they provide care for. A caregiver is operationally defined as an individual who provides instrumental and emotional support to a person requiring assistance due to young age, aging, disability, or other functional limits (e.g., parent, grandparent). The study was approved by the authors’ Institutional Review Board (NO: #18-09-10). All methods and procedures were carried out in accordance with the approved protocol's guidelines and regulations.
Sample and Data Collection
Participants were recruited from the International Cohort Study of Zika in Infants and Pregnancy in the Karst Region, Puerto Rico (ZIP-PR Karst study; Lebov et al., 2019) and the Center for Research on Early Childhood Exposure and Development (CRECE; Manjourides et al., 2020) in Puerto Rico. Exclusionary criteria for the ZIP-PR Karst Study were pregnant women who were equal to or greater than 18 weeks’ gestation at the time of recruitment, younger than 15-years-old, planned to deliver at a hospital different from a study designated hospital, and women who couldn’t adhere to ZIP-PR testing schedules or who were involved in other Zika research studies. Inclusionary criteria for the CRECE cohort were pregnant mothers before 20 weeks’ gestation, residence in the Northern Karst aquifer region, no contraceptives within three months pre-pregnancy, no in-vitro fertilization, and no major pre-existing medical conditions. Participants in the ZIP-PR and CRECE project were all Puerto Rican citizens and Spanish speaking. Mothers in these cohorts consented to be contacted about future research studies and those with children near or at 24 months of age were contacted and asked to participate in this study. Children near or at 24 months of age were also recruited from mainland US using Qualtrics respondent panels. These respondents were from across the US and all data were collected using a web-based survey platform (Qualtrics, Provo, Utah). Exclusionary criteria for children in this study were premature birth (< 37 weeks gestational age), food allergy, congenital anomaly, genetic syndromes, seizure disorder, autism spectrum disorder, developmental or speech delay, diagnosed feeding problem, or not having an age-matched control (i.e., to the exact month of age) in the other cohort. Data from both Puerto Rican and mainland US cohorts were collected between September 2020 and September 2021.
Pediatric Eating Assessment Tool
Caregivers completed the PediEAT, which required them to observe and rate a wide range of feeding behaviors to indicate whether their child exhibits difficulties in a specific feeding behavior. This tool includes 78 items separated into four subscales: Physiologic Symptoms, Problematic Mealtime Behaviors, Selective/Restrictive Eating, and Oral Processing. Each question uses a six-point Likert scale with responses ranging from “Never” to “Always.” Subscale scores were summed to generate a Total Score, per the tool's scoring instructions. The mainland US participants completed the original English version of the PediEAT and the Puerto Rican cohort completed our translated, culturally adapted Puerto Rican Spanish version of the PediEAT.
Translation and Cross-Cultural Adaptation
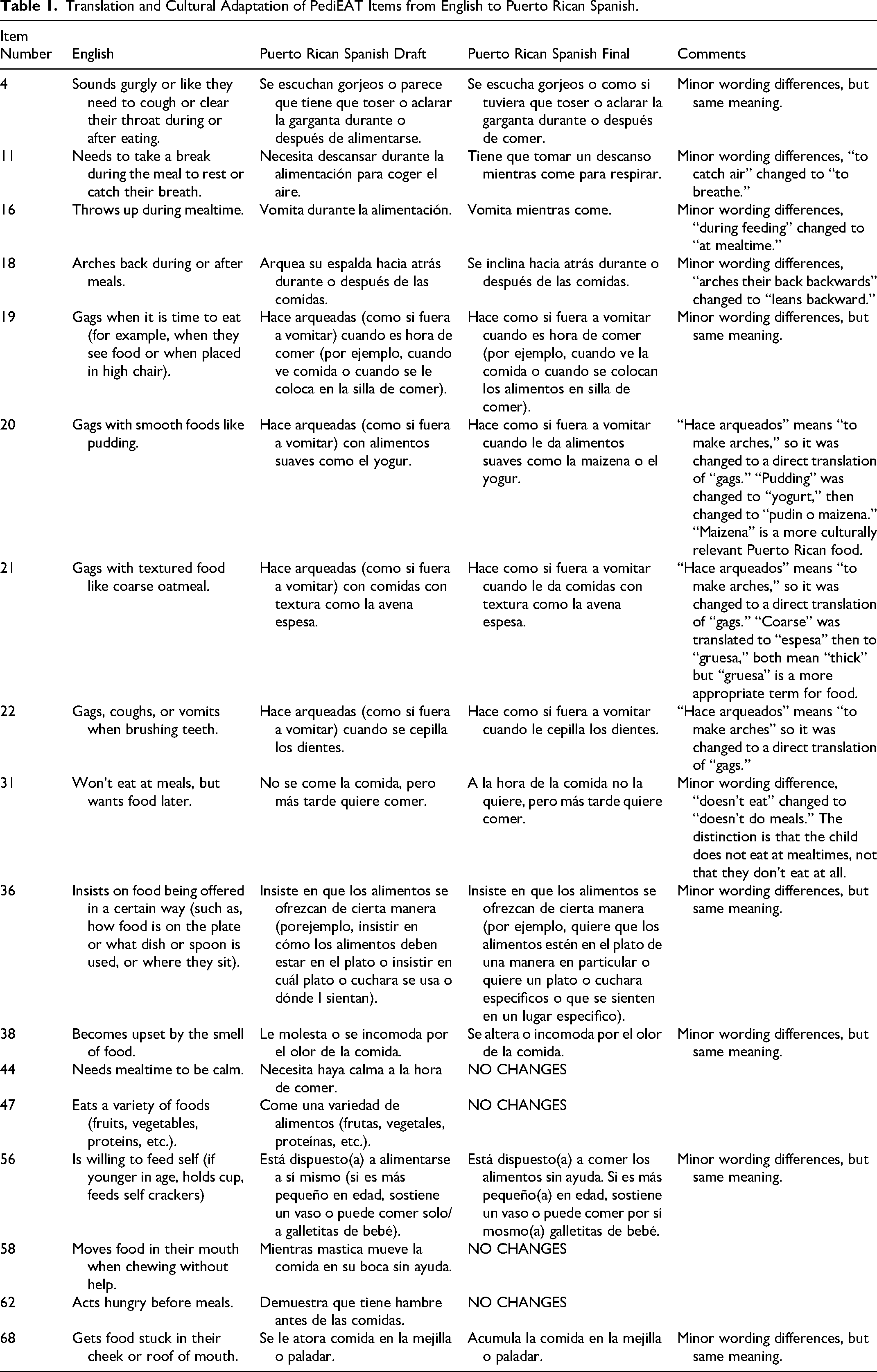
We initially translated the English version of the PediEAT word-for-word into Puerto Rican Spanish using Google translate, which translation is represented in the “Puerto Rican Spanish Draft” column in Table 1. In this process, we opted to use the original English tool as the starting point rather than creating a translation from the existing Spanish PediEAT because, as previously mentioned, that version has not been tested for validity or reliability. In our study, 61 of the 78 questions (78%) were directly translated from English to Puerto Rican Spanish and retained their original meaning. However, 17 questions included phrases or words used in the English PediEAT that could not be directly translated to Puerto Rican Spanish, and therefore were modified for accurate cultural adaptation of the tool (“Puerto Rican Spanish Final” column in Table 1). These translative and adaptive edits were completed by a native Puerto Rican Spanish speaker who is a pediatrician in Puerto Rico and well-versed in medical translations. Our native Puerto Rican Spanish translator initially provided a conceptual translation of each item, and every effort was made to address cultural sensitivity and provide language that is semantically appropriate to the dialect of Spanish spoken in Puerto Rico. These translative and adaptive changes were completed due to minor wording differences, words that are used differently in Puerto Rico, and food items that are not culturally relevant or that Puerto Rican children would have less exposure to compared to children in the mainland US.
Translation and Cultural Adaptation of PediEAT Items from English to Puerto Rican Spanish.
Data Analysis
Descriptive statistics were completed on participant demographics for children's birth weight, age of testing, and race and ethnicity and caregiver's marital status and education. Independent samples t-tests were performed on the parametric comparisons (scaled demographic child variables of birth weight and age of testing between Puerto Rican and mainland US cohorts) and Mann-Whitney U Tests were completed for non-parametric comparisons. Alpha level of significance for participant demographics between groups was set at 0.05.
To evaluate the internal consistency of the Puerto Rican Spanish version of the PediEAT, the Cronbach's alpha was completed on the Total Scores of the Puerto Rican cohort. The Cronbach's alpha is a coefficient of reliability to measure the internal consistency of a test by examining the inter-relatedness of test items. Acceptable scores are generally considered to be between 0.70–0.90, as scores below 0.70 indicate heterogeneity and poor inter-relatedness of test items and scores above 0.90 can suggest redundancies in the test items (Tavakol & Dennick, 2011). Missing responses (four in total) in the Puerto Rican Spanish version of the PediEAT were imputed as the average response for that item from the 14 other participants.
Shapiro-Wilk tests indicated that the PediEAT scores were normally distributed among cohorts. Between groups t-tests were completed to compare means of PediEAT independently for each of the subscales and Total Score between the Puerto Rican and mainland US groups. Two-tailed alpha level of significance was set at 0.05.
Results
Participant Characteristics
Child and caregiver demographics for each cohort are presented in Table 2. Thirty caregiver-toddler dyads were included in this study, with 15 dyads in each cohort. All respondents from the mainland US cohort identified as the child's mother, whereas 12 respondents in the Puerto Rico cohort identified as the child's mother, two as the father, and one as a grandparent. Toddlers (46.67% male) were all between the ages of 23 and 31 months. There was a significantly higher number of White and not Hispanic or Latino toddlers in the mainland US cohort than the Puerto Rican cohort (p < 0.001) and more mainland US caregivers were married than Puerto Rican caregivers (p < 0.001). No other statistically significant differences were found among toddler and caregiver demographics between cohorts.
Participant Characteristics.
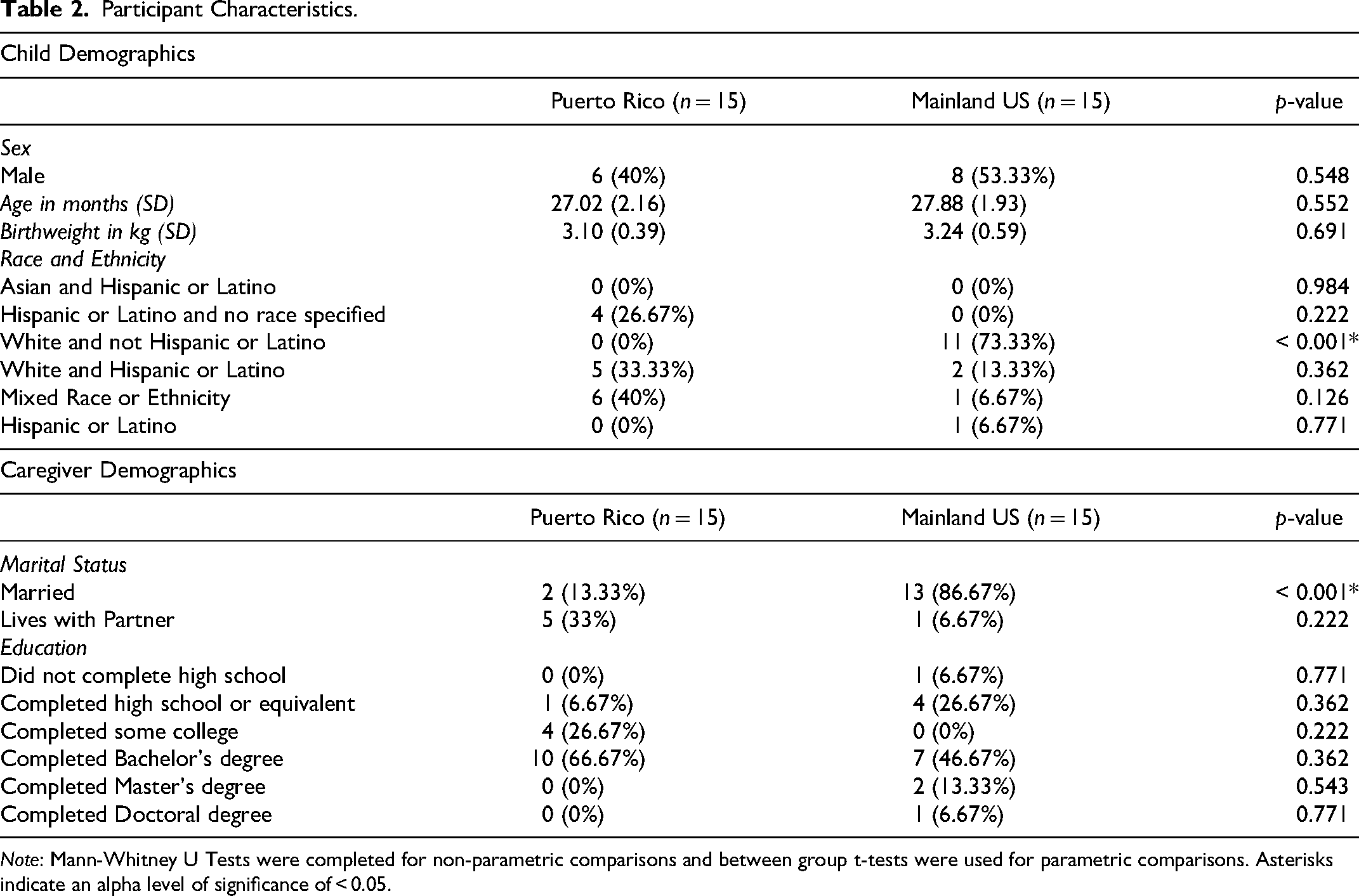
Note: Mann-Whitney U Tests were completed for non-parametric comparisons and between group t-tests were used for parametric comparisons. Asterisks indicate an alpha level of significance of < 0.05.
Internal Consistency of the Puerto Rican Spanish Version of the PediEAT
The Total Score of the Puerto Rican Spanish version of the PediEAT consisted of 78 items; however, only 60 items were included in the Cronbach's alpha test due to 18 items having the same score across the 15 participants. Test items that have zero variance among responses provide no information about individual differences for measures of reliability and thus were excluded. These instances of zero variance in test items were related to the cohort not demonstrating severe or specific symptoms of dysphagia, which is likely attributed to this cohort not being known representations of clinical populations. In support of our research hypothesis, the internal consistency for the 60 items of the PediEAT Puerto Rican Spanish version was high (α = 0.886). These results indicate that the Puerto Rican Spanish version of the PediEAT is a reliable tool to measure problematic feeding behaviors in young children among Puerto Rican Spanish speakers.
PediEAT Scores Between Puerto Rican and US Mainland Cohort
Descriptive statistics and results from the between groups t-tests are shown in Table 3. Contrary to the research hypothesis, the mainland US cohort had significantly higher mean ratings on the Selective/Restrictive Eating subscale (M = 14.33, SD = 8.11) than the Puerto Rican cohort (M = 8.89, SD = 7.22), t(14) = −2.39, p = 0.031. Results indicate that the mainland US cohort reported more problematic feeding behaviors related to selective and restrictive eating. No significant differences were observed on mean ratings of the Physiologic Symptoms, Problematic Mealtime Behaviors, and Oral Processing subscales or Total Score between Puerto Rican and mainland US groups.
PediEAT Subscale and Total Score Results between Puerto Rican and US Cohorts.
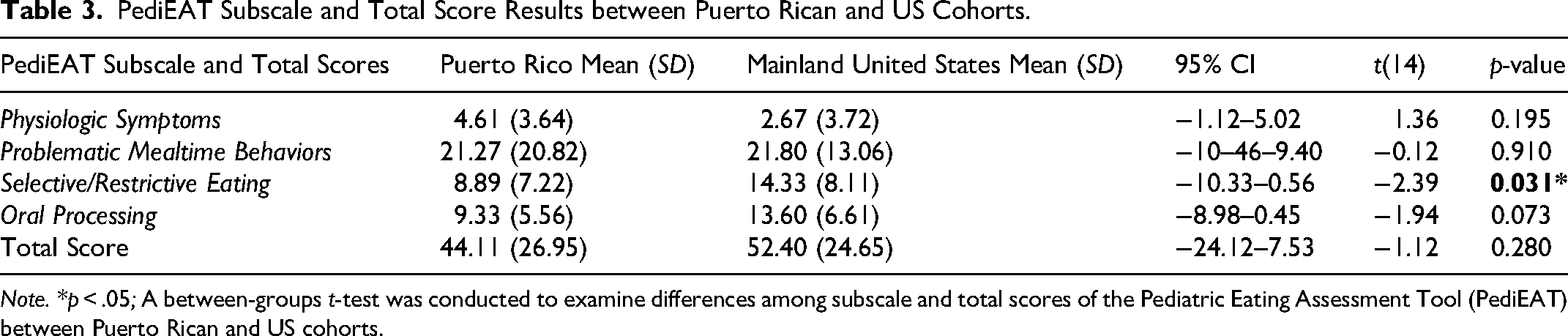
Note. *p < .05; A between-groups t-test was conducted to examine differences among subscale and total scores of the Pediatric Eating Assessment Tool (PediEAT) between Puerto Rican and US cohorts.
Discussion
This study translated and culturally adapted the English version of the PediEAT to Puerto Rican Spanish and examined its internal consistency in a small cohort of caregiver-toddler dyads in Puerto Rico. This is the first time that a valid, parent-report feeding assessment has been adapted to Puerto Rican Spanish. The Puerto Rican Spanish version of the PediEAT is aimed to be used in a different language, culture, and territory than its original English version. Translating healthcare resources into multiple languages can improve accessibility and the quality of healthcare (Squires, 2018), but their mere translation is not sufficient for them to be used effectively in each linguistic population because “word for word” translation often lacks adapting the resource within a specific cultural context (Sousa & Rojjanasrirat, 2011). For a feeding evaluation resource, it is critical that caregivers understand what is being asked and have familiarity in their own cultural context with the foods that may be included in a feeding assessment scale, as certain foods may be of higher relevance to populations and cultures (Ikeda et al., 2002). These factors are why both translation and cultural adaption of the PediEAT was necessary and were systematically completed by a bilingual, native, and Puerto Rican medical doctor.
The high internal consistency demonstrated by the Total Score of the Puerto Rican Spanish version of the PediEAT indicates it is a reliable measure of PFD constructs. Reliability and validity aspects of the Puerto Rican Spanish version of the PediEAT are positively influenced by the English version's content validation and psychometric properties. The English PediEAT version completed content validation among researchers, clinicians, and parents (Thoyre et al., 2014), has excellent test-retest reliability, and demonstrated construct validity by highly correlating with the Mealtime Behavior Questionnaire and known-groups validity by PediEAT scores being significantly different among children with and without a PFD (Thoyre et al., 2018).
Contrary to our research hypothesis, the Puerto Rican cohort did not have higher ratings of feeding challenges in any of the PediEAT subscales or the Total Score compared to the mainland US cohort. Conversely, on average, the mainland US cohort had significantly higher ratings of feeding difficulty than the Puerto Rican cohort in the Selective/Restrictive Eating subscale, which captures a child's feeding performance of accepting and eating foods with different textures and temperatures. Despite these groups significantly differing on a PediEAT subscale, it is important to note that the average ratings for all PediEAT scores for both Puerto Rican and mainland US cohorts were typical to norm-references for children aged 24–30 months (Pados et al., 2018). Although neither group's scores are representative of children with PFDs, the higher incidence of feeding difficulty in the Selective/Restrictive Eating subscale in the US cohort is interesting and could be attributed to several factors.
One possible factor may be the context in which our data were collected between these two cohorts. Our data from the Puerto Rican cohort were collected during the COVID-19 pandemic on toddlers who were born during the Zika virus epidemic. Our data from the mainland US were collected during the COVID-19 pandemic but not in the context of Zika and post-devastating natural disasters. For both cohorts, COVID-19 likely played a pivotal role.
It is well documented that the COVID-19 pandemic had a negative impact on mental health, caregiver-child bonding, child development, and feeding practices (de Araújo et al., 2021; Liu et al., 2022; Rodgers et al., 2023; Vindegaard & Benros, 2020), and these outcomes could be exacerbated if families’ financial needs were not met (Russell et al., 2020). The COVID-19 pandemic negatively impacted psychological well-being in the general public and was associated with a rise in stress, anxiety, and depression (Vindegaard & Benros, 2020). These mental health consequences affected postpartum time periods which led to lower quality caregiver-infant bonding (Liu et al., 2022) and adversely affected children's health and development (de Araújo et al., 2021). COVID-19-related stress also hindered caregiver-child feeding practices and experiences. González et al. (2022) reported that caregivers’ stress increased during the pandemic, which was correlated with greater use of food for emotional and behavioral regulation, decreased enjoyment with eating, less monitoring of their child's diet, and their child demonstrating more problematic feeding behaviors. Additionally, Rodgers et al. (2023) reported that mothers increased their use of food as a behavioral reward and decreased the use of standard meal settings during the pandemic. Although both cohorts’ data were collected during the pandemic and their experiences were likely vastly different, perhaps this mainland US cohort was more affected by the negative consequences of COVID-19 on children's feeding practices.
Another factor that could be relevant to the difference in the Selective/Restrictive PediEAT subscale between cohorts is cultural feeding differences. Puerto Rican infants are reported to exclusively breastfeed for a shorter duration compared to infants born in the mainland US, which in turn introduces them earlier to liquids such as water, juice, and cow's milk (CDC, 2023; Sinigaglia et al., 2016). Similarly, Hispanic infants are more likely than non-Hispanic infants to regularly eat puree baby foods by four-to-five months and eat fresh fruits, baby cookies, and fruit-flavored drinks between six-to-11 months (Mennella et al., 2006). Additionally, Hispanic infants and toddlers eat more foods relevant to their culture like soups, rice, and beans compared to their non-Hispanic counterparts (Mennella et al., 2006). Cultural beliefs and practices can also affect children's feeding experiences. Hispanic mothers report strong attitudes of maternal responsibility for having well-fed children and employ reinforcement strategies, persuasion tactics, and food rules for children to eat plentifully and healthily (Martinez et al., 2014). Cartagena et al. (2014) reported similar findings to these points in a review on factors contributing to Hispanic infant overfeeding. Specifically, nonexclusive breastfeeding, early introduction of solid foods, and maternal perception of chubbier babies are healthy are all relevant Hispanic feeding practices that relate to overfeeding infants (Cartagena et al., 2014). These cultural aspects on feeding may result in an early introduction to a variety of foods, decreased food selectivity, and increased eating of foods with different textures in Hispanic children and thus would correspond to low scores on the Selective/Restrictive subscale of the PediEAT.
This study has several strengths and limitations. A major strength of this study that it is the first to translate, culturally adapt, and test internal consistency of a caregiver-reported feeding assessment in Puerto Rican Spanish. These results can offer a valuable resource for Puerto Rican practitioners and families during pediatric feeding evaluation. Another study strength is that the translation and cultural adaptation of the PediEAT was completed by a Puerto Rican pediatrician certified by the American Board of Pediatrics with ample clinical and academic background in pediatric feeding which facilitates its accuracy and utility for Puerto Rican Spanish speakers. Two limitations of this project include the small sample size used to evaluate the internal consistency of the Puerto Rican Spanish version of the PediEAT and the cohort was not representative of a clinical population. Although our sample size was sufficient for acceptable internal consistency on 60 out of the 78 items in the Puerto Rican Spanish version of the PediEAT (Bujang et al., 2018), future studies using the Puerto Rican Spanish version of the PediEAT should employ the tool in larger samples of populations with a diagnosed PFD to evaluate its internal consistency among its subscales and Total Score.
Conclusion
The adapted version of the PediEAT into Puerto Rican Spanish demonstrated high internal consistency indicating that this tool can serve as a reliable caregiver-report tool to evaluate feeding difficulties among Puerto Rican families. This scale captured significant differences in Selective/Restrictive PediEAT subscale between the Puerto Rican and mainland US cohort, with the mainland cohort reporting significantly more selective and restrictive eating behaviors. Future studies should explore these differences in larger samples with various clinical populations at-risk for feeding difficulties.
Footnotes
Acknowledgements
The authors would like to thank the infants and their families who participated in this research.
Ethical considerations
This study was approved by Northeastern University's Institutional Review Board (NO: #18-09-10).
Consent to Participate
This study was approved by Northeastern University's Institutional Review Board (NO: #18-09-10). Caregivers provided written informed consent for themselves and for their infants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was funded by the Eunice Kennedy Shriver National Institute of Child Health & Human Development under grant 1R21HD095321.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Pediatric Eating Assessment Tool data underlying the findings are available upon request. Requests can be made by contacting: Northeastern University, 360 Huntington Ave, 525 Behrakis Building, 617-373-4670 (phone), or snl@northeastern.edu (email).