
Abstract
This study examines how variation in state-level immigrant policies affects maternal health outcomes among immigrant populations in the United States. Applying a policy bundle approach, this study first identifies supportive and restrictive policies to capture the complexity of state-level contexts. It then evaluates the impacts of four immigrant policy bundles on access to prenatal care, using natality data from the National Center for Health Statistics between 2015 and 2019. The logistic regression model resulted that the education policy bundle, one of the supportive policy types, was significantly associated with improved early prenatal care among immigrant pregnant women. These findings confirm the critical role of education-related policies in prioritizing equitable maternal health outcomes, highlighting the importance of supportive social policy interventions from the earliest stages of pregnancy for immigrant communities.
Introduction
The intersection of immigration policy and health equity has become an increasingly urgent area of concern, particularly considering recent anti-immigrant rhetoric and restrictive policies in the United States. Policy shifts, such as Trump administration’s expansion of the public charge inadmissibility rule to include non-cash public benefits, have had profound consequences for immigrant communities. These policy changes have led to a significant decrease in participation in safety-net programs, including Medicaid, the Supplemental Nutrition Assistance Program (SNAP), and the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC; Barofsky et al., 2020). This decline is largely attributed to a chilling effect, wherein heightened fear and misinformation regarding deportation or legal status repercussions discouraged many immigrant families from accessing critical health and nutrition service (Bernstein et al., 2020; Friedman & Venkataramani, 2021). Consequently, barriers to healthcare access have intensified, exacerbating disparities in preventive care.
Given these policy-driven disparities, it is essential to examine how state public policy environments shape immigrant health disparities. Immigrant law and policies can either expand or restrict rights and eligibility for social benefits critical for healthcare access (Perreira & Pedroza, 2019). Despite growing attention to the impact of immigration policies on immigrant health, several critical gaps remain unaddressed. Much of existing research has focused predominantly on the effects of restrictive policies, those that criminalize immigration based on citizenship status (Novak et al., 2017), while the impact of supportive policies remains underexplored (Sudhinaraset et al., 2021). Therefore, there is limited empirical evidence on whether supportive policies contribute to improving health outcomes or alleviating potential harms of restrictive policy environments. Additionally, previous studies on immigrant policy often examines single policies or policy events (Wherry et al., 2017), failing to capture the broader policy climate that shapes immigrant health. While there is increasing recognition that the social determinants of health play a crucial role in shaping the well-being of immigrants (Hahn, 2021; Islam, 2019), this approach has been underutilized in public health research. A major challenge in measuring immigrant policy effects is the complexity of policy implementation, so that prior studies often fail to account for the intensity of policy enforcement (Sudhinaraset et al., 2021; Young et al., 2020).
To address these gaps, this study aims to investigate states’ policy contexts and their impact on immigrants’ health service utilization by employing a policy bundle approach. The policy bundle approach captures not only the concurrent mechanisms in state policy contexts but also the intensity of policy implementation and modified policy components after adoption (Neeley & Richardson, 2022). By classifying the characteristics of diverse policy contexts rather than using a blunt dichotomous construct of policy adoption, this study can leverage variations in state immigration policies and the timelines of their implementation so as to assess their differential impact on immigrants’ health service utilization. This study employs a logistic regression model to estimate the impacts of policy contexts, incorporating control variables, state and year fixed effects, and standard errors clustered by state. The primary data source is the restricted version of the Natality files from the National Vital Statistics System (NVSS) for 2015 to 2019, merged with state-level data collected through a policy scan. A detailed discussion of this dataset follows in a later section.
Diverging State-level Policy Landscapes in Immigrant Health Disparities
A growing body of literature underscores the multifaced impact of policy environments on immigrant health, with policies exerting both directly and indirectly (e.g. P. Braveman et al., 2011; Dondero & Altman, 2020; Wallace et al., 2019). Some policies have immediate effects on immigrant health, such as access to healthcare and public assistance programs. Others function indirectly, influencing socioeconomic status like educational attainment and income, which are critical to long-term health outcomes (Lee & Zhou, 2020). Furthermore, research informed by the social determinants of health framework has investigated not only the impact of policies specifically related to health benefits but also the influence of non-health policies that shape social conditions essential for health outcomes (P. A. Braveman et al., 2010; Young & Wallace, 2021). Given that immigrants face systemic disadvantages in accessing health-promoting resources and are more likely to experience lower socioeconomic status (Parmet et al., 2017), it is critical to investigate how policy environments influence healthcare utilization and health disparities in immigrant communities.
State-level policies have drawn increasing attention due to their substantial discretion in implementing federal immigration mandates (Wallace et al., 2019). Since the enactment of Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) of 1996, states have assumed a key role in determining whether immigrants can access critical safety-net resources, which are otherwise excluded by federal policies. Some states have executed policies to provide healthcare access and economic protections for immigrants, mitigating the impact of federal restrictions. Conversely, others have adopted more restrictive policies which reinforce federal exclusions and further limiting immigrant rights and eligibility.
The policy climate surrounding immigrants is neither uniform nor static—it varies considerably across states, producing distinctive policy contexts that shape health experiences at the state level. Most of immigrants lives in states with a unique combination of supportive and restrictive policies, creating highly variable policy contexts (Young & Wallace, 2019). Some states have adopted more inclusive approaches, blurring distinctions between citizens and noncitizens by granting access to healthcare resources and protections (Motomura, 2007). In contrast, states with more restrictive policy climates create structural barriers to essential resources, often driven by anti-immigrant sentiment, systemic discrimination, and restrictive legal frameworks (Rhodes et al., 2015). Thus, the intersection of supportive and restrictive policies in each state produces distinctive consequences for immigrant health and access to healthcare. A comparative policy analysis across states is necessary to understand how diverse policy contexts influence health outcomes, offering insights into policy interventions that can reduce health disparities.
Policy Integration Through Policy Bundles
Prior research on immigrant policy and health has largely focused on assessing the effects of individual policies or events by using pre- and post-adoption comparisons (Toomey et al., 2014) or cross-sectional comparisons between regions with and without policy legalization (Sudhinaraset et al., 2021). However, the impact of policies on immigrant health is far more complex than that, so a drawback of their measurements is that they are very specific to certain aspect of policy thereby failing to provide comprehensive measure of wide array of policies with a state where immigrants are living in. Though some studies in this topic have empirically examined the impact of state immigrant policies with a composite measure of the policy context (Dondero & Altman, 2020; Schut & Boen, 2022) but measuring the effects of state immigrant policy methodological issues still remain challenging (Wallace et al., 2019).
To address the complexity in measuring state immigrant policy contexts, this study employs policy bundle approach. A policy bundle serves as a classification framework that extends beyond a binary assessment of policy presence or absence. Instead, it aims to capture more nuanced distinctions that reflect the heterogeneity of policy landscape. By focusing on the diverse variations in policy design and implementation, this approach enhances measurement by moving beyond the initial adoption phase to evaluate the evolution of policies over time during their implementation (Neeley & Richardson, 2022). For instance, bundle scores are assigned based on the number of initially adopted policies and subsequently updated to reflect the bundle of policies over time. Therefore, this approach can offer the advantage of capturing temporal and regional variations in policy development, recognizing that policy decisions are not static at the point of original enactment but rather evolve and adapt throughout their lifespan (Neeley & Richardson, 2023).
State immigrant policy contexts in this study include different policies from multiple categories. States adopted each immigrant policy across different time periods; thus, the intensity of each policy implementation is different from each other. The policy bundle approach here allows for capturing the heterogeneity in policy characteristics across sectors, adoption periods, and implementation effects. To delineate the multiple dimensions of state immigrant policies more clearly, we summarize this policy heterogeneity by assigning scores across four domains based on underlying characteristics. The construction of these policy bundles includes continual measurement of each policy domain as considering implementation across the time period for each policy feature rather than simply the initial policy adoption. We construct policy bundle scales comprising four dimensions from both supportive and restrictive immigrant policies discussed in the next section. Each score in the bundles was measured based on the timing of effective implementation.
The Dual Impact of Supportive and Restrictive Policies on Immigrant Health
Wallace et al. (2019) presented a model of immigrant policy as a social determinant of health, outlining the network of five state-level public policy domains that specifically influence the life chances of immigrants. The domains encompass health and welfare benefits, higher education, labor and employment, and immigration enforcement. Guided by Wallace et al.’s model, this study hypothesizes that it is within these four primary domains presented in Table 1 that state-level policymakers can perpetuate disparities and inequities in access to and opportunities for health based on legal status.
State immigrant supportive and restrictive policies by areas with policy indicators.
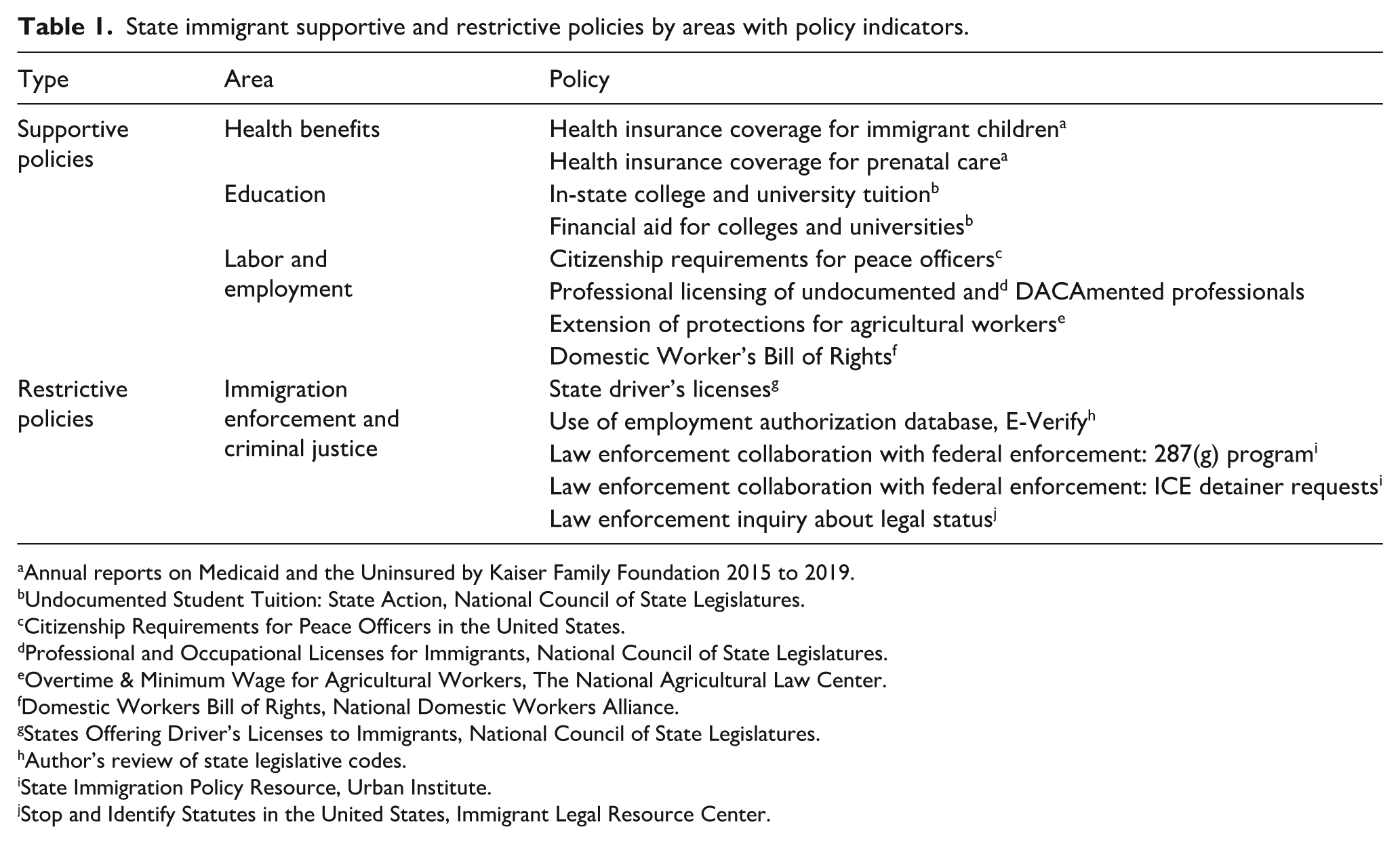
Annual reports on Medicaid and the Uninsured by Kaiser Family Foundation 2015 to 2019.
Undocumented Student Tuition: State Action, National Council of State Legislatures.
Citizenship Requirements for Peace Officers in the United States.
Professional and Occupational Licenses for Immigrants, National Council of State Legislatures.
Overtime & Minimum Wage for Agricultural Workers, The National Agricultural Law Center.
Domestic Workers Bill of Rights, National Domestic Workers Alliance.
States Offering Driver’s Licenses to Immigrants, National Council of State Legislatures.
Author’s review of state legislative codes.
State Immigration Policy Resource, Urban Institute.
Stop and Identify Statutes in the United States, Immigrant Legal Resource Center.
Supportive Immigrant Policies
Supportive policies refer to individual policies that have mechanisms of expanding eligibility and rights, thereby facilitating access to healthcare-related resources or medical. Previous studies have largely explored the impact of state-level supportive policies on immigrant health across three key domains: public health benefits, higher education, and labor and employment (Wallace et al., 2019). While various policies can influence immigrant health, these three areas best illustrate state-level discretion in shaping access and opportunities for citizens and noncitizens alike (Motomura, 2014). A rich body of scholarship argues that expanding access to health insurance and adopting inclusive coverage policies significantly improve prenatal care utilization, preventive services, and overall healthcare access for immigrants (Gennaro et al., 2016). Medicaid expansion, for instance, has been associated with higher healthcare utilization and improved health outcomes (Dave et al., 2008).
Education serves as a fundamental determinant of health, shaping the individuals’ socioeconomic status and health literacy (Ross & Wu, 1996). Previous studies identify three key pathways through which education impacts health outcomes. First, higher educational attainment is associated with greater health knowledge and literacy, enabling individuals to make informed health-related decisions and engage in preventive healthcare behaviors (Sanders et al., 2009). Additionally, educational attainment may be relevant to language proficiency which is necessary for communication and interaction with healthcare providers (Poureslami et al., 2011). Limited language proficiency is consistently identified as a barrier to healthcare access, restricting immigrants’ ability to navigate health services (Pandey et al., 2021). Second, education enhances employment prospects, increasing the likelihood of securing jobs with better working conditions, benefits, and higher wages, which in turn, improves access to healthcare and financial stability (Bartley & Plewis, 2002). Third, education improves greater personal control and stronger social support, all of which contribute to maintaining good health (Greer et al., 2013; Leganger & Kraft, 2003).
Employment plays a crucial role in immigrant health by influencing workplace protections, wage security, and access to employer-sponsored health benefits (Collins et al., 2004). Economic resources, particularly income and wealth, are often linked to health outcomes (Deeming, 2013), as higher earnings provide better healthcare access and private insurance coverage (Pollack et al., 2007). This study also focuses on policies providing occupational opportunities for immigrants. While such policies may not be always directly tied to income or wealth, restrictions on employment access can contribute to social exclusion, limiting immigrants to belong into their communities (The Law Enforcement Immigration Task Force, 2017). In this context, state policies that ensure fair wages and workplace protections can promote health-seeking behaviors and mitigate occupational health risks among immigrant workers.
Restrictive Immigrant Policies
Current immigration enforcement strategies have become increasingly punitive, entangling with criminal law enforcement to blur civil violations and criminal offenses, thereby heightening legal and social vulnerabilities for immigrants and increasing the risk of surveillance, detention, and deportation, creating a hostile policy climate that affects both legal and undocumented immigrants (García Hernández, 2015).
Several state-level policies regulate daily activities through increasing immigrant surveillance and legal scrutiny. These policies require law enforcement officers to verify an individual’s immigration status during routine encounters, such as traffic stops. Refusal to provide documentation can lead to arrest, detention, or further legal scrutiny (Torche & Sirois, 2019). State policies also extend surveillance into the workplace through mandatory employment verification programs, such as E-Verify, which requires employers to confirm a worker’s legal status. These policies increase the risk of workplace discrimination, limit job opportunities, and deter noncitizens from seeking formal employment due to fear of legal repercussions (Amuedo-Dorantes & Pozo, 2019). Additionally, several state policies impose driver’s license restrictions based on immigration status, limiting mobility and making everyday tasks, such as attending medical appointments, more difficult for immigrants. These restrictions further contribute to legal precarity by increasing the likelihood of law enforcement encounters, which could lead to immigration status checks and potential detention.
Beyond surveillance and verification, state-level immigrant policies collaborate with federal enforcement agencies, particularly through programs such as Immigrant and Customs Enforcement (ICE) partnerships. These collaborations could amplify the risks of arrest, detention, and deportation (Yasenov et al., 2020). Under the 287(g) program, state and local law enforcement agencies are deputized to function as federal immigration officers, granting them access to federal databases to identify and detain immigrants deemed removable (Bernstein et al., 2022). In addition to 287(g), ICE often requests local jail to hold immigrants in detention for additional time to process removal proceedings or screen their deportability (Graber & Marquez, 2016). These state-federal partnerships heighten immigrants’ fears of interacting with law enforcement, reinforcing the perception that any encounter could lead to deportation or legal consequences.
Restrictive immigrant policies have far-reaching implications for healthcare access, surveillance in daily life, and interactions with the criminal justice system. The increasing entanglement between immigrant enforcement and criminal law has increased the risks of arrest, detention, and deportation among immigrant populations. As a result, immigrants residing in states with restrictive policies are more likely to experience distrust, fear, and stress related to deportation risks (Salas et al., 2013). Empirical research demonstrates that restrictive immigration policies deter healthcare utilization, as immigrants avoid medical facilities due to fears of status verification and interactions with authorities, which his leads to delayed care, lower preventive service use, and poorer health outcomes (Hacker et al., 2011).
Methods
Data
The main data source of this study is the restricted version of the Natality files in the National Vital Statistics System (NSVV) from the National Center for Health Statistics. This dataset virtually covers record of all births from registered birth certificates across the United States and other U.S. territories (National Vital Statistics System, 2019). This database contains the characteristics of mothers and infants and detailed information upon the birth. The sample studied in this study includes all singleton births from foreign birthing people aged 15 to 44 years and born in a hospital within 50 states and the District of Columbia from 2015 to 2019 (N = 3,812,802).
Table 2 presents descriptive statistics of overall samples by health insurance state during the study period and shows substantial differences in outcome measures and characteristics of mothers and infants. Of the 3,812,802 live births and mothers in the analysis, more than half was publicly insured immigrants. Privately insured immigrants were roughly two out of five and approximately 10% of them were uninsured. Overall, the predominance of mothers initiated the prenatal care service in the first trimester, and this varied across the insurance type. Privately insured immigrants were more likely to make earlier entry into the prenatal care than both publicly insured and uninsured immigrants. In addition, privately insured immigrants showed higher level of education than immigrant with other types of insurance. Such greater education could reflect the substantial differences in mother’s race and ethnicity. The majority of mothers with private insurance were Asian followed by Hispanic and Non-Hispanic White. It is of note that almost half of overall sample were Hispanic populations and their predominant share for publicly insured immigrants and uninsured immigrants. Thus, such a stark difference in the share across racial and ethnic groups could represent greater educational attainment for privately insured immigrants than others. For infant characteristics, first born infants were more likely to have mothers with private insurance compared to mothers with other types of insurance.
Number of immigrants by health insurance status, 2015 to 2019. a
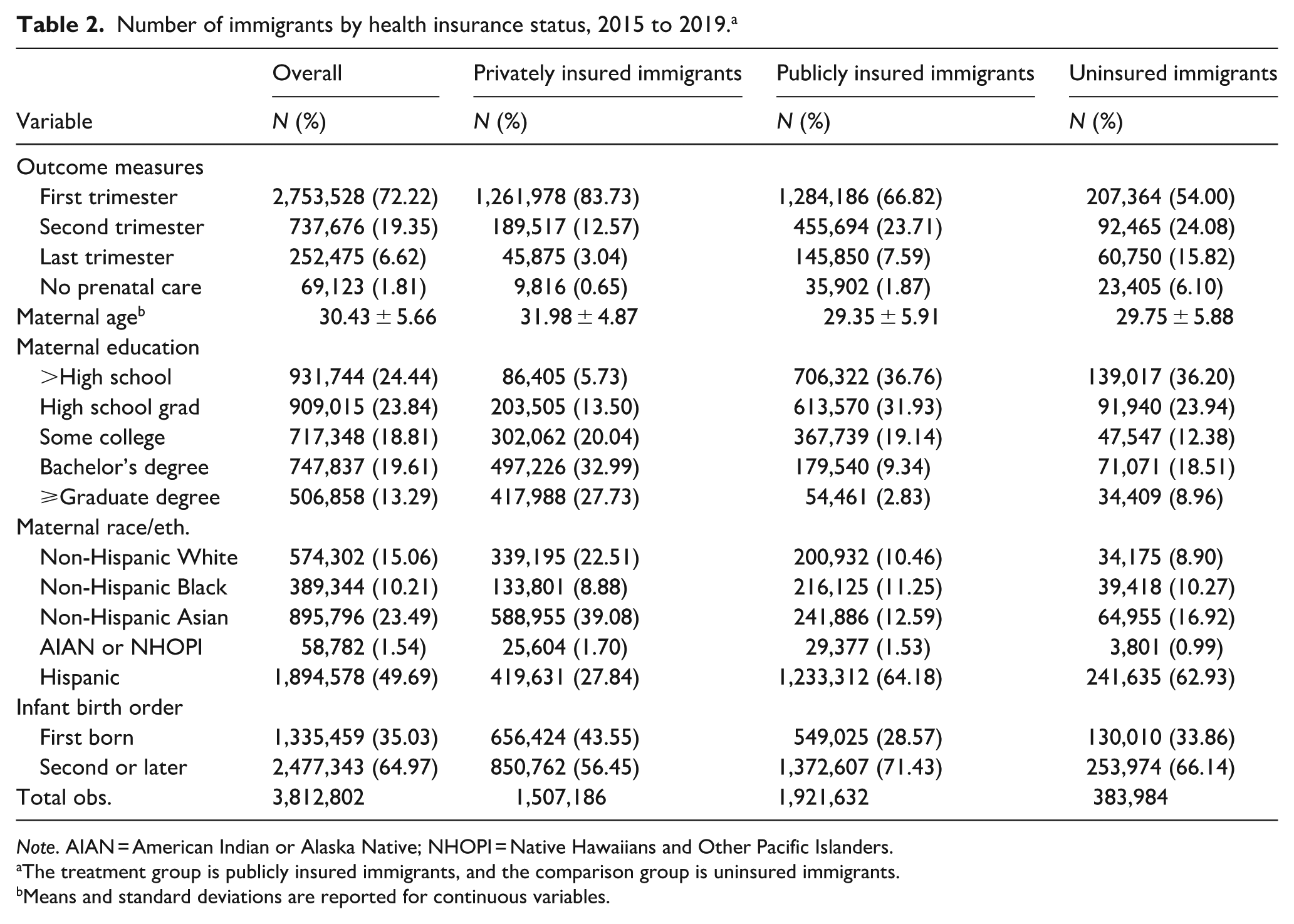
Note. AIAN = American Indian or Alaska Native; NHOPI = Native Hawaiians and Other Pacific Islanders.
The treatment group is publicly insured immigrants, and the comparison group is uninsured immigrants.
Means and standard deviations are reported for continuous variables.
Table 2 presents the descriptive statistics for the overall sample, categorized by health insurance status during the study period, highlighting significant differences in outcome measures and maternal and infant characteristics. Among the 3,812,802 live births and mothers included in the analysis, more than half were publicly insured immigrants. Approximately two in five were privately insured immigrants, while around 10% were uninsured. Overall, the majority of mothers initiated prenatal care during the first trimester, though this varied by insurance type. Privately insured immigrants were more likely to begin prenatal care earlier than both publicly insured and uninsured immigrants. Additionally, privately insured immigrants exhibited higher levels of educational attainment compared to those with other types of insurance, which may be attributed to their differing racial and ethnic composition compared to those with other types of insurance. Most of privately insured mother were Asian, followed by Hispanic and Non-Hispanic White individuals. Notably, nearly half of the overall sample consisted of Hispanic mothers, who constituted the largest proportion of both publicly insured and uninsured immigrant groups. Regarding infant characteristics, first-born infants were more likely to have mothers with private insurance compared to those with other types of insurance.
This study’s dataset comprises both individual-level characteristics and state-level attributes, which were gathered through the authors’ independent policy scan. In addition to these policy scans, data collection on state policies was further supported by an examination of state statutes, legislative codes, and annual policy briefs or reports from various policy research institutions, as summarized in Table 1. Following data cleaning procedures conducted in Stata, the state-level datasets were integrated into the primary dataset to facilitate descriptive and regression analyses.
Measures
Four binary outcome measures were adopted as dependent variables in this study. Four dependent variables are related to both timing of prenatal care initiation and use of prenatal care. The timing of prenatal care initiation is defined based on when the first prenatal care began by gestational trimester. The first dependent variable is whether a mother began prenatal care in the first trimester (first to third month). The second dependent variable is whether a mother began prenatal care between the fourth and sixth gestational month. The third dependent variable is whether a mother began prenatal care during the last trimester (seventh month onward). The last dependent variable is defined as whether mother received no prenatal care until delivery.
The independent variables were the four policy bundle scales which includes 13 different state immigrant policies presented in Table 1. Building on previous studies (Neeley & Richardson, 2022, 2023), this study aggregated policy indicators and scaled each to a bundle score ranging from 0 to 100 for each state-year observation. For instance, a score of 0 would indicate no state-year observation. If a state implements one out of nine supportive policies and two out of five restrictive policies simultaneously, the state will receive a score of 11.11 in the supportive bundle and 40 in the restrictive bundle.
Drawing from previous study that identified relevant control variables influencing prenatal care utilization (Choi et al., 2023), we controlled for key maternal, infant, and regional factors. Maternal characteristics include age at childbirth (15–44 years), educational attainment (less than a high school diploma, high school diploma, or a college degree or higher), and race/ethnicity (Non-Hispanic White, Non-Hispanic Black, Non-Hispanic Asian, American Indian/Alaska Native or Native Hawaiian/Other Pacific Islander, or Hispanic). Infant-related variables encompass birth order and plurality (first-born or second or later). To account for regional socioeconomic conditions, county-level median household income and unemployment rate, derived from the American Community Survey (2014–2018 5-year estimates), were included as controlling variables.
Model Specification
To estimate the effects of state immigrant policy contexts on access to prenatal care among immigrant pregnant women, this study utilizes logistic regression model including control variables and state and year fixed effects with standard errors clustered by state. State fixed effects were used to control unobserved time-invariant characteristics of the states like political ideology, differences in healthcare systems, number of immigrant populations, and number of law enforcement officers which were not accounted for in the models. Based on discussed above, the multivariate logistic regression models with each independent variable as follows:

In this model,
Results
Table 3 presents the odd ratios of the association between four policy bundles and prenatal care initiation and utilization. After accounting for the significant impact of control variables on immigrant access to prenatal care, the findings indicate that educational benefits were significantly associated with improved prenatal care access. The education policy bundle scale shows a 0.1% increase in the odds of initiating prenatal care in the first trimester (OR = 1.001; 95% CI [1.000, 1.003]), a 0.2% decrease in the odds of prenatal care initiation in the last trimester (OR = 0.998; 95% CI [0.997, 0.999]), and a 0.3% decrease in the odds of no prenatal care (OR = 0.997; 95% CI [0.995, 0.998]). These findings suggest that if a state were to shift from the lowest (0) to the highest (100) level on the education policy scale, early prenatal care initiation would increase by 10%, while late prenatal care initiation and lack of prenatal care would decline by 20% and 30%, respectively. Consistent with previous studies, this finding suggests that access to higher education may correlate with well-informed healthcare-related decisions due to enhanced health literacy and improved awareness (Dewalt et al., 2004; Sanders et al., 2009).
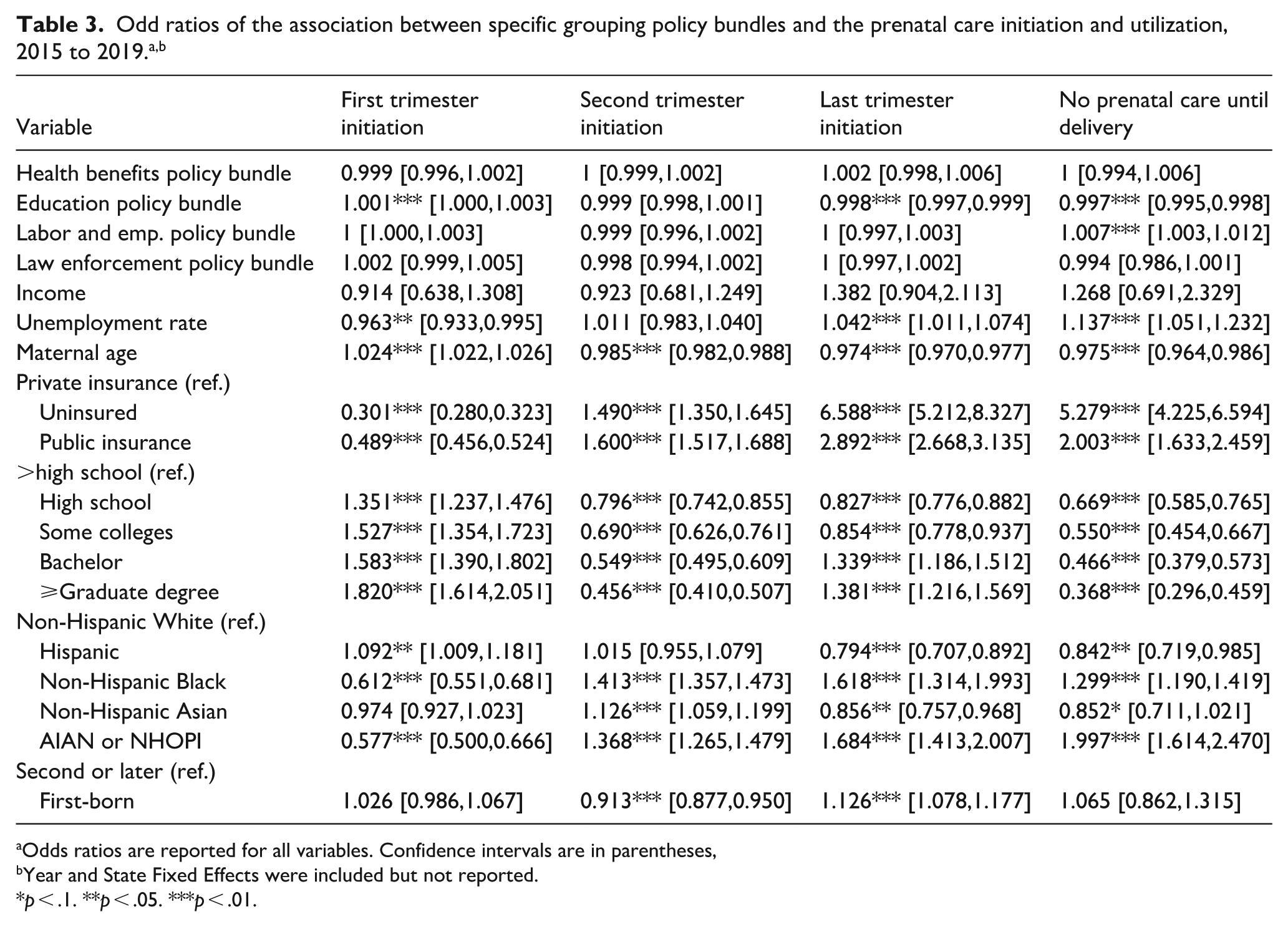
Odds ratios are reported for all variables. Confidence intervals are in parentheses,
Year and State Fixed Effects were included but not reported.
p < .1. **p < .05. ***p < .01.
Contrary to expectations, the labor and employment policy bundle scale demonstrates a 0.7% increase in the odds of not receiving prenatal care until delivery (OR = 1.007; 95% CI [1.003, 1.012]), and this indicates a 70% increase in odds when moving from the minimum to the maximum on the labor and employment policy bundle scale. However, this study found no evidence supporting policies providing benefits in the labor and employment sector were not significantly associated with other outcome measures. It is crucial to note that the labor and employment policies analyzed in this study do not adequately represent most immigrants. For example, the American Community Survey (U.S. Census Bureau, 2022) indicates that only 2% of immigrants were employed in agriculture, forestry, fishing, hunting, and mining as of 2022. This suggests that a small proportion of immigrants benefit from policies providing extensive protections for agricultural workers. Similarly, less than 1% of immigrants (approximately 0.88%) worked as domestic workers in 2021 (Banerjee et al., 2022), meaning that only a minor fraction can benefit from the Domestic Worker’s Bill of Rights. Lastly, an estimated 2.7% of immigrants were engaged in the public administration industry as of 2022 (U.S. Census Bureau, 2022). Given that public administration encompasses various governmental agencies, only a few immigrants can benefit from policies expanding eligibility for noncitizens, such as the policy allowing permanent residents to become peace officers.
Additionally, we found no evidence supporting that health benefits policy bundles were associated with the prenatal care utilization among immigrant populations. For health benefits policy, one possible explanation for such unexpected findings is that the study sample in this study includes a significant proportion of privately insured immigrants, comprising approximately 40% of the entire sample. It is of note that privately insured immigrants often have better access to care or are less likely to face the same barriers in access to care than immigrants with other types of health insurance (Choi et al., 2023. Therefore, large proportion of privately insured immigrants in the sample might lead to underestimation of the policy effects providing public health insurance to immigrant populations on their access to prenatal care.
Furthermore, we found that the law enforcement policy bundle was not significantly associated with the use of prenatal care among immigrants. One possible explanation for this finding is that many states became more restrictive toward immigrants during the study period, and this may lead immigrant populations to prolonged exposure to a stressful environment. Additionally, heightened fear and distrust stemming from anti-immigrant rhetoric and enforcement during and after the 2016 presidential election could have a more significant impact on their limited access to essential social resources for healthcare utilization, such as benefits from safety-net programs (Barofsky et al., 2020). Such pervasive national contexts may overshadow state-level policy changes, thereby diminishing the importance of state variations, considering the magnitude of the chilling effects even on legal immigrants (Friedman & Venkataramani, 2021).
Maternal age was significantly associated with high probability of prenatal care initiation in the first trimester and lower probability of delayed prenatal care initiation and not receiving prenatal care. The estimate also shows that mother’s educational attainment was associated with high rates of early prenatal care initiation and low rates of delayed and not receiving prenatal care until delivery. Health insurance type was significantly associated with the initiation and receipt of prenatal care. Compared to privately insured immigrants, publicly insurance immigrants and uninsured immigrants had lower odds of early prenatal care initiation and higher odds of delayed prenatal care initiation and not receiving prenatal care. Being Hispanic was associated with higher rates of prenatal care initiation in the first trimester and lower rates of delay in prenatal care initiation and no receipt of prenatal care. The estimates suggest that being Non-Hispanic Black and being AIAN or NHOPI was associated with lower probability of first trimester initiation and higher probability of delaying of and not receiving prenatal care until delivery.
Discussion and Conclusion
This study examined how state-level immigrant policy contexts, both health and non-health policies, influence immigrants’ access to care, providing a comprehensive perspective on the macro-level social factors that shape immigrant well-being and health. The primary findings are improvements in access to prenatal care among immigrant populations are associated with increased implementation of social policies, particularly those providing educational benefits regardless of citizenship status. The findings on the education policy bundle are consistent with our expectations based on past research which acknowledges educational attainment as a robust predictor of various life outcomes, including employment, income, health, and overall quality of life, thus making it a crucial focus for interventions aimed at reducing inequities (Mirowsky & Ross, 2003). However, the findings on the labor and employment policy bundle do not comport with the findings from prior research. Though its association with most of outcome measures were not statistically significant, greater labor and employment policy bundle scale is associated with lower odds of using prenatal care among immigrant families. These findings may underscore that immigrant policies in different sectors can have varying effects on healthcare utilization, emphasizing the complexity of policy design in shaping immigrant health outcomes.
Furthermore, this study found that the law enforcement policy bundle was not significantly associated with prenatal care utilization among immigrants. This result may reflect the pervasive national context of heightened immigration enforcement and anti-immigrant rhetoric, particularly during and after the 2016 presidential election, which intensified fear and distrust of public systems (Barofsky et al., 2020). Prior research documents chilling effects in which immigrants, including those lawfully present, avoid health care and safety-net programs out of concern for deportation or immigration consequences (Bernstein et al., 2020; Friedman & Venkataramani, 2021; Watson, 2014). These dynamics likely overshadowed variation in state-level enforcement policies, making it difficult to detect measurable differences across states. At the same time, prior studies also show that enforcement effects are not uniform; local policy actions, cooperation with federal authorities, and regional political climates can exacerbate or mitigate fear-driven barriers to care (Rhodes et al., 2015). Situating our findings within this broader evidence base highlights the importance of considering both localized enforcement intensity and national policy rhetoric when assessing immigration policy impacts on health care access.
While previous studies primarily focus on either supportive or restrictive policies (e.g. Young & Wallace, 2019), this study explores the dynamics of both kinds of policies in the states. This approach allows for determining whether and how supportive policies can offset the negative impacts of restrictive policies. By applying social determinants of health perspective, we also access the effects of public policies across multiple sectors, recognizing that polices outside the healthcare domain, such as those related to education, labor and employment, and law enforcement, can have indirect and long-term health effects on immigrants’ access to care (P. Braveman et al., 2011). While health-specific policies may yield immediate improvements in access, broader policies can have long-term health effects on immigrant health (Perreira & Pedroza, 2019). Additionally, this study addresses key measurement issues in assessing immigrant policy environments. By employing a policy bundle approach, we capture heterogeneity in policy designs across multiple sectors and develop a composite measure that reflects the unique combination of policy contexts within each state (Young & Wallace, 2019), account for immigrants’ simultaneous exposure to multiple policies rather than relying on single policy indicators, ensuring a more accurate representation of policy contexts (Samari et al., 2021), and include an indication of policy implementation intensity (Young et al., 2020). These policy bundle scales can be utilized to assess variations in health outcomes across states and assess changes in state policy environments as new policies emerge or are adopted in other states.
While this study was conducted with rigorous methodology, we acknowledge several limitations, particularly those related to modeling and measurement issues. First, this study heavily relies on state fixed effects in estimating policy changes across states. It is possible that individual mothers with state characteristics are nested within certain state policy environments so that fixed effects are not necessary for this analysis since this can chew up state-level policy effects. Future research is needed to conduct analysis with mixed effects (year fixed effects and state random effects) modeling. Second, this study was unable to incorporate the precise timing of state policy adoptions due to data limitations. Given that many of the policies analyzed were introduced and implemented beginning in the 2000s, extending the study period may allow future research to better capture the long-term and potentially diminishing effects of these policies over time. Addressing this data constraint remains an important area for future research. Third, the findings suggest that the labor and employment policy bundle may not fully capture the policy environment experienced by most immigrants, which could explain the unexpected association with delayed prenatal care. While policies related to agricultural protections, domestic workers’ rights, or eligibility expansions for public-sector employment are important within their respective sectors, these industries collectively employ less than 6% of immigrants (Banerjee et al., 2022; U.S. Census Bureau, 2022). The limited applicability of these policies underscores a misalignment between state-level labor policy measures and the actual distribution of immigrant employment, suggesting that aggregate indices may overrepresent policies affecting niche sectors. This measurement issue warrants caution in interpreting the results and points to the need for future research using more representative labor policy metrics and detailed individual-level employment and visa data.
Fourth, the analysis is limited by the measures available in the NVSS natality data. Although this dataset provides comprehensive coverage of births across the United States, it does not include important social determinants such as housing stability, food security, or neighborhood conditions, all of which disproportionately affect immigrant families and could mediate associations between policy environments and maternal health (Chehab et al., 2025; Dossett et al., 2024; Sharareh et al., 2023). The absence of these factors may constrain our ability to fully capture the mechanisms linking restrictive policies to prenatal care use. Future research should incorporate these intersecting determinants to provide a more comprehensive understanding of immigrant maternal health disparities. Fifth, the current framework places greater emphasis on supportive policies mainly because we observe a broader variety of supportive policies in the context of prenatal care outcomes, thereby resulting in the imbalance between policy types as a limitation of our study. This emphasizes the importance of future studies developing more comprehensive and balanced measures of policy environments.
Lastly, although this study represents a pioneering effort to address key measurement challenges in providing a comprehensive analysis of state-level immigrant policies, the absence of significant effects for certain policy bundles may reflect potential offsetting influences stemming from the simultaneous inclusion of both supportive and restrictive policies. Despite this limitation, the findings offer important insights into the positive role of educational policy bundles in shaping maternal health outcomes for immigrant families from the early stages. Future research should further explore these trade-offs when evaluating the combined effects of diverse policies.
There is growing acceptance that immigrant health is significantly influenced by the policy environments in which immigrants reside, as these serve as critical social determinants (Yang & Hwang, 2016). Some policies are supportive, fostering social inclusion by creating a welcoming climate for immigrant communities. For example, our findings indicate that education-related policies may function as forms of social support that reduce barriers and promote health equity for immigrant families. Conversely, restrictive policies may marginalize and even criminalize immigrants based on their legal status. The rise of anti-immigrant rhetoric and shifting political landscapes not only hinder immigrants’ access to essential health-related resources but also pose threats to their residency and stability.
The findings in this study highlight that social policies can have complex and sometimes unexpected implications for immigrant maternal health. Education-related policies appear to provide meaningful social support, whereas certain labor and employment protections may have unintended consequences when they do not adequately reflect the employment sectors in which most immigrants work. At the same time, restrictive enforcement contexts and anti-immigrant rhetoric can compound vulnerabilities, discouraging health care utilization even among legally present immigrants. These dynamics underscore that social and immigration policies, whether supportive or restrictive, play a central role in shaping maternal and child health outcomes in immigrant communities. Given these intersections, concerns about immigrant well-being extend beyond public health, making it an urgent interdisciplinary issue. Future research should continue to examine policies across various sectors to more comprehensively understand and address how immigration policy environments function as social determinants of health.
Footnotes
Ethical Considerations
There are no human participants in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Following the data use agreement with the National Center for Health Statistics, raw data would remain confidential and will not be shared.