
Abstract
The aging population in the United States continues to grow, emphasizing the need to promote independence and healthy aging. Oral health is an important indicator of overall well-being. Occupational therapists (OTs) are positioned to address oral health. This study examined the relationship between oral health and functional independence in self-care tasks among older adults. A secondary analysis of National Health and Nutrition Examination Survey (NHANES) data, years 2011–2018, was conducted with 4,791 adults aged 65 and older. A multivariable logistic regression was used to estimate odds ratios for self-care difficulty associated with oral health variables. Poorer self-reported oral health and less frequent flossing were significantly associated with difficulty in self-care tasks. Education, income, and age also demonstrated significant relationships with difficulty in self-care tasks. OTs should integrate oral health interventions into practice to enhance functional independence among older adults.
Plain Language Summary
This study used publicly available, federally collected data to test the relationship between oral health and self-cares in a sample of US-based older adults using bivariate analyses and multivariate logistic regression. We looked at self-care because as the population of older adults increases, it is important that we understand how to best support their independence in their daily lives. We were interested in oral health as it is an important health measure, associated with general well-being and other health factors, and is an area where occupational therapists can have an impact with their patients. We found that poorer self-reported oral health and less frequent flossing were associated with difficulty with self-care. We also found variables such as education, income, and age, to have significant relationships with self-care difficulty. These results confirm the importance of occupational therapists taking an active role in oral health interventions with their patients, ultimately supporting older adults in maintaining independence as they age.
The aging population in the United States is rapidly growing. By 2035, there are projected to be 76 million adults aged 65 years and older, representing 22% of the population, an increase from 17% in 2022 (U.S. Census Bureau, n.d.). The growing aging population raises potential concerns for the impact on the economy, health care system, and social programs. An increase in the population of older adults, both in community settings and long-term care institutions, necessitates an understanding of how to promote long-term independence and optimal health outcomes.
To support long-term independence, it is crucial that older adults retain the ability to perform basic self-care tasks such as grooming, dressing, bathing, and toileting—tasks collectively referred to as activities of daily living (ADLs). Health professionals, including occupational therapists and other care providers, play a key role in supporting the maintenance or restoration of these essential skills. Caregivers, friends, and family also support older adults in ADL independence. Declines in ADL independence are associated with lower overall and health-related quality of life, reduced functional capacity in other daily activities, increased risk of hospital admissions and readmissions, greater caregiver burden, higher health care and social support resource utilization, and increased mortality (Beltz et al., 2022; Falck et al., 2022; Fatema et al., 2022; Gao et al., 2023; Lyu & Wolinsky, 2017; Millán-Calenti et al., 2010; Sato et al., 2021; Tuttle et al., 2022).
One particularly vital ADL is oral hygiene, or taking care of one’s teeth and mouth. Poor oral health is associated with an increased risk of diabetes, mental health disorders, cardiovascular disorders, reduced quality of life, and elevated mortality (Badewy et al., 2021; Hazara, 2020; Kandelman et al., 2008). Perhaps unsurprisingly, poor oral health is also related to decreased functional independence in older adults, and functional independence in overall ADLs (Saintrain et al., 2018). Through interventions focusing on oral hygiene, occupational therapists have the ability to directly impact oral health and the associated ADL-related outcomes.
The purpose of this study is to explore the relationship between oral health and overall functional independence in self-care tasks in older adults through the use of a nationally representative, publicly available dataset. Although many analyses using the National Health and Nutrition Examination Survey (NHANES) have investigated oral health, few have focused on the association between functional independence in self-care tasks. Our research question examines the relationship between oral health—measured by time since last dentist visit, self-reported oral health rating, and frequency of flossing—and functional independence in self-care tasks, as assessed by two ADL measures: feeding and dressing. We anticipate that oral health is predictive of self-care difficulties.
Method
Sample and Design
A secondary data analysis was performed using the data from the NHANES. The NHANES is a nationally representative, population-based survey consisting of demographic, socioeconomic, dietary, and health-related questions as well as examination data on various health topics. The NHANES employs a complex, multistage probability sampling design to obtain a nationally representative sample of the noninstitutional U.S. population. Participants are randomly selected for counties across all U.S. Census regions using a household-based sampling framework (Centers for Disease Control, n.d.). For our analysis, following established literature, we pooled data collected in 2011–2012, 2013–2014, 2015–2016, and 2017–2018. More recent data was excluded due to the impact of the COVID-19 pandemic. Data were obtained and locally stored prior to March 2025 (Freilich & Kesselheim, 2025). Our final analytic sample consisted of adults 65 years of age and older with complete information on variables included in the models (N = 4,791). We specifically focused on adults aged 65 and older, the Medicare-eligible population in the United States, a population that often faces distinct health, functional, and health care utilization patterns relevant to our study objectives.
Functional Independence in Self-Care Tasks
Functional independence in self-care tasks was assessed using two tasks central to ADL performance: (a) difficulty using fork, knife, and cup and (b) difficulty dressing yourself. A response indicating inability or any level of difficulty with either task was classified as self-care difficulty. This resulted in a binary variable. In some, but not all years of the continuous NHANES, a third question about functional independence related to difficulty bathing or dressing, as a combined variable, was present. Given that it was not present in all datasets, we excluded this from the analysis. We focused solely on a self-care measure because to fully capture a robust functional independence in ADLs measure, indicators of functional mobility, personal hygiene (e.g., grooming and bathing), continence, and toileting would also be required, though are currently unavailable in the NHANES.
Oral Health
Oral health was defined using three main variables from the self-report questionnaire data: time since last dentist visit, self-report of health of teeth and gums, and how many days dental floss/device are used. This allowed for a multidimensional view of oral health through access to and utilization of oral health care, self-report of oral health, and participation in oral care. Time since last dentist visit and days flossed are categorical measures while the self-report oral health rating utilized a Likert-type scale. Time since last dentist visit was coded 1 = 6 months or less, 2 = >6 months, <2 years, 3 = >2 years, <5 years, 4 = >5 years, and 5 = Never have been. Oral health rating was coded 1 = excellent, 2 = very good, 3 = good, 4 = fair, and 5 = poor. Days flossed per week was coded 1 = 7 days flossed, 2 = 4 to 6 days flossed, 3 = 1 to 3 days flossed, and 4 = 7 days flossed. Oral exam data are present in the NHANES; however, due to high rates of missing data we did not utilize these measures for our analysis (Alyamani et al., 2025; Badr & Sabbah, 2020; Laniado et al., 2021). For example, sensitivity analysis suggests that the rate of missingness for oral exam data on tooth decay is about 80%.
Covariates
Covariates included type of health insurance, categorical income level, highest degree of education obtained, race/ethnicity, sex, and partnership status. Health insurance was coded in four groups: no health insurance, public insurance (Medicare, Medicaid), private insurance, and other. Income level was categorized into four groups: <$20,000, $20,000 to $44,999, $50,000 to $99,999, and $100,000+. Education level was coded into four groups: less than high school, high school, some college, and college or more. Race was grouped by the following self-report: non-Hispanic white, non-Hispanic black, non-Hispanic Asian, Mexican, and other Hispanic. Sex was included as a binary variable: male and female. Partner status was coded as a binary variable, where partnered represented those married and/or living with their partner. Foreign-born status was also coded as a binary variable (1= foreign born). Ages 80 or over are recorded as 80 in the NHANES dataset, age was coded in four groups: 65 to 69 years old, 70 to 74 years old, 75 to 79 years old, and 80 years of age or older.
Statistical Analysis
We estimated logistic regressions to examine the relationship between oral health variables and self-care difficulty. All control variables were included as covariates in the model, including for sex, age, race/ethnicity, education level, income level, partnership status, foreign-born status, and data collection year. Statistical analysis was performed using Stata statistical software (StataCorp, 2023). Statistical significance was determined at α = .05, 95% confidence interval.
Results
Participant Demographics
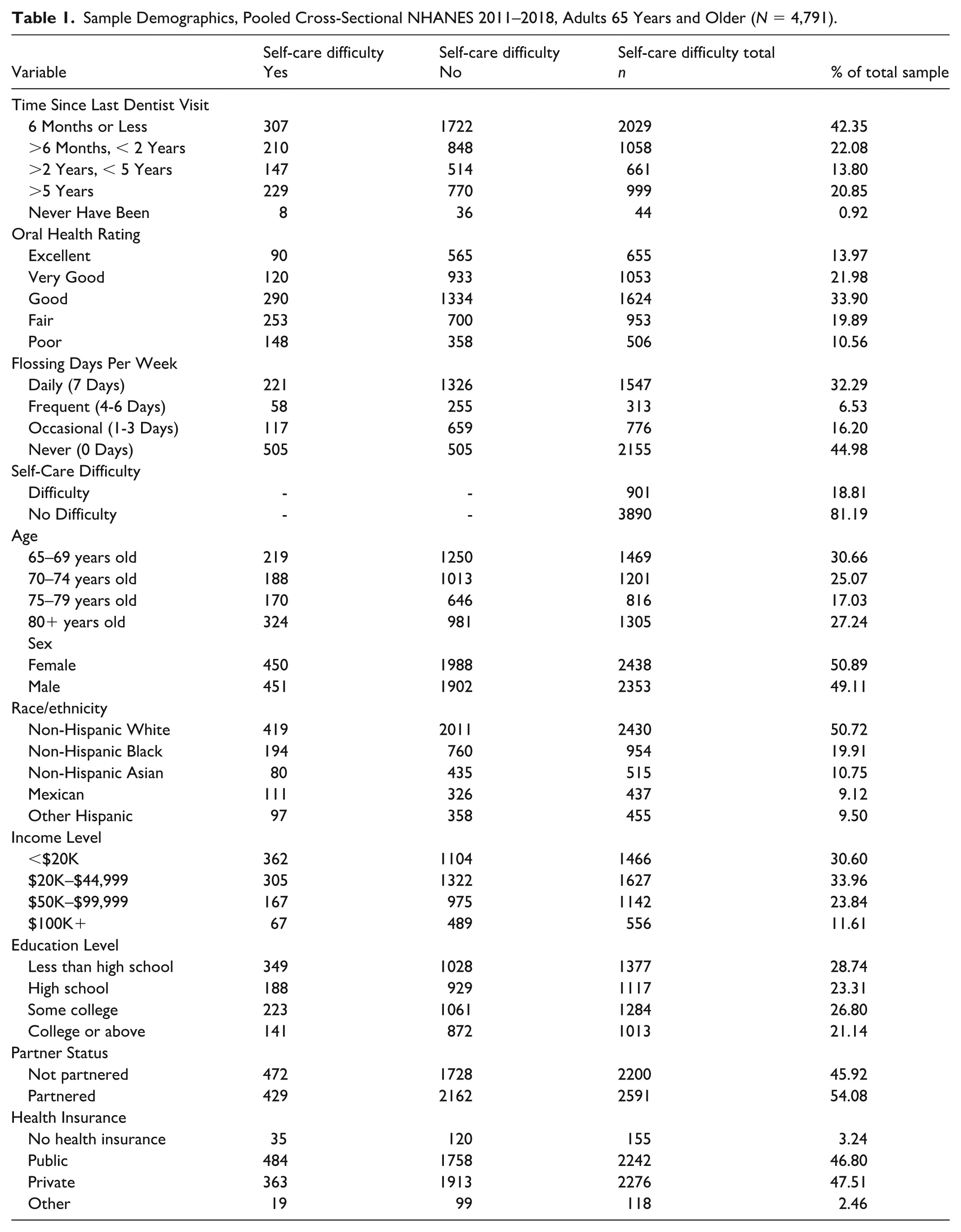
Table 1 displays the demographic characteristics of the analytic sample (N = 4,791) of adults aged 65 years and older, residing in the United States. Slightly more than half were female (51%), the largest age group was 65 to 69 years (31%), and 54% reported being partnered. Non-Hispanic white adults comprised the largest racial/ethnic group (51%). The most common household income was $20,000 to $44,999 (34%), and nearly one-third (29%) had less than a high school education. Having private or public health insurance was fairly equally represented with 48% having private health insurance and 47% having public health insurance. When considering oral health, 42% reported visiting a dentist in the past 6 months or less, one-third (34%) rated their oral health as good, and slightly less than half (45%) reported never flossing. For self-care performance, 19% reported having difficulty with at least one self-care task.
Sample Demographics, Pooled Cross-Sectional NHANES 2011–2018, Adults 65 Years and Older (N = 4,791).
Analysis Results
Table 2 presents the results in odds ratios from the multivariate logistic regression model. Two of the oral health measures were significantly associated with self-care difficulty. Those who rated their oral health as good (OR = 1.36, 95% CI: 1.05–1.77, p = .022), fair (OR = 2.16, 95% CI: 1.64–2.85, p = .000), or poor (OR = 2.31, 95% CI: 1.70–3.15, p = .000) had increased odds of self-care difficulty compared with those who rated their oral health excellent, net of controls. Those who never flossed (OR = 1.42, 95% CI: 1.16–1.73, p = .001) have increased odds of self-care difficulty when compared with those who floss daily, holding all else constant. Sensitivity testing was performed on the variables of interest. Separate models were run with the individual oral health variables and self-care difficulty; no moderation was found.
Logistic Regression Predicting Self-Care Difficulty, Pooled Cross-Sectional NHANES 2011–2018, Adults 65 Years and Older (N = 4,791).
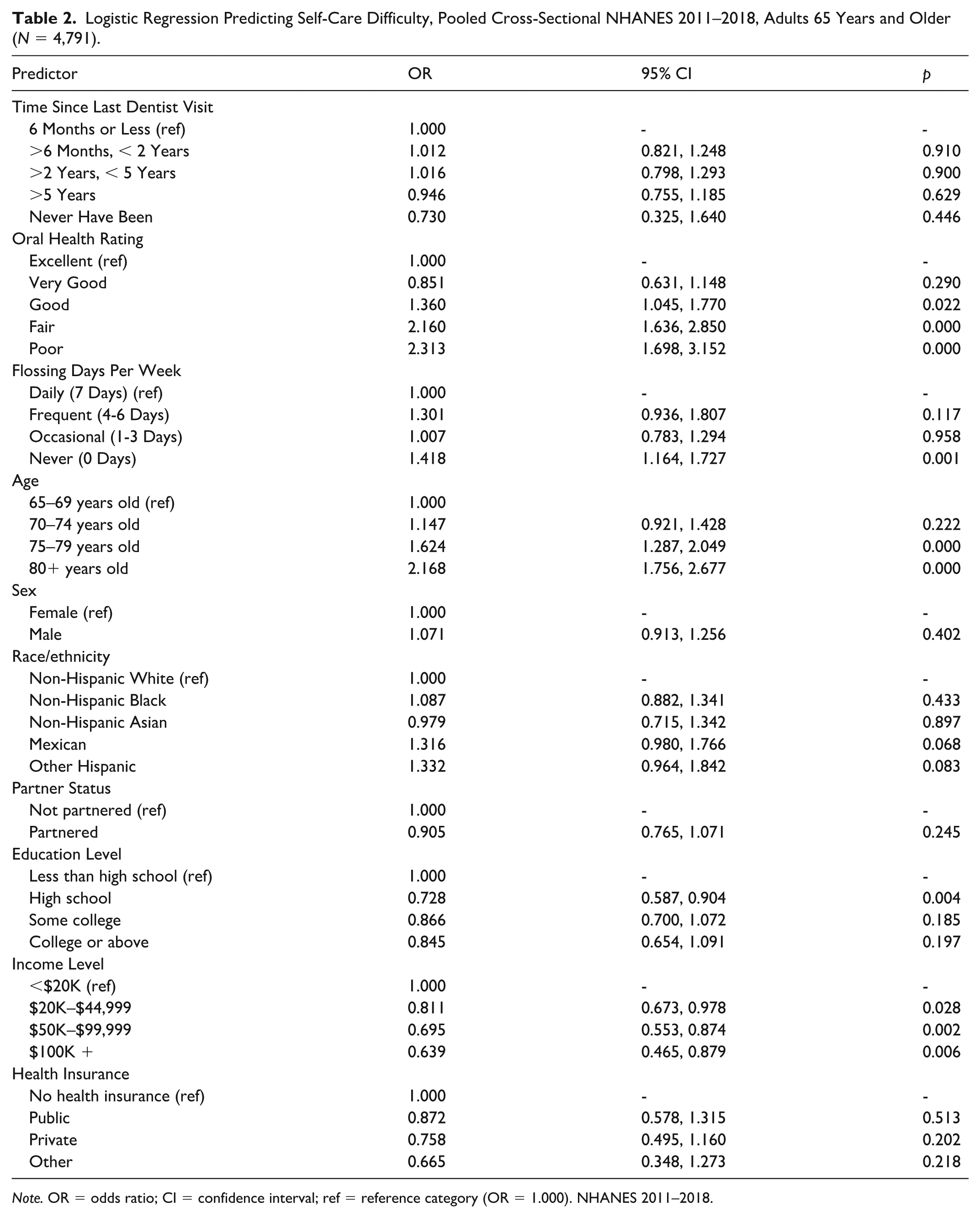
Note. OR = odds ratio; CI = confidence interval; ref = reference category (OR = 1.000). NHANES 2011–2018.
Certain demographic characteristics were associated with self-care difficulty, net of the controls. Compared with adults aged 65 to 69 years, those aged 75 to 79 and 80 years and older had significantly higher odds of self-care difficulty (OR = 1.62, 95% CI: 1.29–2.05, p = .000; OR = 2.17, 95% CI: 1.76–2.68, p = .000, respectively). Those with a high school education (OR = 0.73, 95% CI: 0.59–0.90, p = .004) had significantly lower odds of self-care difficulties compared with those with less than a high school education. Those with an income of $20,000 to $44,999 (OR: 0.81, 95% CI: 0.67–0.98, p = .028), $45,000 to $99,999 (OR = 0.70, 95% CI: 0.55–0.87, p = .002), and $100,000+ (OR = 0.64, 95% CI: 0.47–0.88, p = .006) have decreased odds of self-care difficulty compared with those with an income of <$20,000.
Discussion
The purpose of this study was to explore the relationship between oral health and functional independence in self-care tasks among a nationally representative sample of adults 65 years and older. The analysis aimed to use a multidimensional conceptualization of oral health by using three distinct measures: time since last dentist visit, self-report of health of teeth and gums, and how many days dental floss/device. Functional independence in self-care tasks was captured through combining two variables: difficulty using fork, knife, and cup, and difficulty dressing yourself, with the resulting binary variable referred to as self-care difficulty.
This study extends prior work by examining the association between oral health behaviors and functional self-care within a nationally representative U.S. sample. Previous research, including the study by Saintrain et al. (2018), was conducted in Brazil, our findings suggest that these relationships are also evident in the U.S. context. Furthermore, by operationalizing functional independence through two specific self-care tasks relevant to occupational therapy practice, this study offers a task-level perspective on functional capacity that complements broader measures of disability. These contributions help contextualize existing evidence within the U.S. setting while highlighting the relevance of everyday self-care behaviors to occupational therapy-informed approaches to oral health.
These findings align with existing research. Prior studies have shown that poor oral health is associated with reduced functional performance (Avlund et al., 2001; Zhang et al., 2018). Similarly, the demographic variables linked to self-care difficulty in our study, such as income and education, have also been previously identified as important determinants. Socioeconomic status has been reported as a key factor in influencing functional performance (Beltz et al., 2022; Fuller-Thomson & Gadalla, 2008; Liu & Wang, 2022). Furthermore, increased age has been linked to decreased ADL performance (Millán-Calenti et al., 2010).
Although dental visits are often considered an objective marker of oral health maintenance, we did not observe a significant association between dental visit history and self-care difficulty. This finding does not necessarily diminish the relevance of oral health behaviors. Dental visits capture only one dimension of oral health engagement and may be more strongly influenced by structural and contextual factors such as insurance coverage, cost, access to care, and dental anxiety, rather than by an individual’s functional ability to perform daily self-care tasks. In contrast, self-reported oral health and daily oral hygiene behaviors, such as flossing, reflect habitual health behaviors that are part of everyday routines and may be more sensitive to functional limitations. Prior research has also demonstrated that self-assessments of health are robust predictors of morbidity and mortality, underscoring the clinical relevance of subjective and behavior-based indicators even when objective service utilization measures are not associated (Lorem et al., 2020; Yu et al., 2024). Importantly, our findings reflect associations rather than causal relationships. The lack of association between dental visits and self-care difficulty may highlight the multidimensional nature of oral health, in which service utilization and daily self-care behaviors represent distinct but complementary domains.
Multiple factors affect oral care for older adults, ranging from individual characteristics to broader systemic elements such as health care policies and residential care guidelines (Grönbeck Lindén et al., 2017; Klaic et al., 2022). Occupational therapists are uniquely equipped to address these factors through both direct intervention and education focused on oral hygiene. This work supports integrating oral health promotion within occupational therapy practice across settings can support long-term independence, enhance functional independence in self-care, and contribute to improved overall health outcomes (Bellomo et al., 2005; Schoellig et al., 2025).
The findings of this study have important implications for clinical practice. Occupational therapists should be aware of these associations, as older adults who have lower income or education attainment and demonstrate decreased self-care performance may be at increased risk for oral health challenges. In particular, declines in self-care performance may signal the need for targeted assessment and intervention to support oral health behaviors. Incorporating oral health education, environmental modification, and task adaptation for oral care into routine occupational therapy practice may help mitigate barriers and support oral health among older adults.
It is important to acknowledge the limitations of this study. As a secondary data analysis, this study is constrained by the characteristics and availability of the existing dataset. The variables used are pre-determined and may not fully capture the constructs of interest. Particularly, our oral health measures are limited to non-examination data due to missing or incomplete records. Likewise, our self-care measure was limited to only two self-care tasks, which may not represent the full scope of functional independence and ADL performance. Furthermore, several variables were self-reported, introducing the potential for response bias and reflecting perceived rather than actual self-care performance. In addition, because the data are cross-sectional, we cannot determine causal direction. Declines in self-care functioning may lead to poorer oral hygiene and oral health over time, and poor oral health may also make self-care more difficult.
Despite these limitations, the findings of this study provide insights for occupational therapists working with older adults. Occupational therapists should consider the importance of oral health and its impact on general health, well-being, and potentially self-care performance and functional independence. When and where able, occupational therapists should include oral health intervention and education within their treatment sessions. Occupational therapists should also consider the relationship between patient demographics and oral health, as well as general oral health and self-care performance.
Conclusion
This study examined the relationship between oral health and functional independence in self-care tasks among older adults in the United States. The findings highlight the significant association between poor self-reported oral health and increased self-care difficulty, as well as between decreased flossing habits and greater self-care difficulty. In addition, the findings demonstrate that certain demographic factors such as lower socioeconomic status, like income and education level, and age are linked to self-care difficulty.
By exploring this relationship using a nationally representative dataset, this study contributes to a better understanding of the association between oral health and daily functioning in later life. These results contribute to the growing evidence base supporting occupational therapy’s role in promoting functional independence and participation through occupation. We know that oral hygiene is a core ADL, and oral health is an important indicator associated with multiple health outcomes, and that there are significant relationships between oral health and self-care performance (Badewy et al., 2021; Hazara, 2020; Kandelman et al., 2008; Saintrain et al., 2018). Therefore, occupational therapists should be diligent in applying an occupation-centered approach to improve and maintain the functional independence of older adults.
Footnotes
Acknowledgements
The authors have no acknowledgements to declare.
Ethical Considerations and Consent
This study was a secondary analysis of publicly available, de-identified data from the National Health and Nutrition Examination Survey (NHANES). As such, it was exempt from institutional ethics review. The original NHANES study was conducted by the National Center for Health Statistics (NCHS) and received approval from the NCHS Ethics Review Board. Informed consent was obtained from all participants by NCHS prior to data collection.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study are publicly available from the National Health and Nutrition Examination Survey (NHANES) and can be accessed through the Centers for Disease Control website.
AI Declaration
AI-assisted technology (ChatGPT 5.2) was used solely to refine language and improve readability. The authors verified and approved all edits. No AI tools were used to generate, analyze, or synthesize data, or to draft substantive content of this manuscript.