
Abstract
Older adults with subjective cognitive decline (SCD) experience emotional distress and report challenges or withdrawal from activities that support health and well-being. This qualitative descriptive study explored participation challenges of older adults with SCD, and their determinants. Data were collected through focus groups with 15 occupational therapists (OTs) working with older adults with SCD in community-based clinical settings, and analysed using deductive content analysis. OTs identified two key participation challenges: limited participation in healthy lifestyle activities, and negative occupational experiences (e.g., reduced enjoyment and diminished sense of competence). Personal determinants were subtle (yet normal) cognitive changes, ineffective strategy use, and limited knowledge about cognition and factors influencing it. Motivational determinants were adverse emotions and negative self-perceptions. Environmental determinants were insufficient social support and internalized age-related stigma. Future intervention for older adults with SCD should focus on supporting occupational experience and participation by addressing knowledge, skills, beliefs, and emotional regulation.
Plain Language Summary
Some older adults notice memory problems, even though they do not have dementia or any other medical condition. This is known as subjective cognitive decline (SCD). Individuals with SCD sometimes withdraw from some of their social and leisure activities. This raises concern because staying involved in such activities is important for older adults’ health and well-being. The reasons behind this withdrawal are not well understood. In this study, occupational therapists who work with clients with SCD shared their insights about everyday issues they address. The occupational therapists observed that individuals with SCD may stop participating in activities the know are beneficial for their health, or they may continue doing them but find the activities less enjoyable or rewarding. For example, they may feel less pleasure, reduced connection with others, or a sense of incompetence. The occupational therapists identified several reasons for these changes in activity participation. Personal reasons were subtle (but normal) memory changes, not using helpful strategies, strong negative emotions like shame, and a loss of confidence. Other reasons involved the social environment, and included lack of support from family members or negative self-perceptions about aging and memory problems. Understanding these challenges and causes can assist occupational therapists in developing effective methods to support individuals with SCD in remaining engaged in meaningful activities that promote health and well-being.
Keywords
Introduction
Subjective cognitive decline (SCD) is the persistent experience of decline in cognitive capacity not detected by standardized cognitive tests (Jessen et al., 2020). SCD affects an estimated 25% to 60% of older adults with normal cognition (Röhr et al., 2020). Older adults (typically age 65+) with SCD are twice as likely to develop mild cognitive impairment or dementia (Pike et al., 2022). SCD is also associated with higher symptoms of depression and anxiety (Montejo Carrasco et al., 2020), and poor quality of life (Pavel et al., 2023).
Although older adults with SCD are generally independent (Roehr et al., 2019), they report everyday cognitive lapses, such as trouble retrieving names or words, following conversations, maintaining focus while reading, and navigating unfamiliar environments (Buckley, Ellis, et al., 2015; Kiene et al., 2025). Furthermore, older adults with SCD identified many daily activities they considered important but were not engaging in as often or as successfully as they wished (Rotenberg et al., 2022). Cognitive lapses or challenges in everyday life can trigger strong emotional responses such as frustration, embarrassment, sadness, and anxiety, often explained by a fear of developing dementia, and the stigma related to it (Kiene et al., 2025; Miebach et al., 2019).
Repeated cognitive lapses and embarrassment, particularly in social contexts, can lead to avoidance behaviors (Kiene et al., 2025). Older adults with SCD reported withdrawing from physical, social, or leisure activities (Rotenberg, Maeir, et al., 2020; Wion et al., 2019), a concerning trend, because social-leisure participation is associated with reduced dementia risk (Duffner et al., 2022; Sommerlad et al., 2023), better mood, and greater well-being (Fancourt et al., 2021; Yen et al., 2024). From an occupational therapy perspective, this is especially concerning because participation in meaningful activities is foundational to growth and well-being across the life span (Hooper & Wood, 2024). Participation and performance challenges may also disrupt occupational identity—self-perceptions shaped by what people do and how they evaluate their competence in doing (Ocasio Hansson et al., 2022). Such disruptions are evident in reports from older adults with SCD, who describe cognitive lapses as undermining their perceptions of competence in major life roles such as parenting or volunteering (Miebach et al., 2019; Rotenberg, Sternberg, et al., 2020).
In the absence of effective drug treatments for dementia, prevention in older adults with SCD focuses on healthy lifestyle interventions (Livingston et al., 2024), such as physical activities, social engagement, cognitively stimulating activities, nutrition, and stress management (O’Connor et al., 2021). Systematic reviews found small but significant cognitive benefits, yet they rarely translate to everyday cognitive mistakes, self-perceptions, or stress (Meng et al., 2022; Yu et al., 2024). Furthermore, older adults experience challenges maintaining their participation once intervention programs end (Timmons et al., 2020). To support sustained participation of older adults with SCD in healthy lifestyle activities, there is a need to develop interventions based on a deep understanding of the personal and environmental factors that affect their participation. This article describes the first step of developing an intervention that meets this need, using the six-step Intervention Mapping approach (Fernandez, Ruiter, et al., 2019). This step aims to identify a key behavioral problem and its determinants, and develop a logic model of the problem to guide intervention planning. Subsequent steps, reported elsewhere, will be defining program outcomes and objectives; selecting theory-based methods and practical applications; designing and producing the program materials; initial acceptability testing of the intervention; and developing an evaluation study. These steps will be reported elsewhere.
As the initial step in developing a health-promotion intervention for older adults with SCD, this study examined participation-related challenges and their determinants, from the perspectives of occupational therapists (OTs). OTs play an important role in understanding participation challenges, using a functional-cognition lens to assess how cognitive abilities interact with task demands, personal characteristics, and social and physical environments to shape performance and participation (Wesson & Giles, 2019). They also consider how beliefs, attitudes, and emotional states influence participation across diverse daily activities and contexts (Toglia & Foster, 2021).
The study aimed to explore OTs’ perspectives on participation-related and other daily-life challenges experienced by older adult clients with SCD, and the personal and environmental determinants they perceive to explain these challenges. Following the Intervention Mapping approach, the study also aimed to create a logic model of the problem, using the findings to outline key behavioral problems related to participation, and their determinants (Fernandez, Ruiter, et al., 2019).
Methods
Study Design and Procedures
We used a qualitative description study design (Doyle et al., 2019), with a deductive content analysis (Mayring, 2023) of data collected through focus groups with OTs. A qualitative description design is used to describe patterns and trends in participants’ perceptions, and is highly appropriate in health care areas where limited knowledge exists (Doyle et al., 2019). Ethics approval was obtained (Hebrew University No.14122022), and all participants provided informed consent prior to the focus groups. Focus groups were recorded directly to a secure hard drive using Zoom, and transcribed verbatim. De-identified transcripts were securely stored and video files deleted after coding.
Participants
Participants were 15 OTs (14 women, one man), with at least 1 year of experience working with older adults with SCD (mean 16.3 ± 8.2 years, range 5–30). Eligibility criteria were: (a) registered OT; and (b) confirmed having at least 1 year of clinical experience with older adults who self-reported cognitive decline but scored within normal range on cognitive tests.
Participants were recruited through convenience and snowball sampling, using professional social media groups, and the researchers’ professional networks. Interested individuals contacted the first author and were screened by phone. No employment or power relationships existed between researchers and participants. Participants worked in outpatient geriatric or memory clinics (n = 8), homecare (n = 5), or senior centers (n = 2). all in medium-large cities in central Israel.
Data Collection
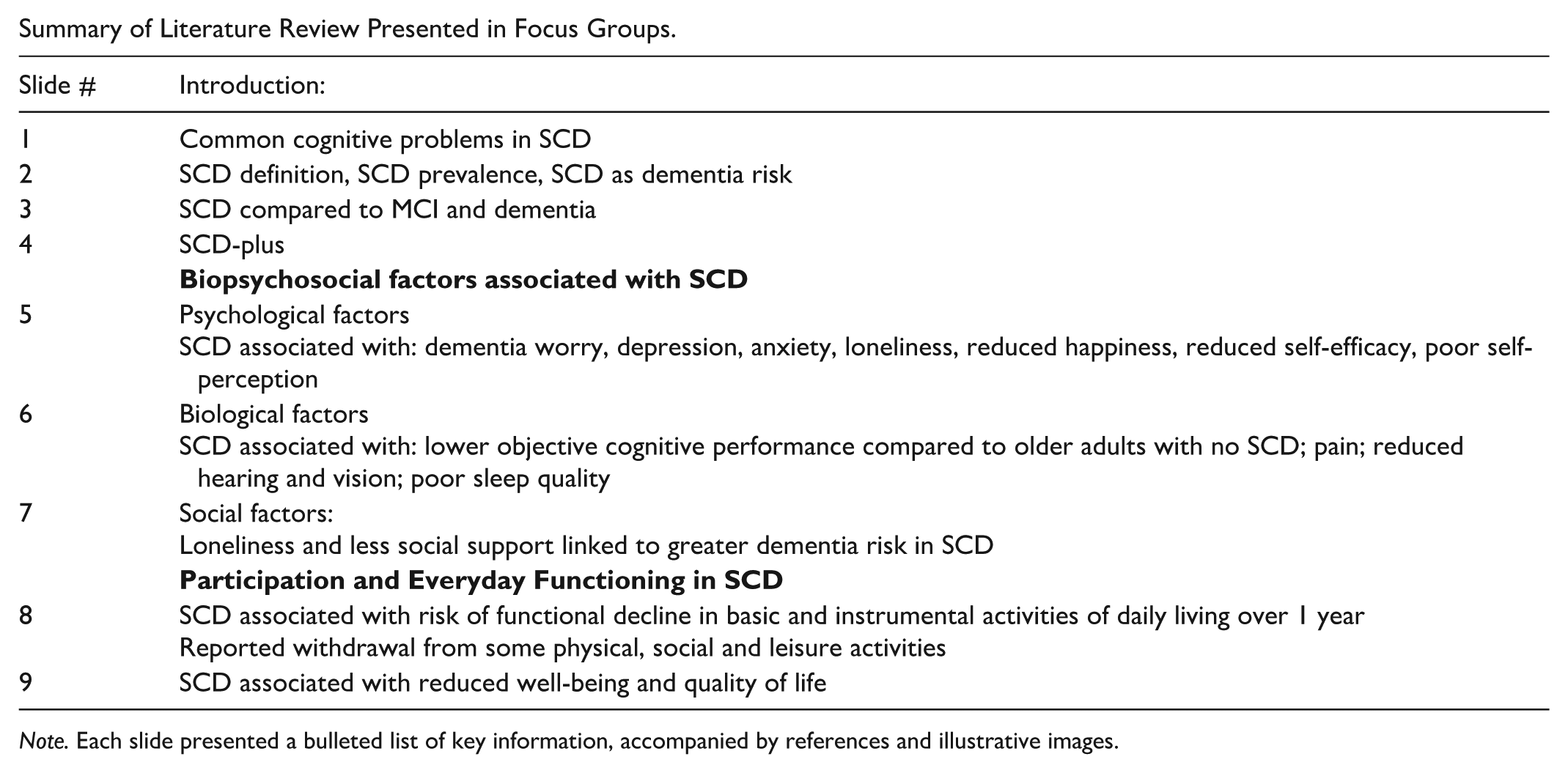
Two identical two-hour focus groups, each with 6-8 participants, were conducted via Zoom (Version 6.3.11) in January 2023, facilitated by MA. A two-part semi-structured question guide (Figure 1) was used to explore participation challenges of older adults with SCD, with a brief literature-based presentation (Appendix) between the two parts. The presentation summarized biopsychosocial factors associated with participation in SCD, linking them verbally to determinants raised by participants in Part 1, to ensure all potential determinants were considered before discussing priorities in part two of the focus group.
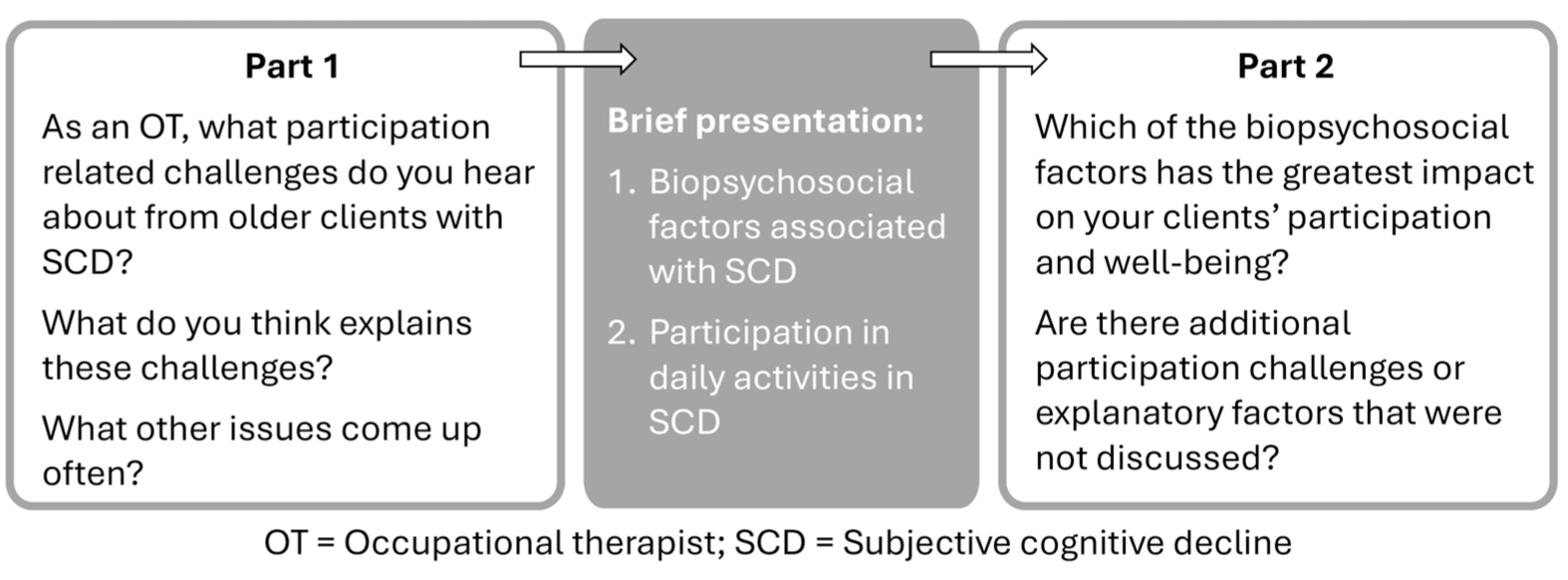
Focus Group Question Guide.
Data Analysis
The transcripts were coded deductively, using the Theoretical Domains Framework (TDF) and the Capability, Opportunity, Motivation- Behavior (COM-B) model (Cane et al., 2012; West & Michie, 2021). The TDF consolidates key behavioral theories into 14 domains encompassing cognitive, emotional, social, and environmental factors that influence human behavior (Atkins et al., 2017), organized under three components of the COM-B model which explain behavior (West & Michie, 2021). Table 1 presents definitions of the COM-B components and relevant TDF domains. We selected the COM-B model and the TDF because they provide a comprehensive yet practical approach to analyzing behavior and its determinants in health contexts, and are often used within the Intervention Mapping approach (Fernandez, ten Hoor, et al., 2019).
COM-B Model Component: Definitions and TDF Domains.
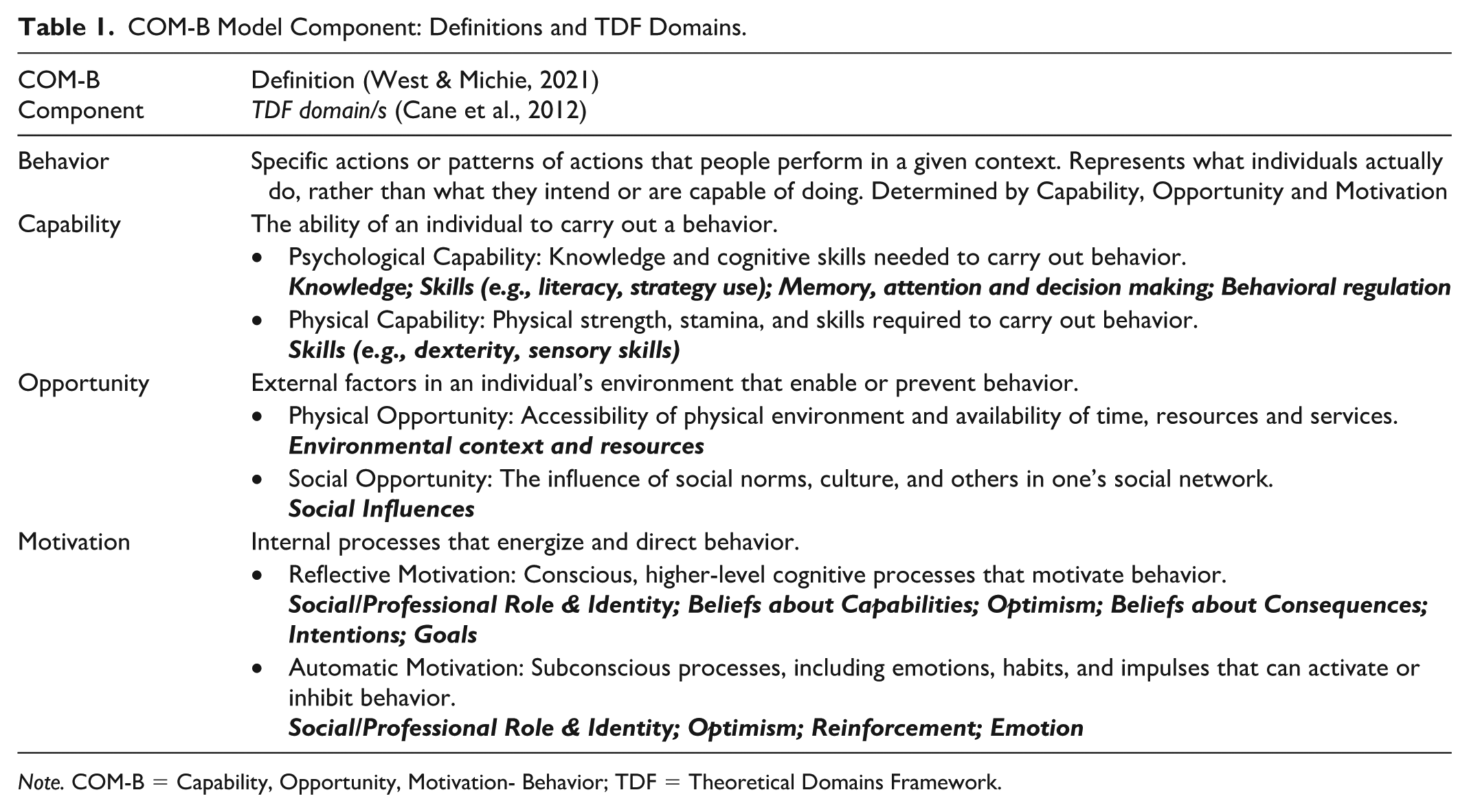
Note. COM-B = Capability, Opportunity, Motivation- Behavior; TDF = Theoretical Domains Framework.
We coded the data on Excel using TDF domains as codes, each nested under the relevant COM-B component, using operational definitions from Atkins et al. (2017). We mapped data to TDF domains rather than to the more granular constructs nested within each domain (e.g., self-efficacy under Beliefs about capabilities) because the literature provides operational definitions only at the domain level, and pilot coding using the constructs showed substantial conceptual overlap among them. MA conducted the initial coding. AM and SR independently reviewed this coding and noted areas of disagreement, which were discussed in team meetings, where coding was iteratively refined until consensus was achieved. The logic model of the problem, outlining the behavioral problem, its determinants, and possible relationships among them, was developed through further team discussions of the data and theoretical and empirical literature. An audit trail was maintained throughout both processes by retaining previous versions of the coding table and logic model, along with notes summarizing discussions and rationale for decisions.
Results
Select quotes demonstrating the findings are presented in Table 2. The OTs described two main participation challenges among clients with SCD. The first was insufficient participation in healthy lifestyle activities, reflected in withdrawal from previously enjoyed social and leisure activities, difficulty identifying activity options, and challenges following through on intentions to participate. The second was negative occupational experiences, referring to the subjective experiences occurring during and/or after participation (Budman & Zaguri-Vittenberg, 2025). OTs observed that clients often expressed reduced sense of competence and frustration with their performance. They also noted that clients chose activities based on health recommendations, rather than on the quality of their experience. As a result, they encountered difficulty sustaining participation in activities that were not enjoyable, interesting, or meaningful. The two participation challenges correspond to the behavior component of the COM-B model, reflecting observable behaviors and reported experiences of these behaviors.
Select Quotes Reflecting the Behavioral Problem and its Determinants.
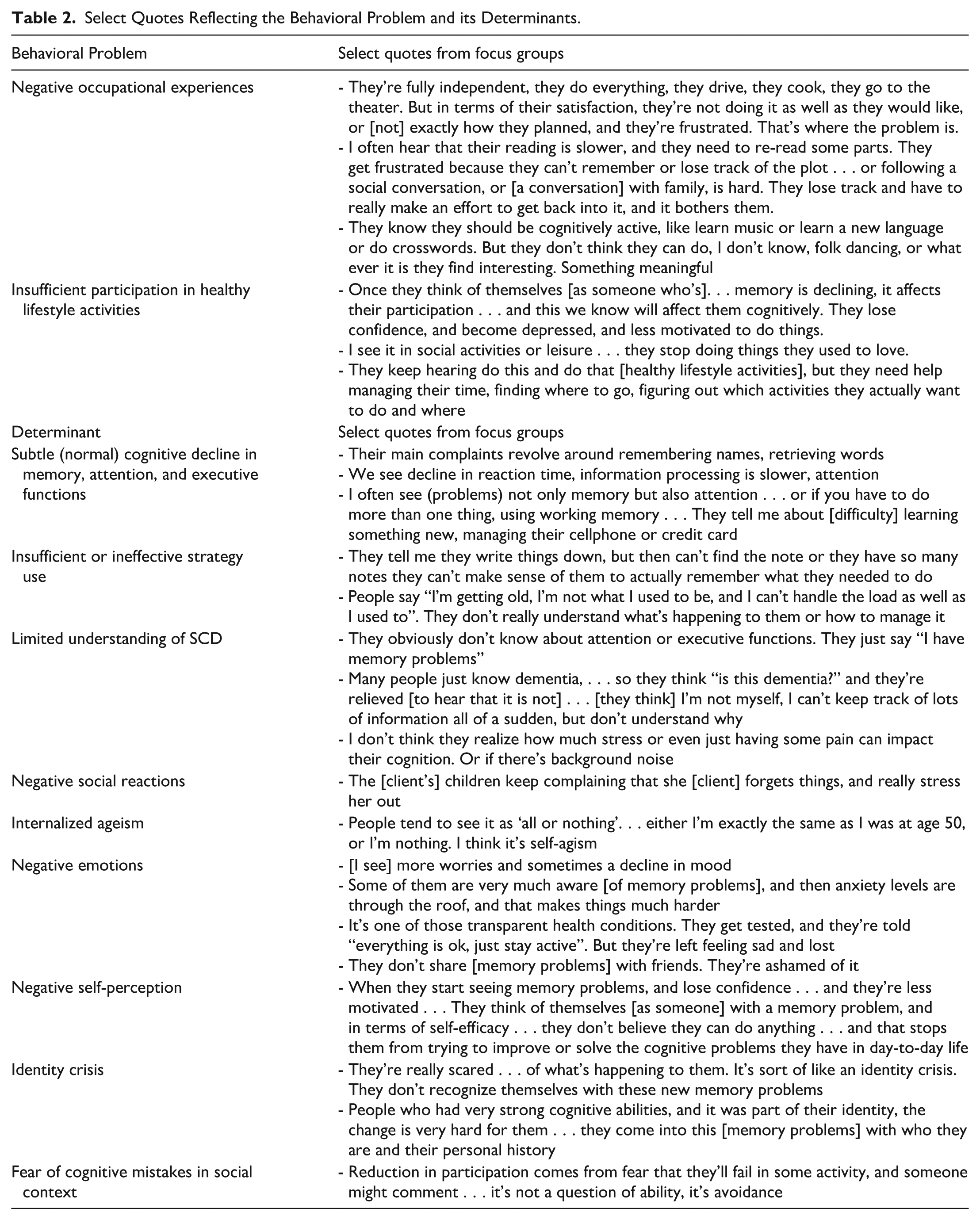
We found determinants of the participation challenges related to all three COM-B components that explain behavior. The OTs described three determinants under psychological capability. First, they described cognitive lapses or mistakes in in everyday life, which they understood as indicating subtle cognitive decline despite normal performance on cognitive tests (TDF domain: Memory, Attention and Decision process). They reported that clients experienced challenges related to memory (e.g., retrieving names, words, or information), processing speed (e.g., following a conversation), attention (e.g., following a book plot), and executive functions (e.g., managing multi-step tasks). Second, OTs indicated that their clients demonstrated insufficient or ineffective strategy use (TDF domains: Behavioral Regulation; Skills), using a calendar but failing to check it regularly, making disorganized lists and notes that were not helpful retrieving information. Third, the OTs thought that their clients had limited understanding of SCD (TDF domains: Knowledge). Clients were confused about how SCD differs from dementia, had limited knowledge about cognitive processes other than memory that can contribute to mistakes in everyday life, and limited awareness of personal and environmental factors that influence cognition (e.g., pain, fatigue, or noise).
In terms of social opportunity, OTs described how criticism, impatience or other unsupportive responses from others (TDF domain: Social influences/support) contributed to stress, shame, and feelings of isolation. OTs noted that some clients internalized ageist beliefs (TDF domain: Social influences/norms), expressed through feelings of worthlessness related to the cognitive decline they experience, and through the use of harsh self-deprecating language (e.g., the clients referred to themselves as stupid or unreliable).
Regarding automatic motivation, the OTs described strong negative emotional responses (TDF domain: Emotion), including worry or fear of dementia, embarrassment, frustration, shame, and grief. OTs observed clients in immense emotional distress, often too ashamed to discuss their cognitive lapses with others, which left them feeling socially isolated.
Under reflective motivation, the OTs described negative self-perceptions among their clients (TDF domain: Beliefs about capability), including low confidence and self-efficacy. OTs attributed this to clients’ limited understanding of SCD described above, which hindered their ability to anticipate and manage mistakes. OTs further described an “identity crisis” (TDF domain: Identity), in which clients struggle to reconcile the cognitive decline they experience with their sense of self, particularly when cognitive ability had been central to their identity. The participants noted that clients’ fear of embarrassment or negative reactions from other people when mistakes occur in social contexts (TDF domain: Social identity) sometimes led to activity avoidance.
Based on these findings, we developed the logic model of the problem–theoretical model of participation in older adults with SCD (Figure 2). The model outlines how subtle (within norms) cognitive decline, combined with ineffective strategy use, can lead to recurring mistakes that trigger negative emotions and self-perceptions. These emotions and self-perceptions are often intensified by internalized ageist attitudes, or through real or perceived negative responses from others. Together, they create a cycle of shame, self-criticism, and a disrupted sense of self. The psychological toll can deter individuals from engaging in healthy lifestyle activities, especially when performance issues lead to negative experiences. Even with awareness of the benefits of such activities, motivation may decline if activities consistently cause distress. The model further suggests that negative occupational experiences and withdrawal from participation can reinforce negative emotions and self-perceptions.
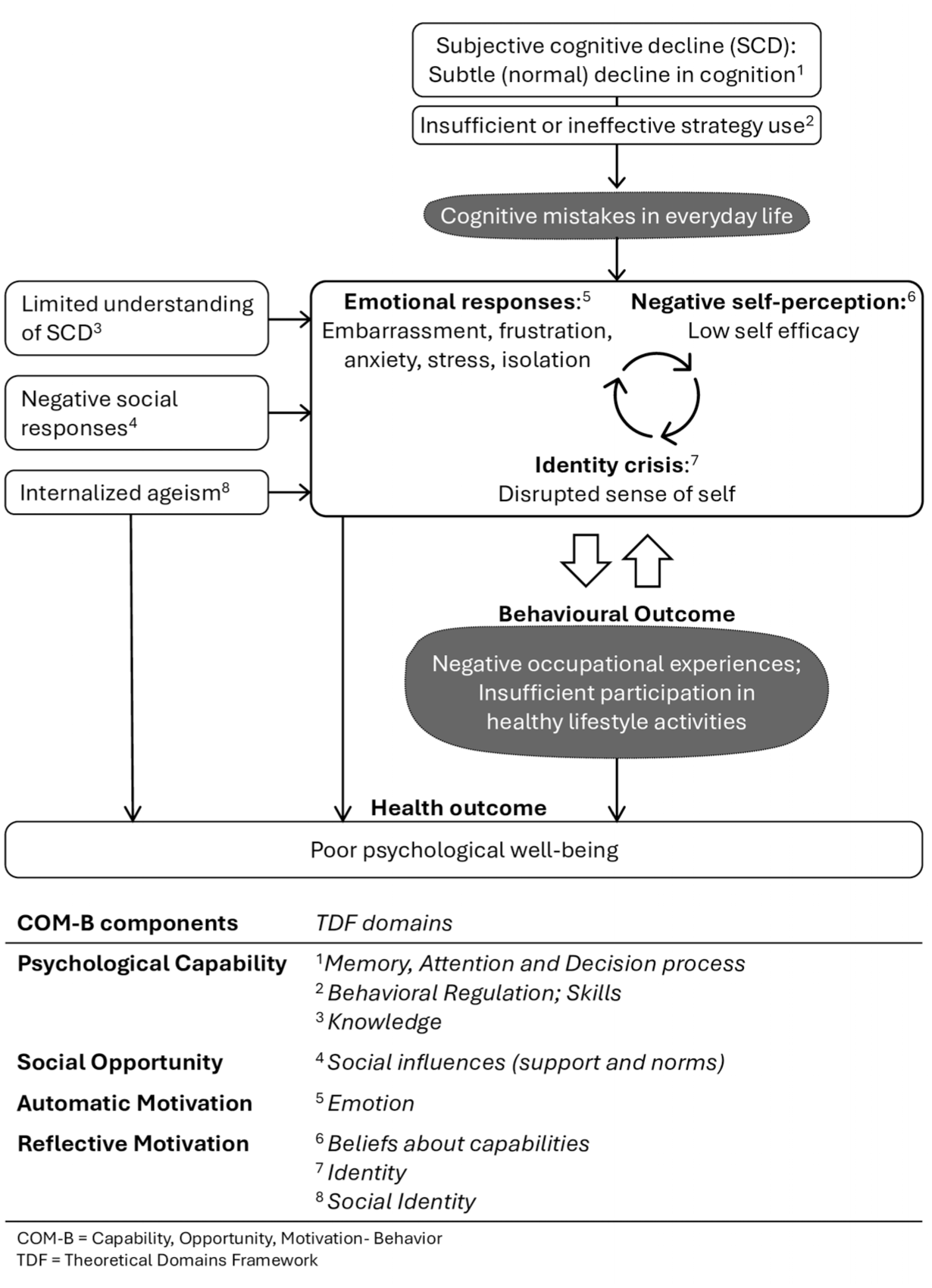
A Theoretical Model of Participation in Older Adults with SCD.
Discussion
This study explored participation challenges faced by older adults with SCD, and the personal and environmental factors that contribute to them. Using focus groups with OTs, we identified two key challenges: limited participation in healthy lifestyle activities and negative occupational experiences. Our analysis revealed determinants related to psychological capability (cognition, behavioral regulation, skills, knowledge), social opportunity (support and norms), automatic motivation (emotions), and reflective motivation (beliefs about capabilities, identity, and social identity). We developed a theoretical model illustrating how these determinants interact to shape the behavioral outcomes of reduced participation and undesirable occupational experience.
Behavioral Challenges: Participation and Occupational Experience
OTs described two key behavioral challenges. The first was decreased participation, where clients withdrew from meaningful activities they used to enjoy, and/or struggled to initiate new ones. Decreased participation was reported in previous research, showing reduced physical, social and leisure activities among older adults with SCD (Lee & Foster, 2023; Rotenberg, Maeir, et al., 2020). The second behavioral challenge was continued participation in activities that do not provide desirable occupational experiences. The OTs suggested that negative experiences are related to clients’ dissatisfaction with their current performance, causing frustration and stress, and emphasized the importance of finding activities that provide positive occupational experiences.
Occupational experience is central to health and well-being (Budman & Zaguri-Vittenberg, 2025). In older adults, negative experiences may contribute to withdrawal, whereas enjoyable, socially rewarding activities are more likely to be sustained (Meredith et al., 2023). While lifestyle interventions for SCD typically target participation frequency or duration (Meng et al., 2022), our findings highlight the need to also address occupational experience to promote sustained engagement and psychological well-being.
Desirable occupational experiences can be achieved by intentionally planning how to engage in activities. (Kuo, 2011). OTs may use guided reflection on past and current experiences to enhance clients’ awareness of personal and contextual factors shaping their experiences and develop strategies to cultivate more desirable ones (Kuo, 2011). Reflection on occupational experiences helped clients in a psychiatric unit plan activities and contexts that support their desired occupational experiences (Bailliard et al., 2021). Reframing provides an additional strategy for enhancing occupational experience (Kuo, 2011), for example by helping older adults with SCD shift focus from word-finding challenges in a conversation, to the social connection it afforded (Budman & Zaguri-Vittenberg, 2025).
Psychological Capability
OTs described lapses in everyday cognition caused by subtle (normal) cognitive decline, compounded by limited or ineffective compensatory strategies. Evidence of subtle cognitive decline can be found in reports that older adults with SCD perform worse than peers without SCD on measures of memory, executive function, and language (Wolfsgruber et al., 2020), although these findings are mixed (Zhou et al., 2024). Functional cognition assessments offer additional support, showing that older adults with SCD reported more everyday cognitive mistakes than a normative age-matched sample and performed significantly worse on an observation-based assessment of a complex real-world shopping task (Rotenberg & Dawson, 2022).
OTs also observed a limited understanding of SCD among their clients, and ineffective strategy use, consistent with evidence that older adults often rely on incidental recall or persist with ineffective strategies (Hertzog et al., 2019). These issues may reflect impaired self-awareness of older adults with SCD. Self-awareness includes general awareness (metacognitive knowledge of abilities, task demands, and strategy use) and online awareness (or real-time monitoring of performance); both can vary across domains and contexts (Toglia & Foster, 2021). By definition, individuals with SCD demonstrate self-awareness of everyday consequences of cognitive decline (Jessen et al., 2020), reporting word-finding, attention, or navigation difficulties (Buckley, Saling, et al., 2015; Kiene et al., 2025). However, as the OTs observed, older adults with SCD may lack awareness of the cognitive processes, task demands, and contextual factors that impact cognitive functioning (Rosenberg et al., 2020). Older adults with SCD exhibited poor online awareness, misjudging their performance in memory tasks (Cappa et al., 2024), and offering vague accounts of their cognitive mistakes, lacking contextual detail (Buckley, Ellis, et al., 2015). Poor online awareness leads to inaccurate anticipation of task demands and failure to recognize the need for strategy use (Toglia & Foster, 2021), which can explain the OTs’ observations of ineffective strategy use. OTs are well positioned to design interventions that target self-awareness of older adults with SCD, using psychoeducation about cognitive processes, and structured reflection on everyday experiences to link lapses with underlying mechanisms and contextual influences (Toglia & Foster, 2021). Enhancing self-awareness is an essential component of interventions aimed at supporting strategy acquisition (Giles et al., 2024) in older adults with SCD.
Automatic Motivation and Social Opportunity
The OTs described high levels of stress, decreased mood, and negative emotions (e.g., shame, anger and frustration), among their clients, similar to emotions reported directly by older adults with SCD (Kiene et al., 2025; Miebach et al., 2019). Such emotions are linked to poorer functioning and leisure participation in older adults with SCD (Fox et al., 2025), confirming their role as participation determinants. Negative emotional responses to everyday cognitive mistakes likely stem from fear of dementia (Buckley, Saling, et al., 2015), rooted in social stigma that devalues older adults with cognitive impairments (Barber, 2017; Jaggers et al., 2022). This is understandable given that older adults described dementia as a tragic condition marked by loss of autonomy, identity, dignity and humanity (Marhánková & Honelová, 2024). Fear of dementia is linked with more self-reported memory problems and depressive symptoms (Divers et al., 2022), which may reflect a tendency to catastrophize or ruminate on minor cognitive lapses, and interpret them as signs of dementia, with negative emotional consequences (Barber, 2017). Interventions for older adults with SCD should focus on challenging internalized social stigma, and providing emotional regulation strategies.
Reflective Motivation and Social Opportunity
Our findings echo reports of poor self-perceptions and diminished self-efficacy in older adults with SCD (Lucas et al., 2016). These negative self-views likely arise from repeated stress related to cognitive lapses (Hughes & Touron, 2021), and are reinforced by internalized social norms that place high value on cognition as central to identity (Jaggers et al., 2022). With these views, cognitive decline can become a threat to sense of self (Buckley, Saling, et al., 2015), as observed by our participants.
Age-based stereotype threat provides one explanation for the link between minor lapses, dementia-related worry, and distress; when aging stereotypes (e.g., “older adults are forgetful”) become salient, they elicit anxiety and constant self-monitoring, deplete cognitive resources, and impair performance (Barber, 2017). Interpreting mistakes through this lens reinforces stigma and perpetuates a cycle of stress, reduced performance, and further stigma. Stereotype threat not only impairs cognition in the moment but also undermines perceived functioning and self-efficacy (Bouazzaoui et al., 2016).
Stress from cognitive errors may also lead to avoidance coping, where older adults withdraw from activities to prevent embarrassment or other negative emotions (MacAulay et al., 2024). Although avoidance offers temporary relief, it can ultimately lead to increased distress and lower quality of life (MacAulay et al., 2024). Interventions to support participation should therefore target internalized stigma and foster internal motivation for continued engagement.
A Cycle of Biopsychosocial Determinants of Participation
Our findings suggest that the experience of cognitive decline in older adults with SCD perpetuates a harmful cycle involving cognitive, emotional, perceptual and social factors leading to reduced participation and poor occupational experiences. As an example, anxiety, negative self-beliefs, and internalized ageism were shown to increase focus on cognitive errors, amplifying the perceived frequency and severity of these mistakes. This leads to impaired self-perception, thereby reinforcing anxiety and negative beliefs in a self-sustaining feedback loop (McWhirter et al., 2020). Particularly concerning is the role of cognitive anxiety sensitivity– i.e., the fear of experiencing anxiety related to cognitive failures. This fear was found to predict worse subjective perceptions of cognitive abilities, and withdrawal from everyday activities (Divers et al., 2022). This suggests that after experiencing distress due to cognitive challenges, older adults may avoid meaningful activities out of fear of recurrence of distress, with detrimental implications to their health and well-being.
Study Limitations
Most participants in our sample worked in medium-to-large cities, limiting transferability of findings to remote areas. Data collection was limited to OTs, while including perspectives of other health care professionals and older adults with SCD may have provided additional insight. Furthermore, the small sample reflects pragmatic recruitment within a specialized population, which may restrict breadth across settings and roles. While no new ideas emerged in the second focus group, broader sampling might have added nuance. We also acknowledge that including a presentation half-way through the focus groups may have influenced later responses. Finally, the absence of intercoder agreement calculations and participant validation may have reduced analytic rigor.
Conclusions
This study offers new insight into participation challenges of older adults with SCD, and emphasizes the importance of addressing both participation and the quality of occupational experiences. OTs can play a central role by supporting older adults with SCD in planning healthy lifestyle activities that provide a sense of competence, meaning, or social connection. Desirable occupational experiences can support sustainable participation in healthy lifestyle activities, promoting cognitive health and well-being. The proposed theoretical model illustrates how personal and environmental contexts interact to shape participation and occupational experience. By describing determinants of meaningful participation and well-being, the model suggests mechanisms of change OTs can leverage, including providing knowledge, promoting strategy use (e.g., compensatory problem-focused strategies, stress management, and emotion regulation), reframing perceptions of cognitive mistakes, and normalizing SCD through peer support.
Footnotes
Appendix
Summary of Literature Review Presented in Focus Groups.
| Slide # | Introduction: |
|---|---|
| 1 | Common cognitive problems in SCD |
| 2 | SCD definition, SCD prevalence, SCD as dementia risk |
| 3 | SCD compared to MCI and dementia |
| 4 | SCD-plus |
|
|
|
| 5 | Psychological factors |
| 6 | Biological factors |
| 7 | Social factors: |
|
|
|
| 8 | SCD associated with risk of functional decline in basic and instrumental activities of daily living over 1 year |
| 9 | SCD associated with reduced well-being and quality of life |
Note. Each slide presented a bulleted list of key information, accompanied by references and illustrative images.
Acknowledgements
Not applicable.
Ethical Considerations
The study was approved by the Hebrew University Ethics Committee (No. 14122022).
Consent to Participate
Participants provided written informed consent, obtained electronically.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Maya Arieli’s postdoctoral fellowship was funded by the Sagol Master’s Program for Specialization in Healthy Aging.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability Statement
In accordance with ethics committee guidelines, full focus group transcripts cannot be shared outside the research team to protect participant confidentiality. Anonymized excerpts have been included in the manuscript. Additional excepts may be available upon reasonable request.