
Abstract
Culturally responsive care (CRC) is essential in occupational therapy (OT) to ensure equitable, relevant, and meaningful client engagement. The use of CRC in OT education and practice remains variable. We aimed to map how CRC is defined, implemented, and integrated in OT literature and to identify knowledge gaps. We systematically searched PubMed (NCBI), CINAHL (EBSCOhost), Scopus (Elsevier), and PsycINFO (ProQuest) using key terms related to OT and cultural responsiveness. Following Arksey and O’Malley’s framework, we charted and analysed 53 studies using the Health Standards Organization (HSO) Cultural Safety and Humility Framework. CRC was conceptualized across a spectrum from cultural competence to cultural humility, with strong engagement in community partnerships, especially with Indigenous groups. Although CRC is a recognized priority in OT, its application across training and service delivery remains limited, especially from the global south. Addressing these gaps is essential for equitable and accountable OT practice to maximize client satisfaction.
Plain Language Summary
Occupational therapy (OT) enables individuals to participate in meaningful occupations that they want to, need to, or are expected to do. To make service delivery effective, OT must respect the cultural identities and lived experiences of the people they serve. This review examined 53 studies on how occupational therapists consider cultural factors and tailor therapeutic services to meet the needs of their clients. We also examined whether occupational therapists are taught to consider cultural nuances from the outset of their professional training. The findings showed that many occupational therapists are actively collaborating with Indigenous communities and employing thoughtful, respectful approaches to make therapeutic services culturally relevant and appropriate for their clients. We found consistent efforts to deepen students’ and practitioners’ exposure to diverse cultures and their influence on clinical decisions across both training and post-professional development. However, there are some gaps. We observed that people from non-Western countries need to be more included in the research. Therapists and educators also need better tools and support to know if their efforts to be culturally safe are working. Currently, cultural responsiveness is often viewed as an individual skill rather than an integral component of health systems, education, or policies. To move forward, occupational therapists must embed cultural respect in every part of their work, from how students are taught to how services are delivered, ensuring care is safe, inclusive, and guided by the people it aims to serve.
Keywords
Introduction
A day-to-day experience for an occupational therapy practitioner involves engaging with clients from diverse cultural identities, values, and lived experiences to deliver high-quality, person-centred care (Rios-Vega et al., 2025). In recent times, culturally responsive care (CRC) has emerged as a central tenet for ensuring equitable access to and outcomes in health care for the diverse clients we serve. CRC refers to the capacity of health care providers to acknowledge, understand, and effectively respond to cultural differences in ways that affirm the dignity and preferences of individuals receiving care (Beach et al., 2005; Truong et al., 2014). It enables professionals to think beyond mere cultural awareness by actively adapting care to align with the social, linguistic, and belief systems of the client, thereby fostering trust, enhancing satisfaction, and improving therapeutic outcomes (Betancourt et al., 2003).
Culture plays an important role in OT, influencing how individuals perceive their health, engage in daily activities, and participate in meaningful occupations (Malkawi et al., 2020). Occupational therapy practitioners strive to support people in performing and engaging in meaningful everyday activities. Human occupations are often deeply rooted in culture (Hammell, 2009). Hence, the effectiveness of OT interventions is closely tied to the practitioner’s ability to deliver culturally relevant and responsive services. The effectiveness of OT services is often tied to factors such as language, religious or spiritual beliefs, family structures, gender roles, and historical or societal influences that our clients bring with them (Liu et al., 2021). The Canadian Association of Occupational Therapists affirms that understanding the client’s cultural context is essential to delivering practical, holistic, and client-centred services (Canadian Association of Occupational Therapists [CAOT], 2024).
Although CRC is widely acknowledged within the OT literature, there remains variability in how this concept is understood and operationalized across education and practice (Gerlach, 2012; Restall & Egan, 2021). For example, the Person-Environment-Occupation (PEO) model provides a foundational framework for understanding the interaction of clients with their environments (Law et al., 1996). However, its application often lacks explicit integration of cultural dimensions. Narrative and client-centred approaches typically emphasize respect for individual life stories and values. However, these approaches may fall short if cultural worldviews and community perspectives are neglected during intervention planning (Iwama et al., 2009).
Demographic shifts and changing social dynamics in many regions worldwide have made cultural responsiveness even more relevant (Crown-Indigenous Relations and Northern Affairs Canada, 2015; Dumont et al., 2025). However, there remains a limited, albeit growing, understanding of how CRC is defined, taught, and practised in OT in a way that reflects this diversity (Jeffery, 2005; Kinébanian & Stomph, 2010). Also, inconsistencies in curriculum content, the absence of unified frameworks for culturally responsive OT practice, and limited research evaluating CRC outcomes in OT interventions have been suggested to contribute to these gaps in knowledge and practice (Beagan & Chacala, 2012; Demers et al., 2021).
Hence, this scoping review was undertaken to (a) explore how CRC is defined or described in OT literature; (b) identify key practices, strategies, and frameworks used by occupational therapists to implement CRC; (c) examine how CRC is integrated into OT education, training, and professional development; and (d) highlight knowledge gaps that can guide future research.
Methods
We selected a scoping review method to identify knowledge gaps and characterize the breadth of the literature on CRC and OT (Arksey & O’Malley, 2005; Levac et al., 2010). The review process and results are reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR; Tricco et al., 2018) and the Joanna Briggs Institute (JBI) methodological guidelines (Peters et al., 2020), respectively.
Inclusion Criteria
We included peer-reviewed, empirical research or published opinion pieces in English from January 2000 to June 2025. Studies were included if they explicitly described OT practice and/or education addressing cultural responsiveness, safety, humility, or related concepts.
Article Search and Selection Process
Four databases were systematically searched, viz. PubMed (NCBI), CINAHL (EBSCOhost), Scopus (Elsevier), and PsycINFO (ProQuest). The search strategy was developed by the first four authors and validated with the help of a librarian to ensure comprehensive coverage (See Appendix I). We used the inclusion criteria described to search databases, and duplicates were removed. Further titles and abstracts were independently screened by two reviewers (PDL and AAG) prior to a full-text review. The full-text review was conducted by three authors (KTC, AG and NG) to promote rigour. In addition, we hand-searched the reference lists and citations of included studies; however, no additional articles were identified. Disagreements were resolved by common consensus. Data extraction was performed using a structured charting Excel sheet to capture study characteristics, OT practices, and alignment with cultural safety and humility principles. The data-extraction Excel sheet was piloted and refined based on feedback received from the coauthor (RCDR). No artificial intelligence tool was utilized across the conduct, analysis and writing of the study.
The research team acknowledged their professional backgrounds in OT and cultural safety, practising reflexivity throughout data collection and analysis to mitigate bias. Consultation with a cultural safety expert informed the adaptation and interpretation of the framework and findings. An iterative and reflexive process was undertaken to map and analyse the included studies. We adopted the Canadian Standard for Cultural Safety and Humility, developed by the Health Standards Organization (HSO; 2025) in collaboration with Indigenous partners. This framework was selected for its comprehensive, outcomes-based structure that articulates clear expectations for governance, leadership, workforce development, service delivery, and client engagement in promoting culturally safe health and social services. Its relevance extends beyond Indigenous populations to inform broader principles of equity, safety, and respect in cross-cultural practice (Occupational Therapy’s Commitment to Diversity, Equity, and Inclusion, 2020). This approach enabled the structured and meaningful synthesis of the literature, guiding the organization of findings into a narrative that aligns with key elements of the CRC.
Results
A total of 53 studies were included in this scoping review, encompassing a diverse range of cultural contexts, populations, and research methodologies. These studies were selected for their focus on CRC in OT, whether in practice, research, education, or systems-level analysis. Figure 1 shows a flowchart of the article section process and rationale for exclusion.
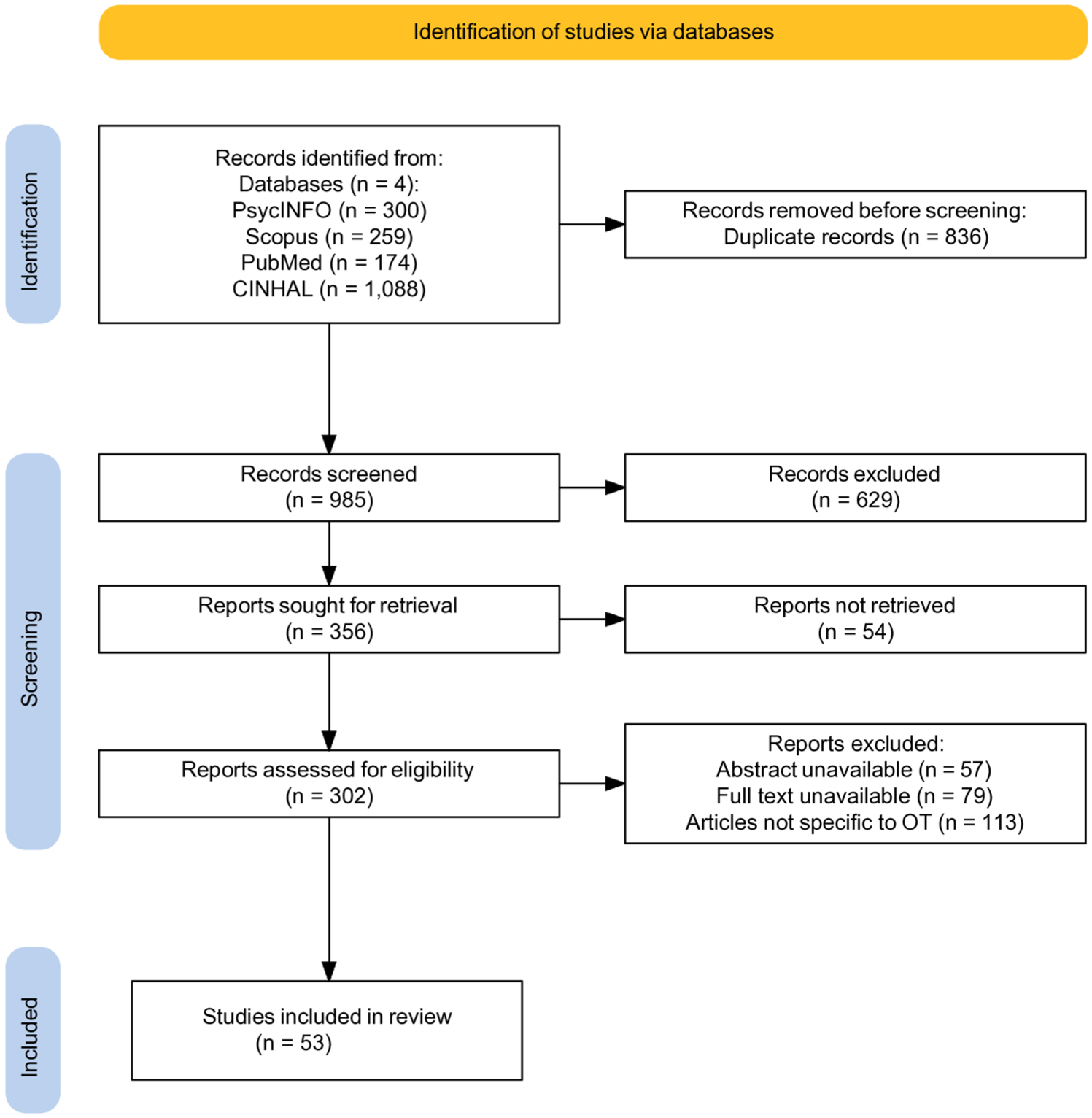
PRISMA Flow Diagram for Scoping Review Article Selection.
Geographically, Australia (n = 16; 30%), New Zealand (n = 10; 20%), and Canada (n = 10; 20%) accounted for the most significant proportion of the studies considered eligible for this review. Followed by the United States (n = 9; 18%), South Africa (n = 3; 7%), China (n = 1; 1%), Japan (n = 1; 1%), Vietnam (n = 1; 1%), Chile (n = 1; 1%), and Brazil (n = 1; 1%). These locations reflect regions where discourses on cultural safety, Indigenous sovereignty, colonization, and systemic oppression have been incorporated into OT scholarship and practice. Table 1 shows detailed information about each selected article.
Summary of Studies on CRC and OT.
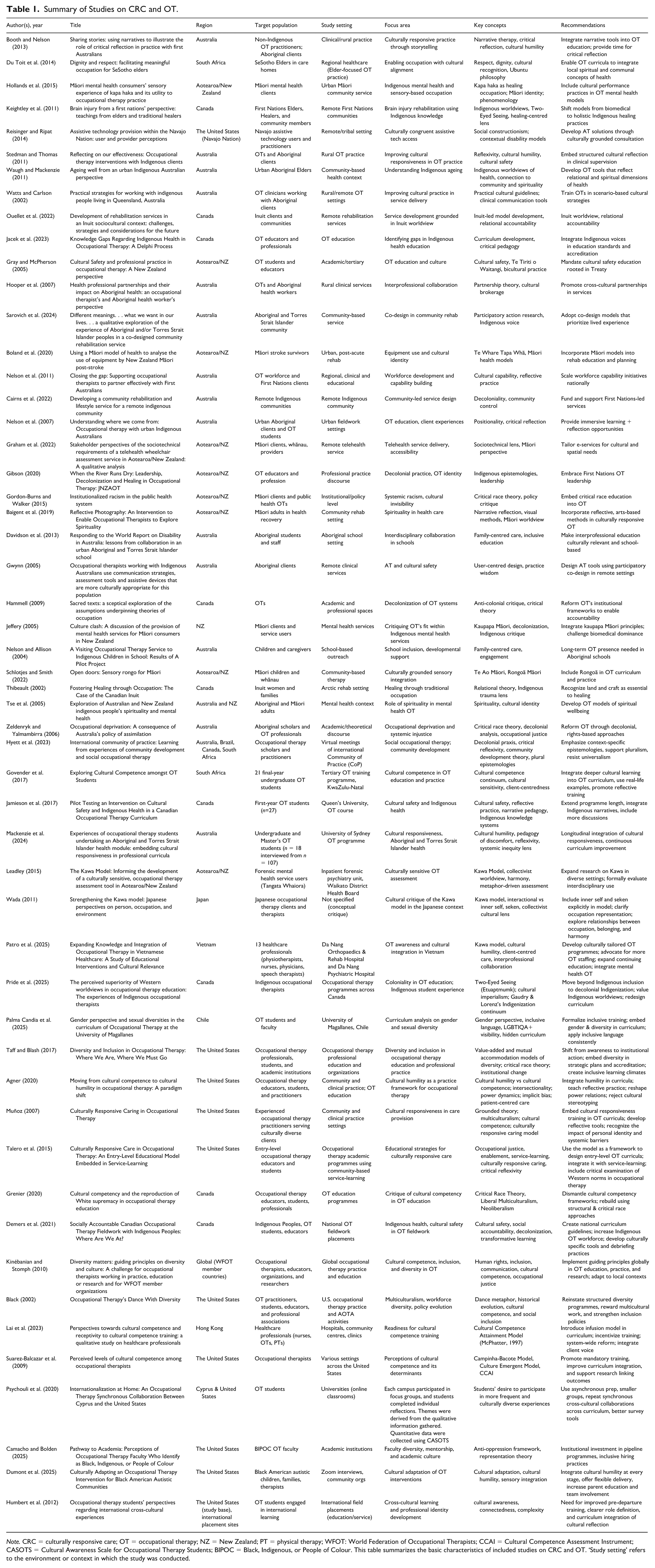
Note. CRC = culturally responsive care; OT = occupational therapy; NZ = New Zealand; PT = physical therapy; WFOT: World Federation of Occupational Therapists; CCAI = Cultural Competence Assessment Instrument; CASOTS = Cultural Awareness Scale for Occupational Therapy Students; BIPOC = Black, Indigenous, or People of Colour. This table summarizes the basic characteristics of included studies on CRC and OT. ‘Study setting’ refers to the environment or context in which the study was conducted.
Target populations spanned a variety of culturally and structurally marginalized groups. Indigenous communities were considered in 36 studies (68%), reflecting a strong scholarly and professional engagement with the legacies of colonization and pathways to self-determination (Baigent et al., 2019; Booth & Nelson, 2013; Cairns et al., 2022). Racialized and immigrant communities were represented in 12 studies (23%), and refugee and asylum-seeking groups were involved in four studies (8%; Davidson et al., 2013; Du Toit et al., 2014). Only two studies (4%) explicitly focused on the gender and sexual minority (GSM) population, primarily transgender and gender-diverse individuals (Palma Candia et al., 2025; Taff & Blash, 2017).
Defining and Describing CRC in OT
CRC was defined and conceptualized with varying degrees of depth across studies. Forty-one studies (77%) contributed to the definitions of CRC or related constructs, such as cultural safety, cultural humility, and cultural competence (Hammell, 2022). Terminological variations were observed, with ‘cultural safety’ being predominant in Canadian, Australian, and New Zealand contexts, whereas ‘cultural humility’ and ‘culturally responsive care’ were more commonly used in US-based literature (Foronda et al., 2016; Gwynn, 2005; Suarez-Balcazar et al., 2009; Talero et al., 2015). Hence, we propose a definition of CRC in OT as: A dynamic, relational, and client-centred approach that integrates clients’ cultural identities, values, lived experiences, and social contexts. CRC in OT involves the therapist being able to engage in critical self-reflection (Foronda et al., 2016), recognizing systemic inequities, and adapting practices to support equity and meaningful participation consistently (Muñoz, 2007). Grounded in cultural humility (Foronda et al., 2016), trauma-informed care and structural competence, CRC in OT should foster collaborative relationships and address power imbalances in care (Cairns et al., 2022; Davidson et al., 2013).
A key trend was the shift from competence-based models (centred on acquiring knowledge about ‘the other’) to relationship-centred approaches that emphasize reflexivity, address power imbalance, and strive for systemic transformation (Beagan & Chacala, 2012; Iwama et al., 2009). Definitions rooted in Indigenous frameworks emphasized client-determined safety, community knowledge, and the integration of traditional healing practices (Lavallee & Poole, 2009). Furthermore, 12 studies (23%) described CRC as rooted in human rights, anti-racism, and social justice, aligning with global efforts such as the Sustainable Development Goals (SDG 3, 10; United Nations Statistics Division, 2025, pp. 12, 28). These definitions consistently recognized culture as relational, dynamic, and inseparable from context.
Practices, Strategies, and Frameworks Used by Occupational Therapists
Thirty-eight (72%) studies described specific strategies and frameworks used by occupational therapists to implement CRC in practice (Gerlach, 2012; Hammell, 2022). These included both individual-level and systems-level approaches. At the practitioner level, common strategies included: Client-centred communication incorporating language access and cultural mediation; Incorporation of culturally meaningful occupations, such as land-based activities, traditional crafts, or gender-affirming roles (Lavallee & Poole, 2009); Use of spiritual or symbolic practices in therapeutic contexts, particularly in Indigenous and Elder community members (Du Toit et al., 2014). At the systems level, frameworks guided the design and evaluation of services. These included: The Kawa Model (Iwama et al., 2009; Wada, 2011), particularly in studies from Japan and multicultural immigrant contexts; The Canadian Model of Occupational Performance and Engagement (CMOP-E; Townsend & Polatajko, 2013), with cultural adaptations; The Te Whare Tapa Whā model, used in Māori health contexts; Participatory action frameworks emphasizing co-design and community governance (George et al., 2018; Gibson, 2020). However, only seven studies (13%) reported on the formal adoption of CRC monitoring tools, such as self-assessment rubrics or community-led audits (Beagan & Chacala, 2012; Gerlach, 2012). The use of critical theoretical frameworks, such as critical race theory, postcolonialism, or Indigenous epistemologies, was also limited, appearing in only 13 studies (25%; Gordon-Burns & Walker, 2015; Graham et al., 2022; Hammell, 2022).
Integration of CRC in OT Education and Professional Development
This review aimed to see how CRC is being integrated into OT education, training, and continuing professional development (CPD). Twenty-seven studies (51%) addressed this directly (Beagan & Chacala, 2012; Gerlach, 2012; Jamieson et al., 2017). Undergraduate curriculum innovations were described in 15 studies, with most incorporating modules on cultural competence/awareness, Indigenous health, or anti-racist practice (Gwynn, 2005). However, only six studies (11%) embedded CRC throughout the entire curriculum or described mechanisms for evaluation and student accountability (Boland et al., 2020; Fijal & Beagan, 2019; Hollands et al., 2015; Talero et al., 2015). Placement and experiential learning emerged as promising educational approaches (Hooper et al., 2007; Humbert et al., 2012). Nine studies (17%) described community-based placements in Indigenous, refugee, or marginalized urban contexts (Keightley et al., 2011; Melchert et al., 2016). These experiences for occupational therapy practitioners and students often led to self-reflection, increased awareness of systemic barriers, and encouraged the development of cultural humility (Nelson, 2009; Nelson & Allison, 2004; Nelson et al., 2007). However, support structures for students (especially those from minority backgrounds) were inconsistently described. In terms of CPD, 13 studies (25%) described training interventions specifically designed for practising therapists (Beagan & Chacala, 2012; Gerlach, 2012). These ranged from half-day workshops to multi-week community partnerships. Notably, the lack of educator preparedness and organizational buy-in were consistent challenges across the studies (Beagan & Chacala, 2012; Paluch et al., 2011; Pidgeon, 2015; Reisinger & Ripat, 2014). Professional associations and regulatory bodies were identified as key stakeholders in six studies, with authors advocating for the inclusion of mandatory CRC competencies in accreditation standards and licensing exams (Restall et al., 2016; Schlotjes & Smith, 2022; Silcock, 2020). The need to diversify faculty and decolonize teaching materials was also strongly emphasized, particularly in Canadian and New Zealand contexts (Fijal & Beagan, 2019; Hammell, 2022; Lavallee & Poole, 2009).
Mapping Findings to the Health Standards Organization (HSO) Cultural Safety and Humility Framework
Mapping is presented in Table 2. Using the HSO Cultural Safety and Humility Framework, five key domains were analysed across the included studies:
Mapping Findings to the Health Standards Organization (HSO) Cultural Safety and Humility Framework..
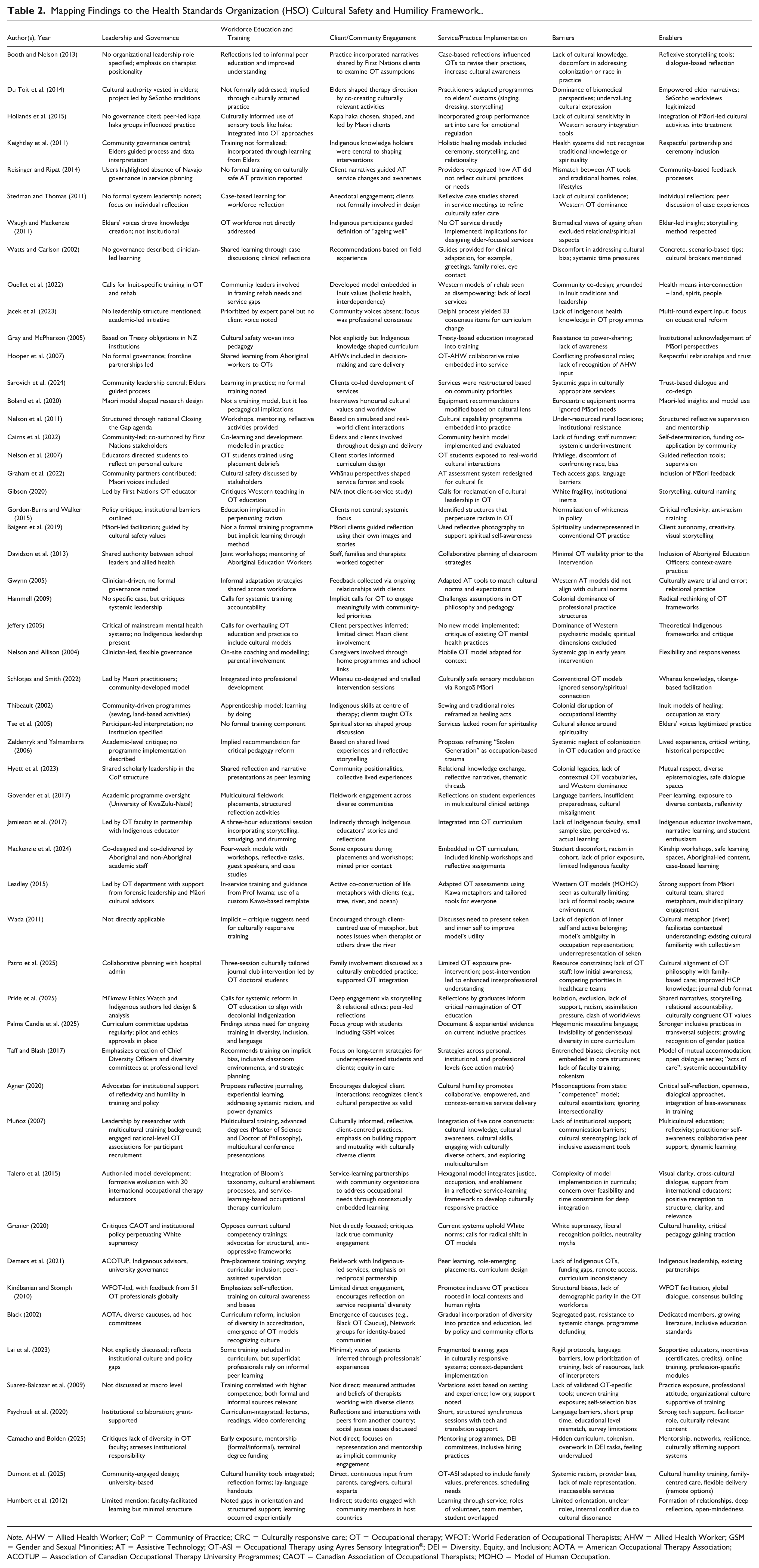
Note. AHW = Allied Health Worker; CoP = Community of Practice; CRC = Culturally responsive care; OT = Occupational therapy; WFOT: World Federation of Occupational Therapists; AHW = Allied Health Worker; GSM = Gender and Sexual Minorities; AT = Assistive Technology; OT-ASI = Occupational Therapy using Ayres Sensory Integration®; DEI = Diversity, Equity, and Inclusion; AOTA = American Occupational Therapy Association; ACOTUP = Association of Canadian Occupational Therapy University Programmes; CAOT = Canadian Association of Occupational Therapists; MOHO = Model of Human Occupation.
Leadership and Governance
Leadership and governance-related information was described in 14 studies (26%), though often as aspirational rather than operational features. Examples of indigenous-led governance models include a co-designed community rehabilitation service (Boland et al., 2020; Sarovich et al., 2024). These were aligned with the HSO emphasis on embedding cultural safety into the leadership and accountability structures of health care institutions. However, most education and service settings lacked formal structures to ensure indigenous or community oversight (Beagan & Chacala, 2012; Gerlach, 2012). For CRC to move beyond intention, future research and practice must articulate models of shared governance and indigenous authority in OT leadership (Stedman & Thomas, 2011; Thibeault, 2002).
Workforce Development and Training
Workforce development and training was one of the most robustly addressed domains, with 31 studies (58%) detailing professional development initiatives (Beach et al., 2005; Beagan & Chacala, 2012). Effective models featured long-term partnerships with communities, reflexive learning approaches, and the inclusion of cultural mentors or Elders in the training process (Lavallee & Poole, 2009). Self-awareness and critical reflection were foundational skills emphasized in almost all educational strategies (Tse et al., 2005). However, evaluation mechanisms and long-term impact assessments were rare, indicating a need for stronger systems of feedback, accountability, and organizational culture change.
Client and Community Engagement
Engagement with clients and communities was the strongest area of alignment with the HSO framework, discussed in 44 studies (83%; Gerlach, 2012). Approaches included co-design, narrative-based therapy, and culturally grounded assessment (Lavallee & Poole, 2009). Engagement was generally characterized by relational accountability, trust-building, and co-ownership. However, a few studies appeared to involve stakeholders in limited or advisory roles rather than in deeper, co-productive partnerships, a pattern that was more noticeable within institutional settings (Beagan & Chacala, 2012; Hammell, 2022).
Recognition of Rights, Trauma, and Racism
We had 26 studies (49%) that recognized rights, trauma, and racism-related domains with a focus on colonial trauma, intergenerational grief, anti-indigenous racism, and intersectional oppression (Gerlach, 2012). Recognition of rights was often linked to Truth and Reconciliation Commission (TRC) calls to action in Canada and the UN Declaration on the Rights of Indigenous Peoples (Restall et al., 2016). Few studies, however, operationalized rights-based frameworks into their practice tools or curricula (Ching et al., 2019). This highlights an implementation gap that future research and policy efforts must address (Hammell, 2022).
Safe Service Delivery
Safe service delivery strategies were found in 36 studies (68%). These included flexible care models, community-based services, and the incorporation of ceremony or traditional knowledge into therapy (Lavallee & Poole, 2009). However, structural barriers, such as funding models, western documentation practices, and a lack of cultural brokers, often undermined safety efforts (Gerlach, 2012). This domain was most successful when service delivery models were co-led, trauma-informed, and responsive to community feedback (Beagan & Chacala, 2012).
Identifying Key Gaps
This review identified gaps in the literature such as: Underrepresentation of GSM population, despite evidence of marginalization in health access; lack of structured implementation tools for CRC frameworks in OT (Beagan & Chacala, 2012; Gerlach, 2012); insufficient attention to Southeast Asian contexts, with only one study from Japan (Iwama et al., 2009) and none from other parts of Asia; limited exploration of power and privilege in OT education and regulation (Hammell, 2022); scarcity of research on the long-term outcomes of CRC education and practice interventions (Boland et al., 2020; Camacho & Bolden, 2025; Fijal & Beagan, 2019; Talero et al., 2015;). The findings indicate an urgent need for internationally diverse, critically grounded, and structurally embedded CRC frameworks in OT.
Discussion
This scoping review mapped 53 studies. We attempted to provide a comprehensive overview of how CRC is defined and its growing integration within OT education and practice through this review. Collectively, the findings present a rich yet uneven landscape, characterized by strong theoretical engagement in some domains and considerable gaps in others.
The included studies represented a range of multicultural contexts, with Canada, Australia, and New Zealand contributing the majority. This reflects the historical and ongoing centrality of Indigenous health equity in these regions and the relatively advanced integration of cultural safety discourse within their OT curricula, service models, and regulatory systems (Gray & McPherson, 2005; Nelson et al., 2011; Restall et al., 2016). Only a few studies came from South Africa, Brazil, and Japan. The Japanese study highlights how culture influences occupational models, such as the Kawa Model. There is still very little research from South and Southeast Asia. Studies from the Global South, especially from countries like India with deep cultural roots and a long history of colonization, should be encouraged to share their perspectives on occupation (Iwama et al., 2009; Leadley, 2015; Wada, 2011).
Conceptual Clarity
Approximately two-thirds of the included studies contributed to definitions of CRC or related constructs, such as cultural sensitivity, cultural safety, cultural humility, and cultural competence. These definitions ranged from skill-based approaches centred on knowledge acquisition to critical approaches grounded in reflexivity, anti-oppression, and Indigenous sovereignty (Booth & Nelson, 2013; Silcock, 2020). A consistent theme was the shift from competence towards humility (Agner, 2020), where culture is seen not as a fixed attribute of clients, but as a dynamic, relational process involving power, history, and identity. Importantly, only a few studies directly cited the HSO framework or similar policy instruments, indicating that its practical application remains nascent (Restall et al., 2016).
Practice Application
The findings revealed a spectrum of strategies used by occupational therapy practitioners to operationalize CRC. These included client-centred communication, the integration of culturally meaningful occupations, and the co-design of therapeutic goals and interventions. Notable practices included the inclusion of Elders in care teams, land-based OT approaches, and the adaptation of standard assessment tools to reflect cultural priorities (George et al., 2018; Hollands et al., 2015; Paluch et al., 2011). These strategies were most prominent in studies conducted in indigenous contexts. They echoed the findings of Meechan et al. (2024), which found that community partnerships and goal alignment with their values were central to culturally safe practice. However, the formalization of such strategies into scalable frameworks or evaluation tools was limited (Stedman & Thomas, 2011). Only a handful of studies described mechanisms to assess the effectiveness or consistency of CRC practices. This reiterates a disconnect between values and infrastructure (Meechan et al., 2024).
Educational Efforts
Workforce education and CPD interventions varied in scope and depth, from stand-alone modules to immersive placements in culturally diverse or indigenous communities (Ching et al., 2019; Govender et al., 2017; Grenier, 2020; Lai et al., 2023). These learning experiences emphasized self-awareness, relational ethics, and anti-racist praxis (Camacho & Bolden, 2025; Melchert et al., 2016). However, the extent of curriculum integration and institutional support remained inconsistent. Like Meechan et al. (2024), many studies have reported that student preparedness for culturally responsive practice is uneven, and faculty capacity to teach these concepts is variable (Nelson, 2009; Pidgeon, 2015). Community placements and reflective pedagogy have shown promise, but the lack of long-term follow-up and assessment frameworks has limited conclusions about their sustained impact (Davidson et al., 2013). To address this, international universities might consider hiring or retaining faculty from diverse cultural backgrounds (especially from the Global South) as visiting or guest instructors. They could also promote online knowledge-sharing sessions and launch externship placements or student exchange programmes as a starting point (Ching et al., 2019; Govender et al., 2017).
Systemic Engagement
Client and community engagement emerged as the strongest and most consistently represented theme in the scholarship. Over 70% of studies included some form of community participation, ranging from co-design of interventions to community-led research (Black, 2002; Cairns et al., 2022; Hyett et al., 2023; Sarovich et al., 2024). These approaches were most successful when embedded in long-term relationships and reciprocal learning. In contrast, studies that treated engagement as a consultative or tokenistic process reported limited success in achieving cultural responsiveness (Waugh & Mackenzie, 2011; Webb, 2021). These findings reinforce the HSO framework’s call for meaningful, context-sensitive collaboration with communities and echo Meechan et al. (2024) emphasis on indigenous-led service design and evaluation.
The recognition of systemic racism, trauma, and rights-based frameworks was evident in nearly half of the studies. These studies discussed the impact of colonialism, institutional racism, and intergenerational trauma on health and occupational engagement (Gordon-Burns & Walker, 2015; Zeldenryk & Yalmambirra, 2006). Restall et al. (2016) explicitly engaged with national and international agencies to promote the welfare of Indigenous people. However, only a few studies operationalized rights recognition into practice through concrete policies or tools. This reiterates the concern raised by Meechan et al. (2024), who noted that although policy frameworks may provide guiding principles, their impact depends on translation into relational, community-specific practice.
Safe service delivery was addressed in 57% of the studies included. Positive examples included mobile clinics in remote areas (Pidgeon, 2015), culturally adapted care environments (Cairns et al., 2022), and flexible scheduling to accommodate spiritual or family practices (Watts & Carlson, 2002). However, structural barriers such as underfunding, bureaucratic rigidity, and provider burnout were recurring limitations (Du Toit et al., 2014; Gray & McPherson, 2005). These challenges suggest that safe service delivery requires not only provider-level change but also systemic shifts in resourcing, accountability, and organizational culture.
Gaps Identified
The findings also highlighted several conceptual and practical gaps in the reviewed scholarship. The limited representation of GSM communities, despite their known vulnerabilities within health systems, highlights an urgent need for intersectional approaches to CRC in OT (Mahapatro et al., 2021; Stugart et al., 2025). Despite global rhetoric around inclusion, OT research in non-Western and Global South contexts remained sparse. The scarcity of scholarships from Southeast Asia/South Asia highlights a lack of cultural diversity in the knowledge base and underscores the need for greater internationalization of CRC discourse (Mackenzie et al., 2024; Patro et al., 2025; Webb, 2021;). Across all domains, few studies have formally monitored and evaluated CRC practices. The values and commitments were clearly articulated, but tools to measure progress, ensure accountability, or guide continuous improvement were rarely described (Jacek et al., 2023).
Study Limitations
This study is not without limitations. We did not conduct a quality appraisal of the included studies, which may influence the interpretation of some thematic findings. Although every effort was made to ensure rigorous and exhaustive data charting, the heterogeneity of terms and frameworks used to describe CRC may have led to the exclusion of relevant studies that used alternative terminology. Attempts were made to mitigate omissions through iterative searching and expert validation of inclusion and exclusion criteria; however, some conceptual literature may have been missed if it did not explicitly mention OT. This review relied on published, peer-reviewed literature in English, which may have excluded valuable knowledge, especially from indigenous, Global South, or non-academic sources. The HSO Cultural Safety and Humility Framework provided a robust and relevant analytical lens. However, its international applicability warrants further research. The HSO framework may not fully capture the nuances of cultural safety practices in countries with different health care structures, cultural dynamics, or indigenous governance systems. Care was taken to interpret findings through the lens of the HSO framework without forcing alignment. Finally, the studies were disproportionately skewed towards focusing on practices with indigenous populations. We believe these contributions are invaluable, but they may not fully represent the breadth of CRC application across all marginalized groups or global contexts.
Conclusion and Implications
The findings illustrate that culturally responsive OT is conceptually well-articulated; however, its practical implementation and evaluation remain inconsistent. The literature demonstrates clear efforts to engage with clients and communities in culturally safe and humble ways, particularly in indigenous contexts. However, it reveals limitations in governance structures, educational preparedness, and systems-level accountability.
Concepts such as cultural humility, anti-racism, and trauma-informed care have been increasingly emphasized, reflecting a shift away from static models of cultural competence. However, several areas remain underdeveloped, including formal evaluation of CRC strategies, engagement with GSM communities, and representation from Southeast Asian and Global South contexts.
Future studies may focus on longitudinal evaluation of CRC training programmes, the development of community-led accountability tools, and the integration of intersectional frameworks that address multiple layers of cultural identity and systemic oppression. This review does not aim to prescribe policy or best practice. However, its synthesis may offer a valuable map of current practices, conceptual debates, and implementation challenges that can inform future work in education, service delivery, and knowledge translation.
The findings provide a foundation for future inquiry and reflection, contributing to an evolving dialogue about what it means to deliver OT that is not only clinically effective but also culturally safe, responsive, and accountable.
Supplemental Material
sj-docx-1-otj-10.1177_15394492261418531 – Supplemental material for Culturally Responsive Occupational Therapy Education and Practice: A Scoping Review
Supplemental material, sj-docx-1-otj-10.1177_15394492261418531 for Culturally Responsive Occupational Therapy Education and Practice: A Scoping Review by Kripa Titty Cherian, Pramod Dattaram Lambor, Abhilasha George, G. Neha, Aleena Anu George and Rod Charlie Delos Reyes in OTJR: Occupational Therapy Journal of Research
Supplemental Material
sj-docx-2-otj-10.1177_15394492261418531 – Supplemental material for Culturally Responsive Occupational Therapy Education and Practice: A Scoping Review
Supplemental material, sj-docx-2-otj-10.1177_15394492261418531 for Culturally Responsive Occupational Therapy Education and Practice: A Scoping Review by Kripa Titty Cherian, Pramod Dattaram Lambor, Abhilasha George, G. Neha, Aleena Anu George and Rod Charlie Delos Reyes in OTJR: Occupational Therapy Journal of Research
Footnotes
Acknowledgements
We extend our sincere gratitude to Carrie Price for her invaluable assistance in reviewing the search strategy. The authors gratefully acknowledge the Manipal Academy of Higher Education (MAHE) for supporting the open access publication of this article.
Ethical Considerations and Patient Consent
This study was conducted as a review of existing literature and did not involve the recruitment of human participants or animals.
Consent for Publication
Not applicable. This review did not involve human participants and, therefore, did not require participant consent for publication.
Funding
The authors received no financial support of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This scoping review is based on an analysis of previously published literature. All data extracted and analysed during this review are available within the included articles, which are cited in the reference list. Additional data (Appendix) used in the review will be made available online.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.