
Abstract
Amid calls for inclusion of autistic people in research, we present findings from our community-engaged study on the experiences of families of autistic girls, who experience disparities in autism identification, and show how the Autistic Lived Experience Collaborators (ALEC) in the Disparity Reduction and Equity in Autism Services (DREAmS) Lab influenced our findings. In Part 1 of our multimethod study, 21 caregivers completed interviews and survey questions. In Part 2, 10 Hispanic/Latino caregivers from Part 1 completed 1 to 3 interviews. Analysis used descriptive statistics and a narrative thematic approach. We also drew from analysis meeting notes. Girls from Spanish-speaking families had later ages of autism identification, which informed our qualitative themes: Survival Explains Stigma, a view of Hispanic/Latino culture that clarified the “stigma” that impacted the diagnostic process; and Intergenerational Influences on staying safe, which could include masking autistic traits. ALEC quotes show their contributions. Our community-engaged approach contributed to our findings and a more complex view of culture.
Plain Language Summary
Introduction
Autistic people have long called for greater inclusion in research (Fletcher-Watson et al., 2017; Raymaker, 2019). Community-engaged research aims to increase participation of community members, providing more equal access to knowledge and capacity building, focusing on issues that matter to the community, and addressing an ethical imperative of inclusion (Charlton, 1998). Well-known approaches include community-based participatory research (CBPR) (Israel et al., 2005) and participatory action research (PAR); other approaches are less structured but involve inclusion and participation to varying degrees (Ritas, 2003).
Community-engaged research aligns with occupational therapy principles of participation and inclusion, and occupational therapy research has historically valued participatory approaches, for example, with people with developmental disabilities (Hammel et al., 2008, 2016; Kramer, 2007; Schwartz et al., 2019; St John et al., 2022; Suarez-Balcazar et al., 2018). In autism research, groups such as the Academic Autism Spectrum Partnership in Research and Education (AASPIRE) (Nicolaidis et al., 2011) and Autistic Adults and other Stakeholders Engage Together (AASET) (Benevides et al., 2020) have created ongoing, sustainable partnerships between academic researchers, clinicians, and autistic communities. We situate our work in the Disparity Reduction and Equity in Autism Services (DREAmS) Lab within these rich traditions of community-engaged research.
Our Community
The DREAmS Lab was created by Angell in her first year in a faculty position. Building on her postdoctoral training in community-engaged research, 1 Angell and autistic research consultant Floríndez began to discuss a shared vision for an autistic collaborator group. During the following year, discussions around priorities, group culture, and accommodations led to the development of the Autistic Lived Experience Collaborators (ALEC). While our group skews as highly educated, a relative limitation, we view its makeup of autistic women of color as a marked strength.
Research Study Context
Around that time, Angell began a multimethod research study that built upon her previous work on disparities in autism diagnosis and services among Black and Latino children (Angell et al., 2016; Angell & Solomon, 2014, 2017) and girls (Moreira & Angell, 2020), who were gaining recognition as an underidentified group (Carpenter et al., 2019; Gould, 2017). Despite burgeoning research on autistic girls, including explorations of phenotypic differences and experiences of delayed diagnosis and “masking” (Hull et al., 2020), there was a dearth of research about girls from minoritized racial and ethnic groups (Lovelace et al., 2021), particularly on how their families come to obtain an autism diagnosis. This study (“Part 1” from here on) therefore sought to understand these diagnosis experiences.
Analysis of this study’s findings pointed to the intersection between autistic masking and culture. This led us to pursue funding for a second part of the study, co-led by Angell and Floríndez, to ask caregivers more directly about this intersection. We had been conceptually exploring notions of masking for safety among Black autistic girls and women, led by PhD student Franklin et al. (2024); our Part 2 research study then enabled a data-driven examination of the phenomenon with Latino culture, additionally exploring intergenerational influences.
The purpose of this analysis is to (a) present key findings from Part 1 of our research study with families of autistic girls that we explored more deeply in Part 2 and (b) show how ALEC contributions influenced the evolution of these findings. Specifically, we aimed to show aspects of our collaborative analytic process that reflect how three founding ALEC members’ identities of being both autistic and Latina uniquely influenced the key findings of our study. In this way, we present research findings alongside the process of their development, providing transparency about the collaborative process and showcasing the benefits of research that is rooted in the community, carried out with and by people who are in close proximity to the research topic.
Method
Study Design
We conducted a two-part, multimethod study with caregivers of autistic girls in Los Angeles County. Part 1 (N = 21 caregivers) used a multimethod approach (qualitative interviews and closed-ended questions) to ask: How do caregivers of autistic girls experience the process of obtaining an autism diagnosis and services for their daughters? Part 2 (N = 10 caregivers from Part 1) used qualitative interviews to ask: How do Hispanic/Latino caregivers of autistic girls describe cultural and intergenerational influences related to understanding and identifying autism? Secondarily, our process-oriented aim asks: How did our community-engaged research approach influence what we “saw” in our data?
Recruitment and Participants
The study was approved by the University of Southern California Institutional Review Board. A Los Angeles County Regional Center distributed our recruitment materials to families who met the inclusion criteria: (a) ≥18 years old, (b) parent/caregiver of an autistic girl ≤12 years old, and (c) able to participate in an English or Spanish language interview. All participants provided informed consent.
In Part 1, we recruited 21 caregivers of 19 autistic girls from 18 families (one family had twins). We had no racial/ethnic inclusion criteria, but our sample reflects the diversity of our recruitment area (see Table 1). In Part 2, we invited all 14 caregivers with Hispanic/Latino identities 2 to participate in further interviews; 10 caregivers (of 10 autistic girls from 10 families 3 ) participated.
Sample Characteristics.
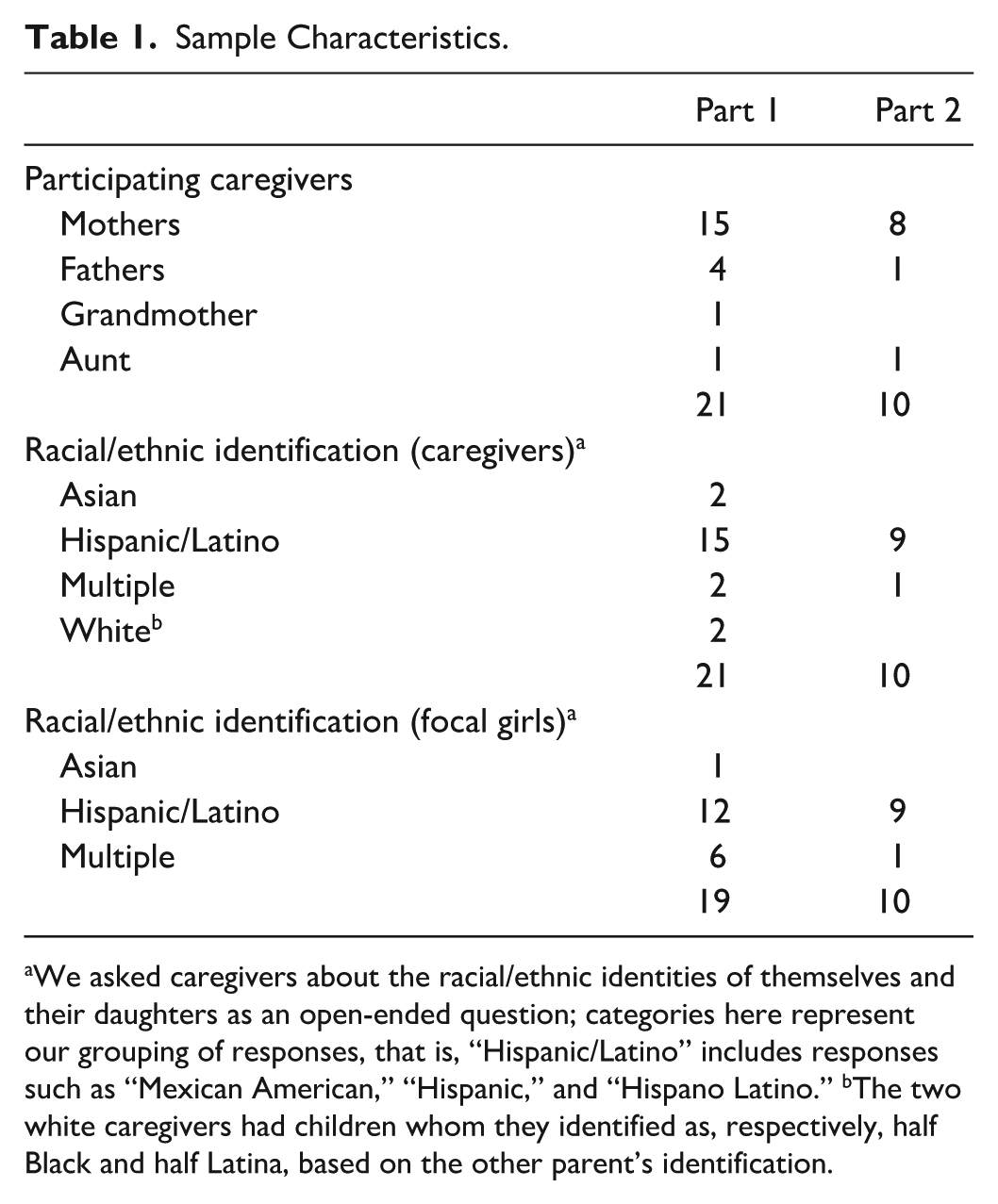
We asked caregivers about the racial/ethnic identities of themselves and their daughters as an open-ended question; categories here represent our grouping of responses, that is, “Hispanic/Latino” includes responses such as “Mexican American,” “Hispanic,” and “Hispano Latino.” bThe two white caregivers had children whom they identified as, respectively, half Black and half Latina, based on the other parent’s identification.
Data Collection and Corpus
In Part 1, we conducted one semistructured narrative interview followed by five closed-ended survey questions (about key points in the diagnosis experience, including the child’s age at first developmental concerns, concerns raised with a professional, and autism diagnosis) with each family between September 2021 and April 2022 (English conducted by Angell, Franklin; Spanish conducted by Lopez). Caregivers from the same family were interviewed together, totaling 18 video-recorded interviews via HIPAA-compliant Zoom (10 English, 8 Spanish; ~45–120 min each).
In Part 2, we conducted 1 to 3 semistructured narrative interviews with 10 caregivers between October 2023 and May 2024, totaling 18 video-recorded Zoom interviews (9 English, 9 Spanish; conducted by Floríndez; ~45–120 min each). The 1 to 3 interview range was intended not only to reach data saturation but also to provide an accommodating approach, important to ALEC priorities; the interview guide (co-designed by Angell and Floríndez with input from the team) was tailored for both neurotypical and neurodivergent needs, allowing for more check-ins and an emphasis on participant-led storytelling and informed choices about the depth in which they wanted to divulge. For example, we provided the questions in advance and reiterated our intention not to revisit difficult topics without active, ongoing consent.
In Part 1, we transcribed interviews; in Part 2, we used AI-generated transcripts and verified them for accuracy. Each caregiver received a $25 gift card after each interview. We replaced all identifiers with pseudonyms. Audio- and video-recorded data were stored on a secure server (Part 1: 23 hr, 25 min; Part 2: 23 hr, 41 min).
For the secondary aim of this analysis, to show how these prominent themes evolved, we also draw on a set of notes and transcripts from 28 analysis meetings (53 pages of meeting notes, 350 pages of AI-generated meeting transcripts) and written and spoken reflections elicited from three founding ALEC members for this article, in response to the prompt, “How did ALEC influence our study analysis and findings?” We drew select quotes from these notes and elicited responses, chosen to provide examples of how the discussion evolved over time. In doing so, we reveal our processes, represented below alongside (and interwoven with) our study findings.
Data Analysis
We summarized our closed-ended survey questions using descriptive statistics and referenced them during qualitative analysis. For qualitative data, we used narrative (Reissman, 1993) thematic analysis (Braun & Clarke, 2006), specifically: (a) a theoretical thematic approach (detailed analysis of some aspect of the data, driven by the investigators’ theoretical lens; namely, a critical approach rejecting common “cultural deficit” views of culture (Angell et al., 2016; Angell & Solomon, 2017) and our ongoing work on “survival” and autistic experiences (Franklin et al., 2024), (b) at the latent level (underlying meanings, assumptions, and ideologies are theorized as informing the explicit/semantic), and (c) from a constructionist epistemology (attention to sociocultural contexts and structures that influence individual stories).
First, Angell and Floríndez read through the Part 1 English-language data corpus and developed an initial codebook. Floríndez then read through the Part 1 Spanish-language transcripts in the original language; discussions led to the determination that no additional unique Spanish-language codes were needed, particularly as many of our English-language interviews were with Hispanic/Latino families. Each transcript had at least two independent coders using NVivo software; we met throughout the coding process, iteratively refining the codebook and then grouping codes into larger themes. To elicit ALEC feedback, we created 1- to-2-page vignettes summarizing each family’s story, creating a more accessible way for everyone to contribute during analysis meetings. For Part 2, we followed a similar process but had only one Spanish-fluent coder at that time (Floríndez), and therefore, otherwise relied on English translations.
Our purpose was to (a) present key findings from Part 1 that we explored more deeply in Part 2 and (b) show how ALEC contributions influenced these findings. ALEC lived experiences of being both autistic and Latina influenced our analytic lens, leading to the development of themes that we may not otherwise have “seen.” In addition to describing the themes with supporting data excerpts below, we include interwoven quotes that we selected from our meeting notes and elicited from ALEC to show how these themes evolved. Although this is an unconventional format, we argue that description of the themes is inextricable from the process by which we identified them.
Reflexivity and Trustworthiness
To build credibility and confirmability, we used peer debriefing with coauthors who were not involved with data collection and (for Part 2) multiple interviews (Letts et al., 2007). Our analysis below makes evident how group identities such as autistic and Latina have influenced our findings. Other identities, for example, White, Black, nonautistic, mother, daughter, occupational therapist, and occupational scientist, also shaped our interests in and framing of the research questions, perspectives we brought to analysis, and interpretation of our findings.
Results
Our descriptive quantitative survey findings were a starting point for our qualitative analysis. They showed the girls’ ages at key points in families’ diagnosis experiences, that is, how caregivers noticed developmental delays or differences in their very young daughter, discussed these with a professional and/or began to suspect their daughter might be autistic, and pursued a diagnosis (see Table 2). Although most of our families had at least partial Hispanic/Latino identities, we noticed that girls whose caregivers interviewed in Spanish were slightly older at all key points. We interpreted this by viewing the process of obtaining a diagnosis as necessarily situated within family and cultural contexts, where narratives about disability “stigma” were often linked to intergenerational influences, such as extended family members objecting to the idea that the girl’s development was delayed or atypical, in some cases because other family members had similar, “normalized” behaviors. These influences not only impacted the child’s age when the caregiver initiated the process, they also shaped how caregivers came to understand autism. Below we describe the two primary qualitative themes that began in Part 1 of our study and were more deeply explored in Part 2, Survival Explains Stigma and Intergenerational Influences, with interwoven supporting ALEC quotes that show our process of coming to these themes.
Girls’ Ages at Key Points in the Diagnosis Process.
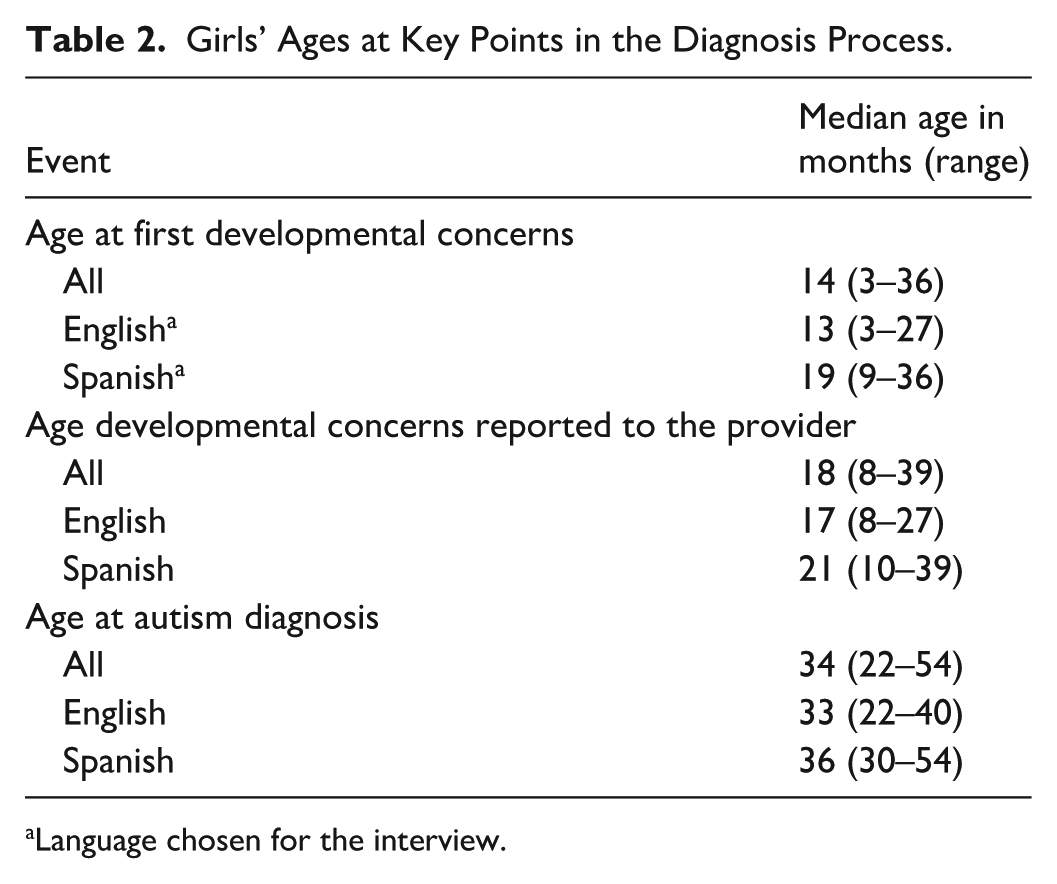
Language chosen for the interview.
Survival Explains Stigma
Parents’ stories about obtaining an autism diagnosis for their daughters elicited a range of reactions among ALEC, particularly around biomedical views of autism implicit in caregiver narratives, that is, caregivers coming to terms that something was “wrong” with their daughters, which could be seen as an implied “disease” view of autism or “normalization agenda.” ALEC member Cogger reflected: We discussed framing, what language is used, and how. If [caregivers] mentioned learning from online community members and sources that had a neurodiversity (affirming) approach, how would that have shown up? Suppose the person was only exposed to the biomedical view of autism. How would that affect their language? What does it look like in the overall discussion of the child’s experience and their journey together—is there more of a focus on hope and progress, or on what can’t be done or the struggles? We talked about how we saw and understood them because of shared experiences.
This arose in analysis discussions about Eve, a mother who participated in Parts 1 and 2. Eve’s parents immigrated from South America when she was a child. When Eve’s daughter Maya was an infant, she noticed that she was not meeting developmental milestones, concerns that were dismissed by Eve’s family and health care providers. Eve felt isolated and struggled to get her husband and parents to validate what she was noticing; her cultural background and familial influence presented pressure to see everything as “normal.” She recounted in Part 1: We went to Disneyland once and I had gotten [Maya] some popcorn, and she was in the stroller and she just started lining up all the little popcorn kernels in a line across the tray and I asked her dad, “Are you seeing what I’m seeing? [. . .] He says, “Oh you’re just Dr. Googling again, and you’re gonna, you know, think she has everything, every element that you read about.” [. . .] My parents were saying “No, no, she’s probably fine. You were bookish, and you took your time, and you were a tiny baby, too.” So, I felt during that time, people were trying to be assuring, to me, but they were kind of dismissing my concerns within my family. It was really lonely and isolating time for me. [. . .] [Maya] just happened to struggle with so much.
In analysis meetings, Floríndez noted the critical importance of mapping Latino culture onto Eve’s stories, adding nuance to the discussion of biomedical views of autism and showing how Eve’s cultural background influenced her advocacy for Maya and resulted in “self-gaslighting” as she struggled to trust her own instincts in the light of her family’s assurances that there was no problem, that she herself was “just like that” as a child. ALEC member Guzman said: When it comes to the Latino families, like around me, they usually try to, kind of like minimize their child’s autism, or try to like talk about it in a way that is kind of like embarrassing. [. . .] It’s like, more like they’re trying to make it a secret.
In the later Part 2 interviews, Eve shared: I think “different” is . . . bad. And I’m only talking, like, from a first-generation standpoint. We’re all so busy trying to get a foothold, you know, like my grandparents, like I said, even my mom, she probably would have been ADHD by today’s standard. But they’ve got five kids, they’re learning English, they both worked, it was, you know, very busy, trying to get a foothold. And the kids are trying to fit in, so they don’t want to make waves. They don’t wanna access services, you know. [. . .] I think that’s why people like in White families don’t mind occupying space. [. . .] I just think culturally that, for first generation, “different” can be perceived as “bad,” so we’re not going to advertise “different.”
Rachel and Alexander, who identified as Hispanic (both participated in Part 1, only Rachel participated in Part 2), had just received an autism diagnosis for their 3-year-old daughter, Leila, but had not yet told their families. Rachel said in Part 1: Even now [everyone is] telling us, “She looks fine. She’s okay.” [. . .] We consider it officially diagnosed as of last week. We haven’t really disclosed it yet to the family. Because we are Hispanic, there’s a lot of stigma behind it and so forth. So, we’re trying to see how to bring it up. [. . .] I’m not ashamed of it or anything like that. [. . .] I just don’t want to—how should I say—expose that information, and then it’s not a concern anymore and people make fun of it. In Hispanic culture, it’s very common to taunt somebody for something, they can make it loving. [. . .] For example, my brother-in-law, his brothers, they still to this day call him “Pelón” because he was bald as a baby, completely bald. So he’s a 40-year-old man and he’s still being called that. It stays with you. So, there are certain reasons why I don’t want to bring things up to certain family members because they’re not going to help. They’re going to judge.
Emily, a mother who identified as Taiwanese and participated in Part 1, echoed the idea that “it could have been a cultural thing” that she did not initially notice her daughter’s delayed speech, that “if something is not ‘right’ . . . we don’t really talk about it.” Our sample of caregivers, however, primarily had Hispanic/Latino identifications, so our efforts to examine culturally influenced disability stigma at a deep level focused on a Latino cultural perspective, although aspects of our analysis may have implications for other cultures (see Discussion).
Our previously mentioned ongoing theoretical discussions about Black autistic girls and women led by Franklin et al. (2024) aligned with how we discussed what could have been considered “disability stigma.” Floríndez noted that “stigma” must be understood within the concept of culturally influenced “survival,” a critical lens to be mapped onto caregivers’ experiences: Sometimes, you know, when parents are saying, “I want my kid to be normal, I want her to have a normal life,” there is that element of, “Oh, I want them to be neurotypical.” And that can be a reflection on the perceptions of autism. But I also hear, “I want my child to be safe. I want them to have friendships. I want them to not know violence. I want them to have stability.” And that is, you know, it’s the terror of knowing that your child is different in the world, that is often not accepting or accommodating of differences. So I see this intergenerational trauma, this intergenerational pressure to not talk about it, and to put on a certain presentation in order to survive and receive opportunities. So I just want to honor that level of the fear of wanting your child to be safe. And the steps that you’ll do to try and ensure that, for someone that you love so much, and at the same time the harmful implications that can stem from it, absolutely.
This lens facilitated a more nuanced understanding of the caregivers’ experiences, listening to caregivers’ framing of autism, or potential autism, in their daughters, with consideration for the possibility of ways that caregivers, particularly from minoritized racial and ethnic backgrounds, sought to protect their children from judgment and harm. It allowed for a contextualization, for example, of Eve’s concerns about Maya’s developmental delays, situated within Eve’s worries about her daughter’s future safety and happiness, in the context of Eve’s own social isolation and lack of support. In other words, it helped our team, including members who initially had difficult feelings about caregivers’ seeming deficit-focused views of autism, to understand them in a broader context, including fear for their daughters’ safety. Eve said in Part 1: I want [Maya] to be safe. She doesn’t express herself enough, to where, if she had a babysitter, or a kid on the playground that did something to her, she can’t tell me with enough accuracy what happened in her day.
Eve worried that Maya would face “a struggle, potentially for life,” yet she also said, “it’s constantly reminding myself to take a break, look at Maya’s face, realize that, although I’m struggling with the future, she is a content kid. Overall, her personality is very joyful.” Contextualizing Eve’s comments with the complexities of culture and struggle, perhaps difficulties Eve herself experienced, helped move the interpretive lens from Eve having a “normalization agenda” to a more nuanced view of the broader context of her concerns for her child’s future and safety, even as she tried to focus on her daughter’s happiness.
Intergenerational Influences
We reflected in analysis meetings on how each generation teaches the next what is considered “normal” child development, what is acceptable behavior for children, and how to stay “safe,” particularly when a family is in a marginalized position in society. These intergenerational influences weighed heavily in our participants’ experiences, not only in older generations insisting that some of the girls’ developmental delays or differences such as delayed language or food selectivity were “normal,” and therefore caregivers should not see them as an indicator of autism, but also in how caregivers felt judged for their daughter’s “misbehavior.” Rather than using a “cultural deficit” framing that often underlies health disparities research, we situated caregiver experiences of being either brushed off in their developmental concerns for their daughters, or told they simply needed to discipline their girls for “misbehavior,” as part of Latino cultural values related to sociality, community, and sometimes even conformity, so as not to stand out from “the pack.” Floríndez called this “intergenerational masking,” that is, passed-down understandings influenced and redefined by culture, unique to each family, that curated a sense of what is safe and acceptable, or unsafe and different.
Anahi, a mother who identified as Hispanic/Latino and participated in Parts 1 and 2, gave direct insight into the relationship between girlhood, autism, and culture. She said that in Latino culture, punishment was viewed as the necessary way to get “good behavior” in children; there was less tolerance for misbehavior. She situated this in Part 2, however, within a historic context where “no había niñez,” “there was no childhood” [original Spanish, followed by English translation]:
[Habia] menos tolerancia a dejar ser niños, realmente antes no había niñez en nuestra cultura, no había niñez porque los ponían a trabajar porque tenían que cuidar a sus niños menores, porque bueno hay tanto, entonces no se ha visto en nuestra cultura una niñez completa de una niña. ¿Que diga no es que es parte del niño, es parte de ser niño, no? ¿Entonces nuestra cultura tal vez se ha cortado, eso se ha oprimido eso entonces? Por eso es que a veces uno es la primera, quizás la cultura tienes menos tolerante a lo berrinche, menos tolerante, a cierta expresión de ciertos niños.
Before, for girls, really, there was no childhood in our culture, there was no childhood because they were made to work because they had to take care of their younger siblings because there were so many, and so in our culture, you haven’t seen a complete childhood of a girl. It’s as if to say that [autistic characteristics or acting out] is not part of being a child, but it is part of being a child, right? So our culture has perhaps been cut off [from childhood], it has been oppressed, then? That’s why sometimes you are the first, perhaps our culture is the least tolerant of tantrums, less tolerant of certain [ways to express yourself] among certain children.
Anahi’s daughter Angelica had been a “fussy baby” and, as a 5-year-old, frequently had “los berrinches,” or tantrums. Anahi described the Latino cultural perception of children’s crying or tantrums as “misbehavior,” that the children were “malcriada,” and said that despite an increasing awareness of autism among Latinos, she had felt judgment from others about Angelica’s behavior. She explained this, however, in a context of generational cycles; when “there is no childhood,” particularly for girls who must help care for younger children, there is “la dureza,” a “toughness,” that gets transferred from one generation to the next. As Eve’s previous quote demonstrates, “staying in line” and not calling attention to oneself or one’s family was critical. This, then, could serve as the vehicle not only for insisting that girls were not autistic but also for teaching and reinforcing the masking of autistic traits that have heritable qualities and can span generations. She said in Part 2:
La mayoría era que iban a trabajar, se iban con sus papás. Eran explotados. Era después, esa cultura viene de que la la dureza de los papás se transmitía, el niño crece y esa dureza la vuelve a pasar a su otra a sus otros, sí, y ahí va la cultura. Y ahí va.
These kids went to work with their parents, there were no rights of the child, they didn’t go to school, they were exploited. And this comes, this culture comes from the difficulty that their parents transmitted, this toughness, this cycle continues on to them and others, and that is the culture, that is culture, there goes culture, continuing on.
Stephanie, a mother who identified as Hispanic American and participated in Parts 1 and 2, described negative consequences that can come from autistic traits not being accurately identified in a child. She said in Part 1 that her daughter Kendall’s dad showed autistic traits as a child that were interpreted as “bad behavior”: Kendall’s dad shows spectrum-like behaviors but has never been tested. [. . .] So many other kids go through all of this. It’s like they’re bypassed, and it sucks. That’s pretty much what kind of happened for her dad, is that his mom just passed it off as bad behavior. And the school passed it off as bad behavior. And then, as he got older, he got into the street life and things like that. And that’s where those bad behaviors just fit right in, you know? So, that’s difficult. And it’s very sad.
In addition to discussing the implications of autistic traits being viewed as “bad behavior” among young men of color, we also considered the unique consequences when girls are overlooked or their autistic traits are misunderstood, given gender differences in societal expectations. In an analysis meeting, Floríndez said: We hear in these stories this almost coded reference to other family members. The moms who see and deeply understand autism as seen through the lens of their children’s behaviors, the nature of their diagnosis is almost a window or intervention that is counterculture, that they had to advocate for because it went against what they were taught. And in caretaking we heard these powerful reflections regarding their own behaviors—or how they saw their parents completely differently—just that these threads of “autistic traits” didn’t appear out of nowhere, once they knew what they were looking at, so much so that they saw these threads within them and other family members—completely shifting their understanding of autism across the generations.
Reflecting on this theme, Guzman said: For a while, I was the only autistic person in my family, but looking back, it’s more like, looking like, you know, with some of my aunts and uncles, you kind of see that they also have traits, but people don’t want to see the possibility that they’re autistic, even though they struggle a lot, similarly, like me. I had an aunt in Mexico who was like me, I guess, when she was younger, cause like, when I go somewhere, sometimes when I go to places, I get kind of overwhelmed, and I don’t really want to go. So I kind of get cranky. And then my mom would be like, you know, “You remind me of your aunt when she was like that, because she would also feel uncomfortable, being in a certain place, and wanted to leave.” Because, you know, she was overstimulated. And I’m like, “Do you think she had autism?” It’s like, “Oh no, she didn’t have autism. She wasn’t like that.”
Our aim was not to label caregivers in ways they would not themselves identify, but rather to “not assume neurotypicality.” However, our team, particularly our autistic members, saw significance in caregivers’ descriptions of autistic traits in themselves and other family members, and pointed to the fact that almost none of them self-identified as autistic as further support for our findings about why labels, for minoritized groups, can elicit fear and unsafety.
Discussion
We presented findings from our two-part multimethod study of the experiences of diverse caregivers of autistic girls, highlighting the complex role of survival in explaining what otherwise appeared to be “stigma,” and how this impacted when caregivers came to identify potential autism in their daughters; as well as intergenerational influences on how children’s behavior is understood and passed-down “teachings” about how to stay safe, which could include masking autistic traits. Our interest in documented disparities in diagnosis among girls, particularly girls of color who have been almost entirely neglected from the literature (Franklin et al., 2024; Lovelace et al., 2021; Moreira & Angell, 2020), guided our desire to understand at familial, intergenerational, and cultural levels how and why delayed or missed diagnosis might occur. Throughout our analysis, we also showed the process by which we came to these key themes with our community-engaged research approach.
Our analysis of culturally influenced disability “stigma” focused primarily on Latino culture, given its prominence within our data and ALEC lived experience. It enabled us to understand participants’ comments about their culture, which on the surface may appear negative or deficit-focused, in a complex, historically situated way. This is in contrast to much of the existing literature about autism disparities that theorizes the role of culture in a straightforward, often decontextualized way (cf. Angell et al., 2016; Angell & Solomon, 2017). However, we showed via our secondary aim how autistic Latina lived experience guided our analytic lens to navigate the challenges of seemingly stigmatizing views of autism, and to understand the complexity in caregiver narratives, rather than flattening them as other theoretical lenses, or polarized online debates, can do. This echoes occupational therapy advocacy for a movement away from “traditional” toward more critical views of culture (Beagan, 2015; Castro et al., 2014), providing a data-driven example for occupational therapists to apply across practice settings and populations.
Consideration of culture in how parents interpret and understand autism in their children has been studied (Gordillo et al., 2020; Singh & Bunyak, 2018), and aspects of our findings echo previous research, for example, showing that Latino caregivers place higher value on sociality and emotion regulation in their children compared to other developmental milestones (Ratto et al., 2016). Less has been studied in autism research, however, about the intersections of culture and gender. Our analysis of Latino culture, histories, and gender expectations of children, that is, for girls “there is no childhood,” along with our conceptual analysis by Franklin et al. (2024) about the roles of safety and survival in masking among Black autistic girls and women, contribute to this emerging body of scholarship.
Gu et al. (2023) found that boys tend to be diagnosed with autism between ages 3 and 11, while girls tend to be diagnosed before 3 or after 11. The difference, however, was moderated by anxiety and mood disorders, raising questions about whether co-occurring psychiatric conditions mask autistic traits, or whether autistic traits are mistaken for psychiatric condition traits. While our findings do not speak directly to this, our sample, which skewed very young at diagnosis, likely due to successful early identification efforts at the Regional Center where we recruited, could represent a distinct female subgroup that is identified earlier due to more pronounced or apparent developmental delays or autistic traits. More research on potential female subgroups could help to understand the unique needs of each.
Our secondary aim showed how analytic and interpretive ideas evolved within a group context, and the important role of Latino cultural perspectives. An important aspect of our team was having an autistic researcher who bridged the spaces between Angell and ALEC; Floríndez’s position as co-lead allowed for constant questioning, engaging, and re-situating of information, sometimes before it reached the rest of the team. It wasn’t about “protecting” anyone but rather subverting traditional power structures and being a critical valve and gage that helped direct the flow of information and take into consideration power dynamics. This highlights the need for ongoing relationships between community partners and academicians as a vehicle for bridging the research-practice gap. Such collaborations not only enrich the findings but may inform the work of occupational therapists, broadening their understanding of how stigma and intergenerational trauma shape the lives of families of Latina girls, paving the way for improved client-clinician rapport and clinical outcomes.
Our analysis has some limitations. First, we focused on Latino culture, which may limit the applicability of our findings to other cultures. However, our approach to culture, incorporating lived experience perspectives and situating “disability stigma” within sociocultural and historic framings, may have transferability (Letts et al., 2007), even for occupational therapy practitioners to consider more critically informed views of culture as they relate to their clients (Beagan, 2015; Castro et al., 2014). Second, our lack of additional Spanish-fluent coders (and reliance on translations) for Part 2 is a weakness. Third, our early-diagnosed sample does not reflect national averages. As previously mentioned, there may be different profiles in girls that uniquely influence their diagnostic experiences; more research is needed.
Conclusion
We presented key findings from our study investigating the experiences of caregivers of autistic girls in receiving an autism diagnosis for their daughters and showed how our community-engaged research approach influenced the evolution of these findings. We showed how diverse team member perspectives evolved to more nuanced understandings of our findings about stigma, survival, and intergenerational influences related to autism, contributing to more critical examinations of culture within occupational therapy and occupational science.
Footnotes
Acknowledgements
We thank Michelle Urquidi, Savannah Runge, Reagan Landis, Liza Abigail Khou, Cortland Jell, and Janis Yue for their contributions.
Ethical Considerations
The University of Southern California Institutional Review Board granted ethical approval for this study (Part 1 HS-20-00851; Part 2 UP-23-00592). Study personnel completed Human Subjects Protections and Health Insurance Portability and Accountability Act (HIPAA) trainings.
Consent to Participate
All participants provided informed consent (written in Part 1, verbal consent in Part 2).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There was no external funding for this Part 1 of this study; we acknowledge the support of the Chan Division. Part 2 was funded by the USC Chan Division ReSPONs Seed Grant Award.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.