
Abstract
Many parents live with enduring health conditions; however, the impact of enduring health conditions on parenting roles is poorly understood. The aim of this study was to explore the experiences, support needs and preferences of parents in Ireland living with enduring health conditions. Data were collected using a custom e-survey, developed and refined using cognitive interviewing (n = 6). Quantitative data were analysed using descriptive statistics and group comparisons, while open-ended responses were analysed using interpretative content analysis. In total, 281 eligible parents completed the survey. Participants reported considerable difficulties with parenting tasks, particularly physically demanding tasks. Participants had limited access to formal services and many reported unmet needs and dissatisfaction with current services. Enduring health conditions have a significant impact on parenting capacity. There is a need for integrated support systems to ensure parents with enduring health conditions are supported to engage in parenting occupations and roles.
Plain Language Summary
This study looked at the experiences of parents living in Ireland who live with an enduring health condition, including chronic diseases, disabilities or mental health conditions. Being a parent can be challenging, and these challenges can be even harder when someone also lives with an enduring health condition. A total of 281 eligible parents took part in an online survey. They shared how their health affects their ability to manage day-to-day parenting tasks and the types of services and supports that they believe would be beneficial to receive. Overall, the findings show that parents with enduring health conditions face extra challenges in their parenting roles and often feel unsupported. The results highlight the importance of creating more flexible and responsive services that take into account both the health and parenting needs of these individuals.
Background
Parenting is a valued occupation and role for many individuals (Lim et al., 2022) and is recognised by occupational therapists as an instrumental activity of daily living (Boop et al., 2020). However, when parents live with enduring health conditions- a term used throughout this study to encompass chronic disease, disability and mental health conditions- the role becomes increasingly complex (Honey et al., 2024; Pituch et al., 2022).
Article 23 of the United Nations (UN) Convention on the Right of Persons with Disabilities (UNCRPD) sets out the rights of persons with disabilities to marry, have children, and receive parenting supports (UN, 2006). Yet, parents with enduring health conditions often encounter barriers to parenting (Honey et al., 2024; Pituch et al., 2022). Many seek support for their parenting roles but struggle to access appropriate services (Mercerat & Saïas, 2021; Pituch et al., 2024). In the United States, an estimated 4.1 million (6.2%) of parents live with a disability (Li et al., 2017), and while specific Irish data is lacking, population estimates indicate that 41% live with a long-term health condition (Healthy Ireland, 2024).
Enduring health conditions vary in visibility, from overt conditions like paraplegia, to invisible ones such as Crohn’s disease or depression, with some, like multiple sclerosis, encompassing both visible and invisible elements (Joachim & Acorn, 2000; Kattari et al., 2018). These conditions can directly affect parenting through symptoms such as pain (Codd et al., 2023), breathlessness (Theander et al., 2014), or psychosis (Reilly et al., 2019), as well as indirectly through psychosocial effects like distress, fear, and grief (Codd et al., 2023; Parton et al., 2022). Medication side effects may also contribute additional difficulties (Morrison et al., 2015).
Beyond these personal challenges, many parents face social and structural barriers including inaccessible environments and biased assumptions about parenting capacity which contribute to stigma and exclusion (Flynn et al., 2023; Kattari et al., 2018). These factors can reduce parental self-esteem, leading to feelings of shame, guilt, and inadequacy (Codd et al., 2023; Hawkey et al., 2022; Law et al., 2021). Health care professionals’ assumptions and lack of understanding may reduce information sharing and access to support (Mercerat & Saïas, 2021; Ordan et al., 2018; Pituch et al., 2024), while fear of judgement further prevents parents from seeking help (Biebel et al., 2016; Flynn et al., 2023). Combined, these factors not only affect parents’ wellbeing but may negatively impact children’s outcomes and overall family stability (Hackett & Cook, 2016).
In Ireland, parents with enduring health conditions are under researched, and underserved (Flynn et al., 2023). Without a clear understanding of parents’ support needs and service delivery preferences, services risk failing to address parents’ needs (Codd et al., 2023; Rider & Selim, 2022). Existing services often lack integration, with poor collaboration between adult and children’s services, leading to unmet family needs and a lack of cohesive support (Hackett & Cook, 2016). Addressing these gaps is not only a matter of equity, but also a human right obligation under the UNCRPD (UN, 2006).
This study aims to explore the experiences, support needs, and service delivery preferences of parents in Ireland living with enduring health conditions.
Methods
Design
A cross-sectional e-survey of parents with enduring health conditions in Ireland was conducted. The survey was developed specifically for this study and included closed and open-ended questions. Design and reporting were guided by the Checklist for Reporting Results of internet E-surveys (CHERRIES) (Eysenbach, 2004).
Survey Development
Given the lack of existing instruments that capture the experiences of parents with enduring health conditions, a study-specific survey was designed. Development was informed by the research aims and literature on parenting with an enduring health condition (Honey et al., 2024; Pituch et al., 2022, 2024). Adaptive questioning was used to reduce participant burden, showing questions conditionally based on prior answers.
Cognitive interviewing was used to improve survey validity, reliability and usability (Peterson et al., 2017). Six participants (three male, three female), aged 31-58 years, with a range of enduring health conditions – including rheumatic, neurological, autoimmune, endocrine, anxiety and mood disorders – were recruited from both urban (n = 4) and rural (n = 2) settings. Each participant completed a draft version of the survey using a think-aloud protocol, providing insights into the accessibility, clarity and relevance of the questions (Drennan, 2013). To clarify participants’ responses, and interpretations, targeted probes were used (Willis & Artino, 2013), such as ‘You look confused – is there something unclear about that question?’ and ‘Can you tell me what you understood by that question?’.
The cognitive interviewing process was completed over three iterative rounds. Interviews took place in person with the researchers maintaining detailed field notes throughout. After each round, the research team reviewed these notes to identify potential issues with the survey. Depending on the nature of the concerns raised modifications were made to the survey, or concerns were flagged for further exploration in subsequent interviews. The changes made included rewording items, merging similar questions, adding instructions, and adjusting response options. At the conclusion of the third round, no additional concerns were raised by participants.
Sampling and Recruitment
Convenience and snowball sampling were used to recruit participants. Inclusion criteria required participants to: (i) self-identify as living with an enduring health condition lasting at least three months, (ii) be in a parenting role for a child under 18, and (iii) reside in Ireland. Recruitment strategies included posters in community spaces, email outreach to parent organisations, and posts on Facebook and Instagram to increase reach and inclusivity.
Ethical Approval
The study received ethical approval from the School of Clinical Therapies Social Research Ethics Committee at University College Cork (CT-SREC-2024-24).
Data Collection
The final survey was hosted on Qualtrics at University College Cork and took approximately 10 minutes to complete. The survey had a total of 34 questions of which 7 were open ended. Study participation was voluntary, with no incentives. No identifying information was sought from participants and where potentially identifying details were included in open-ended responses these were redacted prior to data analysis. Informed consent was obtained via a required agreement checkbox prior to accessing the survey. Data were collected between February and April 2025. CAPTCHA tools were used to prevent bot submissions (Eysenbach, 2004), and survey start, and end times were monitored. to detect automated activity (Yarrish et al., 2019).
Data Analysis
Data were exported from Qualtrics and analysed using SPSS Version 29.0.2.0. Responses with less than 70% completion were excluded. Descriptive statistics were used to summarise the demographic characteristics of the sample. Chi Square tests were used to examine associations between categorical variables. A series of one-way Analysis of Variance (ANOVA) was used to explore the impact of number of enduring conditions on parenting. ANOVA assumptions were checked using the Shapiro-Wilk test and Levene’s test, with post hoc Tukey HSD analyses for significant results. A p-value of <.05 was considered significant.
Open-ended responses were analysed using a hybrid content analysis approach, which combined qualitative and quantitative techniques to capture the frequency of themes and the meaning behind them (Drisko & Maschi, 2009). All responses were exported into Microsoft Word for manual coding. Line-by-line coding was used to examine and categorise each response. Codes that reflected similar ideas were grouped together into broader thematic categories. To enhance the reliability of the analysis, two authors completed the initial coding independently. Following this, all authors engaged in collaborative discussions to compare findings, resolve discrepancies and reach consensus on the final categories. Counts were performed on the final categories to determine the prevalence of concepts. A sample of the categories and codes is provided in Appendix 1 (Supplemental Text).
Results
Characteristics of Respondents (N = 281)
A total of 612 individuals began the survey; 281 met the eligibility criteria and completed at least 70% of questions, giving a 45.9% completion rate. Table 1 outlines participant demographics. Most respondents were female (87.9%, n = 247), Irish (91.5%, n = 257), and biological parents (98.2%, n = 275), with two children (44.8%, n = 126). A majority held undergraduate or postgraduate degrees (76.6%, n = 159). Many (35.6%, n = 100) were employed full-time. Household income varied, with 19.2% (n = 54) earning €20,000-€39,000. More than half (53%, n = 149) owned their home with a mortgage. When asked if they had sufficient financial resources to support their parenting, 24.6% (n = 69) said ‘Yes’, 29.9% (n = 84) said ‘No’, 11.7% (n-33) were ‘Unsure’ and 1.89% (n = 5) ‘Preferred not to say’.
Participants’ Demographic and Parenting- Related Characteristics (N = 281).
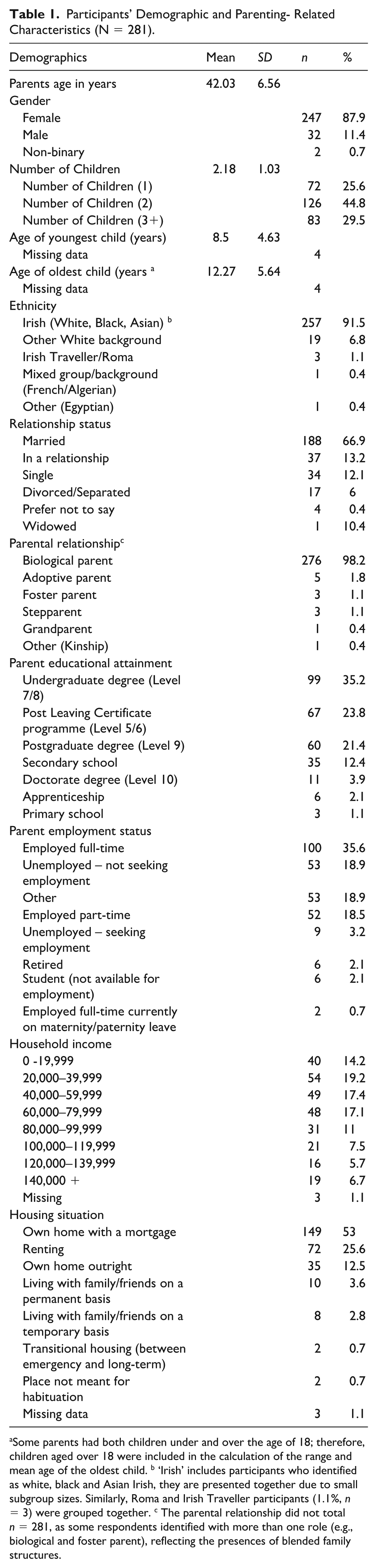
Some parents had both children under and over the age of 18; therefore, children aged over 18 were included in the calculation of the range and mean age of the oldest child. b ‘Irish’ includes participants who identified as white, black and Asian Irish, they are presented together due to small subgroup sizes. Similarly, Roma and Irish Traveller participants (1.1%, n = 3) were grouped together. c The parental relationship did not total n = 281, as some respondents identified with more than one role (e.g., biological and foster parent), reflecting the presences of blended family structures.
Health Conditions
Almost half (49.1%, n = 138) of participants reported 1-2 enduring health conditions; 26.3% (n = 74) reported five or more. A mean of 2.36 physical (SD = 1.7) and 2.5 mental health (SD = 1.5) conditions, with a combined mean of 3.3 (SD = 2.6) were reported. Physical health conditions included autoimmune diseases (30.2%, n = 130), musculoskeletal concerns (29.7%, n = 128), and cardiopulmonary conditions (11.8%, n = 51). Neurological and endocrine conditions were each reported by 9.3% (n = 40). Less common were genetic (3.3%, n = 14), congenital (3.0%, n = 13), and other conditions including Long-COVID, amputation, and sleep apnoea (3.48%, n = 15). Among those with mental health conditions, anxiety disorders were most common (37.7%, n = 136), followed by neurodevelopmental (28.3%, n = 102) and mood disorders (24.4%, n = 88). Fewer participants reported eating disorders (5.8%, n = 21) or personality /dissociative disorders (3.9%, n = 14).
Parenting and Perceived Impact of Enduring Health Conditions
Table 2 provides an overview of participants perception of how their health condition affected parenting. A one-way ANOVA identified a significant effect of the number of conditions, F (3, 252) = 10.05, p < .001, with a moderate effect size (ω² = .096). Post hoc Tukey tests showed those reporting ‘A lot’ of impact had significantly more conditions (M = 4.33) than all other groups (p < .01), suggesting a correlation between number of conditions and the impact on parenting.
Parent Health Related Characteristics (N = 281).
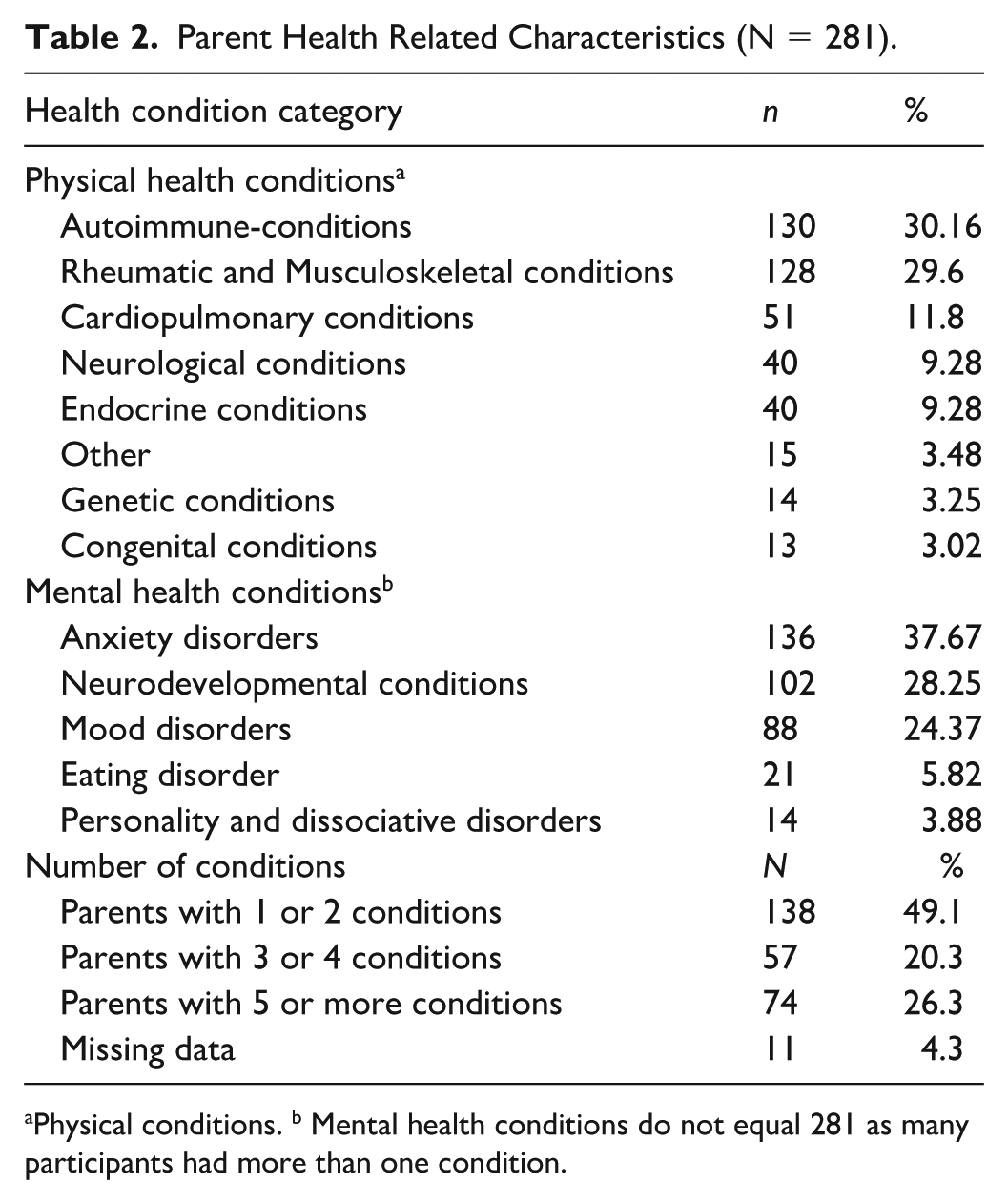
Physical conditions. b Mental health conditions do not equal 281 as many participants had more than one condition.
Parenting Task Difficulties
Of 281 participants, 188 (66.9%), rated perceived difficulty in performing nine categories of parenting occupations previously identified by Lim et al. (2022). (see Figure 1). While the original survey used a 5-point Likert-type scale from ‘Extremely easy’ to ‘Extremely difficult’, to support analysis responses were collapsed into three categories, ‘Easy’; ‘Neutral’ and ‘Difficult’. Respondents were also grouped according to whether their health status was stable or fluctuated. Across both groups the most challenging tasks were playing with children (~61%), moving children (~55%), and managing the child’s social networks (~51%). Chi-square tests revealed significant differences between the groups in two categories. Parents with fluctuating health status more often rated ‘Providing financially’ as ‘Easy’ (45.3%) than those with stable health (26.5%), and less often as ‘Difficult’ (37.3% vs. 48.7%), χ² (2, N = 188) = 7.89, p = .019. Similarly, 51.9% of parents whose health status fluctuated found ‘Managing their child’s health’ ‘Easy’, versus 31.0% of those with stable health χ² (2, N = 190) = 6.78, p = .034. No significant differences were found in perceptions of difficulty for the remaining parenting tasks.
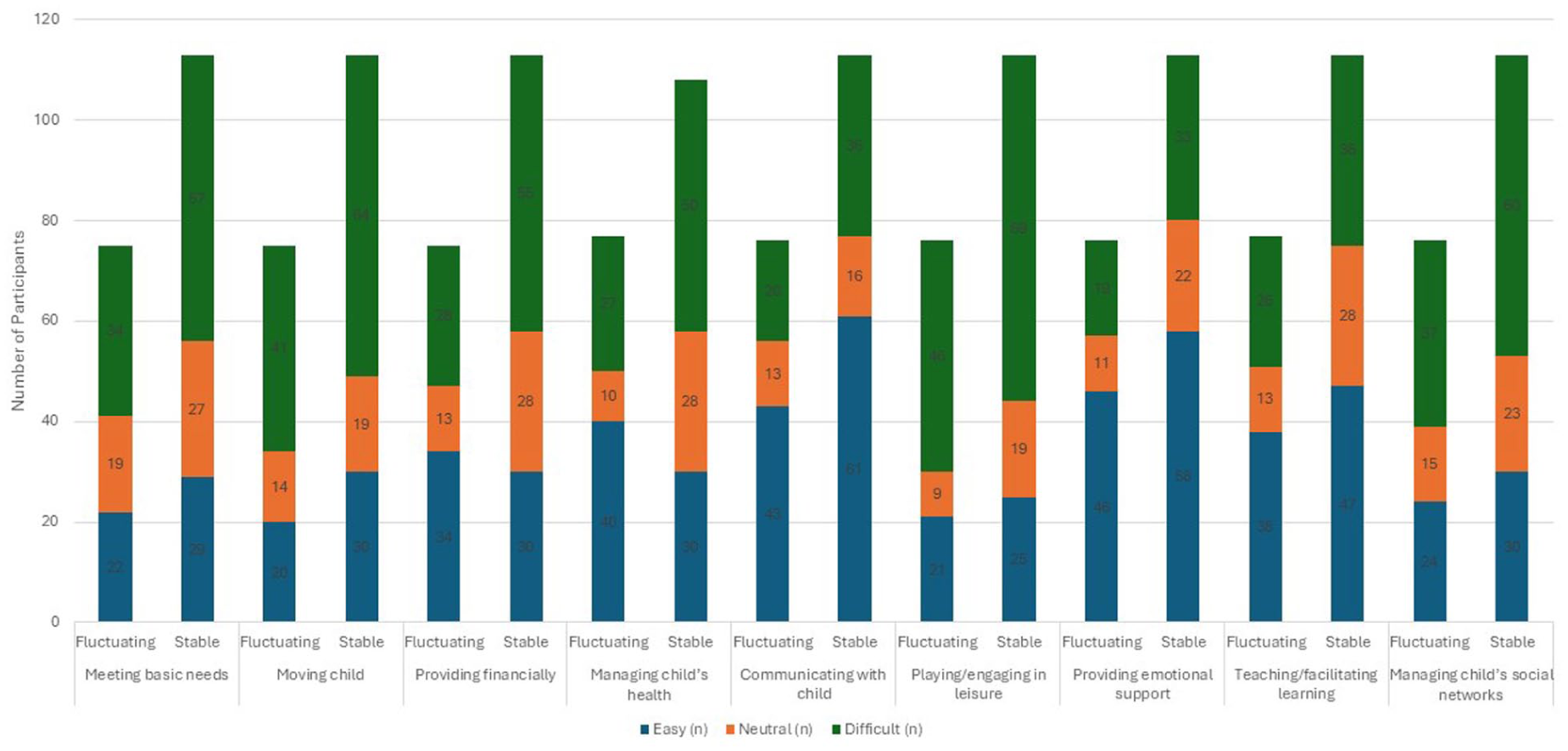
Impact of Enduring Health Conditions on Parenting Tasks by Health Status
Informal Support Networks
Table 3 outlines sources of informal parenting support. Partners or spouses (45.6%, n = 128) and extended family (40.2%, n = 113) were the most common. Open-ended responses (n = 115) further highlighted the critical role of informal support, particularly during symptom flare-ups when parenting was delegated to others (n = 101) ‘They often step into the breach when I’m too ill to carry out parenting tasks”. Parents also identified practical support with child care, transport, and household tasks (n = 56) and emotional support and opportunities for rest (n = 25) as essential supports.
Informal Support Received to Help With Parenting Roles (N = 281).
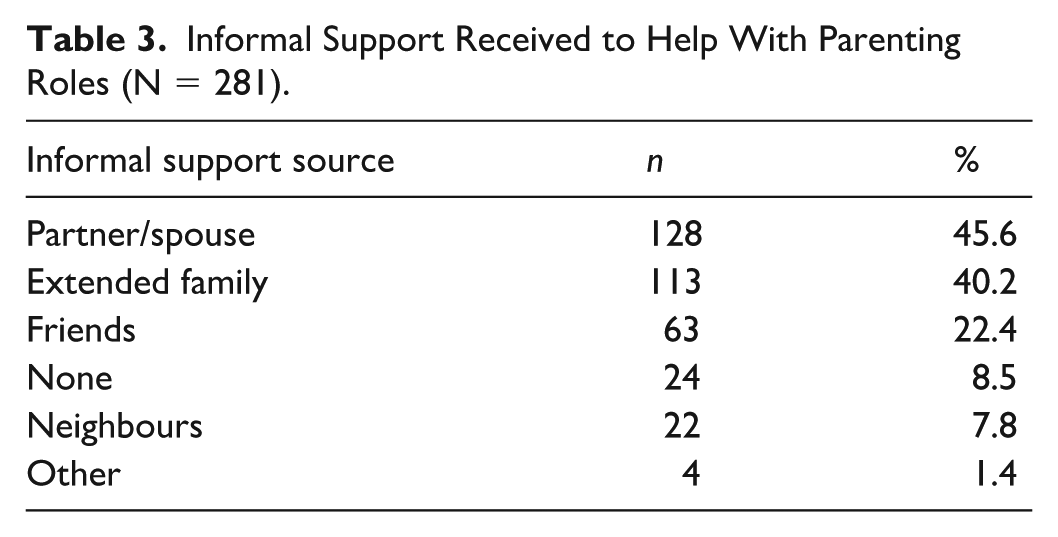
Despite appreciating informal supports, many participants reported feelings of guilt and reduced self-worth. One parent notes ‘It can be challenging . . . as you feel like a burden and not good enough’. Some (n = 8) reported no support and expressed feelings of isolation ‘We are on our own’,
Formal Services
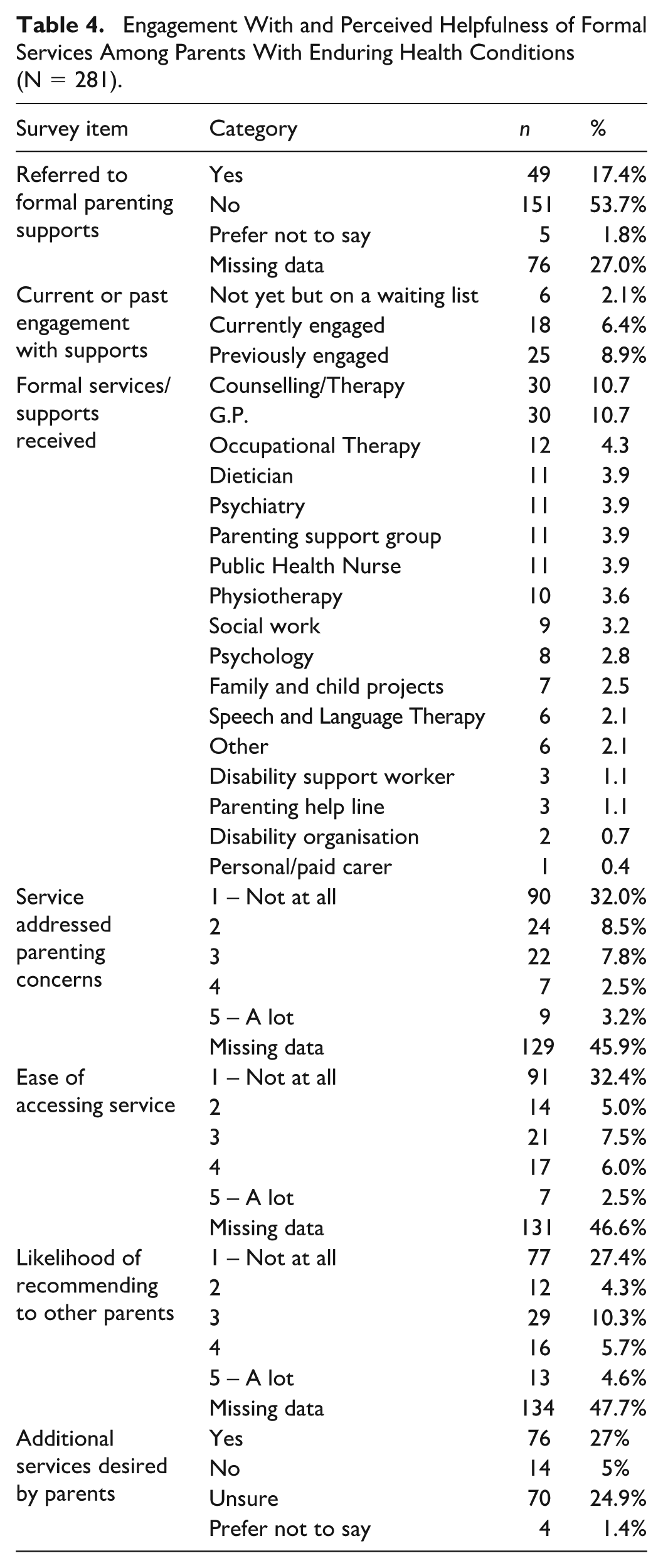
Many participants (53.7%, n = 151), had never been referred to formal services for parenting (Table 4). Few (6.4%, n = 18) were currently engaged with services, while 8.8% (n = 25) had previous experience of services. Common services accessed included general practitioners and counselling (10.7% each) and occupational therapy (4.4%, n = 12).
Engagement With and Perceived Helpfulness of Formal Services Among Parents With Enduring Health Conditions (N = 281).
Barriers to Access
Only 2.5% (n = 7) reported parenting support services easy to access while 32.4% (n = 91) described them as inaccessible. Open-ended responses (n = 143) identified barriers including lack of information (n = 18), long waiting lists, poor geographic availability and insufficient services (n = 45). Some parents felt dismissed when seeking help ‘I’ve only ever been made to feel like a nuisance” and the need for local, timely and flexible services was identified.
Acknowledgement and Validation
Satisfaction with formal services was low and 32% (n = 90) reported their concerns were ‘Not at all’ addressed, while only 3.2% (n = 9) identified ‘A lot ‘of support. Many (n = 16) expressed a need for recognition and support of their dual identity as parents and individuals with health conditions by services, “no one ever asked me about how my chronic pain impacted parenting”. Participants also highlighted the importance of culturally informed and empathetic service providers.
‘Provide support without judgement. Offer support and listen to my concerns’.
Service Delivery Gaps
Some participants (n = 23) reported that current services were poorly designed and lacked continuity of care and follow-up. Few (4.6%, n = 13) would ‘Highly recommend’ the service they had received, while 27.4% (n = 77) would ‘Not recommend the service at all’. Many (27% n = 76) wanted additional supports. Open-ended responses (n = 208) identified parent-focused service development needs in mental health services (n = 21), home-based support (n = 19), and allied health input (n = 20). Some sought peer groups for connection, emotional support and reduced isolation.
Discussion
This study provides novel insights into experiences of parenting with enduring health conditions in Ireland, identifying significant challenges, unmet needs and preferences for service delivery. Consistent with previous international research (Codd et al., 2023; Honey et al., 2024; Pituch et al., 2024), both physical and mental health challenges were associated with reduced parental capacity to fulfil key parenting roles. Our findings highlight the significant impact such conditions have on parenting roles and identify a need for more responsive, needs-led services.
Physically demanding parenting tasks, particularly, ‘Engaging in child-focused leisure’ and ‘Moving your child’ were identified as most difficult. This reflects previous research which associated chronic physical conditions with difficulties in lifting, dressing and playing with children (Codd et al., 2023; Parton et al., 2022; Pituch et al., 2022). Furthermore, ‘Managing children’s social networks’ was an identified area of difficulty, echoing previous research which reports that fatigue and disrupted routines can reduce parents’ ability to facilitate social opportunities for their children (Barnardos, 2024).
Many participants lived with multiple health conditions, and those who reported higher multimorbidity also experienced significantly greater impacts on parenting roles, reflecting the known link between multimorbidity and increased caregiving difficulty (Sand et al., 2021). Interestingly, parents with fluctuating health reported greater ease in managing some parenting tasks compared to those with stable conditions, possibly due to periods of improved functioning. However, this warrants further investigation, as symptom severity and fluctuation patterns were not measured in this study.
In addition to reporting difficulties in performing parenting tasks, parents described frustration when they were unable to meet their own expectations. Delegation of parenting tasks and reliance on others exacerbated feelings of guilt and perceived inadequacy. These findings align with existing literature, linking enduring health conditions to altered parenting roles, diminished self-efficacy and feelings of shame (Codd et al., 2023; Kuswanto et al., 2020; Pituch et al., 2022).
Our findings highlight the pivotal role of informal support in assisting parents who live with enduring health conditions. Informal support networks provided practical assistance with tasks including transport, child care, and household duties in addition to essential emotional support and opportunities for self-care. This reflects previous research which suggests that informal support can buffer stress, facilitate task delegation, and enable parents to adapt to changing capacities while maintaining their parenting roles (Codd et al., 2023; Kuswanto et al., 2020; Pituch et al., 2022). However, as our findings highlight, valuable informal support networks are not always available reinforcing the necessity of formal support services for parents.
Despite the vital role of formal support services, participants in our study reported difficulties accessing them and reported that their parenting needs were often overlooked. Existing literature indicates that health care providers frequently hesitate to address parenting issues, viewing them as private matters or beyond their professional responsibilities (Cooper et al., 2023; Fearnley & Boland, 2017; Hackett & Cook, 2016; Honey et al., 2024). Furthermore, parents with enduring health conditions may be reluctant to seek support due to fears of being perceived as inadequate, judged as unfit, or losing custody of their children (Biebel et al., 2016; Flynn et al., 2023; Hampton et al., 2022; Law et al., 2021; Pituch et al., 2022). These concerns were echoed in our study findings, with experiences of feeling judged, dismissed, or invalidated in their interactions with service providers reported. Such findings reinforce the need for responsive, non-judgemental services that acknowledge the complexities of parenting with an enduring health condition and actively listen to parents’ concerns.
Parent-focused service development and delivery should reflect the diverse and complex needs of those who depend on them (Flynn et al., 2023). The present study offers valuable insights into the preferences and priorities of parents living with enduring health conditions in Ireland. Study participants have expressed a desire for parent-focused services that are accessible and inclusive, and empathetic and responsive. The need for tailored interventions that recognise the dual responsibilities of managing enduring health conditions while parenting has been highlighted. Preferences for service delivery were mixed, with some favouring in-person support and others advocating for hybrid approaches to enhance accessibility. Combined, these findings further emphasise the importance of parent-focused services that uphold choice and accessibility while addressing the diverse and complex parenting needs of individuals with enduring health conditions.
Occupational therapy offers a promising solution to the multifaceted challenges identified by parents in this study due to its focus on enabling participation in meaningful life roles – including parenting. While published occupational therapy interventions to address parenting concerns are limited (Honey et al., 2025; McGrath et al., 2024), occupational therapy interventions for people with enduring health conditions are highly flexible and can be tailored to the specific needs of parents. Examples include: physical task adaption such as use of ergonomic baby carriers and environmental modifications to reduce physical strain, fatigue and energy conservation, including activity pacing, restructuring routines and prioritisation strategies to balance parenting activities with other roles, cognitive and emotional support through goal setting, coping strategies and therapeutic strategies to address reduced self-efficacy, support for social participation through assisting parents to plan and facilitate their children’s social activities, manage routines and engage with social and community resources, parental advocacy including education for health care professionals, collaborative planning, and connecting parents to informal and formal supports. Such interventions not only support performance of specific parenting tasks but also address emotional and social aspects of parenting with an enduring health condition. By focusing on occupational performance and participation, occupational therapy can support parents to maintain their roles, strengthen their parental identity and improve overall family wellbeing (McGrath et al., 2024).
Limitations
As with any research, this study has several limitations that should be considered when interpreting and applying the findings. The use of convenience sampling prevents us from calculating a response rate or assessing how representative our sample is of the broader population of parents living with enduring health conditions. Although efforts were made to recruit a diverse group of parents, fathers remain significantly underrepresented. This gender imbalance affects the generalisability of the results and highlights the need for research to capture fathers’ experiences. The majority of our participants reported higher levels of educational attainment and household income to national averages reported in Census 2022 data (Central Statistics Office, 2022). Specifically, a greater proportion held postgraduate qualifications, and their household incomes tended to fall within higher income brackets.
Participants with higher education and income may have greater access to resources, support networks and services, which could influence their experiences of parenting and their engagement with services. Consequently, the challenges and needs identified in this study may underrepresent those faced by individuals from lower socioeconomic backgrounds. In addition, the survey tool was specifically developed for this study. While a rigorous development process was followed, there remains a possibility that some questions were misunderstood or interpreted differently by participants. Despite these limitations, the study offers valuable initial insights into the experiences and unmet support needs of parents with enduring health conditions in Ireland and highlights the potential role of occupational therapy in supporting parenting.
Conclusion
This study reveals the significant, often overlooked challenges faced by parents living with enduring health conditions in Ireland. It underscores the urgent need for inclusive, flexible, and parent-centred supports. Provision of such supports is critical to upholding the rights of parents with enduring health conditions to parent with dignity and recognition.
Supplemental Material
sj-docx-1-otj-10.1177_15394492251391664 – Supplemental material for Parenting With an Enduring Health Condition: Experiences, Support Needs and Service Delivery Preferences
Supplemental material, sj-docx-1-otj-10.1177_15394492251391664 for Parenting With an Enduring Health Condition: Experiences, Support Needs and Service Delivery Preferences by Dearbhla Anne Quirke, Lillian Kathy Sheehan, Yvonne Codd and Margaret McGrath in OTJR: Occupational Therapy Journal of Research
Footnotes
Ethical Considerations
Ethical approval for this study was provided by the Clinical Therapies Social Research Ethics Committee at the University College Cork (CT-SREC-2024-24).
Consent for Publication
Participation in this study was voluntary. All participants were provided with a participant information statement and were free to withdraw from the study up to the point of submission of the survey response.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, so supporting data is not available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.