
Abstract
Plain Language Summary
Researchers and rural communities partnered to develop a type 1 diabetes research plan. Together, they built research skills, created a patient-focused plan, and formed a lasting partnership that continues to produce important research. This shows the value of community involvement in research.
Keywords
Introduction
Prevalence and Health Care Access
Approximately 244,000 youths and 1.6 million adults are living with type 1 diabetes (T1D) in the United States (Centers for Disease Control and Prevention [CDC], 2021), with rates expected to triple by 2050 (Imperatore et al., 2012). T1D is a complex disease requiring hypervigilance to achieve established target patient outcomes, with only 17% of youth and 21% of adults achieving targeted glycemic levels (Foster et al., 2019). The economic burden is just as worrisome, with an estimated $327 billion annual cost, or $16,750 for each person living with diabetes in the United States. Dramatic shifts in prevalence and incidence rates, especially in underserved populations (Mayer-Davis et al., 2017; Rogers, 2019), coupled with the crushing financial burden, created a need for swift action to advance the health equity of people living with T1D. Social determinants of health (SDOH), such as living in a rural community (lack of resources), can make the disease management process even more arduous.
Families living in rural areas continue to report difficulties accessing quality, up-to-date medical care congruent with current diabetes practice guidelines (Jewell et al., 2022; Kirkbride & Wallace, 2009; Krishna et al., 2010). These families typically receive care from an endocrinologist or a primary care physician, both of which have reported staffing shortages across the United States (Association of American Medical Colleges [AAMC], 2021; Lu et al., 2015; Sadhu et al., 2017). Lu and colleagues highlighted alarming data related to endocrinology access, reporting that only 1.8% of pediatric endocrinologists were in rural communities (2015). Unsurprisingly, families in rural communities are less likely to utilize necessary health care services and have documented worse patient outcomes, including worse glycemic management, mortality rates, and routine visit checkups (AAMC, 2021; Gill et al., 2022; Kobo et al., 2022; Krishna et al., 2010). Although the importance of diabetes management is well-documented to improve health outcomes, implementing evidence-based practice interventions by medical providers into clinical practice has proven difficult, especially within rural communities (Massey et al., 2010), let alone by occupational therapy providers.
One of the biggest challenges in rural health care is connecting endocrinology care teams with those living with diabetes (the University of Nebraska Medical Center, 2018). Similarly, families in Nebraska and Iowa, both largely rural states and were included in this project and must travel to larger communities to access necessary care due to shortages of endocrinologists serving rural areas (Jewell et al., 2022; Suttle, 2017). Rural communities often lack the professional support and resources to provide quality interprofessional care, much less occupational therapy (Oser & Oser, 2020; Wielandt & Taylor, 2010). A multifaceted, multipronged approach, including disciplines such as dietetics, occupational therapy, medicine, nursing, pharmacy, and social work, is imperative to provide such quality care. Providers must have comprehensive knowledge of insulin pumps and continuous glucose monitors, as these technologies are critical to successful daily diabetes management. Unfortunately, training and education on updates in technology may not reach health care providers in rural areas. The lack of experience and exposure to these systems can result in infrequent or no utilization of such devices by individuals living there (Oser & Oser, 2020).
The American Diabetes Association’s (ADA) Standards of Care (American Diabetes Association Professional Practice Committee, 2025) for youth call for the inclusion of psychosocial and behavioral interventions, such as those provided by occupational therapy practitioners, at diagnosis and routine visits. Although a variety of behavioral and psychosocial interventions have shown positive health outcomes across the lifespan for those living with type 1 diabetes, only a few include occupational therapy (e.g., Jewell, Russell, et al., 2025; Mitchell et al., 2023; Pyatak et al., 2018). Leaders within the occupational therapy emerging practice area of diabetes care and youth/adolescents have called for an increased need for the inclusion of occupational therapy services (e.g., Cahill et al., 2016; Gardener et al., 2024; Jewell, Funk, et al., 2025; Pyatak & Khurana, 2024), yet the uptake of these services into standards of care has been slow and limited (Gardener et al., 2024; Kang et al., 2024; Pyatak & Khurana, 2024). Therefore, it is imperative to utilize community-engaged research methods to more rapidly develop, test, and integrate evidence-based psychosocial and behavioral health interventions into T1D care for youth and adolescents to promote the health and well-being of individuals and families living in rural areas.
Stakeholder Engagement in Research to Elicit Health Care Change
Community-Based Participatory Research (CBPR) is a known methodology that includes stakeholders in the research process to improve health outcomes that matter to the community, advance health equity, and speed up the translation of science to practice. CBPR differs from other approaches because it relies on creating knowledge via the community instead of the research institution (Israel et al., 1998). This approach also explores a given community’s cultural and social dynamics with the research process. It emphasizes implementing outcomes that impact health and well-being in that community.
CBPR principles assert that patients are experts in their own lives. This model can produce changes in T1D policies, health care delivery, and access to proper care and provide lasting impacts after the research is concluded (Boaz et al., 2018; Hoekstra et al., 2020). A staple of CBPR is the inclusion of stakeholders in the research process from inception to dissemination. It is quickly garnering attention as a successful way to engage various community organizations, academic institutions, and patients and their caregivers as collaborative partners in health care research (Boaz et al., 2018). A recent scoping review found 17 studies that highlighted the inclusion of patient and public involvement in occupational therapy research, highlighting the increasing importance and acceptance of CBPR (Beate Rossvoll et al., 2023), none of which included those living with diabetes or had a rural focus.
CBPR is a collaborative, equitable partnership among patients, caregivers, organizations, legislators, researchers, and so on, extending beyond utilizing patients as research participants. It is known to improve the adoption and translation of evidence-based interventions. This approach engages stakeholders in the research process by selecting health priorities, collaborating on study implementation, and disseminating findings (INVOLVE, 2020). CBPR can provide lasting impacts after the research has concluded (Boaz et al., 2018), facilitating the patient’s informed health decisions and health care system change (Breault et al., 2018). This research approach reflects the health care values of all disciplines and community partners and demonstrates a team’s commitment to facilitating change in community-led health care practices. Although CBPR is quickly garnering attention as a successful way to engage clients in health care process improvement, few studies exist that fully include the community, especially patients or caregivers, in the entire research process (Cox et al., 2020; McCarron et al., 2021).
Our team identified CBPR as a mechanism to explore the health care needs of families of children with T1D, allowing them to collaborate fully and build a patient-centered research agenda. Deverka et al. (2012) defined stakeholders as “individuals, organizations or communities that have a direct interest in the process and outcomes of a project, research or policy endeavor” (p. 5). Although there is some discrepancy in the existing literature about the definition of stakeholder engagement and the boundaries and limitations of stakeholder contribution in research, it is nevertheless an increasingly customary practice in health care research due to its positive effect on quality, implementation, and project outcomes. The term stakeholders, for this project, is used to express the individuals and organizations with a vested interest or shared identity in the T1D community. The term patient denotes the individual living with T1D or their family or caregiver.
The success of this stakeholder engagement plan relied on the active participation of patients and stakeholders (e.g., health care providers, advocacy organization members, industry representatives) and specifically targeted recruitment of stakeholders with a relationship with families with a child diagnosed with T1D living in rural Nebraska and Iowa. Our plan included (1) establishing a sustainable team of rural T1D stakeholders committed to completing research capacity building and cultural humility training, (2) leading focus groups to garner additional in-depth information regarding stakeholder health needs, (3) analyzing project findings, (4) disseminating project findings to legislators, communities, and scientific conferences and journals, and (5) building a patient-centered T1D research agenda (Jewell et al., 2022; Jewell & Abbott, 2020). However, to meet the long-term objective of building a rural T1D patient-centered research agenda, it was imperative for the team first to implement a stakeholder engagement plan to fully integrate stakeholders into the entire research process. Therefore, this paper describes how our team implemented Wallerstein et al.’s (2005) four-strategy stakeholder engagement plan to build a team of committed stakeholders focused on rural T1D research, complete research capacity training, and build a patient-centered rural T1D research agenda. The four strategies of the framework included (Wallerstein et al., 2005):
Reflecting on individual and institutional capacities to engage in a partnership.
Identifying potential partners and partnerships through appropriate networks, associations, and leaders.
Negotiating or reframing the ultimate health issue(s) for research.
Creating and nurturing structures to sustain partnerships through constituency building and organizational development.
Specifically, the aims of this project were to (a) build a robust community-academic research partnership, (b) complete individual, organizational, and community-level research capacity building, and (c) develop a rural T1D patient-centered research agenda. As this paper describes an engagement plan, and it is not a human subjects research study, we have no IRB, consent processes, or data availability to report. However, Creighton University did provide IRB approval for the focus group portion of the study described briefly in this paper and elsewhere (Jewell et al., 2022).
Method
Setting
This project occurred in the states of Nebraska and Iowa in the United States due to the largely rural nature of the states, shortage of endocrinology care providers, long travel distances to clinic and hospitals, and increased incidence rates of type 1 diabetes in rural versus urban communities (Oser & Oser, 2020; Rogers, 2019).
Stakeholder Engagement Plan and Outcomes
All community and academic partners had a shared identity of either living with or formally or informally caring for a person with T1D, which allowed connectedness among stakeholders. The project leaders and several key personnel had established relationships with the T1D community before the inception of this project, which allowed for the acceleration of the project implementation. In addition, this engagement plan’s fluid yet systematic nature allowed flexibility to implement the steps as needed. This process also provided constant checks and balances (specifically before and after each weekly meeting) to diminish unintentional power discrepancies among university faculty, health care entities, and community partners.
Strategy 1: Reflection on Individual and Institutional Capacities to Engage in Partnership
The two project leads, caregivers of a child with T1D and one an academic partner and the other a community partner began reflecting on their individual and institutional capacities (see Table 1). Both leads provided care for their children with T1D. They frequently discussed the condition’s complexities related to health management routines, caregiver stress, family quality of life, and navigating a complex health care system. Many of these conversations occurred within their typical daily routines, such as at their children’s school, church, and extracurricular activities. Upon reflection on their capacities, they sought guidance and input from a multi-state advocacy organization, a vital stakeholder. To improve engagement, the project leads held all meetings at the community organization’s office building. It was imperative that the academic project lead, although a caregiver, was silent, listened with an open perspective, and was nonjudgmental toward community partners so that their voices were heard and valued. This strategy was especially crucial when the project leads initially met with the advocacy organization to discuss an opportunity to shift their previously established relationships into a formal partnership. During the meeting, the group determined that the executive director of the advocacy organization would join the community and academic project leads as the first three key personnel for the community engagement project, which simultaneously initiated the stakeholder engagement plan. Furthermore, they determined that a health care provider with expertise in diabetes management and a health care provider with rural health care expertise were needed as key personnel (see Table 1).
Stakeholders.
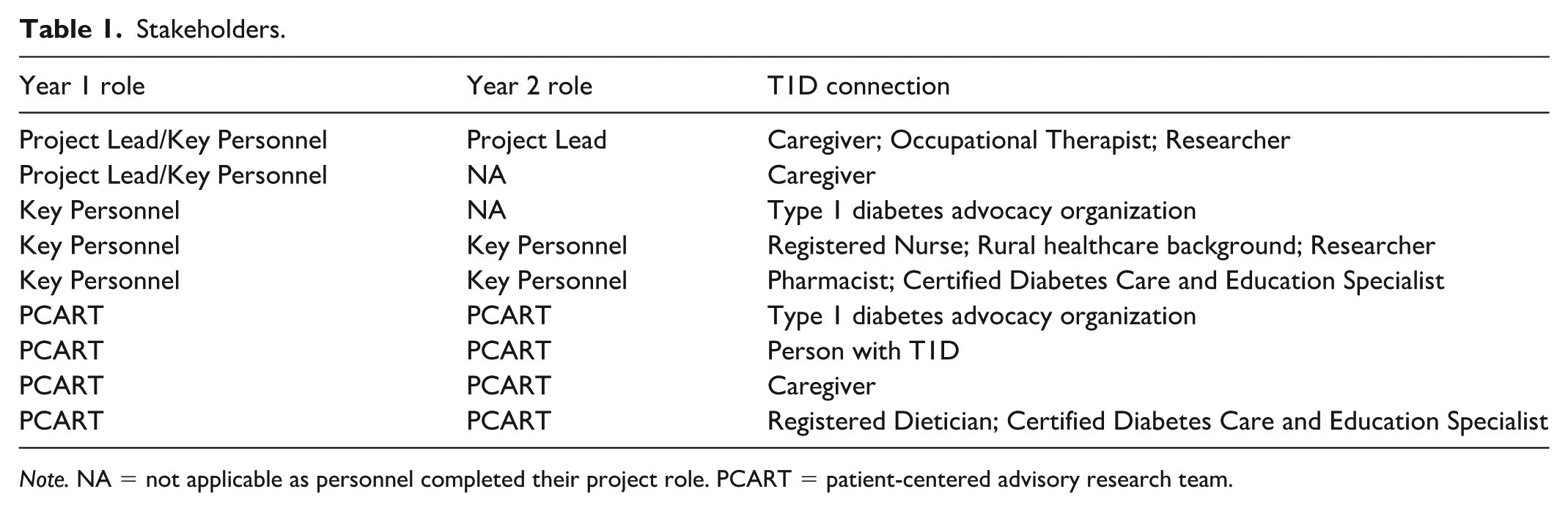
Note. NA = not applicable as personnel completed their project role. PCART = patient-centered advisory research team.
Wallerstein and colleagues’ (2005) four strategy framework emphasizes the importance of candid assessment of the strengths of the institutions and individuals involved in the project, as well as determining any power imbalances between involved institutions and the community stakeholders. The five key personnel completed an in-depth assessment of personal and institutional capacities for active collaboration. That assessment involved an analysis of group dynamics, a reflection of strengths, and strategizing to ensure the stakeholders’ voices were heard throughout the project. Examples of the team’s perceived strengths included organization skills, use of art and creativity, social media influencing, starting non-profit organizations, strong connections across rural Nebraska and Iowa, critical understanding of diabetes management at the personal and professional levels.
Stakeholders received equitable financial compensation for participation in the project and transportation expenses to minimize power hierarchies and institutional differentials (Heckert et al., 2020). Furthermore, the project team critically considered methods to intentionally deconstruct power imbalances and ensure that all stakeholder voices were heard from project inception to completion. This technique is used in CBPR to help elevate the stakeholders’ voices, evoking knowledge sharing via collaboration and hierarchical deconstruction (Harrington et al., 2019).
Further reflection on individual and institutional capacities occurred during team meetings to promote the participation of all stakeholders. For example, a chaplain not affiliated with the project facilitated a strengths-based reflection at the academic institution. This approach follows the theoretical underpinnings of positive psychology, allowing stakeholders to pursue their self-perceived talents and interests instead of focusing on improving their areas of weakness (Dunn, 2017). This approach promoted the empowerment and inclusion of all stakeholders. The project team invited stakeholders to complete reflective processes at several points throughout the project, share their strengths related to the project, and discuss how they felt they could best contribute to the team. This strength-based approach highlighted individuals’ and institutions’ areas of expertise, core beliefs, and principles, forging authentic partnerships with all stakeholders (Israel et al., 2012).
Strategy 2: Identification of Potential Partners and Partnerships Through Appropriate Networks, Associations, and Leaders
To balance key personnel strengths identified in step 1, the project team invited a pharmacist with a Certified Diabetes Care and Education Specialist certification and a nursing researcher to serve as the final two key personnel. The five key personnel had the highest level of project involvement and participated in all decision-making in Year 1, while the three academic partners and the four PCART members were included in all decision-making in Year 2. The primary role for the two community partners in Year 1 was to connect the team to harder-to-reach rural populations who would then form the PCART. The combination of an academic institution, health care practitioners, an advocacy organization, and patients/caregivers allowed for diverse perspectives and contributions throughout the entire project.
Potential partnerships were identified via networking and team member connections to the T1D community in Nebraska and Iowa to expand the stakeholder team further. Wallerstein et al. explain that researchers should invest considerable time in getting to know the community or population of interest before proposing the research partnership. It maximizes credibility with the local community and identifies the community partners that fit best with the project. Examples in this project included involvement in state-wide community outreach events such as family pumpkin patch outings, summer camps for children with T1D, charity bicycle rides, running races, fundraising galas, involvement in leadership roles in professional organizations, and volunteering at primary schools.
The next level of stakeholder involvement was developing the patient-centered advisory research team (PCART) to collaborate with key personnel on the project. All PCART members were knowledgeable about T1D challenges and had established numerous relationships among the T1D community over the years of community involvement. One unique aspect of this team was that due to the key personnel’s long-term participation in the T1D community in Nebraska and Iowa, the team was able to recruit stakeholders that are often harder to access, including parents of children with T1D living in rural communities, as well as those more readily accessible stakeholders (e.g., providers and durable medical equipment representatives). In addition to academic partners, the PCART team consisted of a registered dietician with a Certified Diabetes Care and Education Specialist distinction working in a rural community hospital, an employee of a state diabetes advocacy organization who is also living with T1D, a caregiver of a child with T1D, and a young adult with T1D with substantial advocacy expertise. All PCART community partners resided in rural communities across the state of Nebraska. See Table 1 for stakeholder details.
Strategy 3: Negotiation or Reframing of the Ultimate Health Issue(s) for Research
Current research and literature indicate inadequacies in medical and community support for caregivers and children living with T1D in rural areas (Kirkbride & Wallace, 2009; Krishna et al., 2010; Massey et al., 2010). Two factors compound the complexity of managing T1D in this setting: first, decreased access to health care, particularly to specialized health care practitioners (Suttle, 2017; the University of Nebraska Medical Center, 2018). Second is the shortage of diabetes education programs; according to the Centers for Disease Control and Prevention (2024), 62% of rural communities do not have diabetes self-management programs to help children and families meet health benchmarks. Based on this information, the five key personnel decided that the initial project focus was to gather in-depth information from stakeholders in rural communities across Nebraska and Iowa regarding barriers and challenges to accessing health care services and successfully managing their child’s diabetes care and the secondary focus was to generate potential solutions to the obstacles that families encountered in their daily lives. The process and results from this part of the project are reported elsewhere (Jewell et al., 2022).
Recognition of the children with T1D and their families as experts on their own lives and their chronic conditions was a crucial element of this portion of the stakeholder engagement plan (Haywood et al., 2019). This phase allowed for continuous negotiation, evolution, and reframing of the health issue and addressing various needs as new issues or developments arose from the perspectives of the patient and of the PCART (Wallerstein et al., 2005). The key personnel and PCART aggregated all information from the project to develop a patient-centered and driven rural type 1 diabetes research agenda. This agenda guides future research projects, centering on the dramatic family lifestyle changes after a T1D diagnosis and the lack of access to care. In addition, the research agenda supports that families use their geographic isolation as a strength by reinforcing resourcefulness and technology use in rural communities (Jewell et al., 2022). Although this is an interprofessional team with an academic-community shared leadership model, many research projects that stemmed from this engagement project are co-led by an occupational therapist and community partner(s) and develop and test novel occupational therapy interventions.
Recognizing institutional barriers and differences in beliefs and priorities among community and academic partners is essential for engagement. The PCART team, using Wallerstein’s four-strategy process, minimized these potential issues by listening and continuing to involve stakeholders in identifying the health issue and generating solutions.
Strategy 4: Create and Nurture Structures to Sustain Partnerships Through Constituency Building and Organizational Development
The fourth strategy consisted of sustaining collaboration between academic and community partners through constituency building, organizational development, and the creation of nurturing structures. Developing and maintaining long-term partnerships requires sharing resources, including facilities, personnel, access to data, and power, including decision-making, conflict negotiation, and leadership roles. Honoring commitments to the project and the community must also be prioritized, along with sharing resources and power. Examples include attending meetings on time and including the community past the project termination date. Furthermore, academic and institutional partners must commit to demonstrating cultural humility (Chang et al., 2012) for successful and trusting long-term stakeholder partnerships. Cultural humility is a process practiced across time, not just at a single point within a project. Personal attributes of “openness, self-awareness, ego-lessness, supportive interactions, and self-reflection and critique” were found to be commonly practiced when displaying cultural humility (Foronda et al., 2016, p. 211). The key personnel completed rural-focused, cultural humility capacity training in the first quarter of the project, which encouraged mindfulness of these critical concepts. The team utilized the Rural Health Information Hub (2024) and the total geographic distance (minimum of a 1-hour commute) to a pediatric endocrinologist care team to conceptualize rural for this project. (The Creighton University Center for Promoting Health and Health Equity led the 1.5-day training, which included readings, presentations, and the development of a preliminary logic model.) The five key personnel actively embodied these attributes, allowing for the creation and sustainment of the collaboration between the academic and community partners.
The five key personnel and the PCART practiced self-reflection throughout the project. The academic partners intentionally sought to diminish perceived power imbalances through various strategies. Geographic considerations were made, such as holding meetings within the community, selecting spaces considerate of geographically distant partners (e.g., various towns across the state and held in restaurants and community buildings), and picking times that respected everyone’s unique work schedules (Heckert et al., 2020). Other social strategies used to enhance collaboration were the use of first names rather than formal titles, wearing casual attire, sharing mealtimes, and planning social time to get to know one another on a personal level (e.g., a celebration of birthdays and “diaversaries,” or diagnosis anniversaries). These simple strategies strengthened the academic and community partners’ shared identity and forged long-term relationships.
The key personnel and PCART attended multiple trainings (e.g., cultural humility, community-engaged research, focus group training, analysis, and coding training) to prepare them for continuing research efforts and facilitate participation, collaboration, and camaraderie within the project. Researchers identified institutional barriers and bureaucratic roadblocks that could impact various parts of the project and actively worked to proactively address them at the individual, group, and institutional levels. Project results included continuous engagement of all stakeholders throughout the project, retention of all community partners, and meeting all project deliverables highlighted the success of the engagement plan. The team measured all project deliverables through a detailed audit trail, specifically through meeting minutes and a spreadsheet that included all deliverables and actions. Furthermore, Year 2 of the project was during the first year of the COVID-19 global pandemic, which disrupted the roles and routines of many individuals. Key personnel and the PCART successfully developed strategies to continue their partnerships despite the barriers caused by the pandemic. This team utilized Wallerstein’s four-strategy framework in a fluid and iterative process throughout the project.
Discussion
The success of this stakeholder engagement project relied on the identification of a shared T1D identity, successful networking and community relationship-building, and a demonstration of cultural humility and consideration of various rural social determinant’s of health from the project’s inception. Adverse social circumstances, particularly in rural areas, hinder the optimal management of diabetes multimorbidity. Furthermore, in underresourced communities, the intersecting factors of the disproportionate burden of diabetes risk, geographic barriers to accessing quality care, underdeveloped health infrastructure, and diminishing critical resources such as broadband connectivity and transportation (modifiable social care needs) have exacerbated diabetes outcomes. Similarly, the 2019 National Academies (NASEM) report supports that (a) improvements in health outcomes and well-being within health care systems critically depend on addressing adverse SDOH, and (b) there is a growing need to understand how to best integrate medical and social care to tackle upstream factors that occur outside of clinical visits. For long-term impact, diabetes prevention and management must recognize and utilize the concept of whole-systems integrated care (including occupational therapy), which combines support for social care needs with medical care delivery. Specifically, in our project, the key personnel completed capacity-building trainings centered on thoughtful consideration of rural SDoH (e.g., income, employment, transportation, healthy foods, internet, and access to health food) and how these may impact the successful implementation of the proposed project. The team was successful in budgeting for items to offset potential negative impacts of these SDoH (e.g., providing child care, meeting in rural communities, scheduling meetings outside of work hours, covering transportation costs, and providing food during meetings).
The academic partners carefully considered stakeholder needs and deconstructed naturally occurring power hierarchies. Finally, utilizing a strengths-based approach facilitated the full inclusion of stakeholders in the project. Using a strengths-based approach is common in occupational therapy practice and is a natural extension into occupational therapy research. The stakeholder engagement plan was successful due to the 100% retention rate during the project and 2 years after completion. Although our team experienced high levels of community engagement, as demonstrated by the continued engagement of stakeholders in additional grants and research projects, there has been a slow uptake of full inclusion of stakeholders in the research process across the scientific community. This finding is consistent with results from a recent review by Cox et al. (2020) of research studies aimed at including stakeholders in research as more than just participants. Of the 123 studies in the review, only 39% had some level of stakeholder engagement, and two included stakeholders throughout the entire research process from conceptualization to dissemination. Health care researchers are only beginning to fully engage stakeholders in research. However, it is encouraging to see that funding agencies such as PCORI and the National Institutes of Health prioritize the inclusion of stakeholders in research and offer national centers to assist researchers in improving their conceptualization and utilization of community-engaged research methods (NIH; PCORI).
One explanation for the minimal inclusion of stakeholders in the research process may be the lack of a stakeholder engagement plan (Saunders & Girgis, 2010). Without a framework or logic model, community and academic partners may feel unprepared to form and sustain partnerships. Community-engaged research teams could consider a framework such as the Pathways to Population Health (P2PH; Bolender et al., 2019) or the PCORI engagement resources (Patient-Centered Outcomes Research Institute, 2025) to use for developing engagement plans. These frameworks offer alternative options to Wallerstein’s engagement plan, utilized in our project. Community-engaged research teams are encouraged to select a framework that best fits the needs of their specific teams and proposed projects. Finally, a continuation of the status quo where academic institutions drive research questions and methodologies, and stakeholders are utilized as participants only, is engrained in the academic culture, causing additional barriers to completing community-engaged research methodologies, such as CBPR. Researchers and stakeholders are encouraged to develop meaningful relationships as the first step to dismantling community-academic partnered research barriers.
It is recognized that establishing these initial relationships may seem daunting to early-stage investigators or researchers without previously established community connections. Heckert et al. (2020) identified challenges in building and maintaining relationships when engaging communities, as it is a very time-intensive process. Successful initial relationship-building strategies include identifying a shared identity and a commitment to cultural humility. Academic partners and researchers must be ready to listen to the stakeholders’ needs while setting aside their research agenda (Duran et al., 2013). Authentic, positive interactions, mutual respect, and understanding are also imperative as each party fully engages in the project and communicates effectively. These actions enhance the connection among all parties, especially when establishing new relationships. Heckert et al. (2020) also found that relationships were strengthened when teams leveraged relationships with advocacy organizations and recruited via professional and community events, as was done in this project. As the team collaborated with advocacy organizations, they built trust and accelerated networking across two states. This strategy may benefit early-stage investigators or researchers residing in a new community. For some, long-standing relationships may not be established, so using these strategies and creating opportunities for socializing with face-to-face gatherings and other project-oriented events are beneficial.
Although occupational therapy practice with those who live with T1D is an emerging area of practice, there is a growing interest in the inclusion of occupational therapy services within endocrinology. Recent studies include promising findings to support occupational therapy with youth (Gardener et al., 2024; Jewell, Russell, et al., 2025), young adults (Pyatak et al., 2018, 2025), and mothers (Haines et al., 2023) living with T1D. Furthermore, occupational therapists may use the rural T1D research agenda developed during this project to inform their clinical practice by addressing the dramatic family lifestyle changes, providing telehealth occupational therapy services to address limited health care access, and using a strength-based approach that capitalizes on the families’ resourcefulness and desire to use technology. Although use of community-engaged research methods is somewhat novel within occupational therapy practice, it is imperative to achieve optimal health outcomes prior to developing, testing, and implementing evidence-based interventions into care (Kang et al., 2024).
Limitations
One limitation of this project was the difficulty recruiting racially and ethnically diverse stakeholders, which may have provided new insights and opportunities for the team (Haywood et al., 2019; Israel et al., 2012). Difficulty recruiting stakeholders of varied ethnicities continued despite training from several health care diversity organizations; dedicating funds for translators, travel, and child care services for families; disseminating flyers and other recruitment materials in multiple languages; and utilizing community “gatekeepers” throughout the stakeholder engagement plan. However, it was not surprising that recruiting a diverse stakeholder team was difficult, as it is common for stakeholders who engage in the research process to have high English-language verbal and written proficiency skills, have internet access, and be from middle to high socioeconomic backgrounds (Joyce et al., 2017; Lauckner & Stadnyk, 2014; Player et al., 2014). Furthermore, the racial and ethnic backgrounds of individuals living in rural Nebraska and Iowa are over 80% non-Hispanic whites. The largest prevalence rates for those living with T1D in the United States are non-Hispanic whites (cite). Nonetheless, research teams must engage with historically minoritized populations to ensure that findings can generalize to various populations and that health inequities can be addressed.
Conclusion
Utilizing CBPR principles, stakeholders could fully express their expertise on living with or caring for someone with T1D in a rural community and developing a stakeholder engagement plan before research can create equal partnerships among stakeholders. The collaborative nature of stakeholder inclusion can lead to increased community trust and ownership of future research project findings. Therefore, building and sustaining community relationships is imperative to form more meaningful and impactful health care research projects to help children with T1D.
Footnotes
Acknowledgements
We would like to thank our community partners and additional research team members: Benjamin Feiten, Kameran Dostal, Vicki Brown, Laura Eberly, Kim Radenz, Sadie Schultes, Shelby Hoffmann, Dayna Sur, and Emily Ludwig. Furthermore, we would like to thank John Stone, MD, PhD, and Omofolasade Kosoko-Lasaki, MD, MSPH, for training the team on cultural humility, diversity, and inclusion.
Ethical Approval
This is not a research study; therefore, we do not have IRB approval.
Informed Consent Statement
This project did not include research participants and therefore was not required to have consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: This work was supported by the Patient-Centered Outcomes Research Institute (grant number 10443); Creighton University Center for Undergraduate Research and Scholarship; and the Creighton University School of Pharmacy and Health Professions Student Research Fellowship.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This is not a research study and therefore does not have data.