
Abstract
This study investigated the relationship of chores participation, diabetes management self-efficacy and transition readiness among adolescents with diabetes. Fifty-four youths participated (average age 13.5 years). The CHORES survey evaluated chore participation, the STARx questionnaire assessed health care transition readiness, and the Perceived Diabetes Self-Management Scale (PDSMS) assessed self-efficacy. Results showed that involvement in chores was positively correlated with transition readiness scores (r = .404, p < .05) and important subdomains of transition, namely self-management and provider communication. Mediation analysis found that self-efficacy significantly influenced the link between chores and transition readiness. This suggests that when adolescents assume more household responsibilities, they may develop greater confidence in managing their diabetes, which in turn enhances their readiness for the health care transition. Encouraging chores participation can improve transition readiness directly and indirectly, through self-efficacy. Understanding these mechanisms is key in designing patient education programs, or psychosocial interventions to support transition. Implications for health care providers and parents are discussed.
Plain Language Summary
The transition from pediatric to adult health care is a crucial phase for adolescents and young adults, particularly those with chronic conditions like diabetes. Practical daily responsibilities, self-management of diabetes, and beliefs in one’s ability to complete self-care can influence adolescents’ readiness to transition from pediatric to adult health care. This study evaluated the relationship of household chores participation, diabetes management self-efficacy and the readiness of adolescents to transition to adult health care. Fifty-four adolescents with an average age of 13.5 years participated. The CHORES survey measured their involvement and independence in doing chores, the STARx questionnaire assessed their health care transition readiness, and the Perceived Diabetes Self-Management Scale (PDSMS) evaluated their self-efficacy. The study found positive correlations between chore participation and transition readiness, particularly in self-management and provider communication. More involvement in chores was linked to better transition readiness, self-management, and communication with health care providers. In addition, chore participation was positively related to self-efficacy, which in turn improved transition readiness. Mediation analysis showed that self-efficacy can play a significant role. These findings have important implications for health care providers and parents in developing strategies to support these adolescents.
Keywords
Diabetes impacts a significant portion of the population, with prevalence among children rising steadily over the past two decades (Centers for Disease Control and Prevention, 2024). As this trend continues, it is increasingly important to identify factors that improve pediatric diabetes care to support self-management and facilitate a smooth transition to adult health care. Adolescents’ diabetes outcomes are influenced by a range of internal and external variables, such as adherence and self-care, disease perceptions, social and familial support, relationship with parents, patient education, environment, self-efficacy (Hunter, 2016).
Effective diabetes management requires strict adherence to a complex treatment regimen, including self-care tasks such as blood glucose monitoring (BGM), dietary adjustments, and insulin administration (Hunter, 2016). Consistent participation in self-management activities and adherence to recommended nutritional and exercise regimens is critical (Helgeson et al., 2008; Padma et al., 2012; Paterson et al., 1998). Social and familial support plays a vital role in assisting youth with diabetes management, treatment adherence and transition preparation. Studies have shown that family and social support promote adherence by assisting the individual with disease management tasks and providing education and support that instills optimism, enhances self-esteem, and reduces illness-related stress (Hunter, 2016; Johnson et al., 2015; Kovacs Burns et al., 2013). Young children depend largely on their parents to manage routine aspects of their illness, but as they mature, they are expected to assume greater responsibility for their own care (Hanna, 2012; Hanna & Guthrie, 2003; Holmes et al., 2006; Hunter, 2016; Wiebe et al., 2014).
Autonomy in diabetes self-care is critical for health outcomes. Teaching individuals to become independent, responsible, and self-reliant starts at an early age as becoming autonomous is an important aspect of youth’s psychosocial development (Larson, 2000; Ruiz & Yabut, 2024). Transition from parental responsibility for diabetes care to joint responsibility and then on to young adult responsibility are important steps to optimize diabetes outcomes for pediatric patients (Cameron et al., 2008). The transfer of responsibility for diabetes management is task-specific and may begin earlier for certain components of the treatment regimen (Leocadio et al., 2023; Nightingale et al., 2019). For example, implementing nutritional changes can be easier when children are diagnosed early whereas measuring blood sugar and insulin dosage often poses greater difficulty resulting in delayed independent self-management (Richards et al., 2013; Streisand & Monaghan, 2014). Parental overinvolvement and adolescent–parent concordance on responsibilities for diabetes care (e.g., agreement on BGM responsibilities) are important determinants of metabolic outcomes (e.g., HbA1c levels and diabetic ketoacidosis episodes) in adolescents with diabetes (Cameron et al., 2008).
Participation in household chores may promote the development of autonomy and independence in diabetes management. Engagement in developmentally appropriate roles, including chores and responsibilities, has been shown to support the sense of competence, personal agency, and autonomy in children (Amaral et al., 2014; Blum, 1992; Dunn & Gardner, 2013; Whitehouse et al., 2013). Routine participation in chores was found to benefit children in educational outcomes, social engagement, and life satisfaction (White et al., 2019). Child routines (e.g., household and homework responsibilities) moderate the stress associated with daily hassles and support psychological adjustment (Bridley & Jordan, 2012).
Chores participation is also beneficial for the health outcomes of youths with chronic illness. Richards et al. (2021) found that chores participation predicted overall health care transition readiness in children with different chronic illnesses. Of the three subdomains of health care transition tested (chronic illness self-management, disease knowledge and communication with provider), Richards et al. (2021) found that chores participation positively correlated with successful performance in patient-provider communication.
Self-efficacy, or the belief in one’s own ability to successfully perform specific tasks or manage situations to produce a desired result (Lee et al., 2021) is critical for treatment adherence and health outcomes of individuals who are chronically ill (Johnson et al., 2015; Reed-Knight et al., 2014). Self-efficacy is particularly important in relation to health care and health-related tasks such as scheduling health appointments, talking with health care providers, and filling and picking up prescriptions (Treadwell et al., 2016; Uzark et al., 2020). Self-efficacy strongly impacts health promoting behavior, diabetes self-care, health outcomes and successful health care transition (Alwadiy et al., 2021; Garvey et al., 2020; Hurst et al., 2020; Reed-Knight et al., 2014; Wang et al., 2023). Low self-efficacy is a predictor of poor treatment adherence among adolescents, and it moderates the relationship between diabetes management and parental involvement (Palmer et al., 2009; Wiebe et al., 2014). It is also a key mediator of social support with diabetes self-care and clinical outcomes (Chan et al., 2020).
Transition readiness is associated with better glycemic control, which may signal that transition readiness is critical for diabetes outcomes (Alwadiy et al., 2021). Transition readiness is the degree to which adolescents with chronic conditions are prepared to transition from pediatric to adult care (Richards et al., 2021). This readiness is reflected in disease knowledge, self-management, and communication skills with providers and impact successful transition outcomes (Richards et al., 2021). The transfer of self-care responsibilities should be based on the adolescent’s attitudes and knowledge, rather than age or developmental stage (Hanna & Decker, 2010; Holmes et al., 2006). Based on this recommendation, it is critical to understand the relationship between self-efficacy, transition readiness, and diabetes management in youth with diabetes.
Research has demonstrated that participation in household chores is associated with increased self-efficacy among youth and adolescents with chronic conditions (Riggio et al., 2010; White et al., 2019), which, in turn, supports a smoother transition to adult health care. While self-efficacy, transition readiness, and chore participation are recognized as interrelated factors, the specific nature of their relationships remains insufficiently understood. The present study aimed to further examine the associations among these variables within a sample of children and adolescents.
Methods
Participants and Procedure
Researchers recruited participants from the [redacted for blinded review]. Parent-child dyads meeting inclusion criteria were invited to participate. To meet inclusion criteria, child participants needed to be between 8 and 17 years of age, a diagnosis of either T1D or T2D, and a valid email address. Each dyad received a US$50 incentive for participation. The University Ethics committee approved this study.
The medical director of the Pediatric Diabetes Program created a list of current patients who met inclusion criteria. Members of the study team recruited participants in-person at the Pediatric Diabetes clinic and online. The team emailed patients’ families with links to complete the study through the web-based survey engine, Qualtrics. Researchers provided each family with two sets of questionnaires: a parent and a child version. Researchers emailed 342 parents of patients with invitations. In total, 54 parents and youth dyads completed the surveys yielding a 17% response rate. A small group of 14 dyads completed the data collection in-person while the remaining 40 dyads participated through Qualtrics. Child self-reported data were used for the current analysis. The study team will provide the data upon request.
Measures
Demographic and Diabetes Information
Parent and youth participants reported age, sex, type of diabetes, age of diagnosis, complications due to diabetes, household income, number of family members living in the household, and insurance status. Current age and diagnosis were used to calculate the time spent living with diabetes.
Chores
Researchers assessed chores participation and level of assistance needed in completing chores using the Children Helping Out: Responsibilities, Expectations, and Supports (CHORES) survey (Dunn, 2004; Dunn et al., 2014). Both youth and parents completed the survey to assess youth participation and assistance with household chores. CHORES utilizes 34 items to evaluate two different aspects of household work: performance and assistance needed. The same set of questions are ranked on two different scales to determine the assistance and performance aspects of household participation of the child (from self and parent’s perspective). The CHORES is reported to have strong test–retest validity and internal consistency (Dunn, 2004).
Performance Version of CHORES
For the performance version of the CHORES survey (pChores), participants (child and parent) answer the 34 questions through a dichotomous, yes-no scale that measures the level of age-appropriate involvement in household tasks. Total performance is calculated by adding all yes responses. Scores can range from 0 to 34. Higher scores indicate a greater extent of age-specific participation in household tasks. The instrument has robust psychometric properties. In the current child sample, the reliability calculated for the performance version of CHORES (pChores in Table 2) demonstrated a KR-20 value of .88.
Assistance Version of CHORES
To quantify assistance (aChores), the same 34 items are evaluated using a 7-point Likert-type scale by both child and parent (0 = child is not expected to perform task to 6 = child performs task on own initiative more than 50% of the time). The total assistance score is transformed into a 100-point scale according to the formula developed by Dunn (Dunn, 2004). Total assistance scores may range from 0 to 100. A higher score on this scale indicates a higher level of independence in task completion. For our study, the assistance version of CHORES (aChores) achieved a Cronbach’s α of .90 in the child data set.
Subscales of CHORES
Each of the above-described scales, pChores and aChores, can be further used to assess performance or assistance toward self-care or family care. Of the 34 items, 13 items factor into self-care type tasks, and 21 factor into family care. The Self-Care subscale references household tasks primarily affecting the child, such as “Makes self a hot meal,” in terms of performance (independent execution) as well as assistance needed (pChores Self-Care Subscale and aChores Self-Care Subscale, respectively). The possible score range for pChores self-care subscale is 0 to 13 while the score range from aChores self-care subscale is 0 to 38. The Family Care subscale references household tasks the child is involved with that benefit the entire household, such as “Picks up area shared by others,” in both terms of performance and degree of assistance required (pChores Family Care Subscale and aChores Family Care Subscale, respectively). The possible score range for pChores family care subscale is 0 to 21, and the possible score range for aChores family care subscale is 0 to 62. Both subscales have reported strong internal consistency with the Self-Care subscale’s Cronbach’s α = .96 and the Family Care’s Cronbach’s α = .98 (Dunn, 2004; Dunn et al., 2014). The Cronbach’s αs computed in our study’s child subsample were .83 for the Self-Care subscale and .91 for the Family Care subscale.
Health Care Transition Readiness
To determine health care transition readiness, youth participants answered the Self-Management and Transition Readiness questionnaire (STARx; Ferris et al., 2015). This self-report measure is 13-items in which participants answer on a 5-point Likert-type scale (1 =Never to 5 = Always). Total score is determined by summing all responses, leading to a score range of 13 to 65 with a higher score indicating a higher degree of readiness to transition. Reported Cronbach’s α for the STARx scale is .80 (Ferris et al., 2015). Our study found a Cronbach’s α of .85. The STARx questionnaire has three subscales: Self-Management, Disease Knowledge, and Provider Communication. The Self-Management subscale has 5 items leading to a possible score range of 5 to 25 and evaluates the participant’s ability to engage in disease management tasks with questions like “How often do you make an effort to understand what your doctor told you?.” The Disease Knowledge subscale is four items and determines participant’s understanding of their disease (“How much do you know about taking care of your illness?”). Possible scores for this subscale range from 4 to 20. The Provider Communication subscale is 4 items (possible score range between 4 and 20) and assesses respondent’s ability to interact with the treatment team (“How easy or hard is it to talk with your doctor?”). Previous studies reported Cronbach’s alphas of .73 for Self-Management, .76 for Disease Knowledge, and .63 for Provider Communication (Ferris et al., 2015). Cronbach’s alphas for our study were .75, .62, and .56, respectively in the child data set.
Self-Efficacy
Self-efficacy was measured using the Perceived Diabetes Self-Management Scale (PDSMS) (Wallston et al., 2007). This eight-item self-report questionnaire measures confidence in disease management abilities through a 5-point Likert-type scale response (1 = Strongly Disagree to 5 = Strongly Agree) resulting in a possible score of 8 to 40 with a higher score indicating greater perceived self-efficacy. Reported Cronbach’s alpha of the PDSMS was .83, and our study found a Cronbach’s alpha of .83 in the child data set.
Results
Participation Characteristics
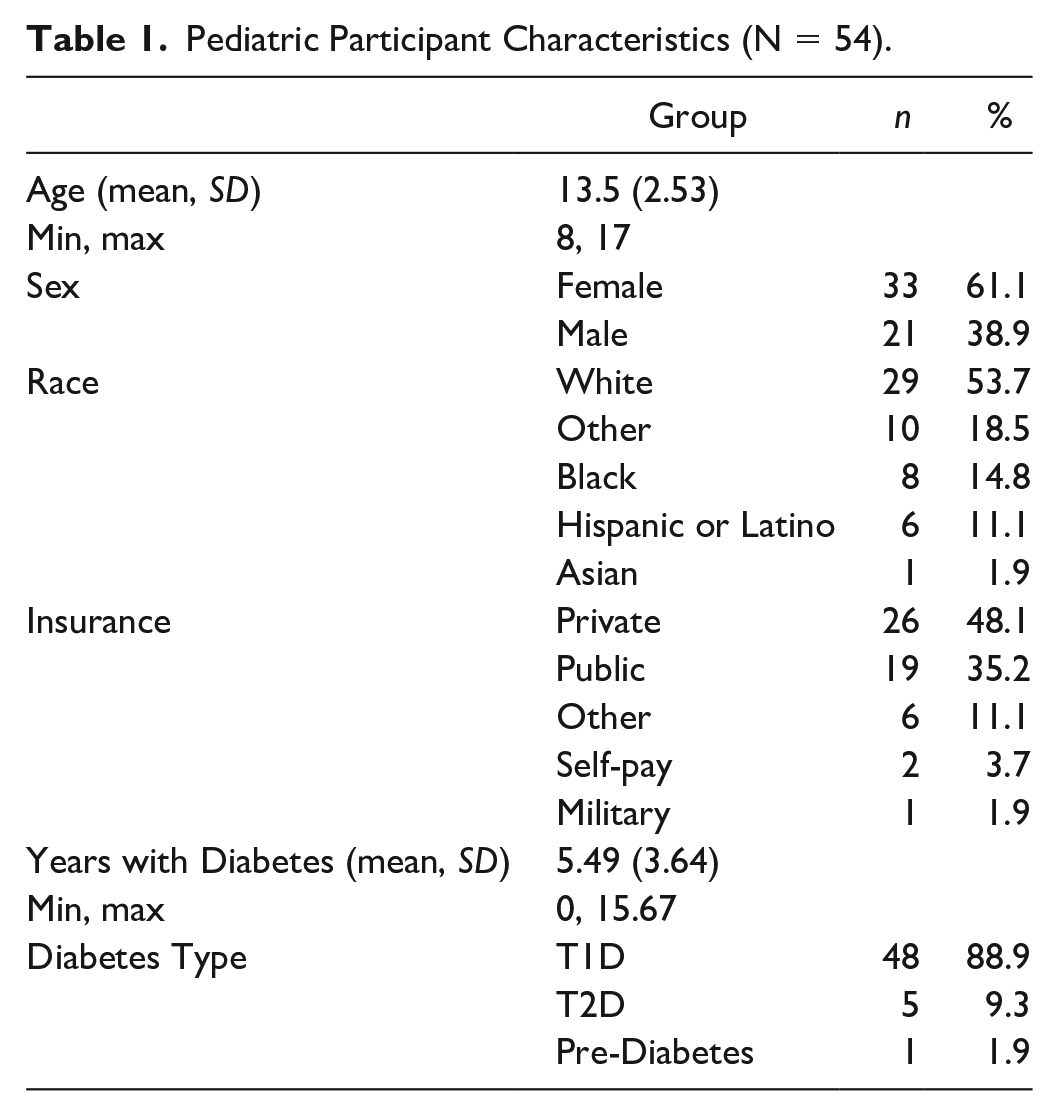
Participant characteristics are outlined in Table 1. Fifty-four children and one of their parents were enrolled in the study with most pediatric participants being White, female, and 14 or older. Nearly all participants had health insurance. The average time since diagnosis was approximately 5.49 years.
Pediatric Participant Characteristics (N = 54).
Associations Between Chores and Health Care Transition Readiness
To determine the relationship of chores (CHORES), diabetes management self-efficacy (PDSMS) and health care transition readiness (STARx), Pearson’s correlations were computed. The performance CHORES scales (pChores), diabetes management self-efficacy (PDSMS) and STARx scores are outlined in Table 2. There were significant positive correlations between the overall pChores scale and the overall STARx scale (r = .404, p < .05), the STARx Self-Management subscale (r = .33, p < .05), and the STARx Provider Communication subscale (r = .383, p < .05). The pChores Self-Care subscale was significantly positively correlated with the same STARx scales (r = .437, p < .001 for overall STARx scale, r = .430, p < .001 for STARx Self-Management subscale, r = .350, p < .05 for STARx Provider Communication subscale). Similarly, the pChores Family Care subscale was significantly positively correlated with the overall STARx scale (r = .341, p < .05) and the STARx Provider communication subscale (r = .361, p < .05). Diabetes-management self-efficacy was positively correlated with pChores Self Care subscale, STARx overall scores, and STARx Disease Knowledge and STARx Self-Management (see Table 2 for r statistics, and p-values).
Associations Between Participation CHORES, PDSMS and STARx Scores.
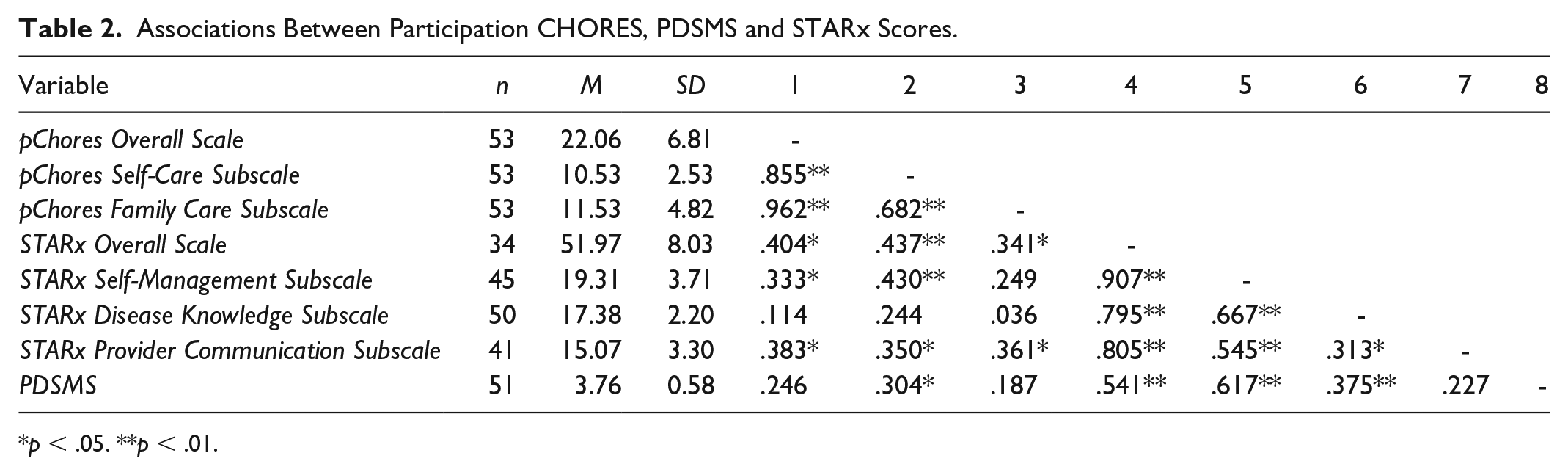
p < .05. **p < .01.
Correlation results between the assistance CHORES scales (aChores), diabetes management self-efficacy (PDSMS) and STARx scale scores are displayed in Table 3. The aChores overall scale was positively significantly correlated with the STARx overall scale (r = .548, p = .001), the STARx Self-Management subscale (r = .416, p = .05), and the STARx Provider Communication subscale (r = .452, p = .001). The aChores Self-Care subscale was also significantly positively correlated with the same scales (r = .520, p = .001; r = .474, p = .001; r = .406, p = .001, respectively). The aChores Family Care subscale was significantly positively correlated with the overall STARx scale (r = .454, p = .001) and the STARx Provider Communication scale (r = .393, p = .05). Diabetes-management self-efficacy was positively correlated with pChores Self Care subscale, aChores Family Care, STARx overall scores, and STARx Disease Knowledge and STARx Self-Management (see Table 3 for r statistics, and p-values).
Associations Between Assistance CHORES, PDSMS, and STARx Scores.
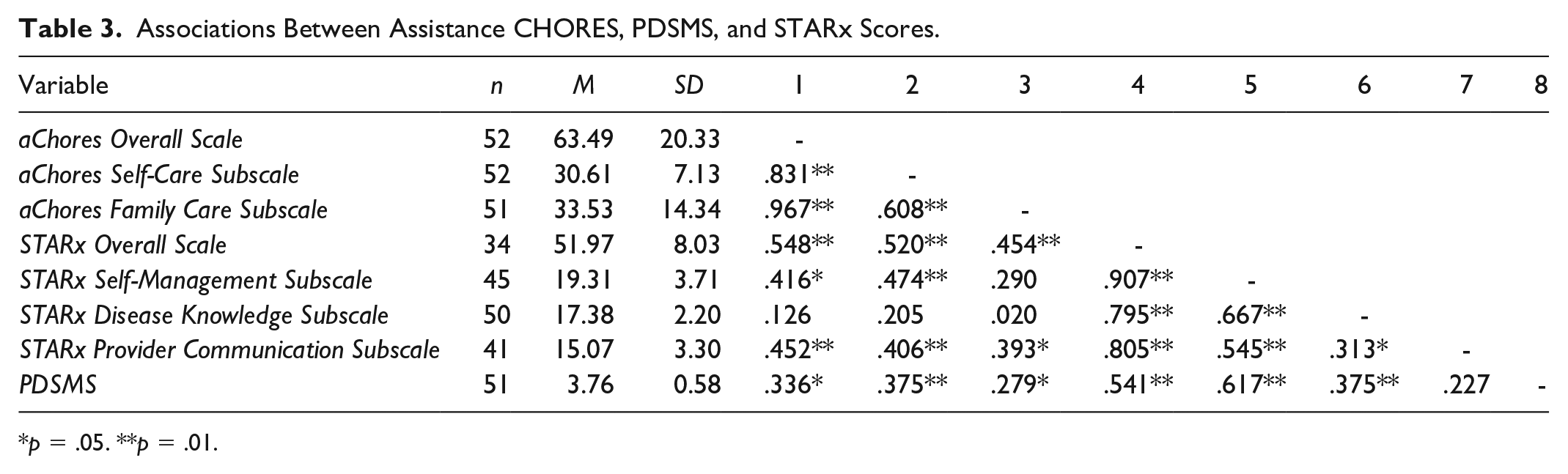
p = .05. **p = .01.
Self-Efficacy as a Mediator
To determine the effect of self-efficacy (PDSMS) on the relationship between chores and health care transition readiness, mediation analysis was completed using a series of regressions. First, regression was used to determine if there is a significant relationship between chores, the predictor variable, and self-efficacy, the mediating variable. Next, another regression was run to determine the relationship between chores, the predictor, while controlling for self-efficacy, the mediator, while noting the effect of the mediator on health care transition readiness, the outcome variable. Finally, a regression was completed to determine the effect of the predictor variable on the outcome variable without controlling for the mediator.
Results from these regressions are presented in Tables 4 and 5. The mediation analysis indicated that diabetes management self-efficacy (PDSMS scores) fully mediated the following relationships: pChores Self-Care subscale and the overall STARx scale, aChores Family Care subscale and STARx overall scale, pChores Self-Care subscale and STARx Self-Management subscale, aChores overall subscale and STARx Self-Management subscale, aChores Self-Care subscale and STARx Self-Management subscale, and pChores Self-Care subscale and STARx Disease Knowledge subscale. The mediation analysis also found that diabetes management self-efficacy (PDSMS scores) partially mediated the following relationships: aChores overall scale and STARx overall scale as well as aChores Self-Care subscale and STARx overall scale.
Self-Efficacy as a Mediator Between Performance in Chores and Health Care Transition Readiness.
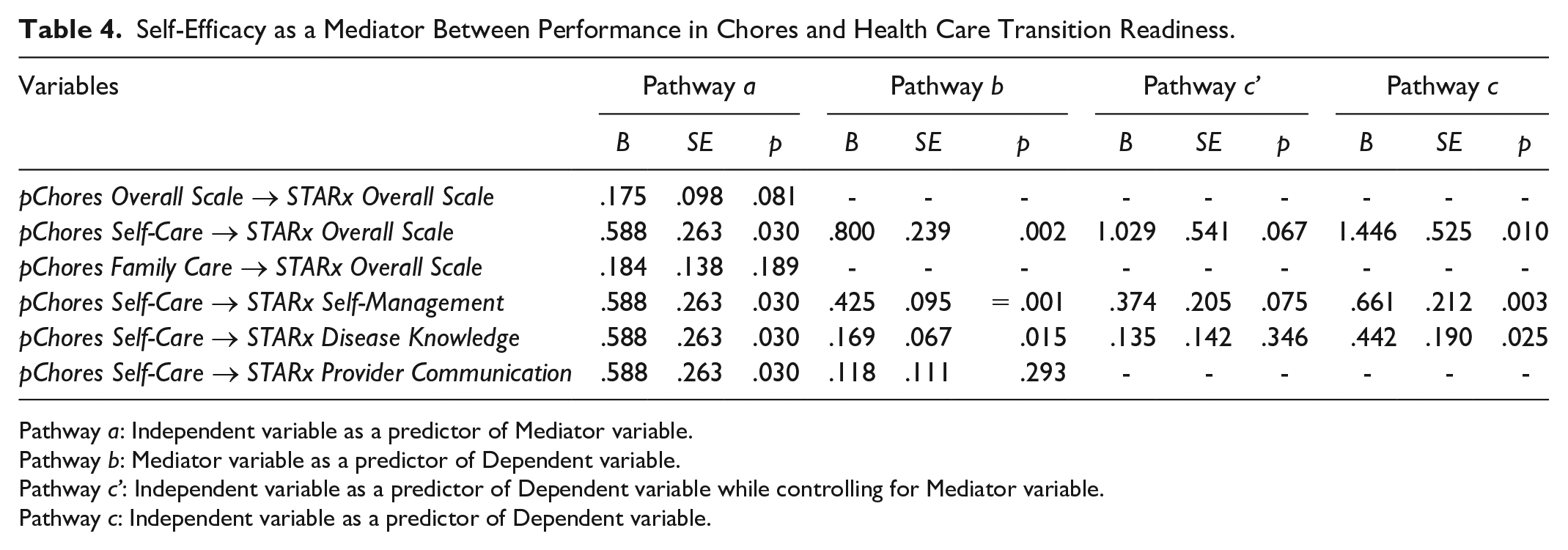
Pathway a: Independent variable as a predictor of Mediator variable.
Pathway b: Mediator variable as a predictor of Dependent variable.
Pathway c’: Independent variable as a predictor of Dependent variable while controlling for Mediator variable.
Pathway c: Independent variable as a predictor of Dependent variable.
Self-Efficacy as a Mediator Between Assistance in Chores and Health Care Transition Readiness.
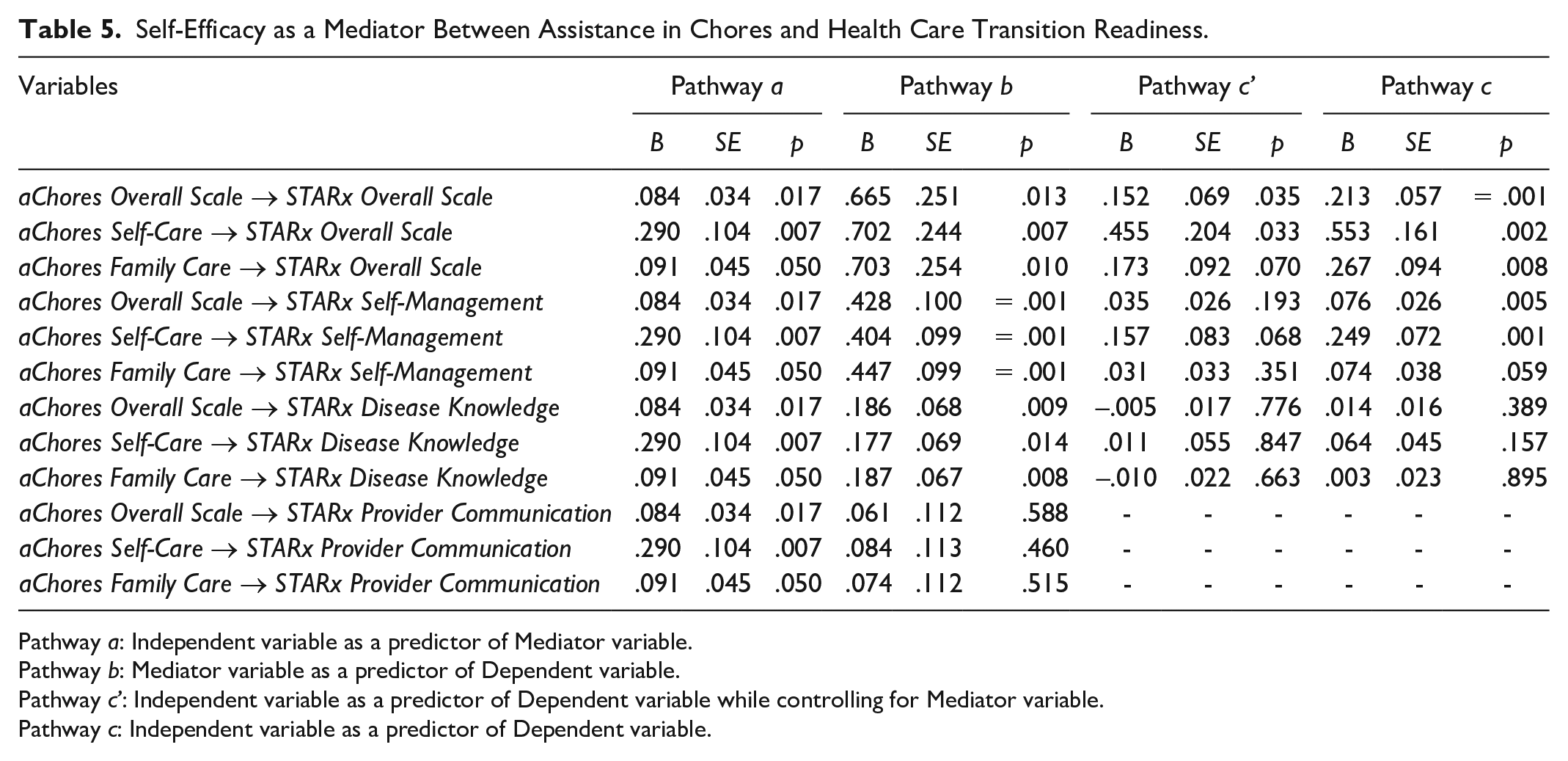
Pathway a: Independent variable as a predictor of Mediator variable.
Pathway b: Mediator variable as a predictor of Dependent variable.
Pathway c’: Independent variable as a predictor of Dependent variable while controlling for Mediator variable.
Pathway c: Independent variable as a predictor of Dependent variable.
Discussion
Transition readiness and a seamless transfer to adult health care are critical for achieving optimal health outcomes and overall well-being. However, health status may decline during this period for various reasons (Campbell et al., 2016), highlighting the importance to better understand and support youth throughout the transition process. A recent study of adolescents and young adults with diabetes found that while many felt confident in managing routine self-care tasks related to transition readiness (e.g., insulin administration and blood glucose monitoring), they were less confident in recognizing or preventing complications (Bryant et al., 2024). Addressing gaps like these is essential for delivering effective, targeted patient education and support.
Our primary variable of interest, chores participation, was positively associated with overall transition readiness, as well as with two specific subdomains: diabetes self-management and independence in communication with health care providers. These findings are consistent with our earlier research (Richards et al., 2021). With a more nuanced assessment of chores, current findings reflect that greater autonomy in both self-care and family-care-related tasks—indicated by higher participation and reduced need for assistance—was positively correlated with transition readiness scores. This aligns with Hong and Im’s (2024) work, which highlights the importance of reduced parental overprotection and increased autonomy support in promoting transition readiness. Similarly, White et al. (2019) reported that engaging in chores during childhood was positively linked to the development of self-competence, self-efficacy, and prosocial behaviors later in life. Taken together, these findings suggest that increased participation in household tasks, coupled with reduced reliance on assistance, may foster independence and a stronger capacity for managing health-related responsibilities.
Our findings indicate that engagement in household chores is associated with enhanced self-efficacy, suggesting that routine responsibilities offer children and adolescents valuable opportunities to develop confidence in managing tasks independently. This aligns with previous research demonstrating the benefits of structured routines not only for psychological well-being, such as less behavioral problems, but also for chronic illness management (Bridley & Jordan, 2012). The consistency and predictability inherent in chores and daily routines may be especially beneficial for youth with chronic conditions, as they help mitigate disease-related stress and foster the development of self-care skills critical for transition readiness (Bridley & Jordan, 2012). By participating in household tasks, adolescents with chronic illnesses may gain confidence in their ability to perform daily health-related responsibilities, a finding also supported by Albalawi (2016).
Self-efficacy plays a significant role in promoting positive health outcomes and transition readiness. In diabetes care, for example, self-efficacy has been identified as a key predictor of critical outcomes, including blood glucose regulation and effective self-management behaviors (Chan et al., 2020; Hurst et al., 2020; Wang et al., 2023). Our study demonstrates that higher self-efficacy is positively associated with greater readiness for the transition to adult health care, consistent with findings reported in previous research in adolescents with chronic illnesses (Albalawi, 2016; Combs, 2021; Lang et al., 2025; Varty et al., 2022).
Importantly, self-efficacy has been identified as a key mediator in the relationship between various psychosocial factors and diabetes-related outcomes. Previous research has confirmed self-efficacy as a mediator between social support and diabetes self-care behaviors (Chan et al., 2020), as well as between resilience and diabetes self-management (Wang et al., 2023). In addition, self-efficacy has been shown to mediate associations between sociodemographic factors and adherence to self-management among individuals with both diabetes and hypertension (Xie et al., 2020). In our study, diabetes management self-efficacy was found to partially or fully mediate the relationship between participation in household chores (both self-care and family-related tasks) and overall transition readiness, as measured by the STARx total score. Similarly, self-efficacy mediated the relationship between chore participation and diabetes self-management, reflected in scores on the STARx self-management subscale. These findings further support the central role of self-efficacy in preparing youth for the transition to adult health care.
Self-efficacy is a modifiable psychological construct with well-established benefits for health-related quality of life (Engel et al., 2019) and should be regarded as a central component of diabetes education and transition planning (Polfuss et al., 2015; Xie et al., 2020). Enhancing self-efficacy, along with recognizing and supporting the evolving roles of parents, adolescents, and health care providers throughout the transition process, is critical for successful outcomes (Polfuss et al., 2015). Our findings emphasize that fostering self-efficacy—particularly through engagement in household chores—can equip youth with chronic conditions with the confidence and skills needed for a successful transition to adult health care (Albalawi, 2016; Varty et al., 2022). Moreover, self-efficacy is associated with a stronger reliance on health care providers as trusted sources of health information. Johnson et al. (2015) found that youth who identified health care providers as their primary source for health education demonstrated higher self-efficacy and greater transition readiness. These findings underscore the importance of integrating self-efficacy–building strategies into both clinical care and family environments to support youth in developing greater independence in managing their health. The assignment of household chores can serve as a practical and effective tool to achieve this goal.
It is important to note that while self-efficacy positively mediates the relationship between chores participation and transition readiness, it may have a complex relationship with specific aspects of health care responsibility. In some studies, higher self-efficacy has been associated with lower adolescent health care responsibility, possibly due to increased confidence leading to less perceived need for active engagement in health care tasks (Varty et al., 2022), suggesting that the impact of other factors would be critical to explore.
Limitations
Several limitations should be considered when interpreting the results of this study. Participants were recruited from a single clinic at one hospital, which increases the risk of a demographically homogeneous sample. A gender imbalance was observed, with higher female patients and mothers’ participation. In addition, factors such as psychosocial functioning, mental health diagnoses (Alwadiy et al., 2021), and the presence of developmental disabilities or other chronic health conditions may influence transition readiness, self-efficacy, and engagement in household chores. We acknowledge that a limitation of our study is the absence of these additional measures, which could have provided a more comprehensive understanding of the factors shaping health care transition outcomes. The online recruitment method may have excluded individuals without reliable access to technology, potentially limiting the diversity of the sample. Reliance on self-reported measures introduces the possibility of reporting bias, which could skew study results. The low response rate presents another potential source of bias, affecting the generalizability of the findings. Significantly, the COVID-19 pandemic posed major challenges to our enrollment efforts. It caused substantial interference with data collection and likely impacted participants’ interest and enthusiasm for completing a research study. The pandemic’s widespread effects on all major life areas may have influenced individuals’ willingness and ability to engage in the study, further complicating the interpretation of our results. Replication of this study with a more rigorous design, addressing the limitations, would yield more robust results with improved external validity.
Conclusion
The findings of this study highlight the potential benefits of chores participation in fostering self-efficacy beliefs and transition readiness skills. Engaging in household tasks can positively influence self-efficacy beliefs, boosting confidence in one’s abilities to manage their health. Moreover, the diverse skill set developed through chore participation may contribute to a smoother transition from pediatric to adult health care providers. This research provides valuable insights for both families and health care professionals seeking to support youth in coping more effectively with diabetes and feel better prepared for health care transition. By recognizing the importance of developmentally appropriate chores and related responsibilities, parents and caregivers can create opportunities for young individuals to build independence, self-reliance and self-efficacy. Health care providers can use this information to guide families in incorporating meaningful tasks into their daily routines, potentially improving long-term health outcomes and overall well-being for youths with diabetes. Enhancement of diabetes management self-efficacy can start early and could involve targeted interventions incorporating chores engagement. Ultimately, this approach may lead to more confident, capable young adults who are better equipped to navigate the challenges of managing their chronic illness.
Footnotes
Data Availability Statement
The data sets used during the current study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by UNC Department of Health Sciences Trust Funds.
Ethical Approval and Informed Consent Statements
This study was approved by the University of North Carolina at Chapel Hill Research Ethics Committee (approval no. 448535). All participants provided written consent to partake in the study.