
Abstract
Occupational performance challenges are common among breast cancer survivors (BCS). In a recent randomized controlled trial (RCT), our rehabilitation intervention catalyzed significantly greater improvements in occupational performance compared to an education-based control condition. To describe BCS’ activity priorities and examine what short-term goal characteristics (i.e., focus) and outcomes (i.e., attainment, satisfaction) predicted long-term occupational performance improvement. Post hoc analysis of intervention session data from an RCT. Content analysis was used to summarize participants’ short-term and long-term goals. Linear regressions were conducted to examine associations between weekly goal characteristics and outcomes and occupational performance improvement. Among 138 BCS, 119 (86.2%) set long-term goals focused on exercise. Self-reported satisfaction with weekly goal outcomes was the strongest predictor of occupational performance improvement (ηp2 = 0.14–0.17, p < .001). Satisfaction with short-term goal outcomes, regardless of goal focus or attainment, predicts long-term occupational performance improvement in the year following breast cancer treatment.
Plain Language Summary
Women often have difficulty performing valued activities after treatment for breast cancer. These challenges can persist and are associated with higher levels of depression and lower quality of life. To support women to engage in valued activities in the year following treatment for breast cancer, we developed and tested a telephone-based occupational therapy coaching intervention. The intervention helps women identify activities they want to improve engagement in and set weekly goals for these activities. In a recent study, women who received the intervention reported greater improvement in performance and satisfaction with valued activities compared with women who only received education. We analyzed data from our study’s intervention sessions to better understand what types of activities women prioritized and to examine what short-term (i.e., weekly) goal characteristics (i.e., focus) and outcomes (i.e., attainment, satisfaction) may have predicted longer-term improvements in activity engagement. We found that exercise was the most common activity that women wanted to improve engagement in. How satisfied a woman felt with the outcomes of her weekly goals was the strongest predictor of long-term improvement in activity engagement, regardless of whether the weekly goals were met or if the focus of those weekly goals was related to the woman’s long-term goals. Our results illustrate how an intervention that shifts the power of decision-making, goal setting, and evaluation to the patient while providing support from a trained clinician, can support women to improve activity engagement after treatment for breast cancer.
Introduction
Occupational performance—engagement in and satisfaction with valued activities that reflect life roles (American Occupational Therapy Association, 2020; World Federation of Occupational Therapy, 2022)—contributes to an individual’s sense of purpose and quality of life (L’Hotta et al., 2022; Pergolotti et al., 2015). Due to the physical, cognitive, and psychological effects of a cancer diagnosis and treatment (Sperlich et al., 2024), nearly one-third of cancer survivors experience limitations in occupational performance (Ness et al., 2006). There is no compelling evidence to suggest these limitations resolve naturally over time. In fact, among breast cancer survivors (BCS), limitations in recreational activities, sexual activities, work, and daily activities can persist for several years beyond treatment (Fan et al., 2023; Jones et al., 2016; Loubani et al., 2022; Yang et al., 2015) and have been associated with higher levels of depression (Huang et al., 2019) and lower quality of life (Hwang et al., 2015). Furthermore, reduced role quality of life, which encompasses an individual’s satisfaction with their specific life roles, is associated with shorter overall survival among BCS (Suzuki et al., 2024).
One approach to address challenges in occupational performance among BCS and other populations is to use a person-driven intervention, leveraging behavioral strategies to support individuals’ engagement in personally selected activities (Hegel et al., 2011; Kang et al., 2022; Lyons et al., 2015, 2019; Warner et al., 2015). In this type of approach, the clinician provides structure and support, but the intervention is guided by a person’s individual needs and priorities (Cameron et al., 2018). A person-driven approach encourages active engagement of the individual in the goal setting process which helps to promote more personally meaningful goals, increased goal ownership, and improved motivation (Kang et al., 2022; Turner-Stokes et al., 2015).
While supporting clients to identify and achieve goals can improve occupational performance, the clinician’s role in a person-driven intervention is often ambiguous as it is unclear how much and what type of support should be offered in the goal setting process. For example, though clients are often encouraged to set “SMART” (i.e., specific, measurable, achievable, realistic, and timebound) goals (Bowman et al., 2015), other factors, including goal type (e.g., performance vs. mastery), focus, and level of challenge, may influence a person’s performance and experience (Bailey, 2019; Swann et al., 2023). Short-term goal attainment may also be critical for clinicians to support and facilitate (Lang et al., 2022; Neuner et al., 2013; Preede et al., 2021). However, the extent to which such short-term goal characteristics and outcomes influence long-term occupational performance, and therefore how much direction or decision-making clinicians should offer, is unclear.
To gain insight into how short-term goal characteristics and outcomes influence long-term occupational performance in a person-driven intervention among BCS, we conducted a post hoc analysis of a recent randomized controlled trial (RCT; NCT03915548). Our telephone-based, coaching intervention, herein referred to as Behavioral Activation/Problem-solving (BA/PS), uses two empirically supported treatments (Behavioral Activation, Cuijpers et al., 2007a, and Problem-solving Treatment, Cuijpers et al., 2007b) and augments them with rehabilitation principles of activity adaptation and environmental modification (Hegel et al., 2011; Lyons et al., 2015). BA/PS clinicians provide structure and education and support the goal-setting process, but participants self-identify long-term priorities and choose what activities they want to focus on each week. In the RCT, compared with an attention control condition (cancer survivorship education), both groups made clinically meaningful and statistically significant improvements in quality of life and social participation; however, BA/PS catalyzed significantly greater improvements in performance and satisfaction with self-selected activities (Lyons et al., 2024) as measured by the Canadian Occupational Performance Measure (COPM; Law et al., 2014).
While the BA/PS intervention appears to promote occupational performance among BCS, what remains unclear is what short-term goal characteristics (i.e., focus) and outcomes (i.e., attainment, satisfaction) predicted long-term improvements in occupational performance in our RCT. Therefore, our post hoc analysis was guided by the following research questions:
While the first question was descriptive (i.e., no hypothesis), we hypothesized that a higher correlation of weekly and long-term goal focus would predict greater long-term improvements (RQ2), and that higher short-term goal attainment and satisfaction would predict greater long-term improvements (RQ3). Insight into BCS’ activity priorities in the year following treatment will allow us to refine the intervention to be more tailored (e.g., educational materials, provider discipline). Identification of factors that predict occupational performance improvement will enhance clinicians’ ability to deliver the intervention (e.g., type and extent of support) to foster occupational performance after treatment for breast cancer.
Method
Study Design and Enrollment Procedures
This is a post hoc analysis of session data collected from a single-blind multi-site RCT comparing the BA/PS intervention against a dose-matched education-based, attention control condition (Stevens et al., 2020). Institutional review board approval was obtained from the investigators’ institutions (Dartmouth College, Dartmouth-Hitchcock Health, University of Alabama at Birmingham, and Mass General Brigham).
Women aged ≥ 18 years, diagnosed with stage I to III breast cancer without recurrence, who reported reduced participation (i.e., scored ≥10 on the Work and Social Adjustment Scale; Mundt et al., 2002) within 1 year of completing locoregional treatment and/or chemotherapy with curative intent were eligible to participate. Exclusion criteria included being non-English speaking, having non-correctable hearing loss, having moderate-to-severe cognitive impairment (i.e., scored <3 on a 6-item cognitive screener; Callahan et al., 2002), and having a documented or self-reported history of severe mental illness, current major depressive disorder, suicidal ideation, or substance use. All participants provided written consent prior to study enrollment.
Participants were recruited between August 2019 and April 2022 from the cancer centers at Dartmouth College and University of Alabama at Birmingham, as well as via Facebook advertisements. Processes of randomization and blinding are detailed elsewhere (Stevens et al., 2020), as is the Consort flow diagram (Lyons et al., 2024). Ultimately, 303 women were enrolled, and of those, 284 completed baseline assessments and were randomized with 144 participants to the BA/PS intervention. The intervention and control conditions were both delivered via telephone by a team of occupational therapist coaches over nine sessions (six weekly then three monthly). This analysis focuses only on participants randomized to the BA/PS intervention as the control condition did not explicitly engage participants in goal setting.
Individualized Outcome (COPM): Occupational Performance (Sessions 1 and 9)
In the first BA/PS session, the coach administered the COPM to elicit participants’ occupational performance priorities and self-perceived current performance status (Law et al., 2014). The COPM is an individualized outcome measure, allowing participants to specify activities they want to increase or modify to foster recovery. Participants rated up to five self-selected activities using Likert-type scales (ranging from 1 to 10) on three distinct but related characteristics: importance, performance, and satisfaction. In the final BA/PS session (Session 9; approximately 20 weeks after baseline), participants re-rated their previously identified self-selected activities using the same three characteristics. These data were recorded on paper forms and then were entered into a secure electronic database. For this analysis, we used a residualized change approach for occupational performance, operationally defined here as COPM performance and satisfaction post-scores controlling for their respective pre-scores (Harrell, 2024).
BA/PS Intervention: Weekly Activity Goals, Attainment, and Satisfaction (Sessions 2–8)
The BA/PS intervention is detailed elsewhere (Stevens et al., 2020). Briefly, in each BA/PS session, the coach followed an eight-step process to guide the participant to use a goal setting, problem-solving, and action planning worksheet to plan at least one and up to three self-selected activities to perform in the coming week. The coaches recorded details regarding the planned activities and goals and the action plan that was set.
At each follow-up BA/PS session, the coach asked about goal attainment, recording whether the participant had met, partially met, or not met their goal(s) in the prior week. Coaches also asked each participant to rate their satisfaction with the effort put into achieving their goal(s) and their satisfaction with the outcome of those efforts using a Likert-type scale of 0 to 10 with higher scores indicating greater satisfaction. These results were used to refine participants’ individual goal setting and action plans for the following week. Through this process, participants performed weekly activity experiments, i.e., set goals and executed action plans, reflected on their performance and barriers to progress, reevaluated priorities, and identified new goals.
Coaches maintained detailed paper notes of each BA/PS session and the above variables (activity focus, goal attainment, and satisfaction with effort and outcome) were subsequently entered into a secure electronic database.
Data Analysis
Development of a Coding Scheme
Participants’ occupational performance priorities (per COPM), weekly activities, and associated goals were recorded by the coaches using non-standardized free text. To systematically summarize these data into meaningful categories to answer RQ1 (i.e., What activities did participants focus on in short- and long-term goal setting?), we performed a content analysis. This approach uses a reproducible process to code the raw data, and then count the data attached to each code.
The intervention variables were extracted into a spreadsheet for the coding process. The first author (S.W.) reviewed these data and applied a coding scheme with operational definitions that was developed by the team in pilot studies of the intervention (Lyons et al., 2012), noting challenges in applying the pre-established codes, and developing additional codes and operational definitions to capture data that did not fit into the pre-established scheme. S.W., K.L., and a doctoral student (S.S.) met to discuss and further develop the coding scheme. To optimize reliability, S.W. and S.S. independently pilot tested the updated coding scheme on 10% of COPM-identified occupational performance priorities to assess inter-rater agreement. After pilot testing, the research team met to examine specific examples of difficult-to-categorize raw data, further refine the coding scheme, and achieve consensus on a final coding scheme with operational definitions (Table 1). S.W. and S.S. then coded the full dataset and met to review and resolve any discrepancies. We achieved 94% and 92% inter-rater agreement applying the final coding scheme to occupational performance priorities and weekly activity goals, respectively; 100% consensus was achieved through active dialogue.
Coding Scheme and Operational Definitions.
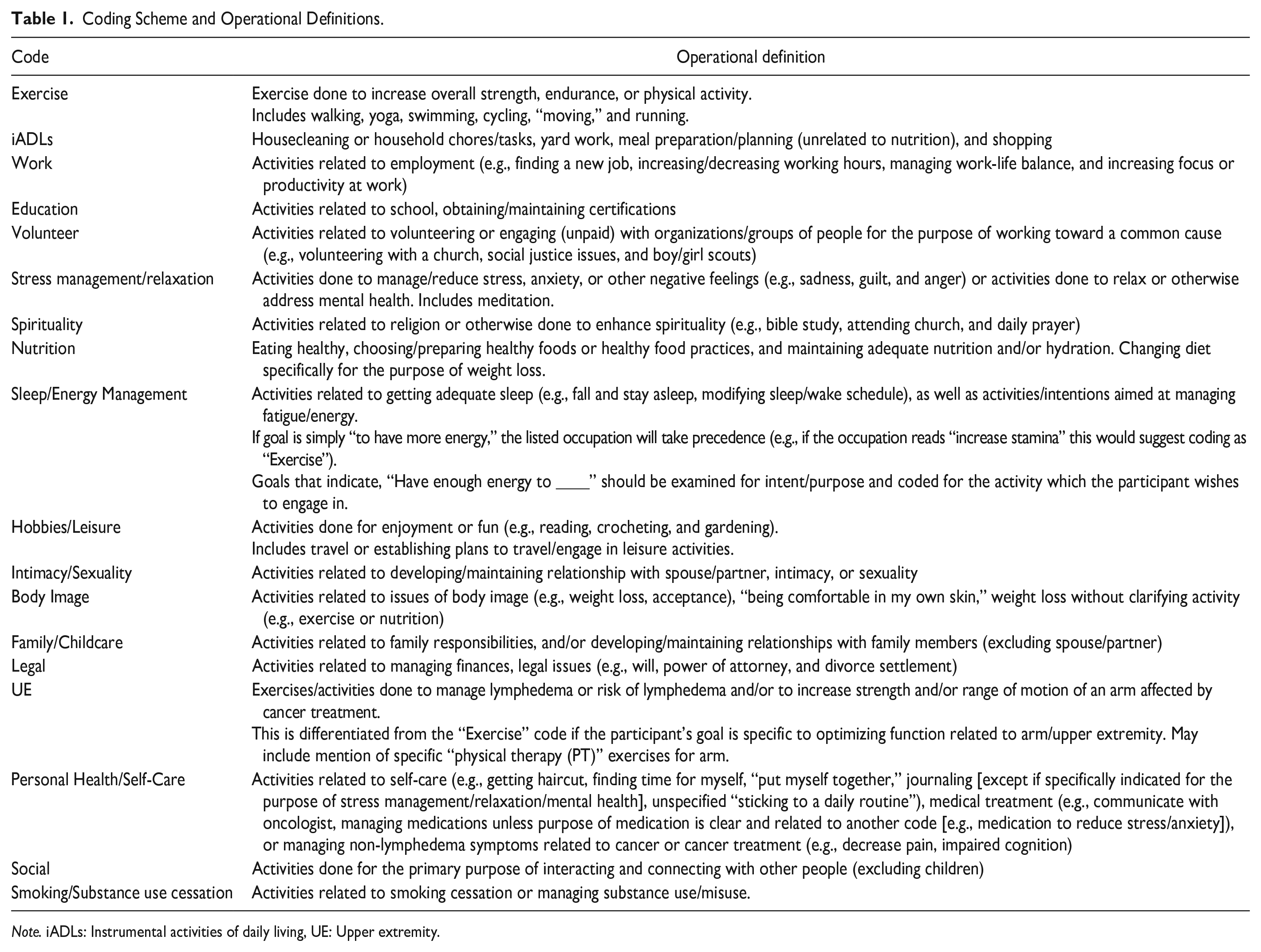
Note. iADLs: Instrumental activities of daily living, UE: Upper extremity.
Descriptive Summary
We used descriptive statistics to quantify coach-documented intervention variables at the level of the session (i.e., session length) and the participant. Participant-level variables included the number of intervention sessions per participant, the number of occupational performance priorities elicited in Session 1, the number of weekly goals set, the proportion of weekly goals that were met, partially met, or not met, and the average level of weekly satisfaction with outcomes and effort related to weekly goals.
Content Analysis: Goal Focus
We summarized the foci of participants’ occupational performance priorities and weekly goals by calculating the frequencies of applied activity codes. We did this first at the level of the participant by calculating the proportion of participants whose data included the code, and then at the level of the priorities/goals by calculating the proportion of total priorities/weekly goals per code. We went a step further to identify the number of unique weekly goals per participant by examining the frequency of identical activity codes within a participant’s intervention period (e.g., if a participant set three goals focused on exercise, this was considered one unique goal relating to exercise).
To inform RQ2 (i.e., Did the association of short-term (i.e., weekly) goal focus and long-term goal focus predict greater improvements in occupational performance?), we compared the activity codes applied to participants’ occupational performance priorities and weekly activity goals. We calculated the proportion of each participant’s priorities that were addressed by weekly goals (i.e., had the same focus) and vice versa. For example, if a participant’s occupational performance priority was coded “Exercise” and one weekly goal was also coded “Exercise,” the occupational performance priority was considered addressed, and this weekly goal was considered directly related to the occupational performance priority. Conversely, if a person’s priority was coded “Work,” and the weekly goals were coded “Nutrition,” “Spirituality,” and “Leisure,” the priority was not considered addressed, and the weekly goals were not considered directly related to the occupational performance priority.
Association Between Occupational Performance Improvement, Goal Focus, and Short-Term Goal Outcomes
To answer RQ2, we conducted two separate linear regression analyses, first with improvement in COPM performance as the dependent variable, and then with improvement in COPM satisfaction as the dependent variable. Predictors of interest in both regressions were: percentage of occupational performance priorities addressed by weekly goals, percentage of total weekly goals related to occupational performance priorities, and percentage of unique weekly goals related to occupational performance priorities.
To answer RQ3 (i.e., Did short-term goal attainment and satisfaction predict greater improvements in occupational performance?), we similarly conducted two separate linear regression analyses with improvement in COPM performance and satisfaction as dependent variables. Predictors of interest in both regressions were: percentage of goals met or partially met, satisfaction with weekly outcomes, and satisfaction with weekly effort.
For all regressions, analyses consisted of (a) multicollinearity assessment with estimation of variance inflation factors (VIFs) and exclusion of redundant predictors, if any, (b) initial unadjusted regression fitting for post-score (as outcome) with pre-score and predictors of interest as explanatory variables, and (c) final regression fitting adjusted for potential confounders, conceptualized as possible influencing factors on both explanatory variables and outcomes. These included education, employment, sociodemographic index score, time since primary cancer treatment (< or >6 months), scores for coping planning subscale, and goal adjustment disengagement and reengagement scales.
Given the effective sample size of N ~120, models were fitted to maintain a limit on the ratio of regression coefficients to a sample of ~1:10 (Harrell, 2012). The percentage of variance explained (R-squared and adjusted R-squared; small ~ .02, medium ~ .13, large ~ .23) and ηp2 (small ~ .01, medium ~ .06, and large ~ .14) were used as measures of effect size for models and individual predictors, respectively, with Cohen’s guidelines (Cohen, 2013) for interpretation of their magnitudes. Adjusted R-squared, F-tests, and Akaike information criterion (AIC) values were used to determine whether the inclusion of the set of adjusting covariates improved the explanatory ability of the regression models beyond that of the unadjusted models.
A traditional statistical significance level of .05 was held. Analyses were conducted in SPSS v29 and R v4.2.3 software packages.
Results
Participants and BA/PS Sessions
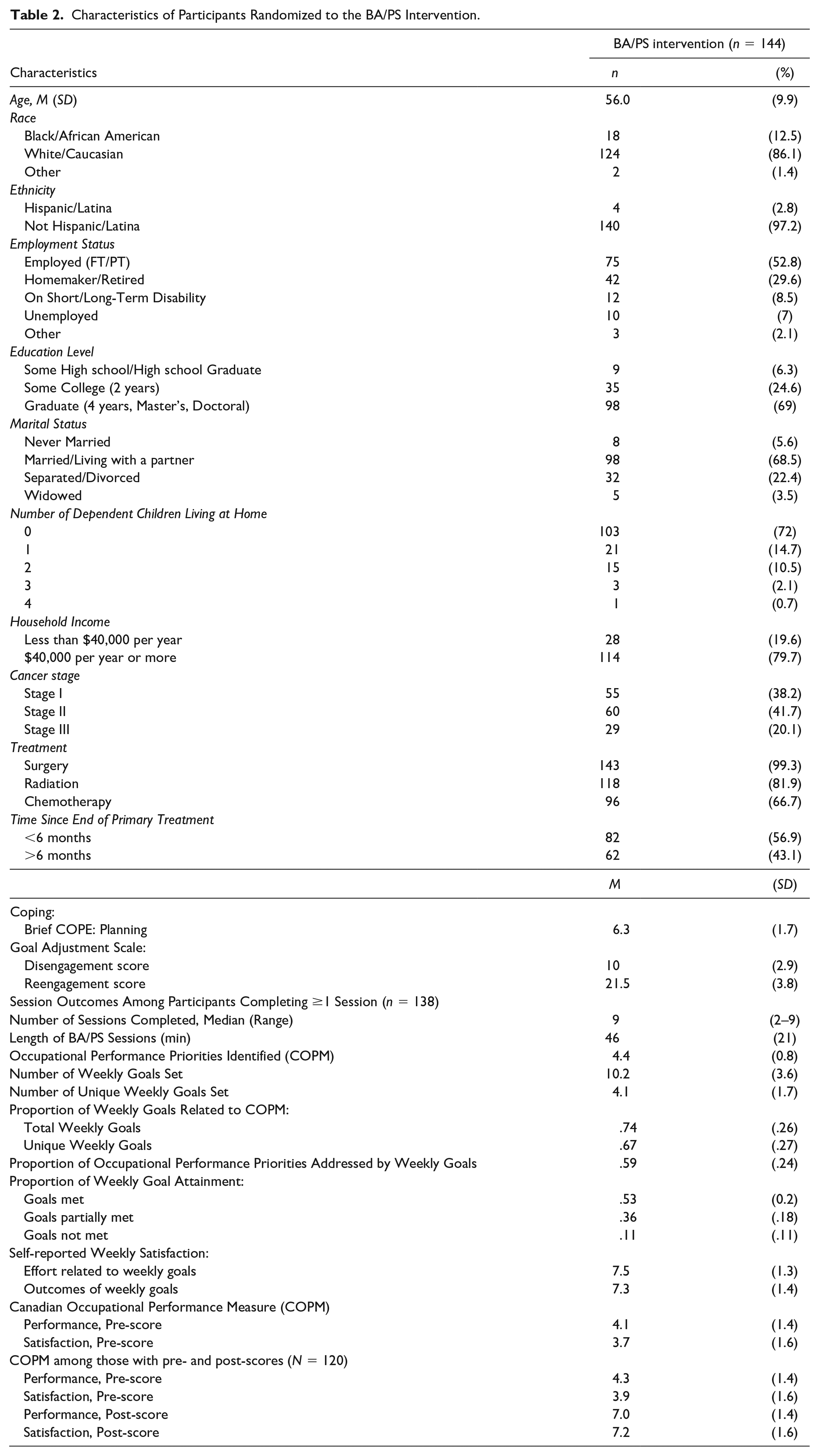
Of the 144 participants randomized to the BA/PS condition, 138 (96%) completed at least the first intervention session (median = nine sessions, range = 2–9) and provided responses to the COPM and thus were included in descriptive/content analyses. Table 2 presents the characteristics of the 144 participants randomized to the BA/PS condition and session outcomes for the 138 participants completing at least one session. In total, 120 (87%) of the 138 participants completed all nine intervention sessions and thus had pre- and post-COPM scores and were included in the regression analyses. Sessions lasted an average of 46 (21) min.
Characteristics of Participants Randomized to the BA/PS Intervention.
Focus of Occupational Performance Priorities Identified via COPM (n = 138)
In total, the 138 participants identified 613 occupational performance priorities (average 4.4 [0.8] per participant). Exercise, nutrition, and instrumental activities of daily living (iADLs) were the most prevalent foci, with 119 (86.2%), 71 (51.4%), and 60 (43.5%) participants identifying priorities in these categories, respectively (Table 3).
Content Analysis Results of COPM-Identified Occupational Performance Priorities and Weekly Activity Goals.
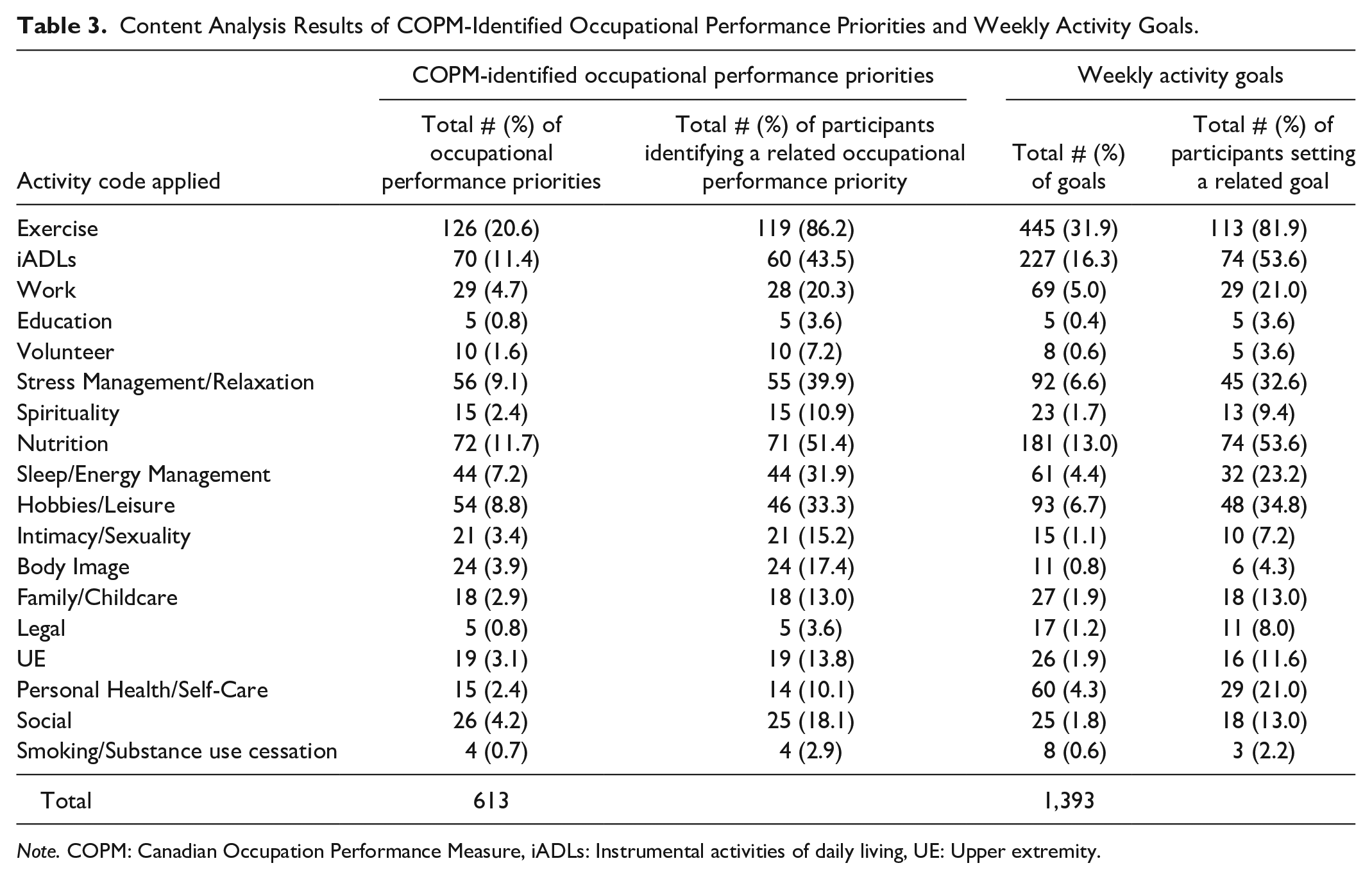
Note. COPM: Canadian Occupation Performance Measure, iADLs: Instrumental activities of daily living, UE: Upper extremity.
Focus of Weekly Activity Goals (n = 138)
In total, the 138 participants set 1,393 weekly activity goals over the course of the intervention (average 10.2 [3.6] goals per participant). Of these, 315 goals were unique (an average of 4.1 [1.7] unique goals per participant). Exercise, iADLs, and nutrition were the most prevalent weekly goal foci with 113 (81.9%) participants setting a weekly goal related to exercise and 74 (53.6%) participants setting goals related to iADLs or nutrition (Table 3).
On average, participants met 53% (SD 20%), partially met 36% (SD 18%), and did not meet 11% (SD 11%) of their weekly goals. Regarding satisfaction with weekly outcomes and effort toward their goals, participants averaged 7.3 (1.4) and 7.5 (1.3), respectively.
Association of Short-Term and Long-Term Goal Focus (n = 138)
A median of 60% (0%–100%) of participants’ occupational performance priorities were addressed by weekly goals within the same activity category. A median of 83% (0%–100%) of participants’ total weekly goals and 66% (0%–100%) of unique weekly goals were directly related to their occupational performance priorities.
Did the Association of Short-Term Goal Focus and Long-Term Goal Focus Predict Greater Improvements in Occupational Performance? (n =120)
The percentage of total and unique session goals related to COPM-identified occupational performance priorities were highly collinear (VIFs > 5.8). Thus, we omitted the percentage of total session goals in favor of unique goals as we felt that unique goals captured a participant’s goal focus while reducing redundancy. Unadjusted and adjusted regression models for COPM performance and satisfaction scores are shown in Table 4. For both outcomes, in both unadjusted and adjusted models, the strongest predictors of COPM performance and satisfaction post-scores were their respective pre-scores, with medium-to-large effects (ηp2 ranging from 0.09–0.14). The data did not indicate effects of relevant magnitude in explaining the outcomes by the percentage of occupational performance priorities addressed by weekly goals or the percentage of unique session goals related to occupational performance priorities (all ηp2 < 0.02). The inclusion of covariates did not provide additional significant explanatory ability to the models, resulting in F(10,106) = 1.33, p = .222 for COPM performance; and F(10,106) = 1.88, p = .055 for COPM satisfaction.
Unadjusted and Adjusted Models for COPM Performance and Satisfaction Scores With Percentage of COPM-Identified Occupational Performance Priorities Addressed by Weekly Goals and Percentage of Unique Weekly Goals Related to COPM-Identified Occupational Performance Priorities as Predictors of Interest.
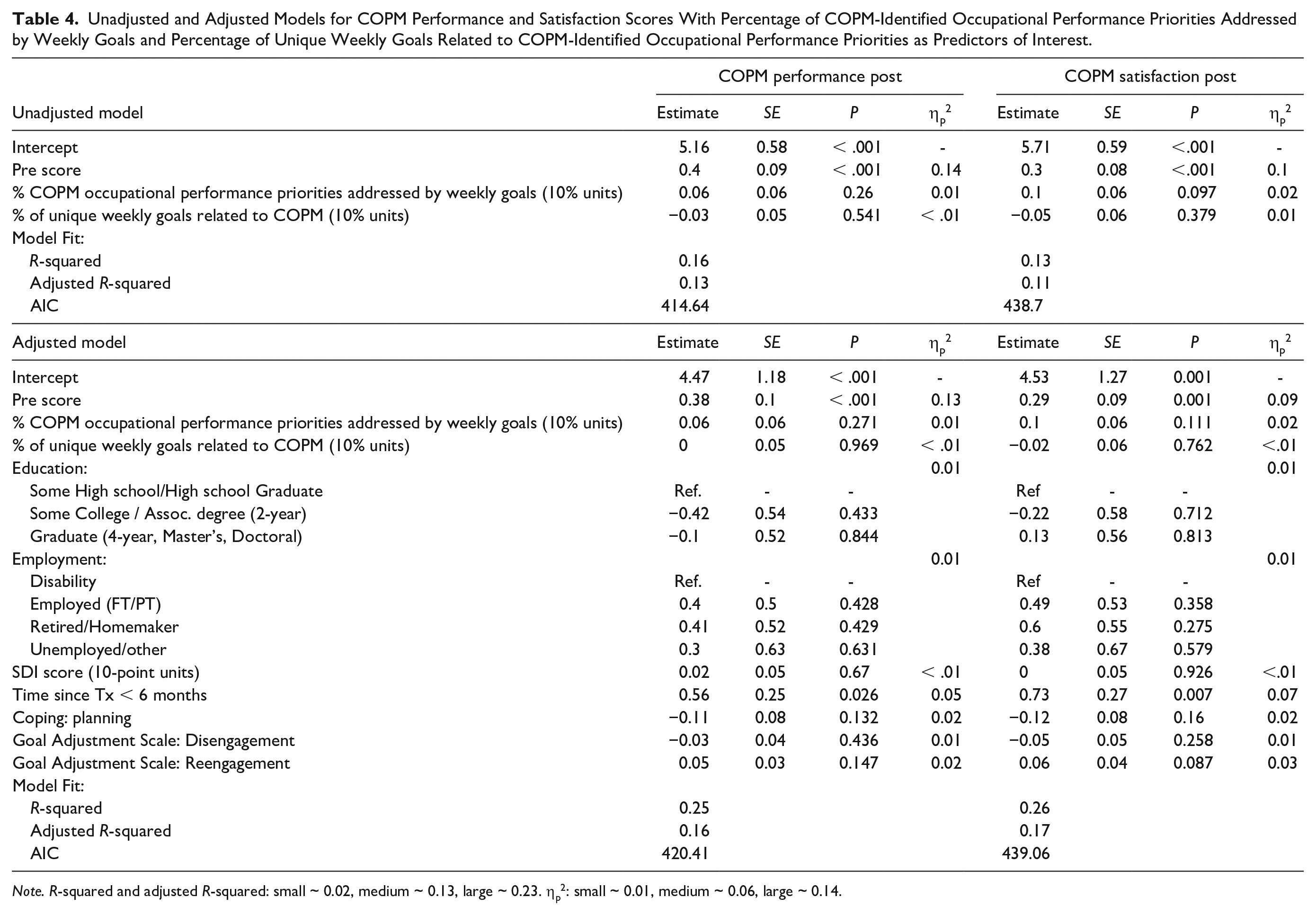
Note. R-squared and adjusted R-squared: small ~ 0.02, medium ~ 0.13, large ~ 0.23. ηp2: small ~ 0.01, medium ~ 0.06, large ~ 0.14.
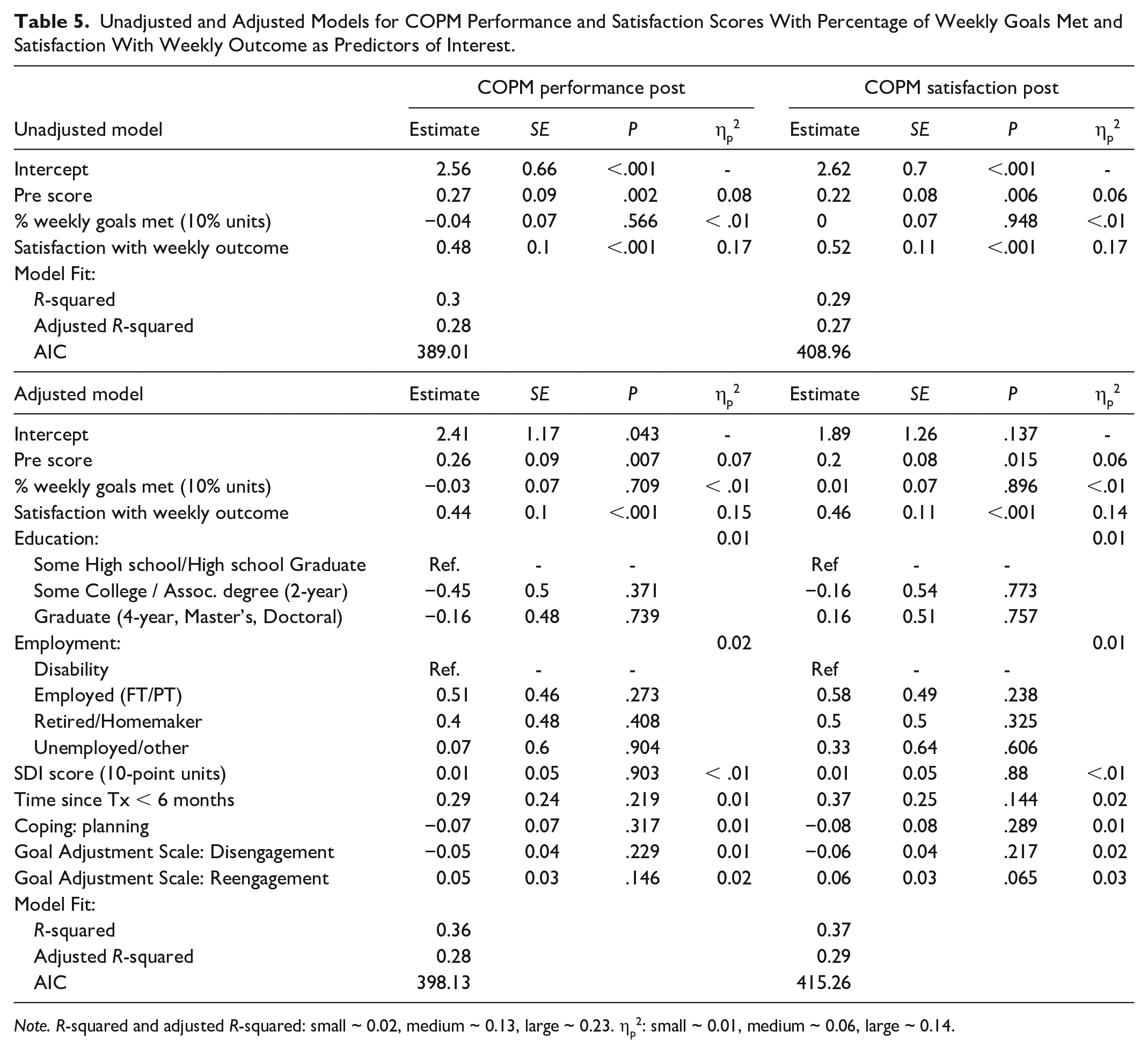
Did Short-Term Goal Attainment and Satisfaction Predict Greater Improvements in Occupational Performance? (n = 120)
The percentage of weekly goals met and partially met were collinear (VIFs > 4.2) and satisfaction with weekly outcomes and weekly effort were also collinear (VIFs > 3.7). Therefore, we omitted the percentage of goals partially met and satisfaction with weekly effort in favor of the retained variables which we felt were more reflective of short-term goal attainment and impact of the intervention. Unadjusted and adjusted regression models for COPM performance and satisfaction scores are shown in Table 5. For both outcomes, in both unadjusted and adjusted models, the strongest predictor of COPM performance and satisfaction post-scores was satisfaction with weekly outcome, with effects of large magnitude (ηp2 ranging from 0.14–0.17). Pre-scores were also relevant predictors with effects of medium size (ηp2 ranging from 0.06–0.08). The data did not indicate effects of relevant magnitude in explaining the outcomes by the percentage of goals met (all ηp2 < 0.01). The inclusion of covariates did not provide additional significant explanatory ability to the models, resulting in F(10,105) = 1.01, p = .444 for COPM performance; and F(10,105) = 1.28, p = .251 for COPM satisfaction.
Unadjusted and Adjusted Models for COPM Performance and Satisfaction Scores With Percentage of Weekly Goals Met and Satisfaction With Weekly Outcome as Predictors of Interest.
Note. R-squared and adjusted R-squared: small ~ 0.02, medium ~ 0.13, large ~ 0.23. ηp2: small ~ 0.01, medium ~ 0.06, large ~ 0.14.
Discussion
Results of our RCT showed that our BA/PS intervention produced greater improvements in occupational performance and satisfaction among BCS compared with an education-based attention control condition (Lyons et al., 2024). The present analysis aimed to identify what activities participants prioritized and what short-term goal characteristics (i.e., focus) and outcomes (i.e., attainment, satisfaction) predicted these improvements among intervention participants. This study adds to the literature supporting patient-centered interventions in oncology rehabilitation (Pel et al., 2022) by deepening our understanding of what activities BCS may prioritize post-treatment and how short-term satisfaction with progress may be critical to long-term success performing self-selected activities. By identifying predictors of occupational performance improvement after breast cancer treatment, this analysis provides insight for researchers and clinicians to design and deliver person-driven behavioral interventions to improve occupational performance among BCS.
Results of our content analysis (RQ1) revealed that most participants’ short- and long-term goals focused on exercise, nutrition, and iADLs. These results are aligned with other research (Elshahat et al., 2021; Fitch et al., 2020) and this team’s prior work elucidating common goals among cancer survivors (Lyons et al., 2012, 2018). BA/PS coaches—licensed occupational therapists in our RCT—are trained to accommodate a wide variety of activity priorities through individualized support, encouragement, and education. While other disciplines (e.g., physical therapy, nutrition and dietetics) may be more apt to provide specific activity prescriptions, the intent of BA/PS is not to be prescriptive. Rather, BA/PS coaches support participants to develop and execute action plans in the context of their lives. A process evaluation of our RCT revealed that, compared with the control condition, BA/PS participants reported significantly more benefit in terms of setting goals, adjusting habits and routines, and increasing exercise (Stevens et al., 2023). This suggests that occupational therapists were effective in delivering this tailored intervention to enhance engagement across goal areas. Still, our results support prior evidence and should enable researchers and clinicians from various disciplines to better anticipate BCS’ priorities and to provide tailored education on these topics.
BA/PS coaches elicited participants’ priorities but did not tell participants what activities they should focus on. This helps explain why only 60% of participants’ occupational performance priorities were addressed by weekly goals within the same category. Contrary to our RQ2 hypothesis, our analysis revealed that the relation between weekly and long-term goal focus did not influence long-term COPM score improvement. This was unexpected given the historical perspective that self-regulatory behavior (i.e., managing thoughts and actions to achieve goals) is most effective when short-term goals are related to personally meaningful overarching goals (Emmons & Kaiser, 1996). More recent research has explored the hierarchy of goals in rehabilitation and the importance of setting specific goals that serve to achieve meaningful long-term goals (Dekker et al., 2019). It is possible, given the perceived benefits reported by BA/PS participants (e.g., setting goals, adjusting habits and routines; Stevens et al., 2023), that the intervention facilitated generalizable knowledge and skills in the short term (regardless of goal focus) that could be applied toward long-term goals. Nevertheless, our results suggest that deferral to patient priorities when setting short-term goals may not limit long-term occupational performance improvement. Providing patients more autonomy may be critical, especially considering evidence that, even in a patient-centered approach, goal setting can still be strongly influenced by clinicians’ views (Cameron et al., 2018; Parsons et al., 2018) which can lead to suboptimal outcomes and lower perceived quality of care (Arnetz et al., 2004). Additional research, possibly using automated prompts, daily goal diaries, or app-based interventions, is warranted to explore patients’ autonomous goal setting and the impact on long-term goal attainment.
Finally, in partial contrast to our RQ3 hypothesis, weekly goal attainment did not appear to influence long-term improvement. In other words, a participant’s occupational performance improvement was not dependent on whether they met their short-term goals. This was surprising, considering that in most rehabilitation models, short-term goal attainment is seen as an important predictor of long-term outcomes (Lang et al., 2022; Neuner et al., 2013; Preede et al., 2021). In our study, however, the strongest predictor of long-term occupational performance and satisfaction improvement was the participant’s self-reported satisfaction regarding weekly goal outcomes.
While satisfaction with a goal’s outcome may correlate with goal attainment, other aspects of a person’s experience may contribute to their satisfaction. For example, an individual may partially meet their goal, but in doing so, they might realize that partially meeting their goal met their needs in the context of their daily life. Conversely, a patient may disengage from a goal, realizing it was unattainable or unnecessary, and this can also lead to satisfaction. In fact, in our RCT, post-intervention goal disengagement scores were significantly higher among the BA/PS group compared with the control group (Lyons et al., 2024). The intervention’s weekly process of activity experiments may support healthy goal disengagement while also supporting goal reengagement. Such goal adjustment can result in increased well-being and quality of life (Barlow et al., 2020; Castonguay et al., 2014; von Blanckenburg et al., 2014), and may help explain why satisfaction with weekly outcomes was a stronger predictor of occupational performance improvement than the weekly goal focus or attainment. Engaging in activity experiments is well-aligned with therapeutic approaches to enhance self-efficacy (Picha & Mills, 2023), an important construct in survivors’ ability to self-manage health throughout cancer survivorship (Leach et al., 2022), suggesting this intervention component may be particularly effective to improve occupational performance.
Limitations
We conducted this post hoc analysis to explore questions that arose during supervision of the BA/PS interventionists in the RCT. Interpretation of our results is limited by a lack of established minimal detectable change (MDC) or minimal clinically important difference (MCID) of the COPM (McColl et al., 2023), our main outcome in these analyses. Furthermore, the interrelated nature of weekly satisfaction and long-term COPM satisfaction must be acknowledged, though the significant association of weekly satisfaction and long-term COPM performance should strengthen confidence in our findings. Finally, while we used all available information to determine whether participants’ short-term goals were in service of their long-term goals, the results of RQ2 should be interpreted with caution as it is possible that our analysis did not account for all underlying relations.
Conclusion
This analysis provides insight into how a clinician-supported, person-driven, rehabilitation intervention can support BCS to improve occupational performance in the year following treatment. Our results suggest that clinicians can guide progress toward long-term improvements in occupational performance by eliciting and monitoring satisfaction with short-term goal outcomes, regardless of goal focus or attainment. Future research is needed to further explore and identify ways to maximize the potency of patient-driven models of rehabilitation for cancer survivors.
Footnotes
Ethical Approval and Informed Consent Statements
Institutional review board approval was obtained from the investigators’ institutions (Dartmouth College, Dartmouth-Hitchcock Health, University of Alabama at Birmingham, and Mass General Brigham [2021P002871]). ClinicalTrials.gov Identifier: NCT03915548. All participants provided written consent prior to study enrollment.
Data Availability Statement
Data is available upon request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant R01CA225792 (Dr. Lyons) and by career development award K08CA259632 (Dr. Stevens) from the NCI.