
Abstract
Fatigue is common, but under-recognized in Parkinson’s disease (PD), with limited treatment options. The aim of this study is to explore the experience of people with PD (PwPD) regarding content and delivery of the individual Packer Managing Fatigue program. This mixed-method study (n = 12) was conducted concurrently with a pilot randomized controlled trial. Data were collected using questionnaires, interviews, and focus groups. Five themes emerged: the program is helpful; the program has strengths; areas for improvement; individual online delivery is feasible; and more support from occupational therapist would be helpful. Quantitative findings confirmed feasibility with high ratings on questionnaires and confidence to use learned strategies. The findings inform future implementation of the Packer Managing Fatigue program and contribute to understanding the needs of PwPD. Future studies might explore program’s effectiveness as stand-alone treatment or in combination with other approaches. Tailoring fatigue programs to PwPD’s unique needs and characteristics of PD fatigue is suggested.
Plain Language Summary
People with Parkinson’s disease list fatigue as one of their three most disabling symptoms. They describe fatigue as a feeling of extreme tiredness that can make it difficult to perform everyday activities. We explored the perspective of people with Parkinson’s disease regarding the individual version of the Packer Managing Fatigue program. The study used video calls and included 12 people with Parkinson’s disease. The program proved helpful and feasible for participants. They learned skills to manage their fatigue, such as prioritizing tasks and balancing rest and activity, and were confident in using them. These findings provide preliminary evidence that could be used by occupational therapists to help people with Parkinson’s disease manage the negative impact of fatigue on their lives. However, reseaech studies, with more people, are needed to be sure the program is effective.
Introduction
Fatigue affects 36% to 50% of people with Parkinson’s disease (PwPD) (Friedman et al., 2016; Zhou et al., 2023) Friedman et al., 2016; Zhou et al., 2023) and significantly affects their occupational performance and quality of life (Herlofson & Kluger, 2017; Mantri et al., 2022). Reduced participation increases the risk of social isolation and psychological distress for PwPD (Herlofson & Kluger, 2017).
The high prevalence and significant impact of fatigue are driving development and evaluation of fatigue interventions for PwPD (Deane et al., 2014). Limited pharmacological success further prompts development of non-pharmacological interventions such as cognitive-behavioral therapy, exercise, and energy-conservation interventions (Nassif & Pereira, 2018). Among these, the Managing Fatigue: A Six-Week Course for Energy Conservation was one of the pioneering programs developed specifically to address fatigue secondary to neurological conditions (Packer et al., 1995) and remains one of the most evaluated programs (Alizadeh et al., 2023; Hersche et al., 2022).
The Managing Fatigue program was developed based on occupational therapy (OT) principles and initially delivered as a 6-week, group-based intervention (Packer et al., 1995). While little is known about its feasibility and effectiveness for PwPD (Hersche et al., 2022), its effectiveness has primarily been demonstrated in multiple sclerosis (MS; Finlayson et al., 2011; Plow et al., 2019), and there is evidence for other conditions such as neuromuscular diseases (Veenhuizen et al., 2019), traumatic brain injury (Raina et al., 2016), and chronic conditions (Van Heest, 2017). Only one study included PwPD in a mixed sample of adults with MS and post-polio syndrome. Although the study found a significant effect on participation and quality of life, it did not report diagnosis-specific results (Ghahari, 2010).
In addition, only a few studies have evaluated individual delivery of the program and all were adaptations of the original protocol (Alizadeh et al., 2023), yielding mixed results. One randomized controlled trial (RCT) evaluating a 12-session program found no significant difference in fatigue or participation between experimental and information-only control groups of people with MS (Blikman et al., 2017). In contrast, a study with five of six modules of the original group program, delivered in four to six individual sessions, found a significant improvement in fatigue impact and quality of life (Van Heest et al., 2017). To provide a standardized and consistent approach to one-on-one delivery and to reduce heterogeneity across studies, the original author developed a protocolized individual version of the program, named Packer Managing Fatigue: The Individual Self-Management Program (Packer et al., 2023).
In this study, a research version of this newly developed protocol was evaluated and delivered using synchronous videoconferencing due to the COVID-19 pandemic. This version embeds the opportunity to tailor content to each individual, while the videoconference format improves accessibility in remote areas. Since this was the first use of the new protocol and the first use exclusively with PwPD, our goal was to evaluate its feasibility prior to conducting a full-scale RCT. This study was part of a larger research project (Alizadeh et al., 2022) focused on clients’ perspective regarding perceived impact of the program on daily life activities, acceptability of delivery and content, and perceived confidence to use skills and strategies learned in the program.
Materials and Methods
Study Design
A concurrent mixed-methods approach (Creswell, 2015) evaluated experiences of PwPD participating in the Packer Managing Fatigue: The Individual Self-Management Program (Packer et al., 2023). This design allowed comprehensive data collection through focus groups, individual interviews, and feasibility questionnaires. Focus group/individual interviews provided insight into individuals’ perceptions, while data from the questionnaires added validity to these findings. Triangulation was carried out during the interpretation phase. The research protocol was approved by the Nova Scotia Health Research Ethics Board (ref: 1027048). The checklist for mixed-method research manuscript preparation and review proposed by Lee et al. (2022) guided reporting of the findings (Supplementary Table 1, Supplementary Figure 1).
Participants and Recruitment
This study was embedded in a pilot RCT [n = 25 PwPD; (Alizadeh et al., 2022)]. Participants in the pilot RCT independently contacted researchers by email in response to flyers. All provided informed, voluntary consent prior to group allocation. Participants in the intervention group composed the sample for this study. Data completed as part of the main study was complemented by individual/focus group interviews. Participants who agreed to follow-up contact at initial consent and who were allocated to the intervention group were recontacted for the interviews. Those who responded were contacted to provide additional consent and schedule an interview. Participants resided in provinces of Ontario or Nova Scotia, due to OT licensure regulations. All were adults with a self-reported diagnosis of PD who scored 4 or higher on the Fatigue Severity Scale (FSS; Krupp et al., 1989), could read and speak English, and had access to the internet, an electronic device, and a private place for videoconferences. Participants with scores of ≤13 on the Mini-Mental Status Examination (MMSE), indicating severe cognitive impairments, were excluded. Participants are required to take an active problem-solving role in the program and a secondary analysis by Finlayson, et al. (2007) demonstrated that cognitive ability has a differential influence on the outcomes of the program.
Study Intervention
The study program consists of six semi-structured individual sessions and is manualized for occupational therapists (OTs), with a dedicated participant manual, sent by mail. The content is consistent with the second edition of the original group program now named as Packer Managing Fatigue: A Six-Week Self-Management Group Program (Packer et al., 2022), which incorporated two additional topics, sleep hygiene and cognitive-fatigue management. Sleep hygiene content is integrated into the first session while cognitive-fatigue management strategies are incorporated throughout all sessions. Content in Sessions 1 to 5 focuses on: (a) the importance of rest and sleep; (b) communication and body mechanics; (c) tools, technology, and ergonomics; (d) priorities and standards; and (e) putting it all together. Session 6 includes a program review and discussion of future plans.
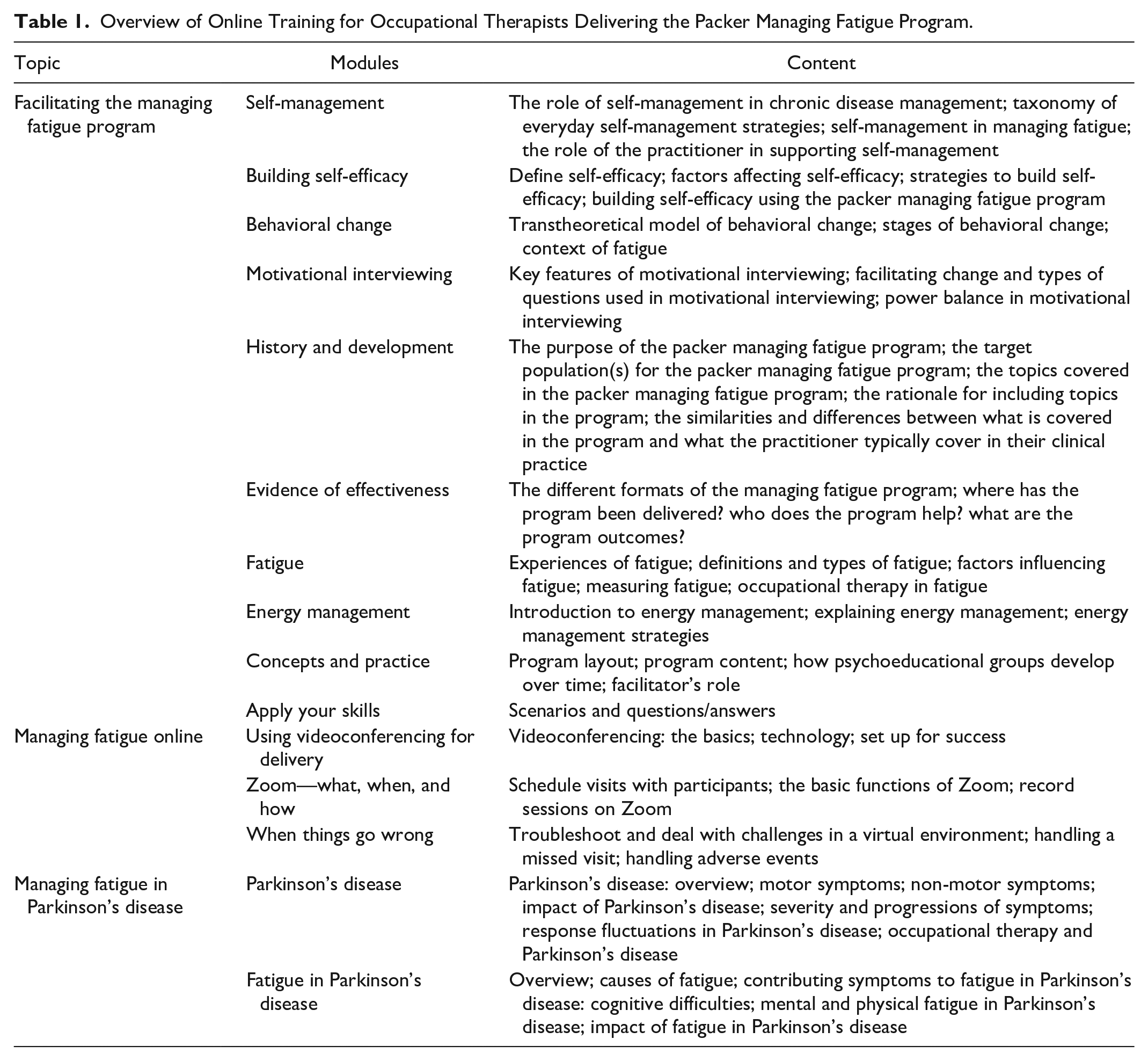
Sessions were delivered using the secure Zoom for Healthcare platform (Zoom Video Communications, 2023) with pre-session, in-session, and homework activities to trial and evaluate strategies. Each weekly session was expected to take 90 min, but times were adjusted based on client needs. Registered OTs who completed a 15-module online training course (Table 1) delivered the program. To ensure fidelity, a checklist designed by the research team was completed by the three involved OTs after each session.
Overview of Online Training for Occupational Therapists Delivering the Packer Managing Fatigue Program.
Data Collection
Participants (n = 12) completed two feasibility questionnaires and the Self-Efficacy for Performing Energy Conservation Strategies Assessment (SEPECSA; Liepold & Mathiowetz, 2005) using Opinio Survey Software (ObjectPlanet, n.d.). Individual interviews and focus groups, depending on participant preference, were conducted using Zoom for Healthcare (Zoom Video Communications, 2023). Both Opinio and Zoom for Healthcare are compliant with Canadian data protection regulations; the Personal Information Protection and Electronic Documents Act (PIPEDA) and the Personal Health Information Protection Act (PHIPA).
As part of the main study, participants also completed a demographic and clinical questionnaire at baseline. The FSS (Krupp et al., 1989) and the MMSE (Folstein et al., 1975) were used for screening purposes. The estimated Hoehn and Yahr scale (HY; Mischley et al., 2017) and the Geriatric Depression Scale: Short version (GDS-15; Sheikh, 1986) measured disease stage and depression, respectively. The main study protocol includes further details on the properties of these measures (Alizadeh et al., 2022).
Feasibility Questionnaires
Two self-report feasibility questionnaires were developed by research team (see protocol for more detail). One to be administered weekly (10 items), and one for completion at the end of the program (11 items), approximately 6 to 8 weeks after the baseline testing. Feasibility was centered on specific program delivery and content, as well as client perceived impact. Consequently, these questionnaires were developed using statements on perceived impact, the content of the program, the frequency and length and pace of the therapeutic sessions, and the organization and logistics. Weekly questionnaires had a greater focus on the weekly content and delivery rather than overall feasibility. For both questionnaires, the agreement level was measured using a 5-point Likert-type scale, ranging from “completely disagree” to “completely agree.” These questionnaires were then transferred to Opinion survey software and piloted among the research team for clarity and user-friendliness. Participants’ perceived confidence in using the strategies taught in the program was measured using the SEPECSA (Liepold & Mathiowetz, 2005). All questionnaires were completed digitally in Opinio via personalized email links. Table 2 summarizes the characteristics and timing of all questionnaires.
Measurements Used in the Study and Their Properties.
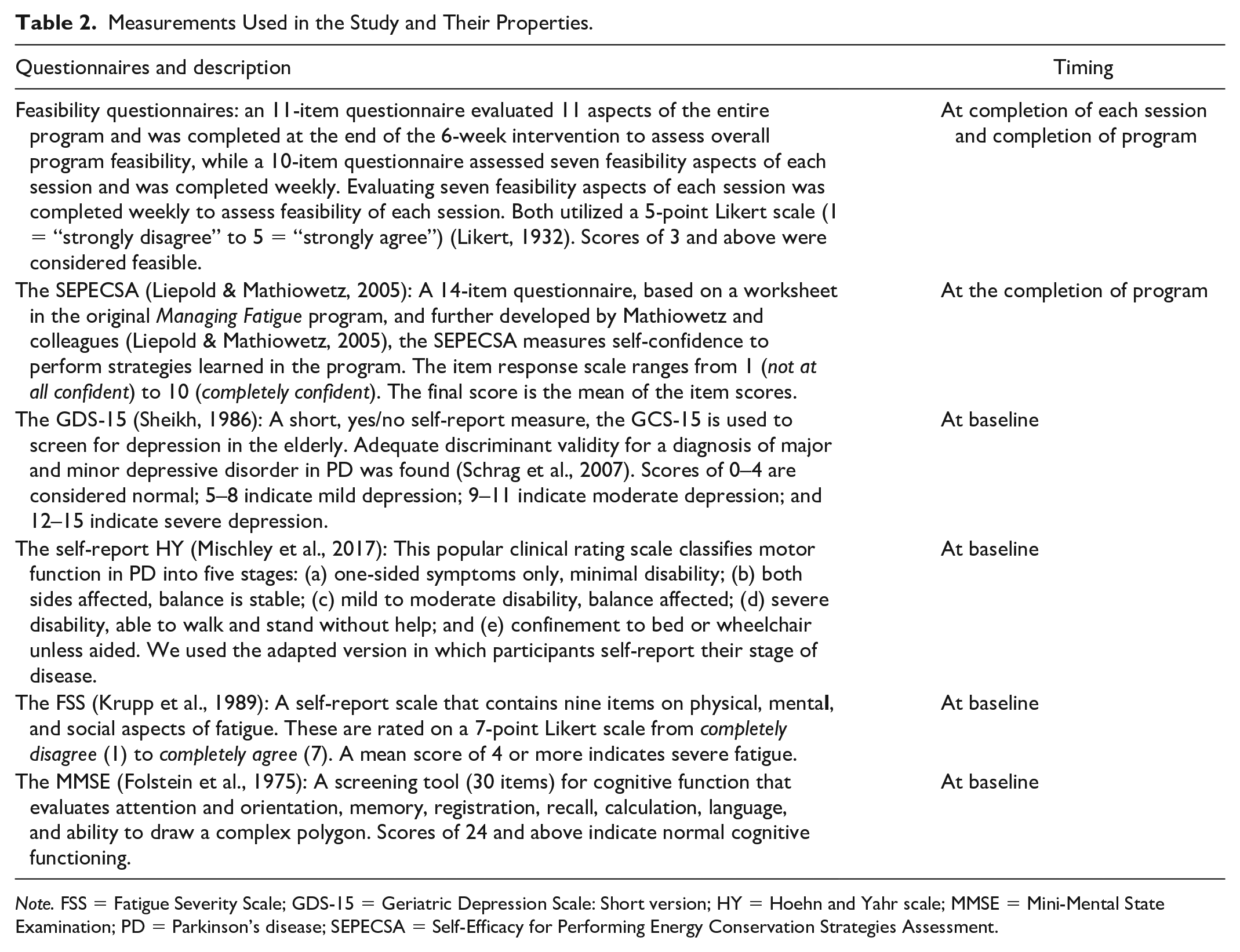
Note. FSS = Fatigue Severity Scale; GDS-15 = Geriatric Depression Scale: Short version; HY = Hoehn and Yahr scale; MMSE = Mini-Mental State Examination; PD = Parkinson’s disease; SEPECSA = Self-Efficacy for Performing Energy Conservation Strategies Assessment.
Focus Groups/Individual Interviews
An experienced researcher (SJ), not involved in delivering the intervention, scheduled, at mutually agreed upon times, and conducted as semi-structured, open-ended, non-directional interviews. Participants could choose between individual interviews or focus groups based on their preferences. An interview guide, developed by the first author and reviewed by the larger research team, sought to explore the perspectives of participants in the program. Questions and prompts related to the feasibility of the program’s content and delivery, barriers or facilitators that prevented or helped apply the skills learned in the program, the perceived impact of the program, and modifications they would like to see made were included.
Data Analysis
Descriptive statistics (mean, SD, and quartiles) examined demographic data and data from questionnaires. Interviews and focus groups were transcribed using NVivo software (QSR International, 2020). Thematic analysis (Braun & Clarke, 2006), using both inductive and deductive coding, was conducted to analyze the text data. A priori codes based on research topics were used to organize the data once the codebook was tested for applicability and intercoder reliability between the two coders. Conceptual categories were identified and connections explored using constant comparative methods. Disagreements were resolved based on consensus. The final list of themes with de-identified sample quotes was reviewed by participants and the interviewer for validity; no changes were suggested. Pseudonyms were used to report findings.
Results
Demographics
All 12 participants in the intervention group of the main study completed the feasibility questionnaires, and 10 completed the SEPECSA due to missing data for two participants. Nine of the 12 agreed and gave consent to participate in an interview or focus group. Most participants identified as male (n = 9), and the overall average age for the entire sample was 68.6 ± 9 years, with a disease duration of 5.8 ± 3.4 years. Participants reported average FSS scores of 5.4 ± 0.9 and MMSE scores of 28.5 ± 1.3. The mean depression score (GDS) was 6.2 ± 3.4, and disease stage ranged from 1 to 3 on the YH scale (median = 2). It is notable that 93% of participants did not receive any other health care services apart from their regular neurologist visits, and none had received OT services. The fidelity of the program was measured and reported as 100% following the program protocol.
Feasibility Questionnaires
The overall program feasibility showed mean item scores of 3 or higher (out of 5; mean range: 3.5–4.3; Supplementary Table 3). Aspects of “helpfulness” and “skill-training” received the highest mean scores. Consistent with the thematic data (see below), “tailoring” and “pace and duration” received the lowest scores (Figure 1, Supplementary Table 3).
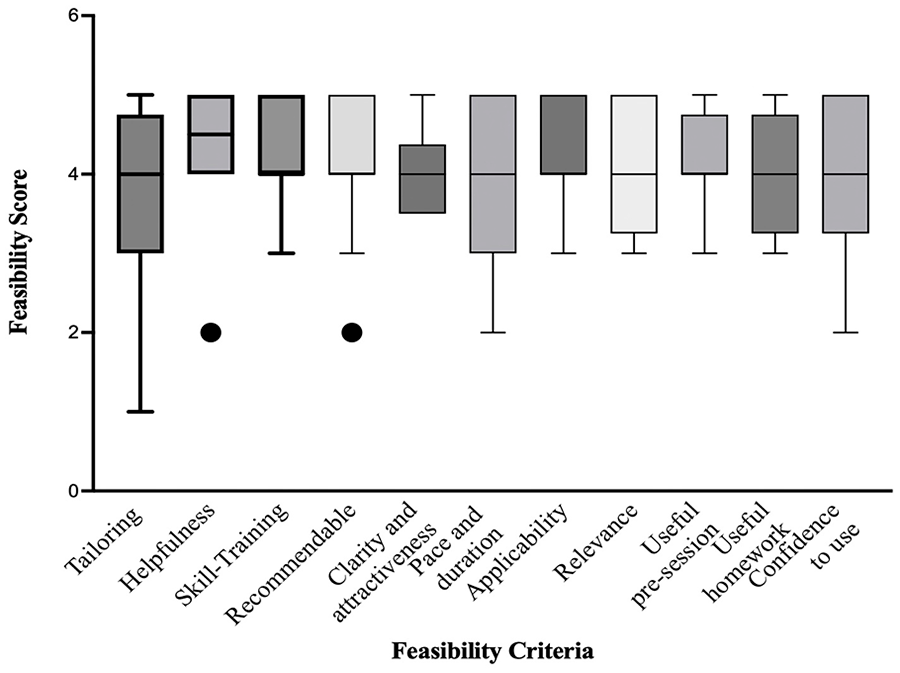
Tukey Plot for the Overall Feasibility of the Packer Managing Fatigue Program.
Feasibility of each session was evaluated individually. All sessions were considered feasible, with mean scores of 3.7 and above, out of 5. The first session was judged the least feasible, while the last session was considered the most feasible. The lowest feasibility score was for “appropriate pace” in Session 1, and the highest score was for the “encouraging aspects” of Session 6 (Table 3).”
Feasibility by Session of the Packer Managing Fatigue: A 6-Week Individual Self-Management Program.
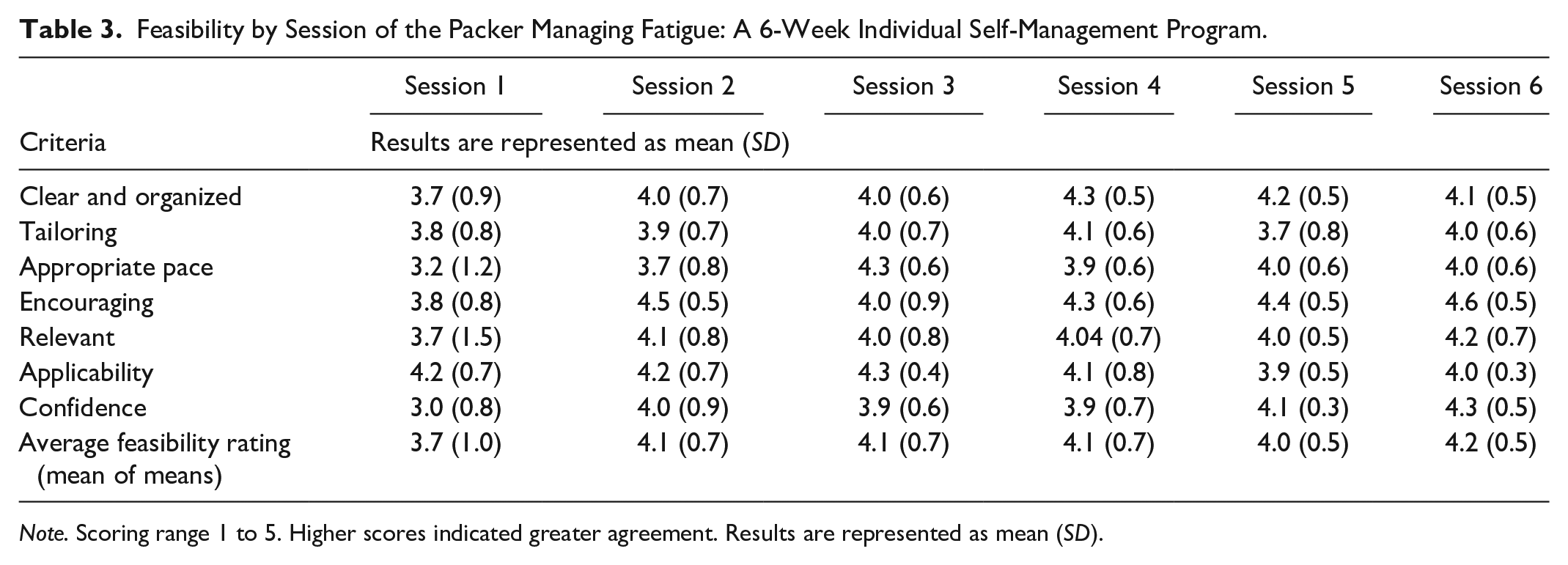
Note. Scoring range 1 to 5. Higher scores indicated greater agreement. Results are represented as mean (SD).
Data from the SEPECSA questionnaire indicated that participants were confident to apply the learned strategies. Mean scores for each strategy were above 6 out of a possible 10 (mean range: 6.4–8.5; Table 4).
Confidence to Use Energy Conservation Strategies Based on the Self-Efficacy for Performing Energy Conservation Strategies Assessment (SEPECSA).
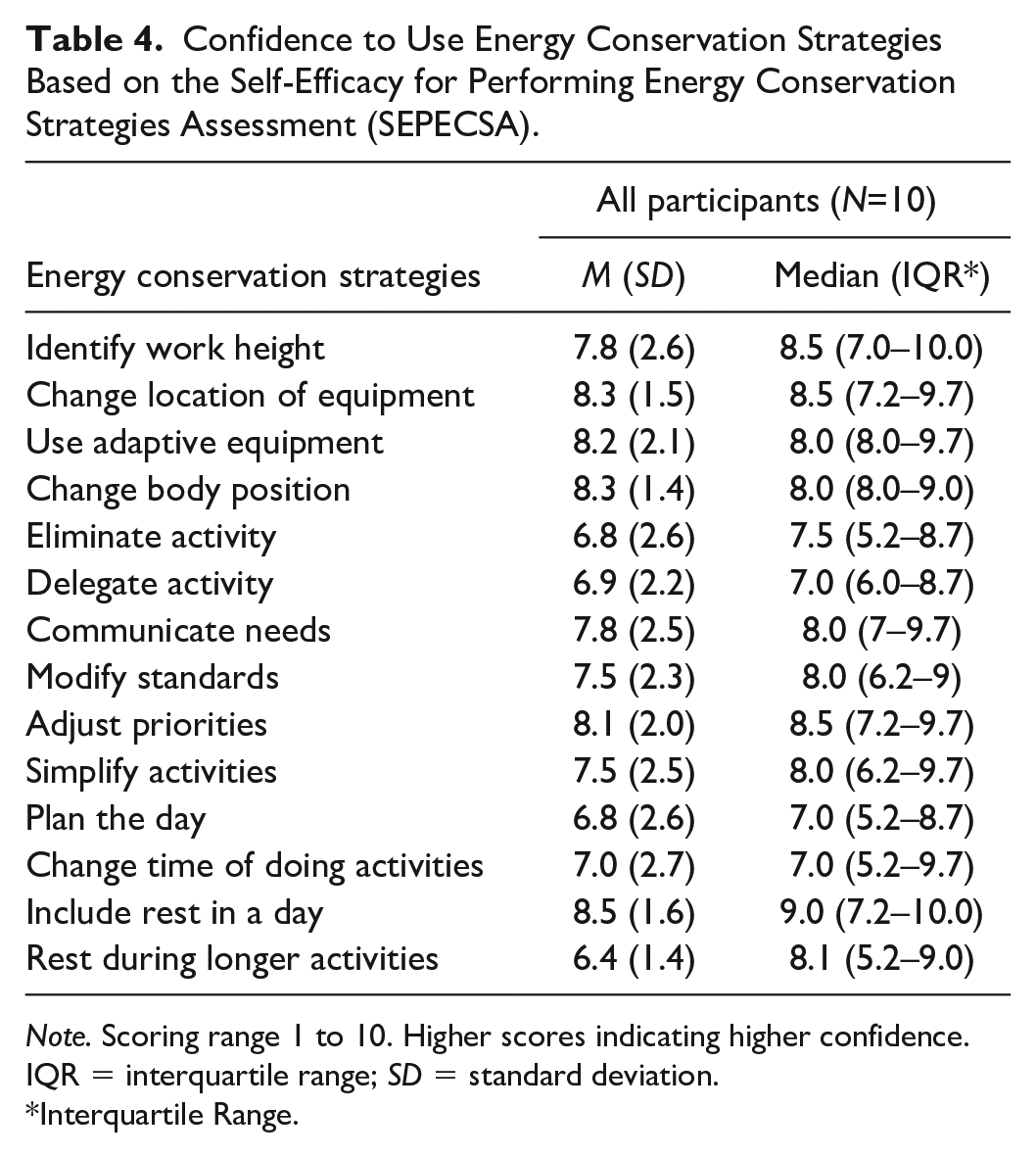
Note. Scoring range 1 to 10. Higher scores indicating higher confidence. IQR = interquartile range; SD = standard deviation.
Interquartile Range.
Focus Groups/Individual Interviews
A total of five themes clustered into three domains emerged and are described below. The first domain was the Perceived Impact of the Program, which included one major theme: Program was helpful. The second domain was Program Content and Structure, which included two themes: Program Has Strengths and Areas for Improvement. The third domain was Support and Delivery, which included two themes: Individual, Online Delivery Is Feasible and More Support from OTs Would Be Helpful (see Supplementary Table 2).
Domain 1: Perceived Impact of the Program, Theme 1: Program Was Helpful
The program was found to be helpful and a positive opportunity to learn and adopt strategies to manage the negative impact of fatigue on meaningful daily occupations. Examples included simplifying tasks, using assistive/adaptive devices, proactively planning, and organizing, and understanding that rest is a permissible and beneficial activity: I found the lessons on dividing tasks into smaller chunks rather than tackling a whole project at once particularly helpful. Before the program, I would often spend a whole or half day in the garden without taking breaks, and the next day I would feel completely exhausted. The program taught me that it’s much more sensible to take frequent breaks and rest, so that you have energy for the next day. When I started the program, I didn’t realize the importance of breaking tasks into smaller pieces, but now I see how much it can help conserve my energy. (Sophia)
In addition, participants experienced increased self-acceptance, optimism, and motivation for self-care: I used to put off things that should have come first, such as taking care of myself, [things] so that you can actually have the energy to do your activities and to help you slow the progression of your disease, your stress, your sleep, your fatigue, and everything else. So yeah, I learnt to put myself first now and that’s very inspiring that it really helped me to do that. (Noah)
Some reported experiencing positive outcome after learning how to say “no” and express their needs. Others realized that communicating their concerns is important but found it challenging due to the belief that others may not fully understand or accept their situation: I know it’s important to communicate my needs, and while I try to share as much as I can, I don’t usually go into detail about everything because it can become overwhelming. I usually stick to simpler things . . . people can easily understand those things. Explaining things like fatigue can be more difficult to convey to others. (Jack)
Although the program was perceived as helpful, most participants reported that the fatigue severity did not decrease. Sophia said, “I think I still get fatigued, and I know it is due to the progression of the disease, not the program.”
Domain 2: Program Content, and Structure
Theme 1: Program Has Strengths
Participants appreciated the printed manual and inclusion of pre-session and homework activities. These elements supported them to prepare for and practice program content. Mohammad said, “Having the physical manual was really helpful. I could go back and review it whenever I needed to. It made me feel confident that I had all-time access to the content.”
The specific focus of the program on fatigue made it important and meaningful. Sophia said: “Well, the word itself, fatigue, was like bingo for me to say this is relevant to me. I didn’t know how really to deal with fatigue. That’s what attracted me.”
Theme 2: Areas for Improvement
Participants wanted more PD-specific language and the incorporation of additional content pertaining to other factors that impact their fatigue. Megan expressed this as, “It was definitely relevant, but I think the program wasn’t specifically designed for fatigue in PD, it was for fatigue in general.” Similarly, Ava noted: “I kept looking for the word Parkinson’s and it wasn’t there. It was all MS.”
Some participants expressed concern that certain factors affecting their fatigue management, such as medication impacts, anxiety, mood swings, and poor physical fitness, were not addressed. For example, Ava mentioned, “I find my energy level low, both physical and mental. There were no exercise components in the program.” Jack suggested, “I have bad and good times, mostly based on my medications. I think some information on that would be helpful for patients.”
Domain 3: Support and Delivery
Theme 1: Individual, Online Delivery Is Feasible
The individual videoconference delivery was feasible, especially during the pandemic. Sophia expressed her appreciation for the personalized sessions stating, “It’s great that the sessions were just for me. Having the OT in an individual session helped me learn more as she could pace things based on my needs.” Some preferred virtual over in-person delivery. Lucas explained this as: “In a virtual way, you’re not overawed by the presence of another person, you can concentrate on the questions and topics. So, I am in favour of the virtual approach.” Freddie found the virtual delivery feasible during the pandemic, though indicated a preference for in-person meetings, “I think meeting over Zoom worked well. Obviously, it’s much nicer to be in person. I like being in a room with my therapist together, so I could actually feel more involved.”
Theme 2: More Support From OTs Would be Helpful
Participants asked for additional support from their OTs including follow-up after the program. Murphy said, “Maybe a reminder or a phone call to review the materials I had to do would have helped me to keep up with the program.” In addition, some participants expressed a desire for more feedback from their OTs. Mohammad said, “I work better with more feedback than free flow.”
Participants voiced a preference for a more tailored pace and duration of the sessions. They recommended that sessions be prioritized or intensified based on individual needs, considering good/bad days. Ava suggested shortening the sessions, “The sessions were too long considering that it was meant to help people with fatigue. I think they need to be shortened.” Jack added, “It’s important to consider how the session will run, whether you’re having a good day or a bad day. Sometimes, I could handle more, but on other days, it felt overwhelming.”
Discussion and Conclusion
While evidence of effectiveness is documented for the Packer Managing Fatigue program in neurological conditions including MS and neuromuscular conditions (Finlayson et al., 2011; Sauter et al., 2008; Veenhuizen et al., 2019), less is known about its effectiveness and feasibility for PwPD. To our knowledge, this is the first study to introduce this program to PwPD and to explore their perspectives and experience.
The findings of this study support the feasibility of the individual format of the program for PwPD across various areas, including the relevance and applicability of the content in the program, the building of confidence, and a perceived positive impact on daily life performance. Similar results were observed in a prior mixed-methods study involving individuals with neuromuscular conditions, which reported overall satisfaction with the impact, content, and delivery of the group format of the program (Veenhuizen et al., 2019).
Among all strategies, participants expressed the highest level of confidence in incorporating rest into daily routines. Strategic resting is a critical strategy of the program, with participants reporting that changes in rest schedules can lead to an instant reward and a sense of control over their fatigue (Packer et al., 1995). This is supported by a previous study that found rest and planning were effective strategies for individuals with MS (Matuska et al., 2007). Based on the theoretical foundation of OT, rest is considered an essential aspect of an individual’s daily activities, and an optimal balance between work, self-care, and leisure is crucial to achieve maximum function and overall health (Reed & Sanderson, 1999). This evidence suggests that interventions aimed at understanding and practicing rest are beneficial for people with fatigue.
In addition to the content and strategies, the one-to-one delivery of the program was also considered feasible by participants. The absence of peer support was not missed by participants in our study, although earlier research has emphasized the significance of group settings and the advantages of peer support and interaction in fatigue programs (Hersche et al., 2022). On the contrary, the majority felt that the individual format provided them with focused attention from the OTs. Similarly, a previous review study that examined qualitative papers (n = 15 articles) focused on telehealth interventions supporting clients with long-term conditions (LTCs) did not find substantial evidence supporting the inclusion of peer support in group-based delivery as a crucial factor for successful intervention (Vassilev et al., 2015).
Participants also expressed satisfaction with the convenience and accessibility of videoconference sessions, which facilitated physical distancing during the pandemic. Telehealth delivery has been shown to be valuable for individuals with chronic conditions, enabling trust-building relationships with practitioners and providing greater control over participation (Vassilev et al., 2015). It is notable that while virtual delivery was found to be feasible, a few participants expressed a personal preference for live interaction with their OT if a safe opportunity was available. The importance of human interaction and personal contact for individuals with long-term conditions has been highlighted in previous research (Barenfeld et al., 2022).
While the program’s content and delivery were considered feasible, participants discussed unique aspects of PD-fatigue experiences. Consistent with a previous study by Mantri et al. (2020), participants in the current study reported that their fatigue was linked to emotional, physical, and cognitive factors. Medication regimens, mood, anxiety, limited physical activity, and disease progression made management difficult. A client-centered, comprehensive approach with regular access to specialists and timely follow-up has been recommended for management of PD (Andrejack & Mathur, 2020). Embedding fatigue programs in a larger multidisciplinary setting where all factors contributing to PD-fatigue can be managed is likely to alleviate shortcomings of a stand-alone program. Incorporating physical exercises, inspired by self-management principles, into fatigue management may further reduce the negative impact of fatigue (Kim et al., 2022). Combining the Packer Managing Fatigue program with aerobic training and relapse prevention has been tested and shown to lead to improved social participation and functional endurance for people with neuromuscular disease (Veenhuizen et al., 2019). In PD, however, evidence of effectiveness of the program, either alone or in combination, is yet to be tested. Given that participants in this study reported limited access to rehabilitation or health professionals other than neurologists, future studies, comparing outcomes in different contexts, may provide unique insights into optimal delivery formats.
The existing literature underscores the importance of tailoring therapeutic interventions to address the unique needs of distinct subgroups within the PD population as PD symptoms and experiences manifest uniquely in different individuals. However, many PD programs struggle to implement such tailored approaches (Greenland et al., 2019; van den Heuvel et al., 2020). PD is a complex and multidimensional condition with differential individual symptom constellation and severity, making individualized care and therapeutic plans crucial (Davis et al., 2003; Greenland et al., 2019). Although the Packer Managing Fatigue program encourages tailoring the program to participant’s priorities, they rated this feature least favorably. When asked to explain this, some described topics, or services outside the scope of the program, such as prescription of assistive devices, treatment of physical problems, and management of sexual relationships. This may reflect the lack of regular access to OTs and other health care professionals with capacity to meet their needs. In addition, considering the perspective of participants, fatigue programs may benefit from establishing a more direct connection by incorporating content and examples specifically tailored to PD. While it may not be feasible to produce stand-alone PD programs, ways to address PD-specific needs are evident. These results also highlight the importance of required therapists’ training modules, particularly for therapists with limited PD experience, arguing for even greater content to address specific needs of PwPD. It is of value to note that, as a result of this study, the newly published individual protocol of the Packer Managing Fatigue program incorporates more disease-specific stories and examples in both the therapists’ and participants’ manuals.
While participants in the program learned skills to mitigate the negative fatigue impact on daily life, few also reported no change in fatigue severity. Previous studies have also shown that fatigue severity did not change for people with MS (Veenhuizen et al., 2019). This is not surprising, given that the program’s goal is not to reduce the fatigue severity but to manage its negative impact (Packer et al., 1995). It is also possible that, as fatigue is better managed, individuals become more knowledgeable finding ways to incorporate new activities or intensify existing ones without experiencing a decrease in fatigue severity. Given that the program’s primary goal remains focused on managing the impact of fatigue rather than solely reducing fatigue intensity, emphasizing and communicating this distinction, participants will better understand that the program aims to equip them with strategies to cope effectively with fatigue-related challenges.
Delivering integrated client-centered care for fatigue management also depends on the expertise of health care providers, including OTs, who can build communication, trust, and client engagement, and deliver care using a personalized approach (Babatunde et al., 2017). Care delivered by OTs specialized in PD care has been associated with fewer PD-related complications, suggesting the need for more extensive training modules to enhance practitioner expertise and the therapeutic alliance (Talebi et al., 2023). One limitation of the current study was the lack of measurement of practitioner expertise and the therapeutic alliance. In addition, this study was conducted during the COVID-19 pandemic lockdown, which introduced many restrictions on participants’ activities, including willingness to participate. While videoconference was considered feasible, it too may have influenced recruitment and participation as it may have introduced bias, especially for individuals without reliable internet access. Future research conducted at different times and contexts is needed to support or repudiate these results. The advantage of researcher-designed feasibility questionnaires is their specificity to the delivered program. The disadvantage however is the lack of psychometric testing. Finally, as a pilot study, the sample size was expectedly small. Like all studies, the inherent limitations mean generalization should be done cautiously.
Conclusion
This study highlights the feasibility of the Packer Managing Fatigue program and its potential to be incorporated into the repertoire of interventions employed by OTs working with PwPD. The study offers new insights into the development and implementation of effective fatigue interventions from the perspective of PwPD, making a significant contribution to the field. Future studies may evaluate the implications and effectiveness of the program in large-scale studies for PwPD.
Supplemental Material
sj-docx-1-otj-10.1177_15394492241262740 – Supplemental material for Client Perceptions of the Individual Packer Managing Fatigue Program: A Mixed-Method Evaluation
Supplemental material, sj-docx-1-otj-10.1177_15394492241262740 for Client Perceptions of the Individual Packer Managing Fatigue Program: A Mixed-Method Evaluation by Neda Alizadeh, Tanya L. Packer, Sabrena Jaswal, Ingrid Sturkenboom and Grace Warner in OTJR: Occupational Therapy Journal of Research
Footnotes
Acknowledgements
We would like to express our gratitude to the study participants and the occupational therapists who took part in this research and shared their time and insights with us. Their contributions made this study possible.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Packer is co-founder, with no financial interest, of Think Self-Management Inc. Think Self-Management provides health care professionals with the tools and resources to empower people living with chronic conditions to cultivate the self-management skills they need to live happier, healthier lives. The Packer Managing Fatigue Program is distributed by Think Self-Management. None of the other authors declares real or potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted as part of the PhD research of the first author. This work was supported by Abdulmajid Bader scholarship; Funding Package for PhD studies from the School of Occupational Therapy, Dalhousie University; Scotia Scholars Award ( George Turnbull Student Research Award), Nova Scotia Graduate Scholarship Program (NSGS); and the LSVT Global Student Grants (LSVT-S).
Ethical Approval
The Nova Scotia Health Sciences Research Ethics Board approved this study (ref: 1027048).
Trial Registration
ClinicalTrials.gov identifier: This study is part of a larger randomized controlled trial study that was registered in ClinicalTrials.gov with the identifier number NCT04267107.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.