
Abstract
Limited evidence exists on the impact of cerebral visual impairment (CVI) on developmental domains in toddlers. This study investigated whether CVI influences social skills and sensory processing in toddlers with cerebral palsy (CP). The study included toddlers with CP, with or without CVI, and typically developing (TD) toddlers. All parents completed the demographic information form. Social skills were assessed by the Brief Infant–Toddler Social and Emotional Assessment (BITSEA). Sensory processing was evaluated by the Infant/Toddler Sensory Profile (ITSP). Analysis of covariance was employed to assess the disparity in BITSEA and ITSP scores. Toddlers with CP and CVI group demonstrated lower social competence than the other groups (p < .05). Having CVI did not cause a statistically significant difference in sensory processing among toddlers with CP (p > .05). CVI significantly affects social competence in toddlers with CP but does not affect sensory processing.
Plain Language Summary
Cerebral palsy (CP) is a lifelong condition that affects a child’s ability to control their muscles and movements. It occurs due to damage or abnormalities in the brain that happen before, during, or shortly after birth. This condition can affect various aspects of daily life, including walking, feeding, and dressing. It often leads to challenges in physical skills and may be accompanied by difficulties in sensory, cognitive, and social functions. One of the accompanying difficulties is cerebral visual impairment (CVI), a common challenge for these children that affects their vision without apparent eye problems. As vision is crucial for social development, children with CVI may experience socio-visual deprivation, leading to cognitive deficits and behavioral difficulties. This study explores how vision influences the social and sensory abilities of toddlers with CP. We compared 66 toddlers: 22 with CP and CVI, 22 with CP without CVI, and 22 typically developing toddlers. The findings reveal that toddlers with CP and CVI group demonstrated lower social competence than the other groups. However, the presence of CVI did not cause difference in sensory processing among toddlers with CP. Understanding the impact of CVI on social and sensory skills is crucial for developing tailored therapy interventions for toddlers with CP. This research sheds light on the intricate relationship between vision and social competence, emphasizing the need for targeted support for these children. By recognizing and addressing these challenges early on, we can enhance the overall well-being and development of toddlers with CP.
Introduction
Cerebral palsy (CP) is a permanent, non-progressive, group of disorders that primarily affect the development of mobility, postural control, and balance (Graham et al., 2016). Motor impairments of CP are frequently accompanied by sensory, perceptual, cognition, and social/behavioral disorders (Horber et al., 2020). According to the International Classification of Functioning, Disability and Health—Children and Youth version, the disturbances associated with CP are multifactorial, influenced by not only the conditions specific to CP but also personal and environmental factors (World Health Organization, 2007). For instance, studies have shown that visual impairment (VI) in children with CP affects communication, emotional contact, self-care, and intelligence (Schenk-Rootlieb et al., 1993). The prevalence of VI in children with CP was found to be between 34% and 59.5% (Rauchenzauner et al., 2021). VIs resulting from neurological events observed in children with CP are considered under the umbrella of cerebral visual impairment (CVI) (Philip & Dutton, 2014). Recently, CVI has been defined as a verifiable VI that cannot be attributed to anterior visual pathway disorders, for example, optic disk pallor, or any other potentially co-occurring ocular problems (Sakki et al., 2018). Severe VI of any etiology has a significant impact on several developmental domains (motor, social, emotional, and academic) (Chadha & Subramanian, 2011). Vision plays a key role in these developmental domains, especially in social development. The first indicators of the formation of the “social brain” are visual-based skills such as sensitivity to eye-like stimuli, biological movement preference, imitation, face recognition, and gaze tracking (Grossmann & Johnson, 2007; Leppänen & Nelson, 2009). Therefore, children with CVI who suffer from severe socio-visual deprivation may manifest severe cognitive deficits and be prone to stereotyped behaviors and mannerisms (Chokron et al., 2020).
While acknowledging the undeniable importance of vision for social development, it is essential to recognize that CP predominantly manifests as motor impairments. These motor skills, such as walking, have been correlated with significant advancements in social development. Nevertheless, the precise nature of the relationship between motor skills and social development remains a topic of ongoing research, with varying study outcomes (Libertus & Hauf, 2017). To comprehensively investigate this complex interplay, it is imperative to also consider the impact of early visual deprivation on the neural architecture and sensory processing in children with CP. In addition, early visual deprivation can affect the functional architecture and connectivity of cortical areas responsible for processing visual inputs, leading to alterations in the size, functional architecture, and neural response qualities of the primary somatosensory area, S1, as observed in studies (Dooley & Krubitzer, 2019). These changes are considered to underlie sensory processing disorders (SPDs) in children with CP (Papadelis et al., 2018). Children with CP often experience a spectrum of SPDs, affecting emotional responses, physical activities, and attentional engagement. These challenges manifest in impaired modulation of sensory inputs, affecting emotional reactions, and diminished resistance during physical activities. In addition, they struggle to register sensory inputs—particularly visual and tactile stimuli—and experience heightened sensitivity to head positioning in space (Pavão & Rocha, 2017). In a recent review, it was shown that SPD affects gross motor skills, everyday activities, balance, communication skills, attention span, and strabismus in children with (Kantor et al., 2022).
Building upon these interconnected behavioral manifestations, we intend to investigate the impact of CVI on social competence and sensory processing in toddlers with CP. The null and research hypotheses of our study posit that CVI has no effect on social competence and sensory processing in toddlers with CP.
Methods
The study was conducted in accordance with the ethical guidelines established by the Declaration of Helsinki and was approved by the Ethics Committee of Hacettepe University (Registration Number: GO 22/351; Registration Date: May 22, 2022). Written informed consent was obtained from all parents before data collection. Participants were recruited between May 2022 and January 2023 in a special education and rehabilitation center that specialized in visual and physical impairment rehabilitation in the capital city of Türkiye.
In this study, all caregivers included in the study filled out a demographic information form related to family structure and environment, the Brief Infant-Toddler Social and Emotional Assessment (BITSEA) form, and the Infant/Toddler Sensory Profile (ITSP) form under the supervision of two researchers with 10 years of experience in pediatric physical and occupational therapy (OT). Each participant’s assessment session took approximately 30 min.
Participants
To reduce the impact of related factors on social and sensory skills and to provide an optimal comparison, in addition to toddlers with CP with and without CVI, typically developing (TD) toddlers were included in this study. The sample size of the study was calculated by analysis of variance (ANOVA) fixed effect, omnibus, one-way test parameter, and a priori type power analysis using G*power 3.1 software. To determine the difference in BITSEA (primary social competence measurement tool) scores between three different groups, the required number for the total sample size was determined as 22 toddlers in each group at a large effect size (f = 0.40), with 95% confidence interval and 80% study power. A large effect size was accepted for the study because BITSEA has high sensitivity (0.84) and specificity (0.90) to detect psychosocial problems (de Wolff et al., 2013). As a result, the sample size should contain 22 toddlers in each group.
Specifically for this study, we determined the CVI status in toddlers with CP using the Special Needs Report for Children (SNRC). Specialized physicians, experts in physical medicine, rehabilitation, child and adolescent mental health, ophthalmology, otorhinolaryngology, pediatric surgery, and pediatric health, conducted the evaluations for this report. If a child had multiple special needs, the report indicated the highest level of need, overseen by specialized boards with at least six permanent members, including four specialist physicians. The report detailed the child’s disability and categorized their special needs (Güller & Yaylacı, 2021). For the toddlers with CP and CVI group, our study included children diagnosed with CVI within the SNRC framework during their application to special education and rehabilitation centers.
The inclusion criteria for the toddlers with CP were as follows: (1) age between 12 and 36 months and (2) having a diagnosis of CP by the SNRC (the group of children with both CP and CVI additionally needs a CVI diagnosis and the absence any of significant ocular disorder by the SNRC).
The following criteria were used to include the TD toddlers: (1) age between 12 and 36 months and (2) absence of any ocular disorder. Toddlers with any of the following conditions were excluded: (1) refusal to participate in the research and (2) being deaf or blind. To promote inclusivity and engagement, invitations were extended on a voluntary basis to parents of TD toddlers during the study period. These invitations were distributed through an announcement prominently displayed on the bulletin board of the special education and rehabilitation center.
Measures
Demographic Information Form
Demographic data, including age, gender, and place of residence, parents’ education levels, and number of children, were collected with a demographic information form. Gross Motor Function Classification System (GMFCS) levels were also recorded for toddlers with CP. GMFCS levels were determined as follows: Level I: toddlers move in and out of sitting and can floor sit with both hands free to manipulate objects; Level II: toddlers can sit but may have difficulty with balance when both hands are free to manipulate objects; Level III: toddlers maintain floor sitting when the low back is supported; Level IV: toddlers frequently require adaptive equipment for sitting and standing; and Level V: physical impairments limit voluntary control of movement.
BITSEA
The BITSEA was developed by Briggs-Gowan et al. (2004) to identify children at risk of early childhood social–emotional/behavioral problems and delays. The assessment consists of 42 questions assessing both problems (Problem Scale [PS]) and delays in acquiring competencies (Competence Scale [CS]). Except for some questions, there are three response options (“not true/rare,” almost true/sometimes “very true/often”). The BITSEA is able to distinguish between children with and without social/emotional problems (Kruizinga et al., 2014). Internal consistencies of the BITSEA Turkish Form PS and CS were found good to excellent (Cronbach’s α = 0.82 and 0.72, respectively). Also, PS scores were found to be significantly correlated with the Child Behavior Checklist (CBCL) internalizing, externalizing, and total problem scores (Karabekiroglu et al., 2009). A higher total score on PS indicates a higher level of behavioral and emotional problems, whereas a lower total score on CS indicates a lower level of competence (Karabekiroglu et al., 2010).
ITSP
The ITSP, which is also known as the Infant Sensory Profile 2, is a standardized assessment tool that measures sensory processing ability and its reflection in daily activities in children aged 7–36 months, using their parents’ observations (Dunn & Daniels, 2002). The scale consists of 48 questions in five sensory processing domains (Auditory, Visual, Tactile, Vestibular, and Oral). The scale is scored by the primary caregiver with a five-point Likert-type scale. Scoring is done in four quadrants (Low Registration, Sensation Seeking, Sensory Sensitivity, and Sensory Avoidance) based on Dunn’s Sensory Processing Model obtained specifically in each sensory processing area (Dunn, 2001). In these quadrants, poor processing abilities are indicated by a score that is either lower (over-responsiveness) or higher (under-responsiveness) than the normal range of scores. A score between ±1 SD of the mean of the norm represents typical performance; a score between ±1–2 SD indicates a possible difference; and a score either lower or higher than 2 SD indicates an explicit difference (Lu et al., 2019).
Data Analysis
Data were analyzed using the SPSS 25.0 program (SPSS Inc. Chicago, IL, USA). Descriptive statistics of the data are given as count-percentage for categorical variables, and mean and standard deviation for continuous variables. The conformity of continuous variables to normal distribution was tested using the Shapiro–Wilk test. It was found that the BITSEA and the ITSP scores did not show a normal distribution. Therefore, non-parametric tests were applied. Participant differences between groups were investigated using the chi-square test for categorical variables and the Kruskal–Wallis test for continuous variables.
Based on the inferential statistics, the only significant difference observed was in parental education levels among all groups. Consequently, an analysis of covariance (ANCOVA) was planned to assess the disparity in BITSEA and ITSP subdomain scores between the groups while controlling for parental education levels as a covariate. However, Quade’s ANCOVA, also known as non-parametric ANCOVA, was employed because the scale scores did not adhere to a normal distribution, thus failing to meet the assumptions of ANCOVA (Quade, 1967). If the difference between the groups was statistically significant according to the results of the non-parametric ANCOVA, pairwise comparisons were performed. Given the variability in motor functionality levels between the CP groups with and without CVI, GMFCS levels were included as covariates in addition to parental education levels for pairwise comparisons between these two groups. This allowed us to isolate differences attributed to CVI. A significance level of .05 was used for the p-value.
Results
There was no difference between the groups in terms of age, gender, number of children in the family, and place of residence (p > .05). It was found that there was a difference between the maternal education level (p < .05). All parents of the TD toddlers had undergraduate or graduate education. It is a known fact that the family factor affects social competence and sensory processing in children (Guralnick et al., 2003; Neufeld et al., 2021). Therefore, our results, which will be presented below, should be carefully examined. On the contrary, it should not be disregarded that homogenizing maternal factors may cause an incidence–prevalence bias (Tripepi et al., 2010).
In children with CP groups, there was a disparity in gross motor functioning levels between the two groups (p < .05). All 44 toddlers included in our study had spastic type CP. Limb involvement was not recorded. Groups’ characteristics and differences between group characteristics are shown in Table 1.
Descriptive Characteristics of the Groups and Differences Between the Groups.
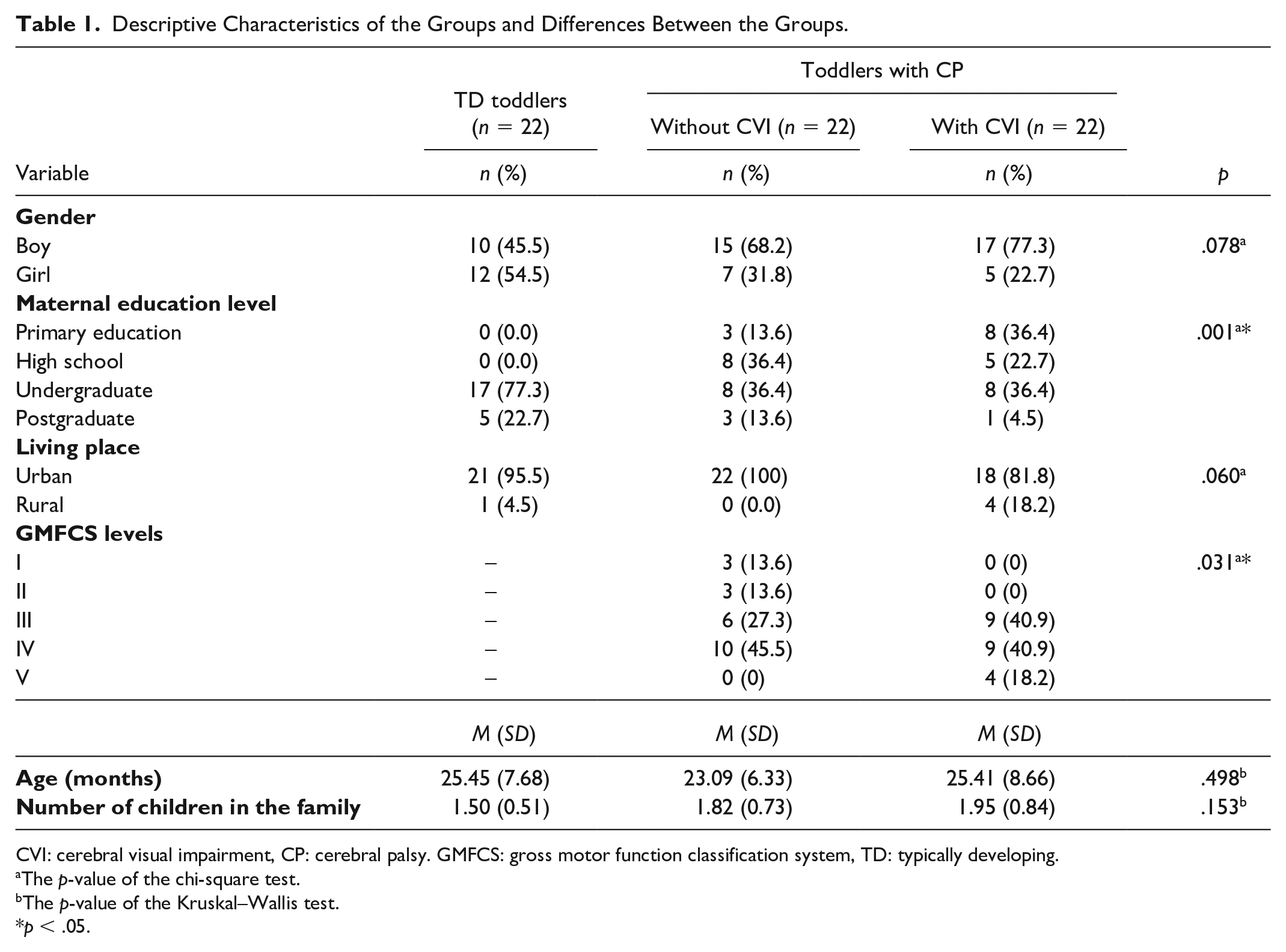
CVI: cerebral visual impairment, CP: cerebral palsy. GMFCS: gross motor function classification system, TD: typically developing.
The p-value of the chi-square test.
The p-value of the Kruskal–Wallis test.
p < .05.
When parental education level was considered as a covariate, differences were found between the three groups in all BITSEA and ITSP domains, except for the ITSP Seeking domain (p = .065). The comparison results of the three groups are presented in Table 2.
Comparison of Groups in Terms of BITSEA and ITSP Scores.
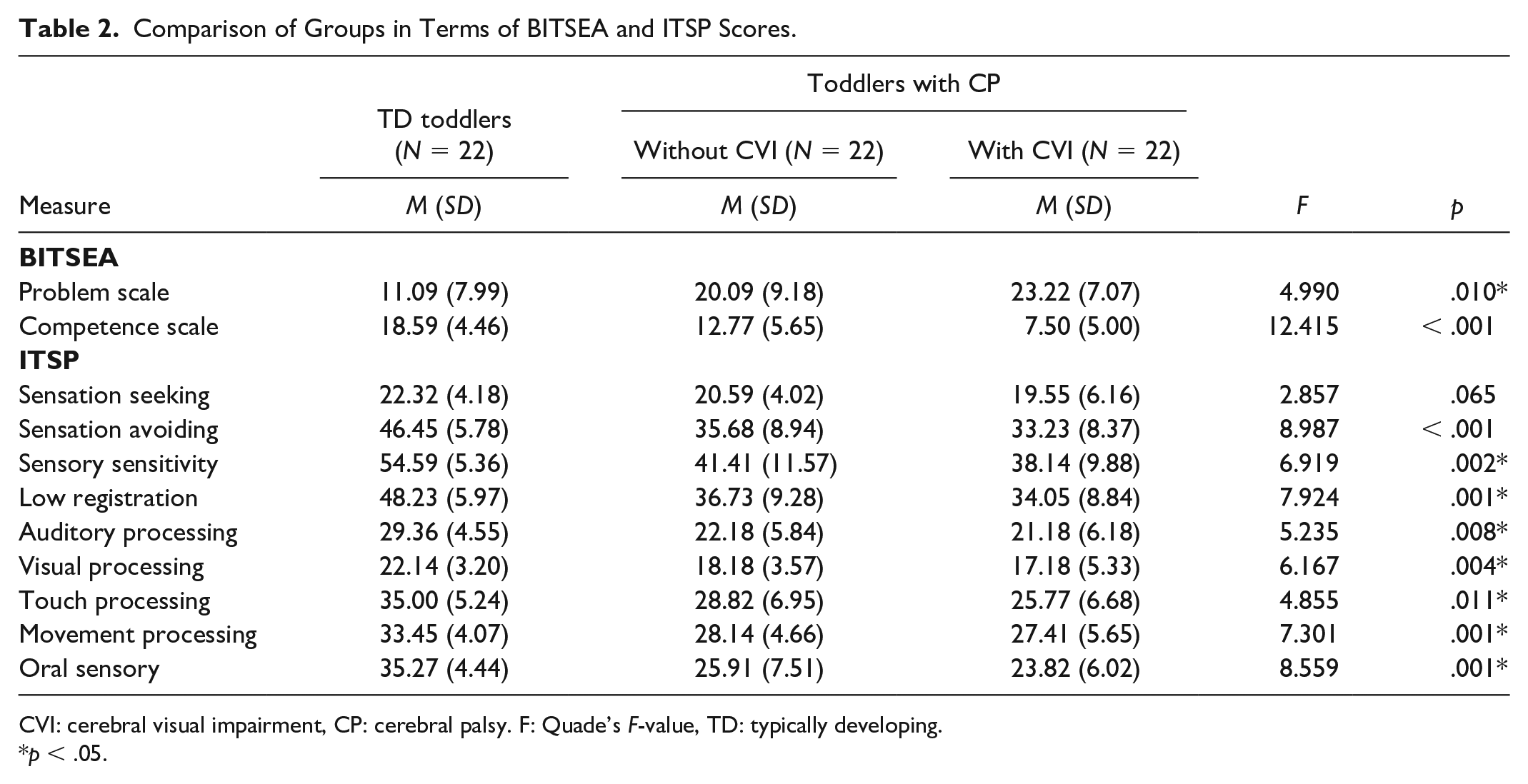
CVI: cerebral visual impairment, CP: cerebral palsy. F: Quade’s F-value, TD: typically developing.
p < .05.
In pairwise comparisons, a significant difference was found exclusively in the BITSEA CS across all pairwise comparisons of the three groups. This distinction implies that the presence of CVI affects the social competence scores in toddlers with CP (Table 3).
Pairwise Comparisons of the Groups.
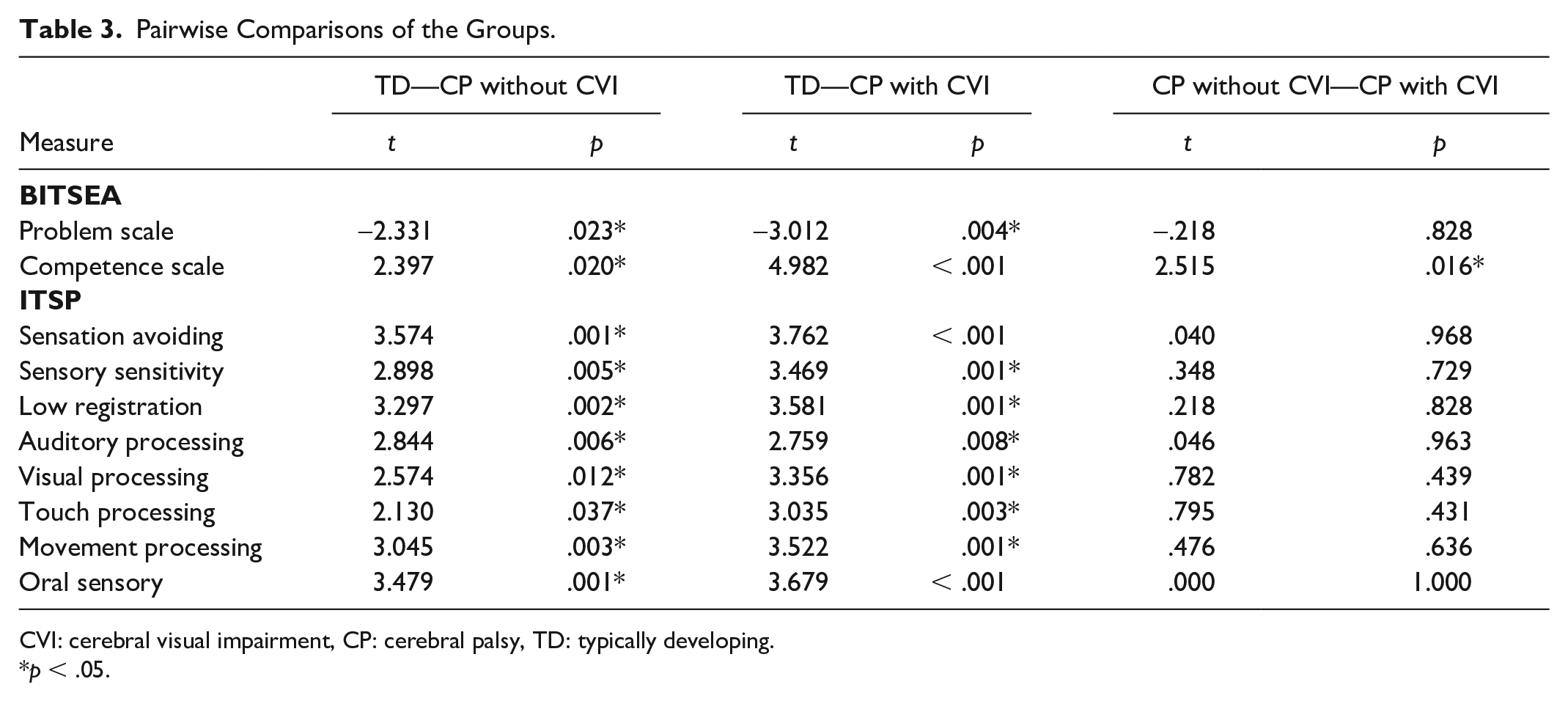
CVI: cerebral visual impairment, CP: cerebral palsy, TD: typically developing.
p < .05.
Discussion
This study aimed to investigate the impact of CVI on social competence and sensory processing in toddlers with CP. It was found that toddlers with CP differed from TD peers in terms of both social and sensory domains except for sensation seeking, and while CVI affected social competence, it did not affect sensory processing. These findings partially reject the study’s null hypothesis.
According to our study, toddlers with CP, regardless of VI, exhibited poorer social and sensory processing skills (except for sensation seeking) compared to TD toddlers. These findings align with previous research demonstrating impaired sensory and social skills in children with CP compared to their TD peers (Jovellar-Isiegas et al., 2020; Pavão & Rocha, 2017; Voyer et al., 2018). In addition, it is well established that several factors influence the social–emotional competence and sensory processing skills of children with CP, including parent-related and perinatal factors for social–emotional development and cerebral lesion severity for sensory processing skills (Park, 2017; Wu et al., 2021). Family factors play a pivotal role in the social competence development of toddlers with CP, affecting their social interactions and participation in activities. Furthermore, non-modifiable factors such as family type, parental education, and family cohesion consistently affect children’s engagement in leisure activities (Tsibidaki, 2020). Paternal roles and mental health, along with family preferences for social leisure activities, directly shape the social–emotional development of toddlers with CP (Ostojic et al., 2023). In our study, we encountered challenges in integrating familial factors due to their broad scope. Despite variations in parental education levels among participants, we addressed this by including it as a covariate in our analysis. In contrast to all other domains, sensory seeking was similar in the three groups in our study. A possible reason for this might be that toddlers with CP were included in habilitation programs at a relatively early stage, and their inadequacies in certain areas did not hinder their search for sensation. In more inclusive words, this could be interpreted as the fact that all toddlers are open and willing to change for the time being. We also would like to highlight that, concerning group characteristics, there were disparities in GMFCS levels among the toddlers with CP groups. Toddlers with concomitant CVI exhibited lower GMFCS levels. While this observation might suggest that toddlers with CVI could potentially have poorer performance attributable to their motor function, our study mitigated this concern by incorporating GMFCS levels as a covariate in the pairwise comparisons of CP groups. Through interpretations that consider differences and similarities between groups, our findings underscore the significance of investigating the impact of CVI on social and sensory processing skills. This highlights the importance of exploring the role of CVI in social competence in toddlers with CP in future studies.
Our findings indicated that toddlers with CVI had less social competence when compared with TD and CP without CVI groups. Social competence refers to handling social interactions in different social contexts (Case-Smith & O’Brien, 2014; Orpinas, 2010). It has been theoretically stated that CVI can negatively affect the processing of socio-visual information. For example, it was stated that impaired visual processing negatively affect parent–child attachment, non-visual senses are dominant during social interaction, and ultimately lead to disorders in interpersonal social interaction skills in the future (Lueck et al., 2019). Our results roughly confirm this theoretical knowledge, because the BITSEA social competence domain questions were consistent with the proposed theory. Specifically, the BITSEA competence domain questions—which cover the areas of mastery motivation, compliance, atypical behavior, prosocial peer relations, attention, empathy, and imitation/play—were collected from the subdomains of ITSEA, which is the long version of BITSEA (Briggs-Gowan et al., 2004; Carter et al., 2003). Recently, Wu et al. (2021) investigated social–emotional development in children with CP without VI and found that children with CP had lower externalization and social competence scores than their TD peers. At the same time, the authors found that preterm infants had higher scores in the ITSEA problem domain and lower scores in the ITSEA competence domain. However, being preterm is a major risk factor for CVI (Geldof et al., 2015). It is likely that there were infants with undiagnosed CVI in the study of Wu et al. (2021, Hellgren et al., 2020). On the contrary, diffusion-based imaging studies have found that CVI is a kind of a brain disconnection disorder (Bauer, 2020). For this reason, neural structures that cannot be specialized due to cerebral disconnection may cause executive dysfunction and lead to social behavior disorders (Bottcher, 2010; Gosling, 2017). In this direction, the neural–cognitive–behavioral model, which is used to explain the social interaction and communication disorders in autism spectrum disorder (ASD), can be used to understand the effect of CVI on social competence (Beauchamp & Anderson, 2010; Soto-Icaza et al., 2015). For example, in emotional face recognition tasks, individuals with CVI and ASD were found to have the same atypical processing and could not be distinguished from each other (Kovarski et al., 2021). It was also reported that the development of social cognition in children with ASD and early brain injury requires preserved structural and functional brain connections of biological motion processing (Pavlova, 2012). Based on the neural–cognitive–behavioral model, considering the prevalence of dorsal stream vulnerability in infants with CVI (Braddick et al., 2003), in the early stage of life the inability to focus on eye-like stimuli and faces due to deficiencies in fixation, visual acuity, and contrast sensitivity (Galli et al., 2022) may prevent the consistent processing of rudimentary face and biological motion processing. This leads to non-visual senses becoming more dominant during social interaction and causes atypical behaviors to emerge (Wrzesińska et al., 2017). Ultimately, this process can negatively affect the development of more complex social skills such as empathy, prosocial peer relationships, and imitation/play (Zimmer-Gembeck et al., 2011).
Another remarkable study result was that sensory processing skills of toddlers with CP and CVI were not differed from toddler with CP without CVI. It has been suggested that the underdevelopment of cortico-thalamic pathways secondary to diffuse white matter damage and neuromuscular deficits resulting from the nature of CP cause SPDs in children with CP (Pavão & Rocha, 2017; Tsao et al., 2014). Moreover, it has also been suggested that the atrophy of the thalami may play an additional role in the abnormal development of visual function in infants (Ricci et al., 2006), and VI negatively affects the integration of multiple sensory modalities (Houwen et al., 2022). Therefore, toddlers with CP and CVI are likely to experience sensory processing difficulties because multiple disorders may negatively affect their sensory development (Cemali et al., 2022). However, a statistically significant difference was not found in ITSP domain scores in our study. This finding may be attributed to the varied severity levels observed among the toddlers with CP included in the study. As children with severe forms of CP are more prone to experiencing SPDs and CVI (Ghasia et al., 2008; Park, 2017), the absence of significant differences could be linked to this variability. Moreover, considering that the visual system continues to mature and certain components of visual ability do not reach full maturity until late teens (Brémond-Gignac et al., 2011), it may take some time for pre-existing VIs to fully manifest their impact on other developmental domains.
This cross-sectional study aimed at investigating the CVI role in social competence and sensory processing skills in children with CP aged 1–3 years. Although social competence includes many different aspects of social development, such as social adaptation, social emotion, social cognition, and social interaction (You et al., 2019; Zmyj et al., 2017), our study provided limited information due to parent reporting only. That is, it was only shown whether social competence or sensory processing skills were affected by CVI. However, it was not shown how and by which mechanism CVI affected them. In addition to our results, further studies should be conducted on the process of the influence of CVI on social competence.
While our study excluded toddlers with significant ocular comorbidities and did not measure toddlers’ primary visual functions, it is worth considering the broader context. High rates of ophthalmic comorbidities have been reported in toddlers with CP and CVI (West et al., 2021). Nevertheless, it is noteworthy that autistic-like manifestations in children with CVI appear to be more closely linked to diffuse brain damage rather than the extent of vision loss (Fazzi et al., 2019). Furthermore, it is essential to acknowledge that our study was conducted within a special education and rehabilitation institution, which posed limitations on conducting comprehensive ophthalmologic examinations for all participants. Due to the practical constraints of our study setting, we were unable to gather detailed ophthalmologic data on the primary visual function of children with CP. In addition, it is important to address the constraints of the scales completed by families. Our study was limited by the lack of observation or simultaneous objective measurement. Another important limitation of our study is the omission of other aspects of CP, including etiological factors and intellectual development. These factors were not solely reliant on parental verbal declarations but required a review of medical files. Future research endeavors would benefit from exploring various facets of CP to provide a more comprehensive understanding of this condition.
This study’s findings hold important implications for OT practice, especially in early intervention for children with CP and CVI. Understanding the intricate relationship between CP, CVI, and sensory processing enables OTs to provide tailored interventions, ultimately improving children’s quality of life and participation in daily activities.
Conclusions
The results of this study suggest that toddlers with CP and CVI may show less social competence skills than toddlers with CP without CVI. On the contrary, CVI was found not to affect sensory processing skills. Habilitation specialists should consider social competence when conducting habilitation programs in toddlers with CP and CVI. More studies investigating the impact of CVI on social competence and sensory processing skills are needed.
Footnotes
Acknowledgements
The authors are deeply grateful to Dr. Serkan Pekçetin for their unwavering support and encouragement throughout this project. His insightful feedback and constructive criticism have been instrumental in helping us improve our work and achieve our goals. Also, the authors thank all the toddlers and their families who participated in our study.
Ethical Approval
Our study was approved by the Ethics Committee of Hacettepe University (Registration Number: GO 22/351; Registration Date: May 22, 2022).
Informed Consent
Prior to gathering data, all parents gave their informed written consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.